Article Text

Abstract
Objectives We carried out an evaluation of a large-scale New Zealand retrofit programme using administrative data that provided the statistical power to assess the effect of insulation and/or heating retrofits on cardiovascular and respiratory-related mortality in people aged 65 and over with prior respiratory or circulatory hospitalisations.
Design Quasi-experimental cohort study based on administrative data.
Setting New Zealand.
Participants From a larger study cohort of over 900 000 people, we selected two subcohorts: 3287 people who were aged 65 and over and had experienced pretreatment period cardiovascular-related hospitalisation (ICD-10 chapter 9), and 1561 people aged 65 and over who had experienced pretreatment respiratory-related hospitalisation (ICD-10 chapter 10).
Interventions Treatment group individuals lived in a home that received insulation and/or heating retrofits under the Warm Up New Zealand: Heat Smart programme. Control group individuals lived in a home that was matched to a treatment home based on physical characteristics and location.
Primary and secondary outcome measures HR for all-cause mortality for treatment with insulation, heating, or insulation and heating relative to control group.
Results People with pretreatment circulatory hospitalisation who occupied a household that received only insulation had an HR for all-cause mortality of 0.673 (95% CI 0.535 to 0.847) (p<0.001) relative to control group members. Individuals with a pretreatment respiratory hospitalisation who occupied a household that received only an insulation retrofit had an HR for all-cause mortality of 0.830 (95% CI 0.655 to 1.051) (p=0.122) relative to control group members. There was no evidence of an additional benefit from receiving heating.
Conclusions We interpret the hazard rate observed for cardiovascular subcohort individuals who received insulation as evidence of a protective effect, reducing the risk of mortality for vulnerable older adults. There is suggestive evidence of a protective effect of insulation for the respiratory subcohort.
- public health
- health economics
- epidemiology
- housing
- insulation
- evaluation
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
A large cohort allows for the analysis of mortality, a rare event that has previously been difficult to explore in this field.
The study’s quasi-experimental cohort design limits the impact of selection bias.
The cohort is constructed from an administrative data set that does not include individual health data such as smoking status or obesity, making it impossible to explicitly control for such factors.
The data do not include causes of mortality, which limits the strength of the conclusions that can be drawn from results.
Population mobility and the limitations of administrative address data introduce the potential for non-differential misclassification bias towards the null.
Introduction
Recent systematic reviews of associations between housing and health have concluded that there is strong evidence for an association between energy efficiency-related retrofits and a variety of health outcomes including respiratory health.1 2 Randomised controlled trials carried out in New Zealand, which has relatively poor quality housing for a first world nation,3 have linked insulation retrofits with reductions in respiratory symptoms and days off work and school.4 They have also linked retrofitted heating with reductions in wheeze for children with asthma and reduced general practitioner visit rates.5 The hypothesised causal pathways include reductions in exposure to allergens such as mould and dust mite faecal matter due to reduced dampness and reductions in bronchoconstriction resulting from increased indoor temperatures. Patterns of excess winter mortality and morbidity observed in New Zealand driven by cardiovascular and respiratory illnesses are also consistent with the exposure of vulnerable groups to low indoor temperatures.6 7 However, none of these prior New Zealand trials, nor those in other countries, have been of sufficient scale to detect statistically significant impacts of retrofits on rare events such as mortality.
