Article Text

Abstract
Objectives In view of the serious ageing of China’s population and the low desire of elderly people to purchase institutionalised elderly care services, we explored the willingness of Chinese elderly people to purchase institutionalised elderly care services and its influencing factors.
Design This was a cross-sectional study. Three multivariate logistic regression analysis models of the willingness of elderly people to purchase institutionalised elderly care services were established (model 1: ‘reluctance – willingness’; model 2: ‘reluctance – hesitation’; and model 3: ‘hesitation – willingness’) to explore the factors that influence elderly people’s willingness to purchase institutionalised elderly care services.
Setting This study was based on the 2022 Psychology and Behaviour Investigation of Chinese Residents database.
Participants Research data from 4123 older adults who met the requirements of this study were screened from the database.
Results Of the 4123 respondents, roughly equal numbers had negative and positive attitudes towards purchasing institutionalised senior care services (1125, 27.3% vs 1079, 26.2%, respectively), and 1919 (46.5%) had hesitant attitudes. The analysis of model 1 showed that medical insurance participation, the number of children and siblings, chronic diseases and per capita monthly household income had an influential effect on the willingness of elderly people to purchase institutional care. In model 2, we found that factors such as per capita monthly household income and anxiety led to hesitancy among older adults to purchase institutionalised senior care services. In model 3, we further found that social support and health literacy led to a shift from hesitation to willingness to purchase institutionalised elderly care services.
Conclusion The number of children, number of siblings, per capita monthly income of the family, medical insurance participation, health status, health literacy and social support were found to be the main factors influencing the purchase of institutionalised care by elderly individuals.
- GERIATRIC MEDICINE
- Health Services for the Aged
- Aged
- Aging
Data availability statement
Data may be obtained from a third party and are not publicly available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The participants were from 148 cities in 22 provinces, 5 autonomous regions and 4 municipalities.
This study used stratified and quota sampling methods.
The factors that influence the purchase of institutional care services by elderly people are varied; thus, it was difficult to include all the possible influences in this study.
This was a cross-sectional study in which only the phenomenon was analysed; an in-depth explanation of the reasons behind the phenomenon requires the design of a rigorous mixed qualitative and quantitative study.
Background
Population ageing has become a global issue. According to the WHO, by 2030, one-sixth of the world’s population will be older than 60 years, and the number of people older than 60 will increase from 1 billion to 1.4 billion from 2020 to 2030.1 China has one of the fastest-ageing populations in the world.1 It is expected that by 2025, China’s elderly population aged 60 years and older will reach 300 million, accounting for more than 20% of the total population.2 According to the National Population Development Plan (2016–2030), it is predicted that the proportion of elderly people older than 60 years in China will be greater than 25% in 2030,3 which means that 1 out of every 4 people will be older than 60 years. As the proportion of China’s elderly population continues to increase, the social burden of old age is gradually increasing.
Along with the increase in the proportion of the elderly population, the fertility rate of mainland China’s population has shown a continuous downwards trend, while the per capita life expectancy has shown an upwards trend; these trends will inevitably lead to an increase in the degree of population ageing and in the burden of old-age pensions faced by society. Moreover, the demographic structure of Chinese families shows an inverted pyramid pattern in which a couple must take care of four elderly parents and one child.4 This ‘4-2-1’ family demographic structure makes ‘how to age’ an important issue in society.
Previous studies have shown that in the Chinese context of old age, family care has long been the core means of supporting older people.5 Compared with Western countries, the Confucian idea of filial piety has led Chinese people to believe for thousands of years that most elderly people who receive care from institutions are there because their children are ungrateful.6 They believe that their children’s unwillingness to take care of them makes them lose face; thus, most elderly people choose to age in their families. This finding suggests that intergenerational ties and obligations are generally stronger in Chinese families than in Western societies.7 However, in Chinese families, children’s ability to care for elderly adults has been eroded by demographic changes and socioeconomic development.8 The younger generation has had to move to cities to work, which means that family-centred forms of care for elderly individuals are gradually disappearing9; thus, there is an inevitable growing demand for institutional care. To cope with the growth of a rapidly ageing population, the Chinese government has released a blueprint for an emerging ageing service and support network that aims to establish a social ageing system of home-based ageing with community-based ageing as the necessary support and institutionalised ageing as a supplement.10 In 2020, the Proposal of the Central Committee of the Communist Party of China on the Formulation of the Fourteenth Five-Year Plan for National Economic and Social Development and Vision for 2035 proposed the implementation of a national strategy of actively coping with the ageing of the population, promoting the synergistic development of old-age care and the old-age care industry, and constructing an old-age care system that combines medical care and recreation with old-age care and the goal of increasing the number of public institutions for old-age care in accordance with the 14th Five-Year Plan for Old-Age Care and Services Development.11 The Chinese government is making great efforts to improve the quality of institutional care services and the training of specialised caregivers. This will promote the rapid development of institutional care services to continue to satisfy the growing demand of elderly people for multilevel, high-quality, healthy old-age care.
