Article Text

Abstract
Objectives To examine the knowledge, attitude and practice (KAP) regarding immune-related adverse events (irAEs) and nutritional support among patients with liver cancer (LC).
Design Cross-sectional study.
Setting Recruitment was carried out at Haikou People’s Hospital, Haikou, China, from December 2022 to April 2023.
Participants Patients undergoing immunotherapy for LC.
Primary and secondary outcome measures Mean knowledge, attitudes, practices, and lifestyle scores were assessed using an investigator-designed questionnaire completed by patients during immunotherapy.
Results The study included 402 participants. The mean knowledge, attitudes, practices and lifestyle scores were 6.60±3.51 (/10, 66.00%), 41.26±5.06 (/50, 82.52%), 30.74±4.20 (/40, 76.85%) and 42.37±6.04 (/55, 77.04%), respectively. Attitude scores were associated with practice scores (β=0.381, p<0.001) and lifestyle (β=1.928, p<0.001). Urban residence was associated with higher attitude scores (β=1.242, p=0.013). Living with someone was associated with a higher attitude score (β=1.619, p=0.044). More than one immunotherapy line was associated with a higher lifestyle score (β=1.928, p<0.001). Finally, the female gender was associated with a lifestyle score (β=1.431, p=0.023).
Conclusion Patients with LC and undergoing immunotherapy had moderate KAP towards irAEs and nutritional support. They also displayed moderate lifestyle scores. Urban residents, people not living alone, females and those having received two or more immunotherapy treatments were positively associated with attitude, while attitude was positively associated with practice and lifestyle.
- Cross-Sectional Studies
- ONCOLOGY
- Hepatobiliary tumours
- PUBLIC HEALTH
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. All data generated or analysed during this study are included in this article and its supplementary materials.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
While a cross-sectional design is useful for capturing data at a single time point, it limits the ability to establish causality or infer temporal relationships between variables.
Conducting the study at a single hospital may introduce selection bias and limit the generalisability of the findings to other settings or populations.
The reliance on self-reported measures for assessing knowledge, attitude, practice and lifestyle introduces the potential for response bias and social desirability bias, impacting the accuracy of the results.
Although the study identifies certain factors that were associated with attitudes and lifestyle, there may be other unmeasured confounding variables that could affect the outcomes.
While the study assessed knowledge, attitude and practices towards immune-related adverse events, nutritional support and lifestyle factors, it may not capture all relevant aspects involved in patient care and outcomes during immunotherapy for lung cancer.
Introduction
The estimated worldwide incidence of liver cancer (LC) in GLOBOCAN 2022 was 865 269 new cases, and mortality was 757 948.1 Most LCs are hepatocellular carcinoma (HCC).2 3 The worldwide age-standardised annual mortality rates of LC are 13.9 per 100 000 in men and 4.9 per 100 000 in women.4 The most important risk factors for LC are pre-existing liver cirrhosis and hepatitis B infection (due to both direct oncogenic effect and risk of cirrhosis).2 3 5 6 Risk factors for liver cirrhosis (and therefore risk factors for LC) include hepatitis C infection, alcohol use and nonalcoholic steatohepatitis.2 3 5 6 The incidence of LC is higher in men and generally follows the geographical distribution of hepatitis B virus and hepatitis C.2 5 6 LC management is multidisciplinary and involves surgery (when possible), chemotherapy, targeted therapy, radiotherapy and immunotherapy.2 5 6 Despite optimal treatments, the 5 year survival is 22% in the USA7 and 12.1% in China,8 with lower survival in rural China (11.2%) compared with urban areas (14.0%).9
Immunotherapy is a recent paradigm in treating cancers, including LC.10–12 Cancer cells can escape the immune system through the PD-1/PD-L1 pathway,13 14 and drugs targeting PD-1 or PD-L1 have been developed to restore the immunosurveillance of cancer cells and their destruction.10–12 Still, the PD-1/PD-L1 usually plays roles in immune tolerance and preventing autoimmune reactions,13 14 and inhibiting the PD-1/PD-L1 pathway can lead to immune-related adverse events (irAEs). The pathogenesis of irAEs is still poorly understood, but they involve inflammatory reactions of normal tissues that can be bothersome but also life-threatening.15–17