In 2009, responding to the global financial crisis and a growing political consensus regarding the energy efficiency and public health benefits of improving housing stock, the New Zealand government implemented a large-scale intervention that part-funded the retrofitting of private homes with energy efficiency measures. Warm Up New Zealand: Heat Smart (WUNZ: HS) was a multiyear $347 million programme (July 2009–2014) that primarily provided part-funding for floor and ceiling insulation and heating retrofits (primarily heat pumps). Heating retrofits were only available to homes that met minimum floor and ceiling insulation standards, either due to pre-existing insulation or as a result of having also received retrofitted insulation under the programme. A consortium of academics and researchers was commissioned by central government to carry out a cost:benefit evaluation of WUNZ: HS,8 which included two reports on health impacts9 10 and a paper describing energy impacts.11 Health-related findings included statistically significant reductions in household-level hospitalisation costs and pharmaceutical use costs and reductions in hospitalisation rates for children following insulation retrofits.12
This paper presents an analysis of the impact of floor and ceiling insulation retrofits and heating retrofits on mortality risk for two subcohorts: older adults with either a pretreatment cardiovascular hospitalisation (ICD-10 chapter 9) or a respiratory hospitalisation (ICD-10 chapter 10). These groups were identified as being particularly likely to experience reduced mortality after home retrofits. The selection of subcohorts was informed by previous New Zealand studies that identified patterns of excess winter respiratory and circulatory mortality in New Zealand,6 a statistically significant correlation between housing type and winter morbidity,7 and relationships between both low income and tenure status and excess winter mortality.13 The hypothesised causal pathways linking low indoor temperatures and cardiovascular mortality and morbidity include increased blood pressure and increased platelet, fibrinogen, and red and white blood cell counts induced by lower temperatures.7 14 The hypothesised causal pathways linking low indoor temperatures and respiratory mortality and morbidity include higher rates of respiratory illness due to cold-induced inflammation of the respiratory tract, bronchoconstriction, suppressed immune response and increased exposure to micro-organisms that cause respiratory illness due to extended survival time in droplets in colder environments.7 14
Methods
The WUNZ: HS evaluation was a quasi-experimental study made possible by the linking of administrative data sets described in Telfar Barnard et al.15 Use of administrative data sets meant that a very large cohort could be created, giving the evaluation greater statistical power to assess the impact of insulation and heating retrofits on rare events such as hospitalisation and death than previous studies. The cohort building process is briefly summarised below.
Cohort construction
After ethics approval was obtained, the Energy Efficiency and Conservation Authority (EECA) provided address and retrofit data for homes whose owners participated in WUNZ: HS during the first 8 months of the programme. This cut-off reflected the time frame imposed by the commissioned evaluation. The data were forwarded to Quotable Value (QV), a commercial entity with extensive high-quality data on New Zealand housing quality and characteristics. QV identified up to 10 matched control homes where possible, based on our matching protocol which combined location, construction decade, quality, size and a number of other factors relevant to thermal performance. Anonymised health and demographic data for treatment and control dwelling occupants were then obtained from the Ministry of Health (MOH) based on the unique National Health Index (NHI) identifiers linked to each address, producing an initial cohort of nearly one million anonymised individuals. NHI-based linkage of administrative data sets meant that it was possible to obtain demographic and hospitalisation data for cohort individuals. Health service-use data were obtained for the period of January 2008–December 2012, enabling the calculation of pretreatment and post-treatment hospitalisation and pharmaceutical use rates. Data cleaning included removal of implausibly old individuals and implausibly crowded homes, a result of the limitations of the address field of the NHI data set, which reflects the most recent address update for an individual, which typically occurs after contact with a healthcare provider. The final study cohort contained 916 504 individuals from 245 778 households: cohort construction is described fully in Telfar Barnard et al10 and Preval,16 and is summarised in online supplementary appendix 1. The data available for each cohort member are summarised in online supplementary appendix 2.
Supplementary file 1
Supplementary file 2
The two subcohorts constructed for the analyses presented in this paper were further limited to individuals who had experienced a circulatory or respiratory hospitalisation during their pretreatment period and who were alive and aged 65 or over at the time that the home that they occupied first received treatment under WUNZ: HS, or in the case of control group individuals at the time that the treatment group home matched to their home received treatment.
Treatment characteristics
Three retrofit treatment types were analysed. First, insulation only, which indicated that a variety of EECA-specified underfloor and ceiling insulation products were retrofitted so that floor and ceiling insulation met the EECA standards (typically an R value of R 2.9 R4 for ceiling insulation and R 1.4–R 1.8 for underfloor insulation). Although no field data were collected, a New Zealand study of insulation retrofits with similar parameters found that insulation retrofits increased the average indoor bedroom temperatures by approximately 0.5°C, reduced time exposed to temperatures below 10°C by 1.7 hours per day and decreased relative humidity by 2.3%.4
The second treatment type was heating only, which indicated the retrofitting of an energy-efficient heater from an EECA-specified list (the majority of homes chose heat pumps) and was only available to homes with pre-existing underfloor and ceiling insulation that met the EECA standards. A randomised controlled trial of similar heating retrofits with baseline underfloor and ceiling insulation recorded an increased average living room temperature by 1.1°C5
The final treatment type was insulation and heating, which indicated the concurrent retrofitting of both insulation and a heater to the above specifications. It is likely that the temperature and humidity benefits of this treatment type would exceed those gained from either of the other treatment types.
