Article Text

Abstract
Introduction Chronic constipation is an independent risk factor for inadequate bowel preparation. The objective of this study is to evaluate the effectiveness and safety of the combined use of linaclotide and oral sulfate solution (OSS) in patients with chronic constipation undergoing colonoscopy.
Methods and analysis This is a prospective, randomised, controlled, single-blind (endoscopist) clinical trial that compares three bowel cleansing regimens for patients with chronic constipation undergoing colonoscopy. Regimen A consists of 2d-linaclotide and OSS, regimen B consists of 3d-linaclotide and OSS, and regimen C consists of OSS. All patients are required to consume a low-fibre diet for 3 days and then a clear fluid diet for 1 day before the colonoscopy. The primary outcome is adequate bowel preparation (defined as a Boston Bowel Preparation Scale (BBPS) score ≥2 for each segment and a total BBPS score ≥6). The secondary outcomes include defecation frequency, caecal intubation rate, adenoma detection rate and colonoscope insertion time and withdrawal time. The tertiary outcomes include complications of colonoscopy, adverse events and degree of comfort, which is evaluated via a self-designed questionnaire of comfort.
Ethics and dissemination The research will be conducted according to Good Clinical Practice principles. Ethical approval has been obtained from the Ethics Committee of Beijing Shijitan Hospital, Capital Medical University (IIT2024-146-003). Study findings will be published in peer-reviewed journals.
Trial registration number ChiCTR2500096394.
- Clinical Trial
- Endoscopy
- Clinical Protocols
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This will be a prospective, randomised, controlled, single-blind (endoscopist) clinical trial focused on bowel preparation for patients with chronic constipation.
This trial discontinues laxatives or prokinetics 7 days prior to colonoscopy, thereby allowing a more accurate assessment of the true impact of linaclotide on bowel preparation.
As a single-centre study, selection bias is inevitable.
The administration regimens of linaclotide and OSS, such as the optimal dosage, administration time and duration, are still uncertain and require further investigation.
Introduction
Colorectal cancer (CRC) has become a major public health concern worldwide, with the second highest mortality rate among all cancers and the third highest global prevalence.1 CRC is largely preventable through screening for colorectal adenomas, which are benign growths but may develop into cancer if not removed.2 Early detection and removal of colorectal adenomas can effectively block the ‘adenoma-carcinoma sequence’ pathway and ultimately prevent the development of CRC.3 Because of the increased use of endoscopic mucosal resection (EMR) or endoscopic submucosal dissection (ESD), the incidence of CRC has stabilised or started to decrease continuously in the USA and other high-income countries over the past two decades.4 In China, however, the all-age disability-adjusted life years rate of CRC has increased by 69.8% since 1990, which may be attributed to the high misdiagnosis rate of colorectal adenomas.5 Adequate preprocedural bowel cleansing maximises adenoma detection rates (ADRs), which is beneficial for CRC prevention.6
Polyethylene glycol (PEG) is widely used for bowel preparation. However, inadequate cleansing is observed in many patients with chronic constipation when 4 L of PEG is used. As a common gastrointestinal disorder, constipation affects 12%–17% of the population and is considered one of the risk factors for inadequate bowel cleansing. Improving water intake to 5–6 L can improve bowel cleansing comfort but is accompanied by worse tolerability and worse compliance.7 The main reasons for poor compliance include low tolerance and acceptance caused by a salty taste and large volume of liquid.8 9 Tolerability should be coordinated with cleansing efficacy to improve patients’ compliance and willingness to repeat colonoscopy. To improve bowel cleansing, several studies have been conducted on the combined use of PEG and additional agents, such as ascorbic acid, lactulose and mosapride.8–10 However, all of these methods have limitations. For colonoscopy preparation, the oral sulfate solution (OSS) is recommended by the European Society of Gastrointestinal Endoscopy (ESGE) and American Society of Gastrointestinal Endoscopy (ASGE) guidelines owing to its non-inferiority efficacy, greater safety and better tolerability.9 11 12 Thus, we aimed to explore an OSS-based derivative regimen with balanced effectiveness, safety and comfort.
