Article Text

Abstract
Background Comfort is a primary goal of healthcare. Theory-informed interventions and measurement are essential for comfort enhancement.
Objectives To categorise and synthesise the international literature on the application of Kolcaba’s Comfort Theory in research and practice aiming to promote adults’ comfort.
Eligibility criteria Papers reporting the application of Kolcaba’s Comfort Theory on adult participants published in English and Chinese.
Sources of evidence MEDLINE, CINAHL, APA PsycInfo, Embase, AMED, Web of Science, Scopus, The Cochrane Library, JBI EBP Database, CNKI, Wan Fang; grey literature of Google Scholar, Baidu Scholar and The Comfort Line were searched from January 1991 to January 2024.
Chart methods Following the Joanna Briggs Institute guidance and Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews checklist, two reviewers selected papers and extracted data independently using a standardised chart embedded in NVivo software. A thematic synthesis and a descriptive analysis were provided.
Results The review included 359 papers. Approximately two-thirds (n=216, 60.2%) had been published since 2017. The majority of papers (n=316, 88.0%) originated from China, the USA, Turkey, Brazil and Portugal. The use of Kolcaba’s Comfort Theory was dominated in a range of hospital settings (n=263) and with participants suffering neoplasms (n=55). Seven categories of theory application were identified: (I) interventions underpinned by Comfort Theory as the theoretical framework, (II) interventions evaluated by instruments derived from Comfort Theory, (III) descriptive or observational studies of services or practices underpinned by Comfort Theory, (IV) surveys using questionnaires derived from Comfort Theory, (V) questionnaires development or adaption based on Comfort Theory, (VI) qualitative studies interpreted by Comfort Theory and (VII) literature reviews and discussion about Comfort Theory use. The most commonly evaluated interventions included music therapy (n=31), position intervention (n=20) and massage (n=19), and the most commonly used questionnaire was General Comfort Questionnaire (n=109).
Conclusions Kolcaba’s Comfort Theory has been largely used in interventions and assessments across a wide range of contexts, providing a set of options for practitioners. However, quantifying evidence is needed through further systematic reviews, and continuous development of Comfort Theory is warranted based on the categorisation by this review.
- Adult palliative care
- Pain Management
- Systematic Review
- Complementary Medicine
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The robust methodology of Joanna Briggs Institute scoping review was employed appropriately.
The literature search and selection were highly comprehensive and systematic.
Three hundred fifty-nine papers were synthesised thematically.
The broad scope of review undermined an in-depth analysis.
Bias was introduced by not including publications in other languages.
Introduction
Comfort is a universal concept understood across different disciplines and cultures.1 In healthcare, comfort is central to patients’ experience and serves as a primary goal of practice. Enhanced comfort is a positive, affirmative and desired health outcome.2–4 Historically, several nursing theorists have defined or discussed comfort in their theory such as Florence Nightingale’s environment theory5 and Janice Morse’s theory of comfort.6 7 Comfort was theoretically defined and operationalised in the concept analysis published in 19918 9 on which the Comfort Theory was developed by American nursing researcher Dr Katherine Kolcaba.8 10 11
According to Kolcaba, comfort is ‘the immediate experience of being strengthened through having the needs for relief, ease or transcendence met in four contexts: physical, psychospiritual, environmental and sociocultural contexts’ (p.14).11 The three types of comfort needs within four contexts form a 12-cell taxonomic structure (TS).8 9 Kolcaba’s Comfort Theory proposes that comfort can be enhanced by three types of comfort measures: technical comfort measures, coaching and comfort food for the soul.2 12 Kolcaba developed General Comfort Questionnaire (GCQ) based on the TS to measure people’ comfort level.13
Existing reviews show that Kolcaba’s Comfort Theory is most widely applied among the different theorists14–16 and is most frequently described its use in guiding practice.17 However, evidence on how to use the Comfort Theory in guiding research and practice remains limited. A systematic examination and synthesis of Comfort Theory application is needed. First, expanding the use of Kolcaba’s theory from nursing care in gerontology, where it was developed to other contexts or disciplines requires tests and adaptations.9 Second, Kocaba’s Comfort Theory needs to be tested because it was developed through concept analysis drawing on existing concepts and theories, which is an up-bottom deductive process instead of a bottom-up inductive process from qualitative studies.4 8 Third, operationalising the TS constructs in application might be problematic. For example, ease and transcendence could be less practised because they might be less presented by patients before their relief is addressed. Furthermore, the four contexts are intertwined and often inseparable in assessments and interventions.