Institutionalised elderly care generally refers to service institutions that provide comprehensive services for elderly individuals, such as food and living, cleaning and hygiene, life care, health management and cultural, sports and recreational activities. Institutional care can reduce the burden of care on children, provide specialised care services and enrich the leisure activities of elderly individuals. However, the results of a cross-sectional survey of several regions suggest that many factors may influence the acceptance of institutionalised care among Chinese seniors. For example, a rapidly changing society is changing traditional family care for elderly individuals, resulting in a tendency for elderly Chinese people to choose institutionalised care as a way of ageing.12 Negative news about elderly care institutions often leads to negative attitudes towards institutionalised care.13 In addition, China is a vast country with enormous differences in economic and cultural conditions in different regions, which may affect the willingness of elderly individuals to purchase institutionalised elderly care services.14 The above-mentioned studies have elaborated on the factors that influence the willingness of elderly people to purchase institutional care services.15 However, the samples of these studies were limited by regional constraints and are thus not representative of the overall situation in mainland China.
Supported by the ‘2022 China Population Psychological and Behavioural Tracking Survey Project’, we conducted a national cross-sectional survey in mainland China to fully understand the willingness of elderly people to purchase institutionalised elderly care services and the factors that influence this willingness. This study can support the improvement of the level of institutionalised elderly care services in society and the enhancement of elderly people’s sense of well-being and security.
Information and methodology
Data sources
The study data were obtained from the Psychology and Behaviour Investigation of Chinese Residents, 2022 database.16 The China Population Psychological and Behavioural Survey aims to establish a database through a multicentre, large-sample cross-sectional survey to provide strong data support for the development of research in various fields and for a comprehensive and systematic understanding of the public’s physical and mental health. The cross-sectional survey was initiated by the School of Public Health, Peking University and conducted from 20 June 2022 to 31 August 2022, using stratified and quota sampling methods to select 148 cities, 202 districts and counties, 390 townships/streets and 780 communities/villages in 23 provinces, 5 autonomous regions and 4 municipalities directly under the central government of mainland China. The questionnaires were distributed to the public one-on-one and face-to-face by surveyors. After the respondents provided informed consent, they could click on a link to complete the questionnaire.
The screening criteria for the sample of this study were as follows: (1) ≥60 years of age or older, (2) nationality of the People’s Republic of China, (3) resident of China (annual time away from home ≤1 month), (4) voluntary participation in the study and completion of the informed consent form, (5) completion of the network questionnaire survey independently or with the help of investigators and (6) understanding of the meaning of each item in the questionnaire. The sample exclusion criteria were as follows: (1) had a mental disturbance, (2) had a cognitive impairment, (3) were participating in other research on similar topics and (4) did not wish to collaborate.
The questionnaire was completed by 30 505 participants from 148 cities in 22 provinces, 5 autonomous regions and 4 municipalities directly under the central government of mainland China. Based on the sample selection criteria and exclusion criteria, research data from 4123 older adults were ultimately included in this study.