Linaclotide is a selective guanylate cyclase-C (GC-C) receptor agonist that softens dejection and increases the frequency of defecation by accelerating intestinal transit and by stimulating the secretion of intestinal fluid.13 Moreover, linaclotide can reduce celialgia by inhibiting the activity of pain-sensing nerves14; its action occurs mainly in the gastrointestinal tract, and the adverse effects are generally mild.14 Thus, the combined use of linaclotide and OSS is believed to be a potentially effective bowel cleansing regimen. To the best of our knowledge, no research has been conducted to evaluate the effectiveness and safety of linaclotide combined with OSS as a bowel preparation regimen. The administration regimens of linaclotide mixed with OSS, including the optimal dosage of linaclotide, the administration time of linaclotide and the duration of linaclotide administration, are still in the exploratory phase and require further investigation. We aimed to explore the effectiveness, comfort and safety of a bowel preparation administration regimen of linaclotide mixed with OSS in this prospective, randomised, controlled, single-blind (endoscopist) clinical trial. The results obtained in this study may optimise bowel preparation protocols in clinical practice.
Materials and methods
Study design and patient population
This is a randomised, controlled, single-blind clinical trial comparing three bowel preparation regimens for patients with chronic constipation undergoing colonoscopy. The study will be conducted at Beijing Shijitan Hospital, Capital Medical University from 1 March 2025 to 31 December 2026.
The inclusion criteria for the study include patients with chronic constipation undergoing colonoscopy who meet the following criteria: (1) are aged 18–65 years; (2) meet the Rome IV criteria15 for chronic constipation which includes the presence of ≥2 of the following: (a) straining for >25% of defecations, (b) lumpy or hard stools (form 1 or 2 on the Bristol Stool Form Scale) for >25% of defecations, (c) sensation of incomplete evacuation for >25% of defecations, (d) sensation of anorectal obstruction/blockage for >25% of defecations, (e) manual manoeuvres to facilitate defecation for >25% of defecations; (3) have the ability to comprehend the trial, sign a written informed consent, including consent for a screening procedure to determine eligibility; (4) have the ability to communicate with the investigators well and follow verbal and written instructions; (5) have the ability to take OSS correctly according to the procedure and (6) have the ability to perform follow-up in accordance with the protocol.
The exclusion criteria include patients meeting one or more of the following criteria: (1) having a lack of indications for total colonoscopy; (2) having general contraindications to colonoscopy bowel cleansing, such as acute surgical abdomen, including intestinal perforation, acute diverticulitis and appendicitis, gastrointestinal obstruction, toxic megacolon; (3) having one of the following diseases: electrolyte disturbances or severe diseases of the heart, liver or kidney; (4) having a history of any colonic surgery; (5) taking or having taken linaclotide or being allergic to linaclotide; (6) being pregnant; (7) lactating or (8) participating in other clinical trials or participating in other clinical trials within 60 days.
Randomisation and blinding method
Subjects will be randomised at a 1:1:1 ratio to regimens A, B or C, via a computer-based random number table. The randomisation process will be performed by clinicians. They will prepare study products, provide education on bowel preparation and will be involved in the day-to-day care of patients. They will not be involved in performing the procedures. All endoscopists in this trial and biostatisticians will be unaware of each patient’s regimen allocation. Blinding of the endoscopist will be strictly enforced, and they will remain blinded until the main analysis is complete. Due to the volume differences and dose differences among the three regimens, blinding of the patients is impossible. Therefore, investigators will ask the subjects to refrain from talking about bowel cleansing with the endoscopists, either before or during the colonoscopy.