Comfort assessments and interventions are complex.18 19 Comfort is dynamic, varying, individualised,16 multidimensional,20 with inherent properties of change over a short period of time.21 22 Individuals’ experience of comfort can be influenced by a variety of factors including patients’ personal strategies, the unique role of family, staff actions and behaviours and factors within the clinical environment.20 Nurses reported that they had difficulties to assess the patient to fulfil their comfort needs.23 Comfort care practices are hindered by the lack of theory-informed experimental studies and the difficulty in assessing outcomes.16
A scoping review is needed to produce an evidence base about how this important theory is applied in comfort enhancement practice or research for adults in an international scope. A scoping review can also be helpful precursors to systematic reviews on more focused questions in relation to the theory use.24 The proposed scoping review in this paper differs from the existing reviews by focusing on the studies reporting the application of Comfort Theory by Kolcaba rather than other theorists, and among adults instead of non-adults,25 by employing a more systematic methodology on a broader scope than other reviews.14 15
Objectives
Our scoping review aimed to categorise and synthesise the international literature on the application of Kolcaba’s Comfort Theory in research and practice aiming to promote adults’ comfort. The specific objectives were: (1) to categorise the practice or research applying Comfort Theory based on purpose and study design/methods, (2) to identify the characteristics of Comfort Theory use in interventions, measurement and interpretation of comfort experience and to determine (3) if further systematic reviews are feasible to evaluate the effectiveness of Comfort Theory for guiding comfort practice and research.
Methods
Study design
We conducted this scoping review following the Joanna Briggs Institute (JBI) guidance.26 27 The choice of the JBI framework was underpinned by the consideration that it is an advanced guidance to the collective work by Arksey and O'Malley28 and Levac et al,29 and therefore has the least deficiencies as a methodological framework for scoping reviews.26 27 30 In line with the JBI framework, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) reporting checklist was used for the report of this review.26 31
Search strategy and paper selection
A three-step search was conducted between 25 November 2021 and 10 January 2022, and updated from 13 October 2022 to 17 October 2022. The final update search on seven main databases was conducted between 27 December 2023 and 4 January 2024 after the manuscript was peer reviewed. The first step was an initial limited search on MEDLINE and CINAHL on the following terms: patient comfort, comfort care, comfort intervention, comfort measurement, Comfort Theory, Kolcaba. This initial search was then followed by an analysis of the text words contained in the title and abstract of retrieved relevant papers, and of the index terms used to describe the articles. A second search using all identified keywords and index terms was then undertaken across all included databases: MEDLINE (EBSCOhost), CINAHL (EBSCOhost), APA PsycInfo (EBSCOhost), Embase (Elsevier), AMED (EBSCOhost), Web of Science, Scopus, Cochrane Library, JBI EBP Database, CNKI (China National Knowledge Infrastructure) and Wan Fang. Grey literature was sought from Google Scholar, Baidu Scholar and The Comfort Line. A brief description of each source with rationale for selection is provided in online supplemental table S1. Third, the reference list of papers that were included in the review was scanned for additional papers. We contacted key authors of primary studies or reviews for further information, including Dr Katherine Kolcaba, Dr April Bice and Dr Sebnem Cinar Yucel. One journal reviewer (librarian) also offered four potential records. The full strategies of update search are listed in online supplemental table S2. The review protocol can be accessed on request.
