Article Text

Abstract
Introduction The only treatment for non-resectable colorectal liver metastasis (CRLM) is medical therapy, and the overall survival (OS) rate at 3 and 5 years is approximately 30%–40% and less than 10%, respectively. In 2020, a group in Norway reported that liver transplantation for non-resectable CRLM improved the 5-year OS rate to up to 83%. Clinical trials have been launched since that report was published, but most have involved deceased-donor liver transplantation rather than living-donor liver transplantation. Our study will assess the efficacy and safety of living-donor liver transplantation for patients with non-resectable CRLM.
Methods and analysis This is an investigator-driven, multicentre, prospective, single-arm study involving 11 university hospitals in Japan. Patients with non-resectable CRLM and resected primary cancers will be enrolled in the study. Any patients with histopathological or genetic mutations, such as those of RAS and BRAF, are eligible. Furthermore, patients who underwent lung treatment for three or fewer pulmonary metastases and experienced no recurrence for more than 6 months are eligible. The eligibility of the candidates will be reviewed by the Central Eligibility Review Committee. The primary endpoint is the 3-year OS rate. Assuming an OS rate of 70% and a threshold of 45%, the number of required patients is 23, with an alpha error of 5% (one-sided), power of 80% and a 10% dropout rate.
Ethics and dissemination Ethical approval was obtained from the ethical review board of Kyoto University (R-1591). All participants are required to provide written informed consent. The results will be submitted for publication in a peer-reviewed journal.
Trial registration number jRCT1050230053 and UMIN000049785.
- TRANSPLANT SURGERY
- Hepatobiliary tumours
- Gastrointestinal tumours
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study was designed for living-donor transplantation, but not for deceased-donor liver transplantations; therefore, the volume of graft is small and donor safety must be considered.
Genetic mutations and a history of pulmonary metastasis are not exclusion criteria if the patient experienced three or fewer metastasis and if more than 6 months have passed since metastasis treatment; compared to those of similar trials, the selection criteria are relatively broad.
This is a multicentre, single-arm trial that does not have a control arm.
The sample size of the study is small.
Introduction
The morbidity from colorectal cancer is increasing worldwide. At the time of diagnosis of colorectal cancer, 20% of patients have metastasis, and the liver is the organ most frequently affected by metastasis.1 The management of colorectal liver metastases (CRLM) is important to improving the prognosis of patients with colorectal cancer. Liver resection is a potentially curative treatment for CRLM, and the 5-year survival rate after hepatic resection is reportedly more than 50%.2 However, only 10%–20% of cases are considered as ‘resectable’ at the time of the primary diagnosis,3 and most cases are considered ‘non-resectable’ because they involve distant metastases to multiple organs (lungs, peritoneal, lymph nodes, etc.) in addition to the liver. Some patients only have metastases to the liver. If patients are at risk for posthepatectomy liver failure (PHLF) because of an insufficient remnant liver volume, then these patients are considered to have non-resectable diseases. When normal liver function is present, up to 70% of the liver volume can be resected. However, if this resected volume is exceeded, then the risk of PHLF is significantly high. An example of a case in which the remnant liver function may not be sufficient to overcome surgical invasion is one that involves multiple liver metastases that have disseminated to both lobes or a tumour that has invaded the major vessels, thus making it difficult to maintain blood flow to the remaining liver.
The liver is also considered non-resectable when liver insufficiency is a concern because of inadequate residual liver function caused by liver dysfunction. Standard medical therapy for colorectal cancer includes oxaliplatin and irinotecan. However, oxaliplatin causes sinusoidal obstruction syndrome and irinotecan causes fatty hepatitis. Both of these conditions are characteristic of drug-induced liver injury and may result in irreversible liver dysfunction. Additionally, the initial cause of liver dysfunction in some patients may cause other conditions, such as non-alcoholic steatohepatitis or infection with hepatitis virus infection, before the development of colorectal cancer. Hepatic resection for such cases is associated with high risk of PHLF. These cases are considered non-resectable, even if the liver metastasis is technically resectable.
Currently, for patients diagnosed with tumours that are non-resectable because of the risk of PHLF, conversion therapy can be considered if the tumour size is reduced by systemic medical therapy and hepatic resection can be performed if the tumour becomes resectable.4 Clinical trials of non-resectable CRLM have reported that 33% of cases remain unresectable after medical therapy.5 Additionally, continuing medical therapy may seem difficult for patients diagnosed with non-resectable disease.