Analysis of mortality data
The models used to analyse the impact of the three treatment types on mortality risk were standard Cox proportional hazards models run using Stata V.13. Despite the similarities of the two subcohorts, modelling attempted to further reduce confounding by considering as potential confounders all available demographic and household-level characteristics. The models included age, gender, ethnicity, pretreatment hospitalisation severity as measured by average annual cost, dwelling quality and climate zone. Continuous variables were transformed using the fractional polynomial approach.17 Biologically plausible interactions with age and sex were considered for inclusion in models. Clustering at the level of matched treatment and control households was adjusted for in calculating SEs. Covariates that were not statistically significant and whose removal did not meaningfully impact the coefficients or CIs of the variables of interest were discarded for reasons of model parsimony.
Mortality data were modelled for the post-treatment period only. This decision was made because including pretreatment period data would be likely to produce misleading estimates, as a death might preclude a household participating in the WUNZ: HS programme but would not impact inclusion in the control group. Mortality calculations were based on the date of death field in the NHI. Cause of death data were not obtained due to concerns about data quality and anonymity.
Results
The circulatory subcohort contained 3287 older adults, 788 who received insulation only, 78 who received heating only, 131 who received both and 2290 control group members. During the follow-up period, 511 subcohort members died. The follow-up period comprised 2 195 452 days total time, with an average follow-up time of 668 days per person (the maximum follow-up period was 883 days). The respiratory subcohort contained 1561 older adults: 401 who received insulation only, 44 who received heating only, 68 who received both and 1048 control group members. During the follow-up period, 379 subcohort members died. The follow-up period comprised 984 895 days total time, with an average follow-up time of 631 days per person.
Comparison of treatment groups with the control group with regard to age distribution, sex distribution, ethnicity, average annual pretreatment period hospitalisation costs, housing characteristics and socioeconomic status measured using New Zealand Deprivation Index scores (an area-based deprivation index derived from census data) did not demonstrate statistically significant differences. Key characteristics of the two subcohorts are presented in table 1, and a complete summary of all characteristics is presented in online supplementary appendix 3 and appendix 4.
Supplementary file 3
Supplementary file 4
Key characteristics of the circulatory and respiratory subcohorts
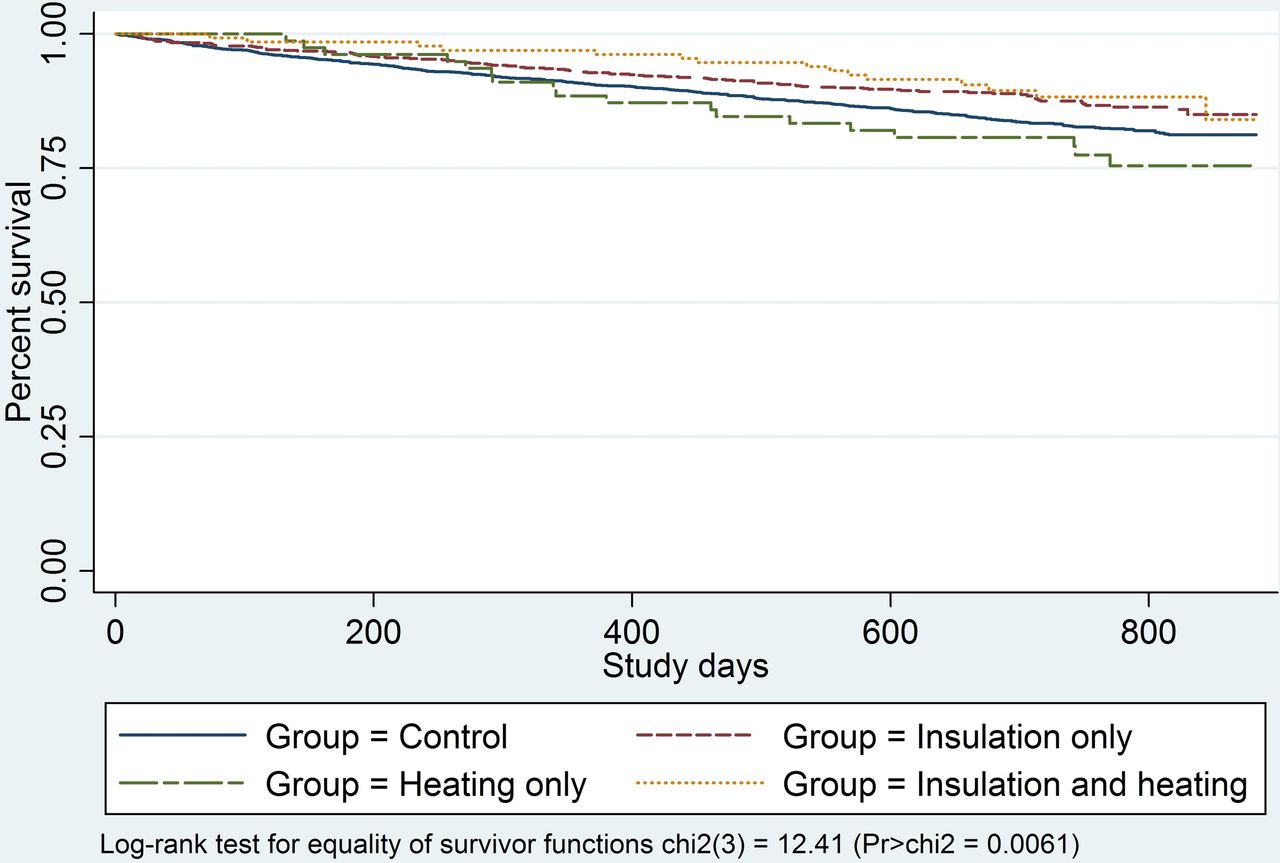
Figure 1 and figure 2 present the Kaplan-Meier survival curves for the two subcohorts. Log-rank tests indicate that there is a statistically significant difference between the survivor functions of the treatment groups for the circulatory subcohort but not for the respiratory subcohort.