Supplemental material
Supplemental material
Papers written in English and Chinese were included as the research team is proficient in the two languages. The majority of papers published in the widely used international databases are written in English so that the consideration of papers in English allows the most extent of coverage on papers met the inclusion criteria. Databases mainly covering publications in Chinese were searched to scope evidence from the context of China. Papers published from 1991 to present were included as the first publication regarding Kolcaba’s Comfort Theory is in 1991.8 9
Following the search, all identified articles were imported into the software Endnote X9 (Clarivate Analytics, Pennsylvania, USA). After removing duplicates, two reviewers (YZ and CC) initially screened the title and abstract of each paper against the inclusion criteria and excluded those we considered completely irrelevant, respectively. Following the screening of title and abstracts (YZ and CC), the full text of the potentially relevant papers was retrieved and reviewed in detail in software NVivo (QSR International, Massachusetts, USA) by two reviewers (YL, YZ, CC, CY and JG) independently. Any disagreements that arose between the two reviewers at each stage of the study selection process were solved through discussion with the third reviewer (YL) to achieve final consensus.
The results of search and the process of paper selection were documented and presented in a PRISMA-ScR flow diagram with the reasons for exclusion.32 A narrative description was written, aligns with the flow diagram to demonstrate the selection process.
Inclusion and exclusion criteria
Our review included adult participants who aged 18 years and older and who could be patients, their family members and healthcare professionals (HCPs), from any geographic locations and any settings. The broad context was not limited to any particular countries or health systems, while it had to be in healthcare settings where all the activities whose primary purpose was to promote, restore or maintain health.
The review sought any types of papers reporting the application of Comfort Theory developed by Kolcaba, including but not limited to quantitative studies, qualitative studies or mixed methods studies (MMS), literature reviews, meta-analyses or synthesis, guidelines, website reports and grey literature.33 The application could be an intervention to enhance comfort, an instrument to measure comfort level, qualitative interpretations of comfort experience or any other types of application of the Comfort Theory. Our review only considered papers that clearly indicated that Kolcaba’s Comfort Theory was used, with cited recognisable references.
Data extraction
The full text of included papers was imported into the software NVivo (QSR International, Massachusetts, USA) for data extraction. After close reading of each paper, relevant data were coded against the charting form (see online supplemental table S3) by one reviewer (YZ or CC) and then checked for accuracy by a second reviewer (YL or CC). Discrepancies and uncertainties of data extraction were solved through discussions within the review team.
Supplemental material
To ensure a standardised data extraction consistently carried out on each source, data items were defined for this review: (1) study participants included the group or individuals investigated or cared for, social demographic and/or clinical characteristics of the participants and sample size; (2) interventions were defined as the care or measures provided to enhance participants’ comfort; (3) outcomes referred to the variables or items evaluated before and/or after interventions showing the effects of interventions; (4) comfort measurement was the assessment or evaluation of comfort via a specific tool or approach; (5) setting referred to the specific location where the study was conducted such as a unit of hospital or an institution while (6) country of origin referred to which country the study was conducted; (7) any other key information related to the review question and objectives were extracted as ‘other key findings’.
Data synthesis
Following data extraction, codes generated from the included papers were grouped as the following categories or themes: year of publication, country, settings, participants, study design, categories of theory application in research or practice. Years of publication were divided into the last 5 years and years earlier. Countries were clustered according to WHO regions system.34 Settings were grouped into different types of institutions, and those in a hospital were further classified according to the typical hospital wards classification. Participants were categorised into healthy people and patients, and patients were further categorised in accordance with the International Classification of Diseases and Related Health Problems-11.35 The typology of theory application was established based on study design and methodology and the purpose of using Comfort Theory. Synthesised results on year of publication and country distribution were visualised in figures. A descriptive narrative was provided accompanying the tables to demonstrate how the findings related to the review objectives.