For patients who are at risk for PHLF and liver insufficiency and have been diagnosed with non-resectable tumours confined to the liver, orthotopic liver transplantation may be a curative treatment. Liver transplantation for patients with non-resectable CRLM has been reported by a study performed in Norway that involved the largest number of cases to date. Furthermore, a study published in 2013 reported a 5-year survival rate of approximately 60% after liver transplantation for localised liver metastases.6 Based on these results, the indication criteria were revised. Another study published in 2020 reported that the 5-year survival rate improved to 83%.7 Although the 5-year recurrence-free survival rate was low (35%), the overall survival (OS) rate was 83%. This is because most recurrent cases involve pulmonary metastases, and therapeutic intervention is usually possible. In contrast, the prognosis of patients with unresectable liver metastasis treated with medical therapy has a 3-year OS rate of 20%–50%, and a 5-year OS rate less than 10%.5 8 9 Therefore, even patients with stage IV disease can be expected to have a good prognosis if liver transplantation is performed under appropriate patient selection conditions. Although clinical trials of liver transplantation for non-resectable liver metastases are currently underway in many countries worldwide, the consensus guidelines for liver metastases attributed to unresectable colorectal cancer were published in September 2021 by the International Hepato-Pancreato-Biliary Association in September 2021.10
Method and analysis
This protocol is reported following the SPIRIT reporting guidelines.11
Study design and objective
This open-label, multicentre (11 university hospitals in Japan), single-arm clinical trial will enrol patients diagnosed with non-resectable CRLM and a living donor for a liver transplantation to explore the efficacy and safety of living-donor liver transplantation for the treatment of non-resectable CRLM. This study will involve 11 institutions in Japan (Hokkaido University Hospital, Tohoku University Hospital, University of Tokyo Hospital, Keio University Hospital, Nagoya University Hospital, Kyoto University Hospital, Okayama University Hospital, Ehime University Hospital, Kyushu University Hospital, Nagasaki University Hospital and Kumamoto University Hospital) and will be led by Kyoto University Hospital. The principal investigator is E. Hatano, MD, PhD, of Kyoto University.
In addition to the aforementioned institutions that perform liver transplantation, supporting institutions will play a role in actively recruiting candidate patients.
Eligibility criteria
The patient selection flowchart is shown in figure 1.

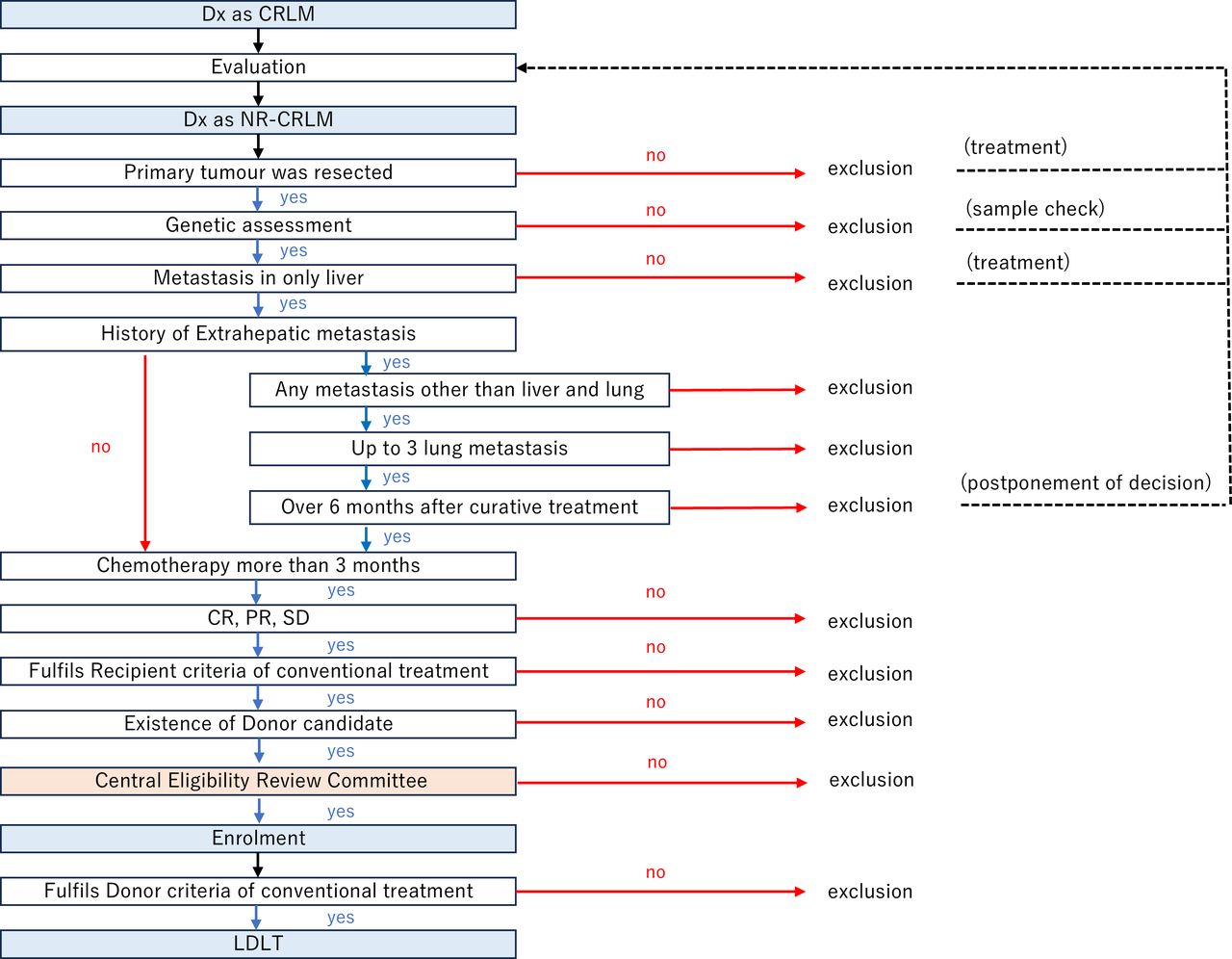{kind=link}