Adequate nutrition is also essential in patients with LC to ensure optimal outcomes, and nutritional support can be necessary in patients with inadequate nutrition due, for example, to gastrointestinal adverse events (AEs) from therapies.18 19 Still, the palliation of some symptoms of HCC (eg, loss of appetite, weakness, fatigue, etc) using androgens (since most LCs occur in males) can help alleviate the need for nutritional support.20 The management of irAEs and nutrition involves healthcare providers. It can involve medical interventions (eg, management of irAEs, enteral nutrition and hospitalisation). However, patient self-management is also important to ensure that preventive measures are taken (such as not smoking, not drinking and eating properly) and so that patients know when to consult.21
A systematic review showed that the eating habits of Chinese patients with cancer and chemotherapy were poor, but no data are available for immunotherapy specifically.22 Another study suggested that Chinese patients with cancer had a basic understanding of irAEs,23 but this study was not specific to LC and did not evaluate attitudes and practices. A knowledge, attitude and practice (KAP) survey is a tool that provides quantitative and qualitative data about gaps, misconceptions and misunderstandings that constitute barriers towards the optimal performance of a given task or set of tasks in a specific group of individuals.24 25 Compared with other types of cancer, for example, breast cancer, patients with LC have a poorer prognosis, and men are more at risk. In addition, the risk factors for LC are different from other cancers, mainly encompassing chronic liver diseases, alcohol drinking and hepatitis virus infection. Those differences could influence patients’ KAP towards irAEs.
Therefore, this study aimed to investigate the KAP lifestyle (KAP-L) of patients with LC and immunotherapy patients regarding nutritional support and irAEs. The results can provide crucial information to design educational interventions to improve patient self-management and outcomes.
Materials and methods
Study design and participants
This cross-sectional study was conducted at Haikou People’s Hospital from December 2022 to April 2023 and enrolled patients undergoing immunotherapy for LC. This study was approved by the Institutional Review Board of Haikou People’s Hospital (2022-Ethical Review-231). All participants signed the informed consent form before completing the survey.
The inclusion criteria were (1) aged 18–90 years, (2) pathologically confirmed locally advanced or unresectable LC and (3) undergoing immunotherapy (any line of treatment). The exclusion criteria were (1) surgical patients; (2) simultaneously suffering from other malignant tumours; (3) before or planned liver transplantation; (4) active autoimmune diseases; (5) ambiguous consciousness, unable to fill out by oneself or with assistance; or (6) withdrawal during the filling process.
Questionnaire and quality control
A self-designed questionnaire consisting of five dimensions was developed based on the relevant literature.15 18 19 22 23 26 After the questionnaire design, modifications were made by incorporating insights from 15 experts in nutrition in oncology and medical oncology, removing similar or redundant questions and refining questions with unclear phrasing. Before the official distribution, a small-scale pilot test (70 participants) was conducted, yielding a Cronbach’s α coefficient of 0.853 (0.879 for knowledge, 0.828 for attitudes and 0.758 for practice), indicating strong internal consistency.
The final questionnaire was in Chinese and encompassed (1) participants’ demographic information (including age, gender, residential area, education level and income level, etc), (2) knowledge dimension (10 items, with a score of one assigned for correct answers and zero for incorrect or uncertain responses), (3) attitude dimension (10 items, scored using a five-point Likert scale, ranging from ‘strongly positive’ (five points) to ‘strongly negative’ (one point)), (4) practice dimension (eight items, scored using a five-point Likert scale, ranging from ‘always’ (five points) to ‘never’ (one point)) and (5) lifestyle dimension (11 items, also scored using a five-point Likert scale, ranging from ‘always’ (five points) to ‘never’ (one point)). Higher scores correspond to better knowledge, more positive attitudes and more proactive practices. Scores <60% were considered poor, scores 60%–79% were considered moderate and scores >80% were considered adequate, based on Bloom’s criteria.27
An online questionnaire was developed using the WeChat-based Wenjuanxing platform. A QR code was generated for data collection via WeChat. The participants accessed and completed the questionnaire by scanning the QR code received via WeChat. In order to ensure the quality and completeness of the questionnaires, all items were made mandatory. Incomplete questionnaires were excluded during the quality control process. Therefore, all items were responded to, which would not affect the results.