Selection of bowel preparation regimens
Before bowel preparation, each patient will be provided with written instructions on dietary restrictions and bowel cleansing methods. The following strict dietary restrictions will be given to all subjects: (1) follow a low-fibre diet for 3 days before the colonoscopy, (2) follow a clear fluid diet for 1 day before the colonoscopy and (3) fast on the day of the colonoscopy. A low-fibre diet is defined as a diet with a total fibre intake of less than 10 g/day. Patients will stop taking laxatives or prokinetics 7 days before the colonoscopy.
The study participants will be equally divided into three groups via a random number table. In regimen A, the subjects will (1) take 1d-linaclotide at 07:00 on the day before the procedure, (2) ingest a diluted OSS dissolved in approximately 500 mL of water followed by 1 L of water on the night before the procedure starting at 19:00, (3) take 1d-linaclotide at 05:00 on the day of the procedure and (4) drink 500 mL of a diluted OSS and 1 L of water on the day of the procedure, starting at 07:00 and completing at least 4 hours before the colonoscopy. Previous studies16 17 revealed that a single dose of linaclotide taken 1 hour before video capsule endoscopy significantly improved bowel preparation quality and visualisation, reducing transit time by 20% compared with published standards. Patients with chronic constipation would experience their first spontaneous bowel movements within 24 hours, accompanied by a shortened first defecation time and an increased number of defecations after taking linaclotide. Considering that the OSS is taken the day before and the day of the colonoscopy, regimen A was designed with the combined use of 2d-linaclotide and the OSS.14
In regimen B, the subjects will (1) take 1d-linaclotide at 07:00 2 days before the procedure, (2) take 1d-linaclotide at 07:00 on the day before the procedure, (3) ingest a diluted OSS dissolved in approximately 500 mL of water followed by 1 L water on the night before the procedure starting at 19:00, (4) take 1d-linaclotide at 05:00 on the day of the procedure and (5) drink 500 mL of a diluted OSS and 1 L water on the day of the procedure, starting at 07:00 and completing at least 4 hours before the colonoscopy. Regimen B was adapted from Wang et al18 and Xu et al,19 who combined 3 L PEG and 3d-linaclotide and reported that this regimen was satisfactory for patients with chronic constipation.18