Patient selection flowchart. CR, complete response; CRLM, colorectal liver metastasis; Dx, diagnosis; LDLT, living-donor liver transplantation; NR-CLRM, non-resectable colorectal liver metastasis; PR, partial response; SD, stable disease.
The inclusion criteria are as follows:
Eligibility criteria for the disease
Histological evidence of colorectal adenocarcinoma.
Genetic examination for RAS, BRAFV600E, MSI and mismatch repair gene.
Curative resection of primary colorectal cancer.
Liver metastases from colorectal cancer were diagnosed as surgically non-resectable, including those after repeated hepatectomies. Non-resectable cases are associated with the risk of PHLF because of insufficient remnant liver volume or function.
‘Non-resectable’ refers to the following cases (1) and (2):
Cases involving the concern of liver failure because of the anatomical inability to secure a sufficient volume of the remaining liver.
Cases in which the residual liver volume does not allow a total liver volume of approximately 30% after resection and those in which tumour invasion of the major vessels makes it difficult to maintain blood flow to the residual liver.
Causing concern regarding liver failure because of inadequate function of the residual liver caused by liver dysfunction.
When the multiplication of disappearance rate of indocyanine green (K-ICG) value of the residual liver is less than 0.05 in the indocyanine green (ICG) test.
Based on the diagnosis determined by imaging, the metastatic lesion was present only in the liver. Diagnostic imaging modalities include contrast-enhanced CT, MRI and fluorodeoxyglucose-positron emission tomography.
No history of distant metastases, except in the liver. However, patients with no more than three lung metastases without recurrence for more than 6 months after treatment are eligible as exceptions.
Medical therapy was administered more than 3 months before enrolment.
At least 18 years of age and provided written consent to participate in this study.
Conventional eligibility criteria for living-donor liver transplantation
Age is 18 years or older but younger than 70 years of age.
Performance status score of 0 or 1
The following values of the main organ function are maintained:
Neutrophil count: ≥ 1.5 x 109/L
Platelet count: ≥ 30 x 109/L
Haemoglobin: ≥ 75 g/L
Serum creatinine level: ≤1.5 mg/dL
New York Heart Association cardiac function class II or lower.
Hugh-Jones respiratory function classification II or lower.
The exclusion criteria are as follows:
Progressive disease was diagnosed after medical therapy and an evaluation using RESIST V.1.1. was performed
Presence of an infectious disease that requires treatment.
Pregnancy
Psychiatric disorder or psychiatric symptoms that interfere with daily life and create difficulty with participation in this study
Other cases are considered not eligible for living-donor liver transplantation at each participating institution.