Patient and public involvement
None.
Results
The entire PRISMA-ScR flow chart is shown in figure 1. The initial search yielded 16,167 results. Removing duplicates and applying the eligibility criteria resulted in a total of 1,483 articles. At the end of study selection, 359 papers were included in the review, and information about the characteristics of Kolcaba’s Comfort Theory application were properly extracted (see online supplemental table S4). The excluded full texts during update are listed in online supplemental table S5.
Supplemental material
Supplemental material

The Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews flow chart.
Year of publication
The publication year of one document was unknown, and the remaining 358 papers were published between 1992 and 2023 (figure 2). The number of papers published annually increased steadily since 1996 with fluctuations in between. The largest number of publications within a year was 39 in 2017. Approximately two-thirds of the papers (n=216, 60.2%) had been published since 2017.

Number of publications per year (n=358). One included paper’s year of publication was unknown. Each blue bar shows the number of publications (on the top of bar, vertical axis) in a year between 1992 and 2023 (horizontal axis). The dotted curved line is an exponential trendline showing the number of publications rose at increasingly higher rates.
Country of origin
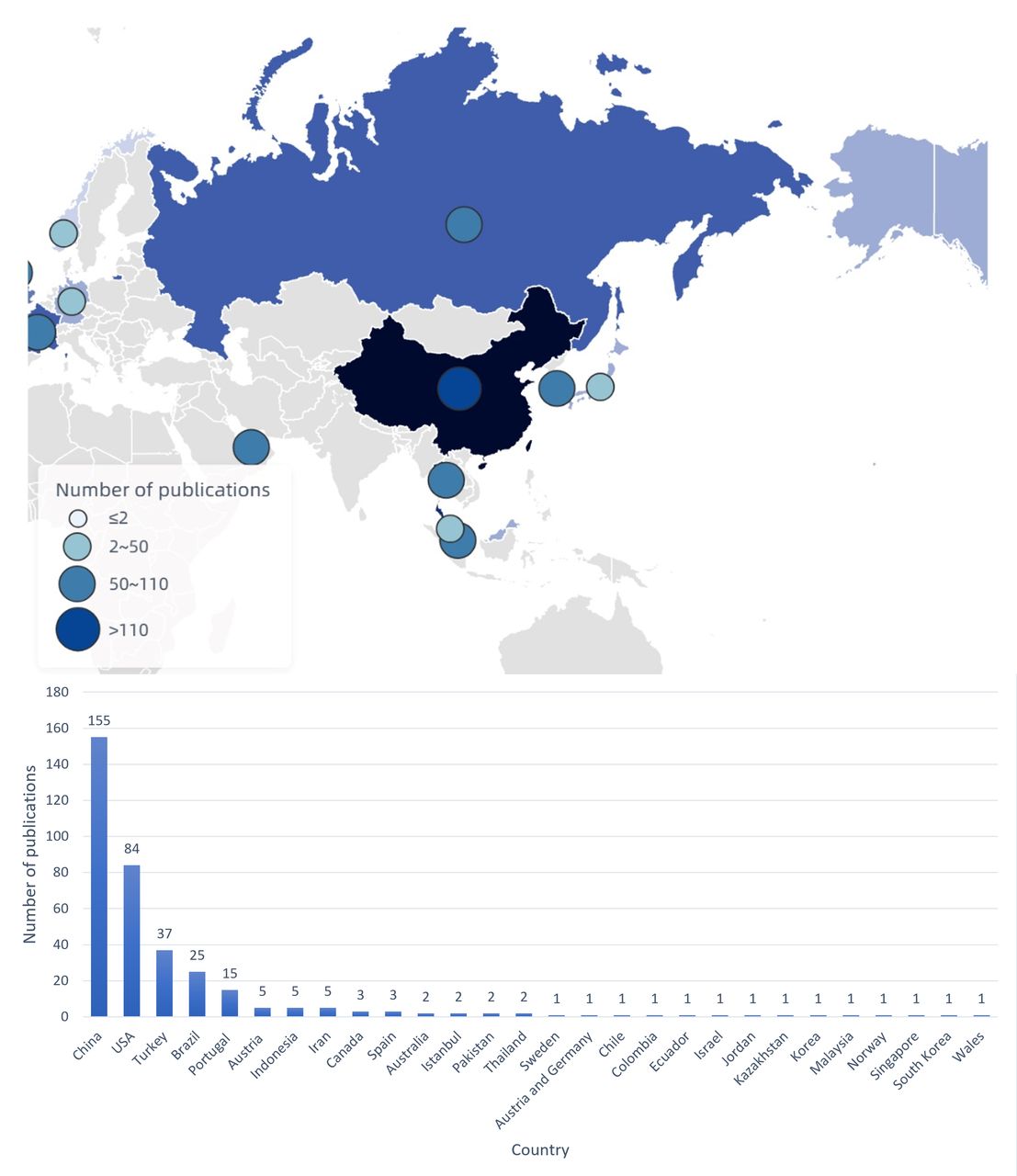
The included 359 papers reported the application of Kolcaba’s Comfort Theory in 28 countries or regions (figure 3) covering Western Pacific (n=161), Americas (n=115), South-East Asia (n=7), Europe (n=68) and Eastern Mediterranean (n=8). Whereas many countries published one or two papers, the majority of papers (n=316, 88.0%) originated from the following five countries: China (n=155), the USA (n=84), Turkey (n=37), Brazil (n=25) and Portugal (n=15).

Number of publications by country (n=359). The blue bar shows the number of publications (vertical axis) in each country (horizontal axis) ranking from high to low, corresponding to the size of bubble summing up the number of publications in different countries within each region on the world map according to WHO regions system.
Settings