In regimen C, the subjects will (1) ingest a diluted OSS dissolved in approximately 500 mL of water followed by 1 L of water on the night before the procedure starting at 19:00 and (2) they will drink 500 mL of a diluted OSS and 1 L of water on the day of the procedure, starting at 07:00 and completing at least 4 hours before the colonoscopy. All patients will receive 5 mL of simethicone solution mixed with the last dose of laxative. Regimen C is the control group, consisting of a traditional 1 L diluted OSS and 2 L water.
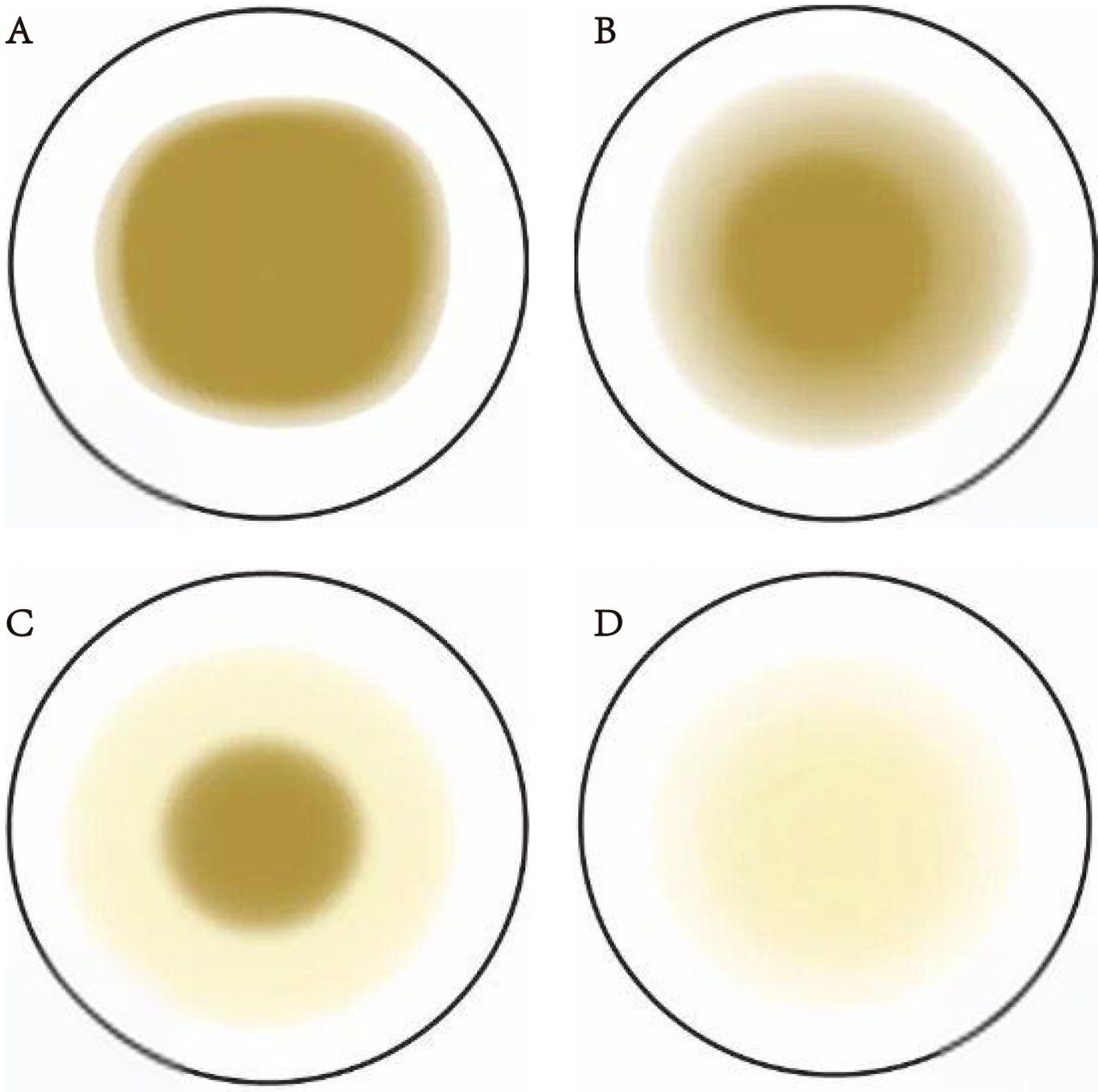
As a rescue regimen for inadequate bowel preparation, clinicians will gauge whether the last excreta is adequate before colonoscopy according to standard pictures (figure 1). For inadequate cleanings, 500 mL of diluted OSS and 1 L of water will be taken. The rescue regimen will be recorded on a case report form (CRF). The schedule of enrolment, interventions and assessments is presented in table 1.
Schedule of enrolment, interventions and assessments

{kind=link}
Standard pictures for the last excreta before colonoscopy. (A) Turbid liquid with faecal residue; (B) opaque liquid without residual stool; (C) slight-staining and clear liquid; (D) colourless and clear liquid. For patients with inadequate cleanings (A or B), supplement 500 mL diluted OSS and 1 L water will be taken.
Study procedures
The investigator will perform all the observations, investigations and evaluations according to the descriptions provided. The subjects will be given written instructions including the diet, dose and timing of the experimental drugs, in accordance with randomisation. Clinicians will distribute the study drugs to the participants, provide instructions on the administration and face-to-face bowel preparation education to ensure that the participants will take their drugs correctly. All colonoscopies will be performed by designated, professional endoscopists (who had performed more than 1000 colonoscopies individually) via the Olympus CV-260 or CV-290 colonoscope (Olympus Medical Systems, Tokyo, Japan). All participating endoscopists will be standardised and trained in the use of the Boston Bowel Preparation Scale (BBPS) before they participate in the study, and bowel preparation quality will be evaluated based on the BBPS. Endoscopists cannot use additional adjuvant devices or adjuvants to improve bowel preparation.