Central eligibility review committee
The central eligibility review committee consists of eight multidisciplinary, six permanent and two non-permanent members. The six permanent members include an expert liver transplant surgeon from a non-participating institute, three expert hepato-biliary-pancreatic surgeons from institutes that do not perform transplantation, a colorectal surgeon and an oncologist. Regarding the two non-permanent members, one is a coresearch investigator of the 11 collaborative institutes who is not involved in recruiting candidates, and the other is an expert surgeon or oncologist who is not affiliated with the collaborative institutes. This committee will discuss eligibility based on the candidate’s medical history, imaging data and other characteristics.
Data and safety monitoring committee
These five members of the data and safety monitoring committee are an expert hepato-biliary–pancreatic surgeon, a transplant surgeon, a hepatologist, the chief of the patient safety unit and a biological statistician. All are independent of the principal investigator and not directly involved in this trial. This committee will meet after every five transplantations or every 6 months. If the committee raises concerns about the conduct of this study, then discontinuation may be recommended.
Criteria for discontinuing the study
This study will be discontinued if the postoperative mortality rate within 60 days is clearly higher than that of living-donor liver transplantation for other diseases. The perioperative mortality rate of living-donor liver transplantation is reportedly 8.4% in Japan12 and 13% in other countries.13 During this study, 23 liver transplantations will be performed. Therefore, if two deaths occur within 60 days after transplantation, then the mortality rate will be 8.7%, which is considered equivalent to that of the conventional living-donor liver transplantation described above. A maximum of three deaths will be tolerated. If the number of deaths reaches four within 60 days (mortality rate of 17.4%), then the principal investigator may decide to discontinue the study because the mortality rate would be higher than that for conventional living-donor liver transplantation. The enrolled participants will be notified if the study is discontinued. The Efficacy and Safety Evaluation Committee will meet after the performance of every five living-donor liver transplantations is performed for non-resectable CRLM or every 6 months to review the progress of the study and safety information. The committee may recommend the discontinuation of the study if concerns are raised regarding its performance.
Endpoints
The primary endpoint is the 3-year OS rate.
The secondary endpoints are as follows:
Short-term (from living donor liver transplantation to discharge from hospital) outcomes of living donor liver transplantation.
Operative time, blood loss, perioperative complications (type, severity, treatment details, date of occurrence and outcomes) and in-hospital mortality rates.
Short-term (within 90 days of living donor liver transplantation) results of living donor liver transplantation
Survival rate at 30 days and 90 days after transplantation.
Tumour recurrence rate, type of recurrence and type of treatment for the recurrence tumour
Adverse events other than tumour recurrence after transplantation
The 2-year and 3-year recurrence-free survival rates and graft survival rates after transplantation.
Trial duration and schedule
This trial will be performed between 15 September 2023 and 14 September 2032 (9 years). Patient recruitment will be performed over the course of 5 years. The duration of observation will be 3 years. The statistical analysis duration will be 1 year.
Intervention
Living donor liver transplantation will be performed according to the usual transplantation procedure at each institution. After transplantation, adjuvant therapy will not be performed until colorectal cancer recurrence is observed.
Participant timeline
Table 1 and table 2 list the time points when efficacy and safety will be assessed using laboratory tests (haematology, coagulation, chemistry and tumour markers), physical examinations and other evaluations. Blood test results, imaging results and complications will be examined every 4 weeks during the first 6 months postoperatively. During 6 months to 2 years postoperatively, these factors will be examined every 6 weeks. During 2–3 years postoperatively, these factors will be examined every 8 weeks.
Examination agenda (before transplantation and during hospitalisation)
Examination agenda (outpatient)
Data collection and management
All patient data will be collected using an electronic data capture system established at Kyoto University.
All study data will be confidential and maintained uniformly using the electronic data capture system for 10 years after the end of the trial. Original copies of the signed informed consent forms will be stored at each institute.
Sample size calculation and statistical analysis methods
The expected 3-year OS rate of patients who undergo transplantation is 70%, which is reasonable based on the report from the SECA-I study. The expected 3-year OS rate of patients who do not undergo transplantation is 45%. Therefore, assuming an OS rate of 70% and a threshold of 45%, the number of required patients was calculated as 21, with an alpha error of 5% (one-sided) and a power of 80%. After considering the small number of patients excluded from the analysis, the target number was set to 23.
The primary outcome (3-year survival) will be estimated using the Kaplan–Meier method, and a two-sided 90% confidence interval (corresponding to a one-sided 5% alpha error) will be calculated using the Greenwood method. The efficacy of the treatment will be confirmed when the calculated lower CI exceeds a threshold of 45%.
