Article Text

Abstract
Introduction Fibrotic interstitial lung diseases (F-ILD) are severe and often progressive lung disorders that frequently lead to respiratory failure, with patients experiencing high symptom burdens, including severe dyspnoea. This is also evident in patients with severe chronic obstructive pulmonary disease (COPD). Many patients will eventually require ambulatory oxygen therapy (AOT) due to exertional desaturation. Although AOT has shown benefits like increased walking distance and improved quality of life, adherence remains a challenge due to practical issues. AOT can be given by oxygen bottles that provide continuous oxygen flow or as portable concentrators; however, there is a lack of studies comparing the different methods and assessing patient preferences. Data from the present study help guide the selection of patients for different AOTs and provide information on patient preferences.
Methods and analysis The study design is a single-centre, randomised, open-label cross-over exploratory comparative study to investigate the efficacy of two different oxygen delivery systems. Patients with COPD or F-ILD who, during a 6-minute walk test (6MWT), can walk at least 50 m and desaturate below 88% are eligible for inclusion in the study. The participants are randomised to perform the 6MWT with either oxygen bottles or portable concentrators first. The primary endpoint is the difference in the lowest oxygen saturation (SpO2) between the two systems. Secondary endpoints include, among others, the difference in percentage of time and number of minutes when SpO2 falls below 88%, mean and maximum pulse rate, and distance and time taken to recover during the 6MWT. Quality of life and patient preferences will be evaluated by scores from the COPD assessment test and the King’s Brief Interstitial Lung Disease health status questionnaire to help gain a better understanding of symptom impact during activity and limitations in daily life.
Ethics and dissemination The study has been approved by the Central Denmark Region Committees on Health Research Ethics (1-10-72-115-24). The results of this trial will be submitted for publication in an international peer-reviewed journal.
Trial registration number NCT06767904.
- Interstitial lung disease
- Pulmonary Disease, Chronic Obstructive
- Adult palliative care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The cross-over design allows each participant to experience both systems, controlling for factors like age and baseline health, which might otherwise confound the results.
Since participants serve as their own controls, variations between individuals are minimised, increasing accuracy of the comparison between different oxygen delivery methods.
Randomisation of the treatment order reduces bias and ensures that any order effects are distributed equally across the sample.
The results may not be easily generalisable to broader populations, if the participants are homogeneous in terms of age, health conditions or oxygen requirements.
Introduction
Long-term oxygen therapy (LTOT) is commonly prescribed for patients with chronic respiratory failure. Fibrotic interstitial lung disease (F-ILD) is a group of severe scarring lung diseases with a dismal prognosis.1–3 The introduction of antifibrotic therapy has resulted in delayed disease progression and prolonged survival. However, despite the optimism surrounding antifibrotic therapies, a substantial number of patients with F-ILD will progress.4–8 Over time, patients will suffer from an increased symptom burden, including increased exertional dyspnoea and reduced exercise capacity due to respiratory failure, initially exercise-induced but later resting hypoxaemia. Similarly, patients with advanced chronic obstructive pulmonary disease (COPD) often develop chronic respiratory failure due to structural changes in lung architecture, especially emphysema, with compromised oxygen transfer from the lungs to the blood. These patients will also develop exertional desaturation and ultimately respiratory failure, requiring oxygen supplementation.
LTOT has been shown to improve pulmonary haemodynamics and survival in patients with COPD and is also recommended for respiratory failure in F-ILD,1 9 typically recommended for 15–24 hours a day for patients with chronic respiratory failure.
Before developing chronic respiratory failure, many patients will experience significant desaturation during exertion. As a result, ambulatory oxygen therapy (AOT) is often prescribed, though for different and variable indications in F-ILD.10 11 Additionally, patients using LTOT will often desaturate even more on exertion as the oxygen demand increases during activity. The potential benefits of ambulatory oxygen are not sufficiently studied. It is still unclear whether the use of AOT itself can improve the prognosis of hypoxaemic patients or if exertional desaturation is related to increased mortality per se. In the recent Ambox study, the effects of AOT versus no AOT were studied in a 2-week cross-over design. AOT resulted in increased walking distance, less dyspnoea and improved quality of life.12 However, despite these positive results, one-third of patients decided against AOT due to practical issues like the weight of the portable equipment. Similarly, Ciarleglio et al have shown that AOT, compared with placebo, provides significant benefits in patients with F-ILD.12
AOT can be delivered by oxygen bottles providing a continuous oxygen flow, but this equipment is heavy to carry for many patients. Therefore, a portable concentrator is often preferred. Portable concentrators often come with a demand oxygen delivery system (DODS) that can sense the beginning of an inhalation. This triggers immediate delivery of a short bolus of oxygen, thus limiting oxygen delivery to the onset of inhalation. As a result, the oxygen consumption is reduced, and the time that patients can use the portable system is extended.