Research instrument
The visual analogue scale (VAS) was used to assess the willingness of elderly people to purchase institutionalised elderly care services. The items were rated from 0 (unwillingness to purchase) to 100 (strong willingness to purchase). The higher the score, the greater the willingness of elderly respondents to purchase institutionalised elderly services. The first 27% of the participants with VAS scores were considered to have a negative attitude towards institutionalised elderly services, the last 27% were considered to have a positive attitude towards institutionalised elderly services, and the remaining sample was considered to have a hesitant attitude towards institutionalised elderly services.17
The short-form Health Literacy Survey (HLS-SF12) was used to assess the health literacy level of the respondents. The HLS-SF12 was developed by Sun et al18 to assess respondents’ ability to find, understand, evaluate and apply health-related information. The options are rated on a Likert scale ranging from ‘very difficult’ (one point) to “very easy” (four points). The total score of the items ranges from 0 to 36, with the top 50% of the scores considered to indicate a high level of health literacy and the bottom 50% considered to indicate a low level of health literacy.19 The Cronbach’s coefficient for the HLS-SF12 in this study was 0.910.
The Perceived Social Support Scale (PSSS) was applied to assess respondents’ feelings about the social support they received. The PSSS evaluates the extent to which individuals feel supported by family, friends and others in terms of three dimensions, namely, family support, friend support and support from others, with the total score reflecting the degree of total social support felt by the individual. A Likert scale is used that ranges from ‘strongly disagree’ (one point) to ‘strongly agree’ (seven points). The total possible score is 21, with a higher total score indicating a higher level of social support for the individual.20 Respondents with scores in the top 50% are considered to have a higher level of social support, and respondents with scores in the bottom 50% are considered to have a lower level of individual social support. Cronbach’s coefficient for the PSSS in this study was 0.928.
The General Anxiety Disorder-7 (GAD-7) scale was used to measure the respondents’ anxiety. Each entry on the GAD-7 scale is rated from 0 to 3, and the total score ranges from 0 to 21. The seven items are summed to produce a final rating that indicates the frequency of anxiety symptoms. A score of 0–4 indicates no anxiety, 5–9 indicates mild anxiety, 10–14 indicates moderate anxiety and 15 or more indicates severe anxiety.21 The Cronbach’s coefficient for the GAD-7 scale in this study was 0.927.
The Patient Health Questionnaire-9 (PHQ-9) was used to measure the depressive state of the respondents. Options are rated on a Likert scale ranging from ‘never’ (zero point) to ‘nearly every day’ (four points). The nine items are summed to give a total score ranging from 0 to 36, indicating the frequency of depressive symptoms. A score of 0–4 is categorised as no depression, 5–9 is categorised as mild depression, 10–14 is categorised as moderate depression and 15–27 is categorised as severe depression.22 The Cronbach’s coefficient for the PHQ-9 in this study was 0.916.
Statistical methods
Descriptive statistics were applied to analyse the percentages of patients’ sociodemographic information, social structure, economic status and other factors for different samples. A χ2 test was applied to analyse the differences in the willingness of elderly respondents to purchase institutional care in different sociological contexts. Three multivariate logistic regression analysis models of elderly people’s willingness to purchase institutionalised elderly care services were established (model 1: ‘reluctance – willingness’; model 2: ‘reluctance – hesitation’; and model 3: ‘hesitation – willingness’) to explore the factors that influence elderly people’s purchase of institutionalised elderly care services. The data were organised using Excel 2019 (Microsoft, Washington, DC, USA), and the data were analysed using IBM SPSS Statistics (V.26, IBM) and R language (V.4.2.3).
Patient and public involvement
No patients were involved in setting the research question or the outcome measures, nor were they involved in developing plans for design or implementation of the study.