As reported in the 359 papers retrieved, the studies or practices applying Kolcaba’s Comfort Theory were carried out largely in hospitals (n=263), followed by a range of settings comprising: nursing home (n=8), university (n=7), hospice or palliative clinic (n=5), online (n=4), community (n=4), home (n=3) and others (n=21). In the documents specifying the setting in hospitals (n=192), Comfort Theory was mainly applied in: surgical ward (n=63), internal unit (n=61), critical care unit (n=22), obstetrics and gynaecologic unit (n=16), outpatient (n=19), operating room (n=6) and emergency (n=5).
Participants
Participants included in the studies or practices applying Comfort Theory were dominated by those with neoplasms (n=55), followed by genitourinary diseases (n=30), circulatory diseases (n=30), pregnancy, childbirth or the puerperium (n=26), surgical or post-surgical status (n=25), healthy people (n=23), digestive diseases (n=19), palliative care patients (n=18), nervous diseases (n=12), musculoskeletal or connective tissue diseases (n=10), respiratory diseases (n=7), mental, behavioural or neurodevelopmental disorders (n=6) and injury, poisoning or certain other consequences of external causes (n=5).
Study design
The included 359 papers adopted a range of study design and methodology with a domination of interventional studies, comprising: randomised controlled trial (RCT) (n=83), quasiexperimental study (n=60), cross-sectional study (CSS, n=52), literature review and discussion (n=47), questionnaire development or adaption (n=34), qualitative study (n=21), longitudinal study (n=16), MMS (n=15), case study/report (n=13), service description (n=10), case-controlled study () (n=6) and cohort study (n=2).
Categories of theory application in research or practice
Based on the study design and/or methods as well as the purpose of using Kolcaba’s Comfort Theory by the 359 papers, theory application was synthesised into seven categories (I–VII), which is presented in table 1 and figure 4. A detailed categorisation with characteristics of each paper in every category is available in online supplemental table S6.
Supplemental material
Seven categories of Kolcaba’s Comfort Theory application in healthcare (n=359)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Number and percentage of papers in seven categories of Comfort Theory application (n=359).