However, clinical experience shows that many patients with F-ILD have difficulties triggering the flow sensor on exertion due to the accelerated respiratory rate and reduced tidal volume, whereas patients with COPD do not seem to have similar challenges. As a consequence of this clinical experience, all patients with F-ILD and some patients with COPD are referred for a 6-minute walk test (6MWT) with continuous oxygen from bottles (COB) followed by a 6MWT with a portable DODS to ensure they benefit similarly from both oxygen devices. The current practice is resource-demanding from both the patient and health provider’s perspective. The data from this study will help refine the patient selection process for portable DODS, aiming to streamline the prescribing process and potentially reduce unnecessary trial and error. In addition, the study will explore patient preferences and comfort, which are crucial for optimising the clinical application of these devices.
Aim
In this trial, we aim to compare various outcomes of the two oxygen delivery systems—COB and DODS—in patients with F-ILD and COPD. Specifically, we will evaluate oxygen saturation (SpO2), pulse rate, walking distance, recovery time, health-related quality of life (HR-QoL), patient preferences and comfort. By doing so, we hope to improve the efficiency of the oxygen prescribing process, ensuring that patients are matched with the most appropriate device based on their individual needs.
Trial design
This trial is a single-centre, randomised, open-label cross-over exploratory comparative study to investigate the efficacy of two different oxygen delivery systems for AOT.
Methods and analysis
Eligibility criteria
The inclusion and exclusion criteria for the trial can be seen in table 1.
Eligibility criteria
Randomisation
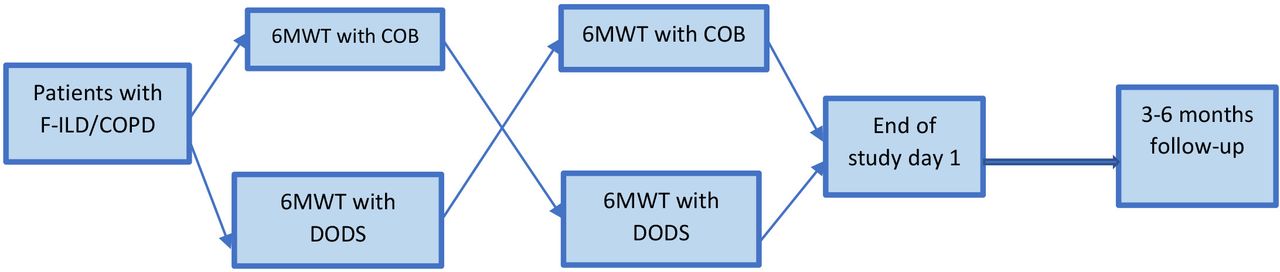
After confirming that the research subjects meet all the eligibility criteria and none of the exclusion criteria, and the patient has signed the informed consent. The patient will perform the 6MWT using AOT by COB or DODS in random order (1:1) (figure 1). Allocation tables for randomisation will be created by a data manager at the Clinical Trial Unit at the Department of Clinical Medicine, Aarhus University, who is not involved in the study. The allocation tables will be uploaded to the Research Electronic Data Capture (REDCap) database and randomisation of individual patients will be conducted in REDCap after inclusion.

{kind=link}
Study design. COB, continuous oxygen with bottles; COPD, chronic obstructive pulmonary disease; DODS, demand oxygen delivering system; F-ILD, fibrotic interstitial lung disease; 6MWT, 6-minute walk test.
Study setting
The study takes place at Aarhus University Hospital. 30 patients with F-ILD and 30 patients with COPD will be assigned to either COB or DODS in random order. Patients who fulfil criteria for (AOT) will be asked to participate by the treating physician or the physiotherapist performing 6MWTs. Physiotherapists who are a part of the research group will perform the study-related tests.
Study intervention
Before any test, patients with F-ILD will complete the Kings Brief Interstitial Lung Disease questionnaire, an interstitial lung disease specific HR-QoL patient-reported outcome measure (PROM),13–15 and all patients will complete the COPD Assessment Score (CAT).16 Both scores are translated and validated in Danish. CAT has been validated both in COPD and F-ILD.17
At the hospital, patients will receive oxygen during the 6MWT by either COB 4 L/min or DODS at the max. setting. Patients will rest for 30 min between tests. Saturation, pulse rate, walking distance and rating of perceived dyspnoea will be recorded for each test.