Kaplan-Meier survival estimates for the circulatory subcohort.

{kind=link}
{kind=link}
Kaplan-Meier survival estimates for the respiratory subcohort.
Unadjusted HRs (relative to the control group) for the treatment variables of interest for both subcohorts are presented in table 2. The adjusted coefficients are presented in table 3.
Unadjusted Cox proportional hazards model results: circulatory and respiratory subcohorts
Adjusted Cox proportional hazards model results: circulatory and respiratory subcohorts
The adjusted model results indicate that receiving an insulation retrofit had a strongly protective effect for the circulatory subcohort, with a statistically significant HR of 0.673 for the insulation group relative to the control group, interpretable as a 32.7% reduction in mortality risk during the period studied. Individuals in the circulatory subcohort that received both insulation and heating also demonstrated a lower mortality hazard rate, which was indistinguishable from the insulation-only group using the Mann-Whitney test. Results for circulatory subcohort individuals who received heating only did not indicate any statistically meaningful impact. Results for the respiratory subcohort suggested a protective impact of receiving insulation, consistent both for individuals who received insulation only and insulation and heating. Neither result was statistically significant at the p<0.05 level, although the HR for insulation only relative to the control group approached statistical significance at the p<0.1 level (p=0.122). There was no evidence for a statistically significant impact of heating only on mortality hazard for the respiratory subcohort.
Model testing indicated that the HR reported for the insulation-only group in the circulatory subcohort was robust to the influence/exclusion of individuals, although this was not the case for the smaller heating only and insulation and heating groups, which reflected the smaller size of these groups but meant that the beneficial reduction in mortality risk observed for the insulation and heating group may not be robust. The respiratory subcohort did not contain individuals who had excessive influence on the coefficients of the variables of interest.
The underlying proportionality assumption of the models was tested by assessing Schoenfeld residuals for each covariate. Where residuals were large enough to suggest that the proportionality assumption was violated, interaction terms between these covariates and functions of study time were included in the model. Inclusion of these interaction terms in the models did not materially alter the coefficients and CIs of the variables of interest (none of which demonstrated non-proportionality) and thus the terms were not retained for reasons of model parsimony. Model goodness of fit was evaluated using the Royston and Sauerbrei R2D measure: the circulatory subcohort model had an R2D value of 0.32 and the respiratory model a value of 0.27. Evaluation of each individual’s risk-score quantile using a method suggested by Hosmer et al18 indicated that the models had a good fit as did graphical analysis of the relationship between Cox-Snell residuals and study time.