Category I: Interventions underpinned by Comfort Theory as the theoretical framework
Of the 359 papers, 56 (15.6%) reported interventions using Kolcaba’s Comfort Theory as the theoretical framework, including: music therapy (n=13), massage (n=8), health education (n=8), position intervention (n=7), therapeutic touch (n=6), guided imagery (n=6), cold and hot therapy (n=6), aromatherapy (n=5), coaching (n=3), traditional Chinese medicine (TCM) (n=3), progressive muscle relaxation (PMR) (n=2), cognitive strategies (n=2), positive connotation (n=2), pet visit (n=1), silent therapy (n=1), mindfulness (n=1), still point induction (n=1) and Robusta coffee (n=1). Many studies reported positive effects in improving comfort (n=40), pain (n=10), satisfaction (n=9), anxiety (n=8), depression (n=4), stress (n=3), sleep quality (n=3), urine leakage (n=2), quality of life (QoL) (n=1) and well-being (n=1).
Category II: Interventions evaluated by instruments derived from Comfort Theory
The largest number of papers (n=96, 26.7%) reported interventions that did not apply Kolcaba’s Comfort Theory as the theoretical framework but were evaluated using instruments derived from Kolcaba’s Comfort Theory. The common comfort measures evaluated in this group included: TCM (n=13), health education (n=11), music therapy (n=11), position intervention (n=7), massage (n=5), exercise (n=4), cold and hot therapy (n=3), foot reflexology (n=2), PMR (n=2), therapeutic touch (n=2), guided imagery (n=2), shower (n=1), doll intervention (n=1), labour dance (n=1), paradoxical intention therapy (n=1), aromatherapy (n=1), art therapy (n=1) and yoga (n=1). The commonly used questionnaires to measure comfort before and/or after interventions included Chinese version GCQ (n=67), Turkish version GCQ (n=9), Turkish version Paranaesthesia Comfort Questionnaire (n=5), English version GCQ (n=3) and Turkish version Postpartum Comfort Scale (n=3). Many studies reported the intervention had an effective improvement in comfort (n=92), pain (n=31), anxiety (n=20), satisfaction (n=19), length of hospital stay (n=11), constipation (n=7), depression (n=6), QoL (n=5), nausea and vomiting (n=4), sleep quality (n=4), loss of appetite (n=4), swelling (n=3), difficulty urinating (n=3) and costs (n=3).
Category III: Descriptive or observational studies of services or practices underpinned by Comfort Theory
Thirty-four (9.5%) papers reported a description of a specific service or practice applying Kolcaba’s Comfort Theory, and some of which applied the theory at case level (n=4), unit level (n=8) and institution-wide level (n=2). The following comfort measures were reported in this group: music therapy (n=7), position change (n=6), massage (n=6), aromatherapy (n=3) and healing touch (n=2). Comfort (n=9) and comfort related variables were investigated including: pain (n=3), satisfaction (n=3), anxiety (n=2), depression (n=1), QoL (n=1); and symptoms such as sleep quality (n=1), delirium (n=1), nausea and vomiting (n=1).
Online supplemental table S7 lists the comfort interventions and comfort variables across categories I–III. Music therapy (n=31), position intervention (n=20) and massage (n=19) were the most commonly experimented comfort measures. In addition to comfort, pain (n=44), satisfaction (n=31) and anxiety (n=30) were often evaluated as outcomes of comfort interventions.
Supplemental material
Category IV: Surveys using questionnaires derived from Comfort Theory
The second large group was surveys investigating comfort level and associated factors in different populations (n=71, 19.8%). Sociodemographic factors such as education level (n=19), age (n=18) and gender (n=15) were often reported to be influential to comfort. The relationship between comfort and the following variables were examined by the included papers: pain (n=9), satisfaction (n=9), anxiety (n=6), QoL (n=5), depression (n=2), length of hospital stay (n=2), stress (n=1) and perceived nursing caring, social support and emotion-focused coping (n=1). In these surveys, comfort was often measured by Chinese version GCQ (n=25), Turkish version GCQ (n=6) and Childbirth Comfort Questionnaire (n=3).