Results
Sample distribution
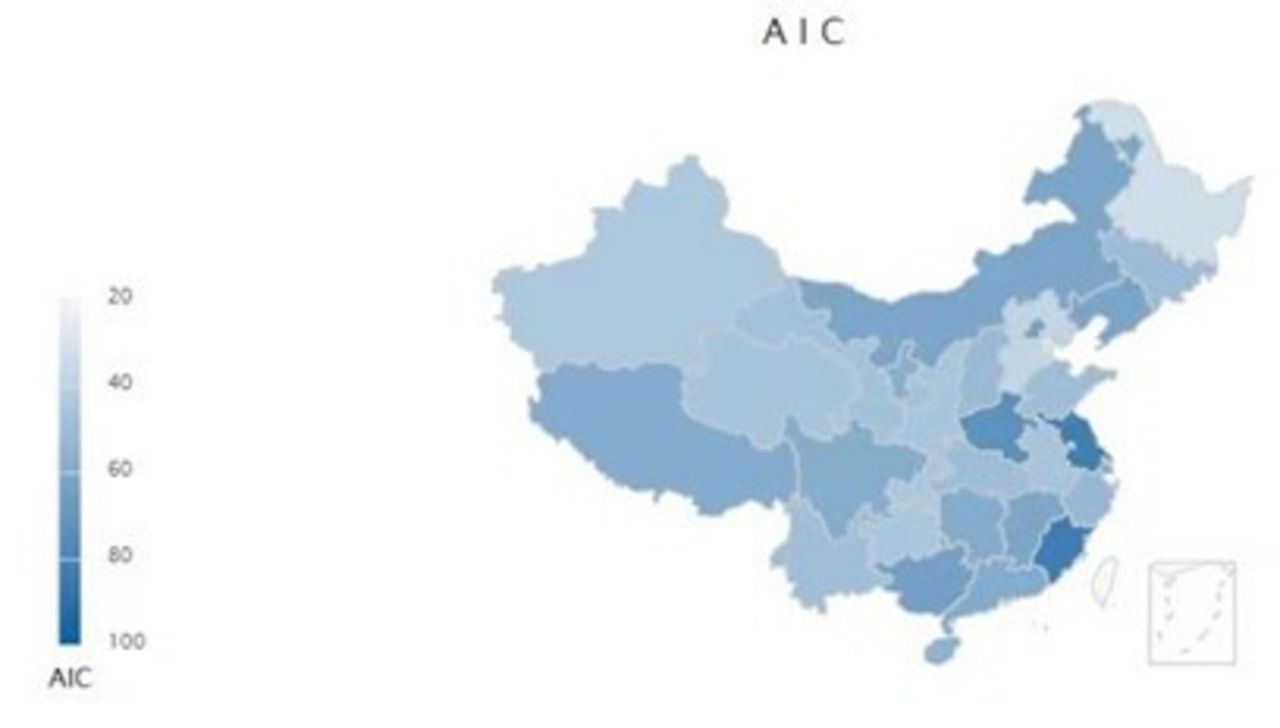
The 4123 study samples came from 780 residential communities in 22 provinces, 5 autonomous regions and 4 municipalities in mainland China. Overall, the willingness of elderly people to purchase institutionalised elderly care services was generally high in central and eastern China, while the willingness of elderly people to purchase institutionalised elderly care services was generally low in northwestern and northeastern China. The distribution of elderly people purchasing institutional care services in different provinces in mainland China is shown in figure 1, and the scores of elderly people purchasing institutional care services in different provinces in mainland China are shown in figure 2.

Distribution of older adults purchasing institutional care services in different provinces in mainland China.

{kind=link}
{kind=link}
Purchase of institutional care services by the older adults in different provinces in mainland China online supplemental figure 1. Univariate (χ2) analysis of the ‘reluctance-reluctance’ attitude of older adults towards purchasing institutionalised elderly care services (****p<0.0001, ***p<0.001, **p<0.01, *p<0.05) online supplemental figure 2. Results of regression analysis of ‘reluctance – willingness’ of older adults to purchase institutional care services online supplemental figure 3. Results of regression analysis of the ‘reluctance-hesitation’ attitude of older adults in purchasing institutionalised elderly care services online supplemental figure 4. Results of regression analysis of ‘hesitant-willing’ attitude of older adults towards purchasing institutionalised elderly care services. AIC, Acceptance of institution care.
Supplemental material
Current situation of elderly people’s willingness to purchase institutional care services
The basic characteristics of the 4123 respondents are shown in table 1. Of the 4123 respondents, roughly equal numbers had negative and positive attitudes towards purchasing institutional care (1125, 27.3% vs 1079, 26.2%, respectively), and 1919 (46.5%) had hesitant attitudes. The results of the one-way analysis of the purchase of institutionalised elderly care services by elderly people showed that in the ‘unwillingness-willingness’ model, there were significant differences in the willingness to participate in institutionalised elderly care services among elderly people with different places of residence, highest educational level, marital status, age, number of children and siblings, occupation, per capita monthly household income, indebtedness, medical insurance participation, property, health status and health literacy factors, as shown in Figure 3 (online supplemental figure 1). Further analysis of the results of the “reluctance-hesitation” and “hesitation-willingness” models revealed that other factors also affected the willingness of elderly people to purchase institutionalised elderly care services and that there were significant differences in the willingness to purchase institutionalised elderly care services among elderly people with different levels of social support and anxiety, as shown in table 2.