Data collection
The following clinical variables will be collected: (1) Demographics of the participants: sex, age, body mass index, comorbidities, use of calcium channel blockers, smoking or alcohol consumption, family history and laboratory indices (routine blood tests, liver and kidney function, coagulation function). (2) Bowel preparation: subject compliance, ability to understand and follow the instructions for bowel preparation, usage of laxatives, interval between the first OSS and the first defecation, and interval between the last OSS and colonoscopy. (3) Colonoscopy: BBPS score (total score and each segment score), caecal intubation rate, colonoscope insertion time and withdrawal time and ADR. (4) Safety: We will assess adverse events (AEs) and serious AEs (SAEs) associated with the agents before, during and after colonoscopy bowel cleansing. (5) Comfort: Results of the comfort questionnaire, including discomfort symptoms (nausea, vomiting, abdominal pain, abdominal distention, bowel incontinence, dizziness, headache, fatigue and tiredness), sleep quality (somnipathy, total sleep duration, frequency of sleep awakenings in the evening before colonoscopy) and willingness to duplicate colonoscopy bowel cleansing.
Study outcomes
The primary outcome will be adequate bowel preparation, defined as each segment’s BBPS scores being ≥2 and/or having a total score ≥6.20 21 The BBPS is based on three colon segment scores (right-sided colon, transverse colon and left-sided colon), and each segment score is defined by a four-point scoring system (0–3). The right-sided colon included the caecum and ascending colon, and the transverse colon was defined from the hepatic flexure to the splenic flexure, whereas any more distal colon or rectum was defined as the left-sided colon. Each segment score is between 0 and 3 as follows: 0=an unprepared colon segment with solid stool on the mucosa; 1=portions of the mucosa can be seen, but other areas are covered by staining, residual stool and/or opaque liquid and thus cannot be seen clearly; 2=minor areas covered by residual staining, small stool fragments and/or opaque liquid, but the colon segment can be seen well; 3=the entire mucosa can be adequately seen, with no residual staining, small fragments of stool or opaque liquid. As a superior trial, the BBPS total score and segment scores in regimens A and B should be statistically superior to those in regimen C.
The secondary outcomes include defecation frequency, the interval between the first OSS and the first defecation, the interval between the last OSS and the colonoscopy examination, the caecal intubation rate, the colonoscope insertion time and withdrawal time, and the ADR.
The third outcome will be the degree of comfort, which is evaluated via a self-designed questionnaire of comfort (QSC). The QSC was adapted from previous studies9 22 and is composed of complications and sleep quality during bowel preparation, as well as preprocedure anxiety and willingness to repeat bowel preparation. The complications included abdominalgia, abdominal distension, nausea, vomiting and bowel incontinence during bowel preparation. Sleep quality, including somnipathy, sleep duration and the number of sleep awakenings during bowel cleansing, was also recorded.
Safety indicators, such as AEs and SAEs, including abdominal pain, abdominal distension, faecal incontinence, allergic reactions and other adverse drug reactions, will be recorded and evaluated. Moreover, we will record complications of EMR or ESD, such as intraprocedural haemorrhage (any immediate bleeding that requires any form of endoscopic haemostasis or oozing lasting for at least 60 s), delayed haemorrhage (any bleeding requiring endoscopy reintervention or hospitalisation within 2 weeks), intraprocedural perforation (any perforation requiring endoscopic clip sealing), delayed perforation (any perforation occurring within 2 weeks) and intestinal infection (bellyache, fever and/or increased C-reactive protein requiring antibiotics).