The research team members reviewed the integrity, internal consistency and rationality of all collected questionnaires for quality control. A given IP address could be used to submit a questionnaire only once. Questionnaires that took <110 s to complete were excluded. Questionnaires completed using all the same options (eg, the first option) were deemed invalid. Finally, questionnaires containing impossible values (eg, impossible age, height or weight) or logical errors were excluded. The Cronbach’s α coefficient for all valid questionnaires was 0.840 (0.913 for knowledge, 0.800 for attitudes and 0.718 for practice).
Statistical analysis
The statistical analysis software was SPSS 26.0 (IBM, Armonk, NY, USA). Quantitative variables were described as means±SD, while group comparisons were conducted using Student’s t-test or analysis of variance. Categorical variables were presented as n (%). Pearson’s correlation analysis explored the relationships between KAP scores. The study used a structural equation modelling (SEM) analysis to validate various causality hypotheses empirically. These hypotheses encompassed (1) knowledge has direct associations with attitudes, practices and lifestyles, (2) attitudes have direct associations with practices and lifestyles, (3) residential area and status have direct associations with attitudes, (4) gender has direct associations with attitudes and lifestyles and (5) the number of immunotherapy medication usage has a direct association with lifestyles. All statistical tests were two-tailed, and P values <0.05 were considered statistically significant.
Results
Characteristics of the participants
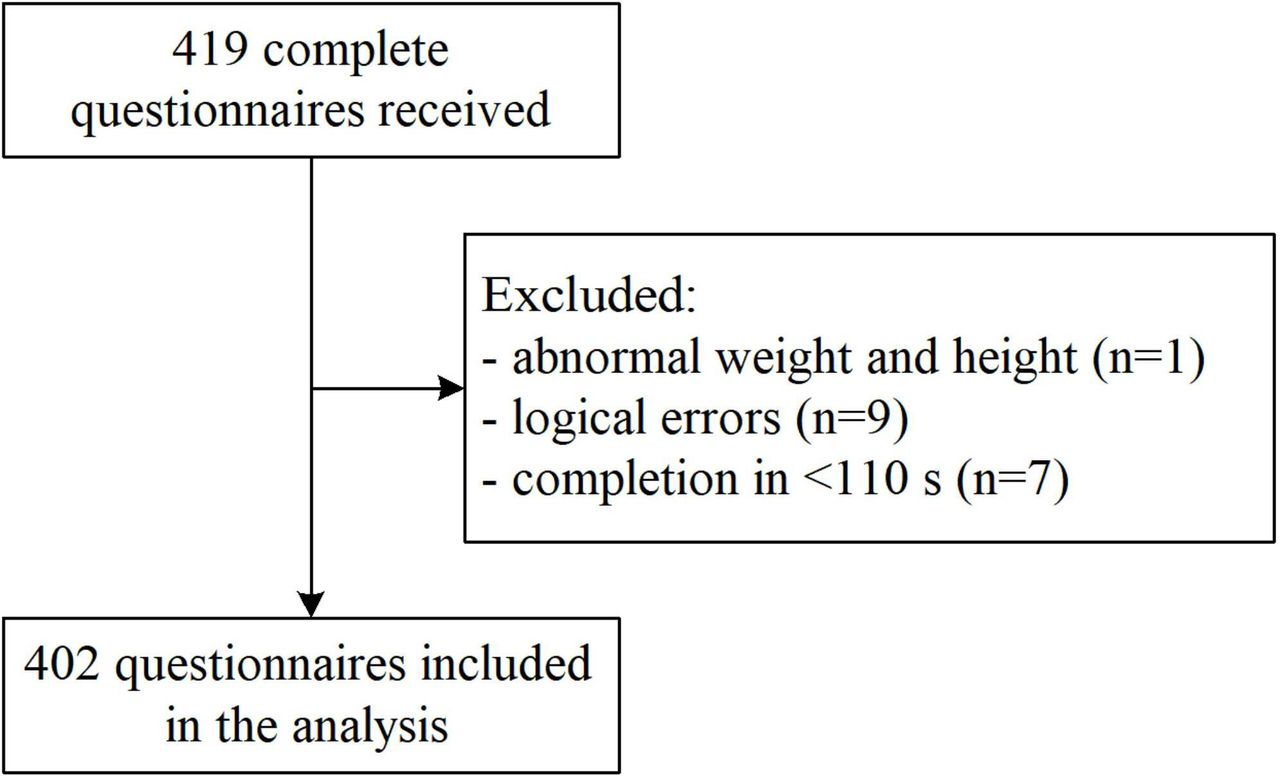
The study included 419 respondents. After removing the following cases: (1) one respondent with impossible height and weight, (2) nine respondents answered with contradictory answers and (3) seven respondents with a completion time of less than 110 s, a total of 402 valid questionnaires were included in the analysis (figure 1). The participants’ ages were 56.84±11.93 years. Most participants were male (71.89%), had a body mass index of 18.5–23.9 kg/m2 (60.95%), were living in rural areas (55.97%), were not living alone (89.30%), were married (90.05%), had high school or technical secondary school education (34.08%), had an income of 2000–5000 RBM/months (48.76%), had health insurance (99.50%), had gastrointestinal symptoms (50.75%), did not experience irAEs (89.80%), received one line of immunotherapy (54.23%) and were not familiar with the name of their immunotherapy (65.17%) (online supplemental table S1).