Category V: Questionnaires development or adaption based on Comfort Theory
There were 34 (9.5%) papers that reported questionnaire development or adaptation for measuring comfort among different groups, with tests of reliability and validity. The questionnaire that was widely translated and adapted was GCQ (n=9), followed by Epilepsy Monitoring Unit Comfort Questionnaire (n=4), Immobilization Comfort Questionnaire (n=2), Radiotherapy Comfort Questionnaire for patients with head and neck neoplasms (n=2) and Holistic Comfort Questionnaire-Family (n=2).
Category VI: Qualitative studies interpreted by Comfort Theory
A small group of papers (n=21, 5.8%) reported a qualitative study understanding comfort experience. The authors of studies in category VI mapped their findings onto the four contexts depicted in Kolcaba’s Comfort Theory: physical comfort (n=14), psychospiritual comfort (n=14), sociocultural comfort (n=13) and environmental comfort (n=9).
Category VII: Literature reviews and discussion about Comfort Theory use
The last group was literature reviews and discussion papers or book chapters (n=47, 13.1%) that summarised the use of Kolcaba’s Comfort Theory mainly surrounding the following topics: comfort care models (n=23), comfort measures (n=14), wide application (n=11), questionnaires (n=10), institution-level application (n=5), best practices (n=5), alternative and complementary therapies (n=4), comfort needs (n=3) and the usefulness of nursing theory (n=2). The commonly discussed care model using Kolaba’s Comfort Theory included: palliative and hospice care (n=9), paranaesthesia nursing (n=5), childbirth care (n=4), cardiac care (n=3), elderly care (n=3), and nursing in critical care (n=1).
Discussion
To our knowledge, this is the first comprehensive review mapping the international literature regarding the application of Kolcaba’s Comfort Theory in healthcare to generate an evidence base for research and practice with an aim to promote adults’ comfort. In addressing the three objectives, our review identified 359 papers reporting seven categories of the Comfort Theory application across different healthcare contexts for comfort enhancement over the past three decades. An overview of each category was provided with amount, scope and characteristics of evidence, on the basis of which our review has identified some pitfalls of the theory application and priorities for further studies.
Our findings show that Kolcaba’s Comfort Theory has been applied in a wide range of contexts, among which the most common context was a patient in a crisis or critical situation like suffering cancer or receiving a surgery. Patients in such crisis have evident and complex comfort needs that HCPs need to assess and deliver interventions to improve comfort. Integrating a crisis concept or construct36 into the Comfort Theory might be a useful step for the continuous development of the theory, specifying the characteristics of high comfort needs.
Within the seven categories of application identified by our review, Kolcaba’s Comfort Theory was often used to inform or evaluate interventional studies (categories I–III). How effective the theory in guiding these interventions requires quantifying effects through further systematic reviews. Furthermore, most of the comfort measures being tested were identified as coaching or ‘comfort food for the soul’ according to the typology by Kolcaba,11 and they are considered important as an ‘expert’ nurse.2 However, because the authors of included studies did not name these measures in Kolcaba’s typology, it was not easy for us to differentiate the two types on some measures, suggesting issues in operationalising the theory.
A second common application type of Kolcaba’s Comfort Theory lied in quantitatively measuring comfort needs and levels, as outcomes of interventions (categories I and II) or for testing relationship between comfort and other variables (ie, pain, satisfaction and anxiety, in category IV). Although a small number of comfort questionnaires were developed and adapted to particular populations (category V), GCQ was largely used across contexts and cultures; such a broad application of scales developed from a middle range theory indicates the need for a further systematic review to evaluate how reliable and valid Kolcaba’s comfort questionnaires were in measuring comfort of different populations internationally.