Statistical analysis and sample size
Statistical analysis will be executed by SPSS V.20.0 (IBM Corp, Armonk, New York, USA). Continuous variables are expressed as the mean±SD or median (IQR) according to a normal/non-normal distribution and will be analysed with independent samples t tests or Wilcoxon’s rank-sum tests. Categorical variables are represented as counts (percentages) and will be evaluated by the χ2 test or Fisher’s exact test appropriately. To address the issue of multiple comparisons across the three study arms, we will employ adjustment methods, such as the Bonferroni correction, to ensure the robustness and validity of our statistical inferences. P value <0.05 will be set as the cut-off for statistically significant.
In the study protocol, the sample size calculation is performed with an alpha of 0.05 and a power of 0.8, assuming a 20% difference in the rate of colonic cleansing and a 10% dropout rate. Over the past year, approximately 500 patients with chronic constipation have undergone bowel preparation using OSS at our centre, resulting in an adequate bowel cleansing rate of approximately 70%. A final inclusion of 65 participants in each group was needed. The efficacy, safety and tolerability of bowel preparation will be compared based on intention-to-treat approaches or per-protocol analysis.
Patient and public involvement
Patients and the public were not involved in the development of the protocol.
Ethics and dissemination
The study has been registered with the Chinese Clinical Trial Registry and permitted by the Ethics Committee of Beijing Shijitan Hospital, Capital Medical University (IIT2024-146-003), and informed consent will be obtained from all patients prior to enrolment (see online supplemental material 1). The researchers will do their best to protect the personal information provided by patients from being leaked or used without informed consent. Data will be collected through paper forms directly from investigators. Data from the forms will be extracted and input into a database on a password-protected computer. The data will be supervised by an independent data monitoring committee.
Supplemental material
The findings of this study will be published in peer-reviewed journals for widespread dissemination. Individuals who contribute significantly to the research will be granted authorship, including research design, implementation, subject recruitment, data collection, statistical analysis and manuscript writing and revision.
Discussion
The aim of this study is to explore an innovative bowel preparation regimen that combines linaclotide and an OSS, which balances efficacy, safety and comfort in patients with chronic constipation undergoing colonoscopy. Bowel cleansing is an essential component of colonoscopy. OSS and PEG are widely used in clinical practice11 but are not optimal for patient satisfaction or the quality of bowel preparation in patients with chronic constipation. Improving PEG water intake to 5–6 L can improve effectiveness but can lessen comfort and influence compliance with bowel preparation.23 Discomfort and low compliance caused by a large volume of liquid are critical factors for inadequate bowel preparation.23
There are several PEG-based derivative regimens, such as those combined with ascorbic acid, lactulose and mosapride.8–10 However, some patients have difficulty tolerating PEG, and all PEG-based derivative regimens have limitations. OSS is recommended by the ESGE and ASGE guidelines due to its non-inferiority efficacy, greater safety and better tolerability than PEG.9 11 12 OSS, a newly developed bowel preparation agent in China, is composed of sodium sulfate and functions as an osmotic laxative; it improves the osmotic pressure derived from sulfate ions and replenishes sodium and potassium ions, thereby mitigating the risk of water-electrolyte imbalances. Phase III clinical trials have indicated that the OSS results in significantly higher BBPS scores than the 3–4 L PEG split-dose regimen does. Additionally, OSS facilitated swift bowel movements and achieved clear, watery stools, with a reduced incidence of nocturnal defecation. Hence, we aimed to explore an innovative OSS-based derivative bowel cleansing scheme that can lead to adequate bowel preparation in patients with chronic constipation.
As a selective GC-C receptor agonist, linaclotide has proven to be effective and safe for the treatment of chronic constipation (RR=3.26, 95% CI: 2.45 to 4.33) and irritable bowel syndrome with constipation (RR=2.26, 95% CI: 1.86 to 2.74), with slight adverse reactions such as diarrhoea.24 Linaclotide binds to the GC-C receptor, resulting in accelerated gastrointestinal motility, increased fluid in the intestine and reduced abdominal pain.25 Based on the pharmacological mechanism mentioned above, we believe that linaclotide may be an effective, comfortable and safe adjuvant for colonoscopy bowel preparation. Few studies8 14 18 have used linaclotide as an adjuvant to improve the cleansing efficacy, especially in patients at high risk of inadequate bowel preparation.26 However, the appropriate administration regimen has not been confirmed, and high-grade evidence from clinical trials is also very limited.