Supplemental material

Questionnaire flowchart.
Knowledge
The mean knowledge score was 6.60±3.51 (/10, 66.00%) (table 1). No significant differences were observed according to the characteristics of the participants. The knowledge item with the lowest score was K1 (50.75%; “Adverse reactions can occur during immunotherapy, but they are normal occurrences that do not require excessive attention.”), while the item with the highest score was K9 (72.39%; “Prompt identification and timely reporting of symptoms of malnutrition and immune-related events to healthcare professionals are not only beneficial for immunotherapy and ameliorating immune-related adverse symptoms and nutritional status but also increase the likelihood of continuing immunotherapy.) (online supplemental table S2).
Knowledge, attitude and practice scores
Attitude
The mean attitude score was 41.26±5.06 (/50, 82.52%) (table 1). Higher attitude scores were observed in urban dwellers (41.99±5.19 vs 40.68±4.89, p=0.010), those not living alone (41.44±5.07 vs 39.72±4.76, p=0.035) and those with higher income (>20 000 CNY/month: 43.50±3.46; <2000 CNY/month: 39.66±5.88; p=0.005) (online supplemental table S1). The attitude item with the lowest score was A1 (64.52%; “I consider nutritional support to be highly significant throughout the entire course of immunotherapy.”), while the item with the highest score was A10 (93.28%; “I believe that maintaining a positive mindset and quality sleep are important during immunotherapy.”) (online supplemental table S2).
Practice
The mean practice score was 30.74±4.20(/40, 76.85%) (table 1). No significant differences were observed according to the characteristics of the participants. The practice item with the lowest score was P6 (39.53%; “If required, I am prepared to receive enteral feeding through nasogastric/nasoenteric tubes.”), while the item with the highest score was P1 (86.07%; “I am capable of cooperating with medical personnel for comprehensive treatment monitoring and follow-up.”) (online supplemental table S2).
Lifestyle
The mean lifestyle score was 42.37±6.04 (/55, 77.04%) (table 1). Higher lifestyle scores were observed in females (43.43±5.36 vs 41.95±6.24, p=0.027), widows (widows: 45.20±5.55; married: 42.49±5.99; unmarried: 39.09±6.45; p=0.031) and with more than one immunotherapy line (43.46±6.06 vs 41.45±5.88, p=0.001) (online supplemental table S1). The lifestyle item with the lowest score was L11 (30.35%; ‘citrus fruits (grapefruit, pomelo, honey pomelo, etc.).)’), while the item with the highest score was L2 (83.84%; ‘alcohol consumption’) (online supplemental table S2).