Discussion
The most statistically robust result from this study was the reduction in mortality following an insulation retrofit for older adults with a pre-existing circulatory condition. Although we did not have cause of death data, it is plausible that this finding is the result of reductions in fatalities resulting from cardiovascular events, a novel scientific finding that has been previously noted, but not fully explored. The lack of previous indications of an effect is likely to be due to prior studies’ small sample sizes, which meant that studies were incapable of detecting impacts of retrofitted insulation on rare events. The finding is consistent with a growing body of evidence linking higher indoor temperatures with reduced blood pressure and other markers of cardiovascular health.19–24 It is important to note that generalising these results to other jurisdictions requires caution as a number of conditions would need to be met, including similar baseline internal temperatures and similar treatment characteristics such as R values for insulation.
The finding of reduced mortality risk also has significant policy implications. When using ‘value of statistical life year’ derived values and conservative assumptions, the benefit gained per treated household per year was estimated at $NZ750, which drove the calculation of a highly favourable benefit:cost ratio over the 30-year lifetime of an insulation retrofit of 6.4:1 based on the assumption that retrofitted homes would house a reasonably consistent proportion of vulnerable occupants gaining health benefits during this period.16
It is important to acknowledge the limitations of these findings: the WUNZ: HS evaluation, as a quasi-experimental design, depends strongly on how well the controls represent what would have happened in the absence of the intervention. For instance, the differences in the health status and trajectory of the treatment and control groups might bias estimates of the effects of the intervention—for example, participation in the programme could indicate justified optimism in ongoing health, or it could indicate that a household/individual had been encouraged to participate in the programme due to poor health. In addition, the limitations of the administrative data used meant that other relevant health characteristics of cohort members, such as lifestyle factors like smoking and obesity, could not be controlled for. Furthermore, the quality of EECA and MOH administrative data, while audited and of a relatively high standard, can reasonably be expected to be poorer than that collected as part of a clinical trial. In addition, the data set creation process had an initial address match rate of only 79%, and because NHI address data are typically updated after an interaction with the health system a proportion of the cohort, particularly healthy individuals and more mobile groups such as young people and Māori, may not have lived at these addresses during some or throughout the study period. Fortunately, older adults are less likely to move than younger adults, which reduces this concern for the subcohorts analysed here. The pretreatment hospitalisation criterion also makes an accurate address more likely because all subcohort members have had recent interactions with the health system. Further mitigating these concerns is the likelihood that non-differential misclassification would bias results towards a null finding. Finally, it is important to note that because the majority of treatment group subcohort members lived in homes that received retrofitted insulation only rather than heating only or insulation and heating, the study had much greater potential to detect statistically significant changes for insulation. Similarly, because the circulatory subcohort was much larger than the respiratory subcohort, the likelihood of finding statistically significant changes was greater for that subcohort.
Despite these limitations, these findings are derived from two relatively large subcohorts that uniquely give this study the power to identify the impacts of retrofitted insulation on mortality, setting it apart from previous randomised controlled trials. The findings have had ongoing policy influence, reflected in the continuation of WUNZ: HS and in the creation of its successor, Warm Up New Zealand: Healthy Homes. The generalisability of these findings to other contexts will depend on the similarity of housing stock and the similarity of the insulation retrofits undertaken.
References
Footnotes
Contributors NP: wrote the PhD thesis the article is based on; carried out statistical analyses presented. MK: supervised PhD thesis; contributed statistical advice on analyses presented and reviewed and contributed to structure and presentation of statistical content of this paper; aided in drafting and revision of paper. LT-B: designed the Warm Up New Zealand: Heat Smart study protocol; led the analysis of health data from that study; carried out initial analysis of mortality presented in the 2011 report; contributed to literature review and paper generally; aided in drafting and revision of paper. AG: supervised thesis; led cost benefit-based evaluation that this study contributed to; contributed to design of Warm Up New Zealand: Heat Smart study protocol; contributed advice on statistical analyses presented; contributed to structure of paper, discussion section and terminology; aided in drafting and revision of paper. PH-C: supervised thesis; contributed to design of Warm Up New Zealand: Heat Smart study protocol; contributed to discussion, literature review and wording; aided in drafting and revision of paper.
Funding This article was derived from a PhD thesis based on a comprehensive policy evaluation that was funded by New Zealand’s Ministry of Economic Development in 2009.
Competing interests None declared.
Ethics approval Research approved by New Zealand Multiregion Ethics Committee on 2 March 2010, ethics ref MEC/10/EXP/002.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data available.