The category having the smallest number of publications was using Kolcaba’s Comfort Theory for explaining qualitative findings (category VI). The included qualitative studies did not explicitly report revisions or modifications of Kolcaba’s Comfort Theory, but we found that the three types of comfort defined by Kolcaba were less identified in these studies compared with the four contexts. In terms of the contexts, environment was less reported compared with other three. In addition, it was often difficult in our data extraction to differentiate between physical and psychospiritual, as well as between psychospiritual and sociocultural comfort. Our findings suggest operationalisation challenges in validating Kolcaba’s TS constructs in qualitative studies, and a further meta synthesis on the 21 included qualitative studies might be useful.
An increasing interest in applying and developing the theory can be seen from the increasing trend of publications over time and from the hot discussion and reflection on the theory (category VII). However, one major limitation in the Comfort Theory application across the seven categories was not informing and reporting the theory use transparently. Many studies retrieved in our review did not clearly describe how the Comfort Theory was used in guiding their research or practice. Limited information could be extracted on how the theory was adapted in different contexts according to the guidance that when a middle range theory is applied directly into practices in specific context, it needs to be adapted or modified to situation-specific theories.37 38 An informed use of theory that provided the framework for the research and a clear description of theory use to guide practice provide a means by which other studies using the same theory can be used to build the body of scientific knowledge, thus advancing best practices in healthcare.39 More informed use of theory can strengthen improvement programmes and facilitate the evaluation of their effectiveness.40 Explicit descriptions of using theory to guide practice promise a substantive step toward meeting the mandate for making a difference for society through theory guidance.17
Future research
Based on the evidence base generated in our review, more research is needed to further test and explore the effects of Kolcaba’s Comfort Theory in guiding different types of research and practice that aim to promote comfort. The theory needs to be developed and adapted when guiding intervention or practice in specific context. Further quantitative or qualitative systematic reviews can be conducted to answer more focused questions in relation to the effectiveness of theory use in guiding interventions, developing instruments and interpreting qualitative findings. How the theory is used in research and practice need to be more explicit and informed.
Limitations
Our literature search may have introduced selection bias and missed relevant articles by restricting inclusion to studies written in English and Chinese. We excluded literature from non-adult groups, thus limiting the application of results to adults’ healthcare practice. We did not formally assess the quality of included studies, as we respected the scoping review approach, but we took a critical stance in the overall quality of evidence by considering limitations in study design and methodology.
Conclusions
Kolcaba’s Comfort Theory has been used largely in interventions and assessments for a range of participants in hospital settings. A variety of holistic comfort measures and questionnaires have been proposed and tested for adults’ comfort enhancement, offering many options for HCPs, researchers, patients and public members. Our overview of evidence and categorisation of Kolcaba’s Comfort Theory application can serve as the first step in enabling stringency in the field as well as inspire further exploration, and thereby support for the needed growing research interest in comfort care. Nevertheless, there are still several issues that deserve further research by the scientific community in order to match the quality of scientific evidence to the undeniable complexity inherent in comfort theory use in guiding research and practice.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
Approval of IRB exemption for this study was granted by Shanghai Ethics Committee for Clinical Research (approval number: SECCR/2022-111-01) because we conducted a scoping review following the JBI and PRISMA-ScR guideline.
Acknowledgments
We thank Dr Katherine Kolcaba for her comments and suggestions on the scope and purpose of review. We also thank Dr April Bice for her assistant on clarification for some grey literature sources.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
X @Yeelin00
Contributors YL conceptualised the study, drafted the protocol and wrote the manuscript. YZ and CC performed searches, study selection and data extraction, supervised by YL. For update search, YL conducted searches, and YL, CY and JG completed the paper selection and data extraction. YZ formed tables. CC created figures. All authors have read and approved the final manuscript. YL acted as guarantor.
Funding This scoping review was funded by Shanghai University of Traditional Chinese Medicine Budget Projects (2021WK145).
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.