Basic characteristics of the respondents
One-way (χ2 test) analysis of elderly people’s willingness to purchase institutionalised elderly care services
Influential factors related to the willingness of elderly people to purchase institutional care services
Variables with significant differences in the univariate analysis were further substituted into the three multivariate logistic regression models of older adults’ willingness to purchase institutionalised senior care services.
The results of the analysis of model 1 (reluctance-willingness) showed that the sociodemographic factors of medical participation (β=−0.555), one child (β=−0.771) or more than two children (β=−0.854), two or more siblings (β=−0.323), and one (β=−0.517) or two or more chronic diseases (β=−0.845) were related to elderly people’s unwillingness to purchase institutional care services. The willingness to purchase institutionalised elderly care services was greater among elderly individuals whose per capita monthly household income was ¥2000–4000 (β=0.349) or ¥4000 or more (β=0.554) than among those whose per capita monthly household income was <¥2000, as shown in figure 4 (online supplemental figure 2).
The results of the analysis of model 2 (reluctance-hesitation) showed that elderly people who had one child (β=−0.522), two or more siblings (β=−0.526), two or more chronic diseases (β=−0.343) or a higher level of social support (β=−0.452) were reluctant to purchase institutionalised elderly care services. In contrast, older adults with a per capita monthly household income of ¥2000–4000 (β=0.296) or more than ¥4000 (β=0.357), a high level of health literacy (β=0.464), or mild anxiety (β=0.238) had a hesitant attitude towards purchasing institutionalised senior care services, as shown in figure 5 (online supplemental figure 3).
The results of the analysis of model 3 (hesitation-willingness) showed that older adults who were medically insured (β=−0.517), had one sibling (β=−0.309) and suffered from one (β=−0.397) or two or more chronic illnesses (β=−0.505) were hesitant to purchase institutionalised senior care. In contrast, willingness to purchase institutional care services was generally greater among older adults with higher levels of health literacy (β=0.189) and higher levels of social support (β=0.482), as shown in figure 6 (online supplemental figure 4).
Discussion
This study examined the willingness of older Chinese adults to purchase institutionalised elderly care services and the factors that influence this willingness. Our study revealed that 26.2% of mainland Chinese older adults were willing to choose institutionalised elderly care services, 46.5% were hesitant to do so and 27.3% were clearly unwilling to choose institutionalised elderly care services. Various factors may influence the purchase of institutional care services by elderly individuals.
In model 1, we analysed the factors that influence the reluctance/willingness of elderly people to participate in elderly services. The first factor that was found to influence the willingness of elderly people to purchase institutionalised care is their healthcare participation. Our investigative study showed that older adults without health insurance were generally more willing to purchase institutionalised senior care services than were younger adults without health insurance, which is consistent with the findings of Chengcheng Gao and other scholars.23 A possible explanation is that because this group of older persons is not covered by health insurance, they would consider purchasing institutionalised elderly care services as security for their old age. Another possible reason is that as China’s per capita GDP increases annually,24 the disposable income of elderly people has also greatly increased, which may lead to an increase in the willingness of elderly people to purchase institutionalised elderly care services. In addition, there may be other reasons for the effect of health insurance participation on the willingness of elderly people to purchase institutionalised senior care services, which need to be further explored in future studies. Second, our study showed that the number of children was a key factor influencing the willingness of elderly people to purchase institutional care. The willingness to purchase institutional care services was weaker among older adults with more children. Similar phenomena have been reported in studies conducted in countries such as China and Turkey.25–27 This finding suggests that children are an important resource for elderly people in their old age and that taking turns taking care of elderly adults is still the mainstream concept of old age in society. However, with the development of society and economy, the young generation is currently facing the double pressure of career and family28; thus, whether the traditional concept of old age can succeed requires further research. Third, the willingness of older people with siblings to participate in institutionalised care was generally lower, suggesting that siblings can care for older siblings and accompany each other in their lives. Finally, our study revealed that economic conditions had a major influence on the willingness of elderly people to purchase institutional care. In China, the better the economic conditions of elderly people are, the greater their willingness to participate in institutionalised elderly care is. This indicates that economically affluent elderly individuals lay the material foundation for purchasing institutionalised elderly care services. However, in Japan, which is also in the Asian Cultural Circle, the results of related research are the opposite; that is, an increase in income of elderly Japanese people improves their ability to perform daily life activities, which reduces their willingness to purchase institutionalised elderly care services.29 Therefore, the influence of economic conditions on the willingness of elderly people to purchase institutionalised elderly care services should be further analysed in depth with respect to sociocultural factors.