Correlations
The knowledge scores were correlated to the attitude scores (r=0.105, p=0.035). The attitude scores were correlated to the practice (r=0.460, p<0.001) and lifestyle (r=0.486, p<0.001) scores. The practice scores were correlated to the lifestyle scores (r=0.269, p<0.001) (table 2).
Pearson correlation analysis
SEM
As shown in table 3 and figure 2, higher attitude scores were associated with higher practice scores (β=0.381, p<0.001) and lifestyle (β=1.928, p<0.001). Urban residence was associated with higher attitude scores (β=1.242, p=0.013). Living with someone was associated with higher attitude scores (β=1.619, p=0.044). More than one line of immunotherapy lines was associated with higher lifestyle scores (β=1.928, p<0.001). The female gender was associated with higher lifestyle scores (β=1.431, p=0.023). (online supplemental table S3) shows that the SEM analysis had a good fit.

{kind=link}
{kind=link}
Structural equation modelling.
Structural equation modelling, including lifestyle
Discussion
Very few data are available in the literature concerning the KAP of patients with LC towards irAEs and lifestyle habits. The present study revealed moderate KAP towards lifestyle habits and irAEs. A previous systematic review has shown that the eating habits of Chinese patients with cancer and chemotherapy were poor.22 Although no data were available within this systematic review for immunotherapy, its findings are generally in alignment with our present study. Another study has shown that Chinese patients with cancer had a basic understanding of irAEs,23 but the study was not specific to LC and did not evaluate attitudes and practices. Intrinsic differences between patients with LC and those with other types of cancer could explain the differences in findings.
Symptoms of advanced HCC affect quality of life, and the treatment of HCC can restore quality of life.28 Thus, immunotherapy can potentially reverse the HCC-related symptoms and help improve quality of life. Nevertheless, the side effects of immunotherapy need to be factored in, as it can affect empowerment and self-management. Self-management is a critical component of cancer care. Indeed, the patients must remain aware of the signs and symptoms that should prompt consultation. At home, they are also responsible for maintaining lifestyle habits that could improve their prognosis or, at least, not worsen it.21 A previous systematic review revealed poor KAP towards good eating habits among Chinese patients on chemotherapy for various types of cancers.22 That previous study supports the present one, which also showed poor lifestyle scores for several foods in patients with LC and immunotherapy. Increasing evidence indicates that a healthy diet can improve the outcomes of immunotherapy.29 30
In this study, many participants with LC were still regularly smoking, drinking alcohol and had unhealthy dietary habits, all of which are associated with LC development and progression.31–34 Especially, smoking and alcohol consumption are independent risk factors for confirmed LC2 3 5 6 because of their impact on inflammation, cancer progression and health in general,35–37 and they affect liver function and immunotherapy efficacy.38 Still, the high rates of smoking and drinking could reflect a poor knowledge of the risk factors for poor outcomes in LC but could also reflect patients wishing to maintain activities they associate with pleasure in the face of a disease with poor prognosis. The majority of the participants were not eating citrus fruits. Citrus fruits are rich in vitamins and antioxidants and play roles in maintaining the integrity of immunological barriers and in supporting immune cells.39–41 On the other hand, citrus fruits are rich in active ingredients, such as furacoumarin, naringin and bergamot, which can inhibit the activity of metabolic enzymes (mainly UGT1A3 or UGT2B7).42 Therefore, in the future, intervention research on the impact of fruits such as grapefruit on medication can be strengthened. Therefore, the lifestyle of the study population was not ideal in terms of LC prognosis.31–34
The participants mostly reported not taking probiotics. Recent data also suggests that probiotics should be encouraged to prevent irAEs.43 Indeed, regulation of the gut microbiome appears crucial in preventing irAEs.44 The gut microbiota was also shown to modulate the response to immunotherapy, with distinct responses to immunotherapy according to the composition of the microbiome.45 Gut dysbiosis can even lead to resistance to immunotherapy.45 Hence, administering specific bacteria could be used to improve the response to immunotherapy and prevent irAEs.46
People living in urban areas and not living alone often enjoy a higher socioeconomic status, and it is well-known that higher socioeconomic status is associated with better health literacy.47 In this study, living in urban areas was associated with higher attitude scores than participants from rural areas.