To elucidate the administration protocol, we have conducted an exhaustive literature review for this trial design. Considering the absence of prior studies on the combined use of linaclotide and OSS, our regimen is modelled on the combined use of linaclotide and PEG. According to Yang et al8, the BBPS total score and individual segment score in the 2LPEG+1d-linaclotide group were greater than those in the 2LPEG group (p<0.001), with a compatible sleeping quality or adverse reaction incidence. Compared with the 4LPEG group, the 2LPEG+1d-linaclotide group showed no significant difference in adequate bowel preparation but had better sleep quality and fewer adverse reactions. Song et al14 performed a prospective randomised study and reported that the 3LPEG+1d-linaclotide group was comparable to the 4LPEG group in terms of adequate bowel preparation with a shorter withdrawal time (p<0.05). In a prospective, randomised, observer-blinded, multicentre study,27 2d-linaclotide+PEG were used for bowel cleansing. This regimen shortened the first defecation time after consuming PEG (p<0.01), which may contribute to adequate preparation with minimal side effects. Moreover, nausea and vomiting were less common in this group, which could be interpreted as a reduction in volume. The use of linaclotide shortened the first defecation time and increased the mean number of defecations before starting PEG.28 These findings encouraged us to choose a 2d-linaclotide regimen with greater cleansing efficacy, better tolerability and a more pleasant experience during colonoscopy.
In a randomised controlled trial (RCT)18 conducted in patients with chronic constipation, compared with the 4LPEG group, the 4LPEG+1d-linaclotide group and the 3LPEG+3d-linaclotide group were superior in terms of adequate bowel preparation rates, with a lower percentage of mild AEs (p<0.01). In a prospective, single-centre RCT,19 the combination of 3LPEG and 3d-linaclotide demonstrated significantly higher rates of adequate and excellent bowel preparation (p<0.05) with a reduced volume of intake. These findings suggest that linaclotide could improve the cleansing efficacy without additional AEs. These PEG-based derivative regimens still display poor compliance due to the large volume of liquid and unacceptable taste. OSS has shown non-inferiority efficacy, greater safety and better tolerability than PEG.3 12 Based on these previous studies and clinical practice, we hypothesise that the additional use of linaclotide may improve the cleansing efficacy without additional OSS intake. Given that patients with chronic constipation first experience spontaneous bowel movements within 24 hours after taking linaclotide,28 the OSS is taken the day before and the day of the colonoscopy. We designed 2d-linaclotide (the day before and the day of the colonoscopy) +OSS and 3d-linaclotide (2 days before, the day before and the day of the colonoscopy) +OSS. This trial includes patients who reflect the real clinical situation, which makes the results more valuable for clinical practice. We expect that this study will provide propositions for patients with chronic constipation undergoing colonoscopy bowel preparation.
Ethics statements
Patient consent for publication
Acknowledgments
We thank all participants for their voluntary participation in this study and thank all researchers for their hard-working in study procedures.
References
Footnotes
Contributors All authors contributed to the study conception and design. Material preparation, data collection and analysis were done by CG, JW, LL, JC, HL and GY. The first draft of the manuscript was written by CG, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript. GY is the guarantor.
Funding This work was supported by the Beijing Municipal Administration of Hospitals Incubating Program (PX2021030); the Science and Technology Development Project of China State Railway Group (J2021Z609) and Youth Fund of Beijing Shijitan Hospital, Capital Medical University (2022-q12).
Competing interests CG received funding from Beijing Shijitan Hospital, Capital Medical University during the conduct of this study. The study sponsor had no role or influence in the study design, in the collection, analysis and interpretation of the data, in the writing of the report or in the decision to submit the paper for publication. The authors declare no competing interests.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.