Regarding the secondary outcomes, short-term outcomes will be analysed based on the statistical description of the items, and an exploratory study will be conducted to determine which patient characteristics influence these parameters. The post-transplant tumour recurrence rate, form of recurrence and post-recurrence treatment will be described in contingency tables as the number and percentage of cases. Adverse events other than tumour recurrence will be described.
Regarding the 2-year and 3-year recurrence-free survival rates and 2-year and 3-year graft survival rates after transplantation, the Kaplan–Meier method will be used to estimate the cumulative incidence of progression-free survival of the transplantation group. Because the number of patients in this study will be small, supplementation will not be performed for missing values. Additionally, an interim analysis will not be conducted during this study.
Patient and public involvement
None.
Ethics and dissemination
This study protocol was approved by the ethics committee of Kyoto University (C1591) in December 2022, and the Ministry of Health, Labour and Welfare of the government. This study will be conducted in compliance with the principles of the Declaration of Helsinki. The results of this trial will be published in peer-reviewed journals and presented at international conferences.
An investigator at each institution will explain the treatment and anticipated clinical course of this study to the research participants. The explanation will include the fact that the liver transplant will come from a living donor. After explaining the donor risks and costs, we will select patients who are willing to undergo this treatment and for whom a living donor is available. The research participants will be fully informed orally and in writing using an explanation document approved by the Ethics Committee (online supplemental files 1a,b). Written informed consent will be obtained from all participants. The study will be covered by clinical research insurance. If the requirements are met, then compensation payment will be provided by the insurance in the event of postoperative health problems. If the protocol is revised, then this information will be shared with the coresearchers as soon as possible. The results of the trial will be submitted for publication in a peer-reviewed journal.
Supplemental material
Supplemental material
Discussion
Although several protocols for liver transplantation have been created for patients with non-resectable colorectal cancer worldwide, the protocol presented here has some distinctive features. First, this study was designed to include living donor liver transplantation, not deceased donor liver transplantation. Because of the small number of deceased donors in Japan, most liver transplantations have been performed with living donors. Although living donor liver transplantation has the disadvantage of a smaller liver graft, it also has advantages such as a shorter cold ischaemic time. The findings of this study will be different from those obtained during studies involving deceased donor liver transplantation. Second, the handling of the history of pulmonary metastasis during this study will be different from that of other studies. Patients with a history of three or fewer pulmonary metastases and no recurrence for more than 6 months after treatment will be included in this study. Many studies have suggested that the resection of a small number of pulmonary metastases from colorectal cancer can prolong survival.14–16 Furthermore, it has been reported that even if pulmonary metastases appear after liver transplantation, the prognosis is not poor if these metastases are treated.7 Therefore, our protocol does not exclude all patients with pulmonary metastases. However, patients who have experienced more than three pulmonary metastases and recurrence within 6 months will not be included. Third, the handling of the histopathology and genetic statuses of patients will be different from that of oither studies. Consensus guidelines published by the International Hepato-Pancreato-Biliary Association suggest that some types of histopathology and genetic statuses, such as signet ring cell carcinoma or the BRAFV600E mutation, should be excluded from trials because the prognosis for these patients is considered poor. Regardless of the histopathology or genetic status, a good prognosis may be expected if medical therapy is effective. Additionally, Gagniere et al reported that metastases of colorectal cancer with the BRAFV600E mutation tend to be confined to the liver.17 Therefore, liver transplantation may be suitable for improving the prognosis when metastases are confined to the liver and medical therapy is effective. Among ongoing trials, this trial has some of the most challenging eligibility criteria. Furthermore, this trial will explore novel criteria for liver transplantation for patients with non-resectable CRLM. Fourth, this study is a multicentre, single-arm trial without a control arm. Furthermore, the sample size of this study is small (23 patients). Future clinical trials should be designed based on the result of this study.
Trial status
This trial has been registered in the UNIN-CTR (registration number: 000049785) and iRCT (registration number: 1050230053). Participant recruitment is ongoing. The protocol version number is 5.3.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors KF drafted the manuscript and developed the study design and methodology. SK, TIt, NO, SO, TA, KN, YU and TIs designed the study and developed the methodology. EH developed the original concept and study design, edited the manuscript and applied for funding. All authors have read and approved the final version of the manuscript. EH is the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.