Women often have a higher healthcare literacy and higher health awareness than men,48–51 supporting the association observed in the present study between gender and lifestyle. In addition, family support plays an undeniable advantage in the management of cancer patients, helping them with daily tasks, cooking for them, caring for them and remembering instructions and advice that the patients might forget due to the emotional charge associated with cancer-related events.52 53 The present study was not designed to assess that point. Nevertheless, efforts should be taken to teach patients with LC the proper lifestyle habits necessary to optimise prognosis. Expanding the scope of the survey and including hospitals in different regions and levels are recommended to validate the results of this study. Clinical intervention research should be performed on the knowledge, attitude, behaviour and lifestyle level of nutrition and irAEs in patients with LC and immunotherapy and evaluate the effectiveness of the intervention. The impact of good sleep and moderate exercise (as good lifestyles) in relation to nutrition and irAEs should also be examined.
In the present study, the knowledge scores were only correlated to the attitude scores, while the attitude scores were correlated to the practice and lifestyle scores. Although knowledge was not associated with attitude in the SEM, improving knowledge could translate into attitude, practice and lifestyle improvements. Healthcare providers are a primary source of information for the patients, but previous studies revealed relatively poor KAP towards cancer nutritional support26 54 and irAEs55 among healthcare providers. Patients with LC and immunotherapy should be encouraged to perform physical activity, which is akin to prehabilitation for liver resection to improve tolerance to treatment.56 It should help reduce the side effects or increase the patient’s tolerance to them, hence improving patient outcomes.
This study has limitations. It was a single-centre study. Even though 402 patients with LC and immunotherapy represent a relatively large sample size, it is still too small to derive correlations and recommendations regarding the KAP-L in patients with LC. The questionnaire was designed by the investigators. It was reviewed by 15 experts in LC management, which could introduce bias from the healthcare perspective. In addition, some questions contained medical jargon that could introduce the Hawthorne effect (a type of reactive human behaviour in which people change their behaviour when they feel observed). The question length could be a potential source of bias on the importance ratings. Participants can consider a long and complicated sentence as important and a short sentence as being less important, causing bias. Future surveys should also be reviewed by nursing experts, laypeople and a variety of professionals. The study was cross-sectional in design, preventing us from drawing conclusions around causality. Still, a SEM analysis was performed to examine the structured associations between variables, but it must be remembered that the associations are purely statistical and remain to be confirmed. In addition, the data represent a single point in time. Still, the results could serve as a historical baseline to evaluate the effect of future interventions. The questionnaire was designed by local investigators based on local practice, policies and reality, limiting generalisability. Finally, all KAP studies are at risk of social desirability bias, in which some participants might be tempted to answer what they know they should do instead of what they are actually doing.57 58
In conclusion, patients with LC and immunotherapy had moderate KAP towards irAEs and nutritional support. They also displayed moderate lifestyle scores. Urban residents, people not living alone, females and having received two or more immunotherapy treatments were positively associated with attitude, while attitude was positively associated with practice and lifestyle.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. All data generated or analysed during this study are included in this article and its supplementary materials.
Ethics statements
Patient consent for publication
Ethics approval
This work has been carried out in accordance with the Declaration of Helsinki (2000) of the World Medical Association. This study was approved by the Institutional Review Board of Haikou People’s Hospital (2022-Ethical Review-231). All participants signed the informed consent form before completing the survey.
References
Footnotes
Contributors WW and FG carried out the studies, participated in collecting data and drafted the manuscript. YC and LT performed the statistical analysis and participated in its design. WW and YC participated in the acquisition, analysis or interpretation of data and drafted the manuscript. All authors read and approved the final manuscript. FG acted as guarantor.
Funding This study was supported by the Hainan Provincial Natural Science Foundation of China (823MS169) to Wen Wen and the Healthy Department of Hainan Province (22A200123) to Wen Wen.
Competing interests None declared.
Patient and public involvement Patients with LC were involved as participants. The patients with LC or the public were not involved in the study design or its completion.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.