In model 2, we analysed the factors that influence older people’s reluctance/hesitation to purchase institutional care services. Combined with the results of the analysis in model 1, our investigation revealed that economic factors not only affected the willingness of elderly people to purchase institutionalised elderly care services but were also related to anxiety. Similar issues have been found in related studies conducted in Australia.30 The transition of older adults from home care to institutional care is a stressful life experience that is prone to anxiety. Our study agrees with the view that elderly people are prone to insecurity, fear of separation from their families and greater difficulty in adapting to changes in their living environment, which leads to hesitancy to participate in institutionalised aged care services.
In model 3, we further found that social support and health literacy led to a shift in attitudes from hesitation to willingness to purchase institutional care. Older adults with higher levels of social support generally had a greater willingness to purchase institutional care services. Similar ideas have been validated in a series of studies conducted in East Asian countries.31 32 Previous research has demonstrated that older adults with higher health literacy have a greater utilisation of health services.33 In conjunction with the results of this study, we found that health literacy also played a key role in changing the willingness of older adults to purchase institutional care. This indicates the need to strengthen the health literacy of elderly people through health education to increase their willingness to participate in institutionalised elderly services.
In addition, the role of health status in the purchase of institutional care by elderly people is an issue that should be explored in depth. Our research suggests that older people in poorer health generally have a lower willingness to purchase institutionalised elderly care services. This may be because, based on the rates charged by institutionalised elderly care services, the poorer the health of an older person is, the greater the corresponding level of care is and the greater the related fees are.34 The high cost of expenses may have led to a significant reduction in the willingness of elderly people to purchase institutional care services. In addition, when older adults are in poor health, they prefer their relatives to be by their side,27 which further reduces their willingness to purchase institutionalised elderly care services.
Limitations
This study has several limitations. First, the factors that influence the purchase of institutional care services by elderly people are varied; thus, it was difficult to include all the possible influences in this study. Second, this was a cross-sectional study in which only the phenomenon was analysed; an in-depth explanation of the reasons behind the phenomenon requires the design of a rigorous mixed qualitative and quantitative study. Third, China is a multiethnic country with Han Chinese individuals as the main ethnic group, and the vast majority of the research samples in this study came from areas inhabited by Han Chinese individuals. However, further in-depth research is needed to determine the factors that influence the purchase of institutionalised elderly care by elderly people in areas inhabited by ethnic minorities.
Conclusions
The number of children, number of siblings, per capita monthly household income, medical insurance participation, health status, health literacy status and social support were found to be the main factors influencing the purchase of institutionalised care by elderly individuals. China’s social institutions for elderly people need to not only continue to improve their capacity and quality of service but also provide diversified, multilevel institutional care for elderly people to respond more actively and effectively to the problem of population ageing in Chinese society.
Data availability statement
Data may be obtained from a third party and are not publicly available.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Ethics Research Committee of the Shaanxi Institute of International Trade and Commerce (JKWH-2022-02). Informed consent was obtained from all subjects who participated in the study. All data were collected anonymously and kept confidential. Participants gave informed consent to participate in the study before taking part.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors RZ, WH, LW, CZ, XG, DL and FW designed the study. RZ and WH conducted the data analysis. RZ wrote the manuscript. RZ, WH, LW, CZ, XG, DL and FW proofed the final manuscript. FW is responsible for the overall content as guarantor.
Funding This study was supported by funding from the Anhui Province Philosophy and Social Science Planning Project (Grant no. AHSKY2021D24) and Humanities and Social Science Major Research Project of Department of Education of Anhui Province (Grant no. 2023AH040283).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.