After both 6MWTs are completed, the patients will complete questions related to their preference for the oxygen system, comfort and reliability (table 2).
Study parameters
Patients will continue with the oxygen system that results in the least desaturation or is preferred by the patient. Participation in the study will not affect the indication or prescription of ambulatory oxygen.
After 6 months, follow-up will take place where patients will complete HR-QoL PROMs and participate in a semistructured qualitative interview (table 2).
Duration for each subject
Study participants will be informed about the study and asked to participate during an elective outpatient visit. If they agree and informed consent is signed, the study will take place either the same day or on another day, depending on the availability of health professionals and patient ability to participate in the tests. Follow-up will be conducted during a subsequent scheduled visit, at 6 months after the baseline visit. Thus, the study period has a duration of 6 months.
Study parameters
Primary outcome measure
The primary endpoint is the difference in the lowest SpO2 (%) between COB and DODS during the 6MWT.
Secondary outcome measures
Secondary outcomes are described below.
Percentage of time when SpO2 falls below 88% during the 6MWT (%).
Number of minutes when SpO2 falls below 88% during the 6MWT (minutes).
Minimum value of SpO2 during the 6MWT (%).
Mean pulse rate during the 6MWT (per minute).
Maximum pulse rate during the 6MWT (per minute).
Difference in 6MWT distance (m).
The time taken to recover SpO2 after 6MWT to the level obtained at rest (minutes).
Maximal rating of dyspnoea on the Borg scale.
Change in dyspnoea from rest to end of 6MWT measured by the Borg scale.
Patient preferences for COB or DODS (‘Which system do you prefer?’).
Comfort measured by a Likert scale (‘How much do you like using COB/DODS’ on a scale from 1 to 7).
Reliability measured by a Likert scale (‘Do you feel you get sufficient oxygen using COB/DODS’ on a scale from 1 to 7).
Semistructured qualitative interviews about patients’ view on AOT with COB/DODS.
Questions regarding the use of AOT by COB/DODS with respect to comfort and frequency of use.
Change in HR-QoL between baseline and 6 months.
Associations between baseline characteristics and effect of and patient views on AOT with COB/DODS.
Semistructured qualitative interviews
To record participants’ experiences of using AOT, including benefits and concerns, audio recorded semistructured interviews will be audio recorded following a topic guide, conducted by one of the study researchers 6 months after inclusion. The audio recordings will be transcribed, anonymised and entered into NVivo qualitative data analysis software (V.10), then analysed according to the framework approach—a systematic, well-recognised method for qualitative analysis that is based on a process of summarisation and subsequent mapping onto framework matrices, which enables generation of themes.18
Sample size and recruitment
The purpose of this clinical trial is to demonstrate non-inferiority between COB and DODS. Based on an SD of 3.6 in SpO2 difference between COB and DODS, as reported by Tiep et al,19 a sample size of 30 patients with COPD and 30 patients with F-ILD is calculated, assuming a power of 80%, a significance level of 0.05, a non-inferiority margin of 3.5 and a 10% dropout rate.
Regarding the qualitative interviews, the study aims to reach data saturation, and as such, the number of both idiopathic pulmonary fibrosis and patients with COPD is undecided until the study commences. It is expected that the number will be around 10–15 patients in each category.
Blinding
This trial is an open-label trial, as blinding of the two different oxygen delivery systems is unachievable.
Data collection and management
All data will be collected and recorded in a REDCap database designed specifically for this trial.
Study overview
The study is planned to recruit patients from 1 May 2025 to 30 April 2026, and the study will end 6 months after the last patient has been recruited.
Statistical methods
Analysis will be conducted after all patients have been included and data cleaning is completed.
Descriptive analysis of patient groups at baseline
Distribution and summary statistics of baseline demographic data will be calculated for the full data set. For nominal variables, category frequencies and proportions will be calculated. For continuous variables, summary statistics, including means with SD or medians with IQRs, will be calculated.
Data analysis of the primary endpoints
Categorical variables will be compared using the McNemar test. Continuous variables are examined for normality and analysed with either a paired t-test or mixed effects models (in case of normality) or Wilcoxon signed-rank test (in case of non-normality). The statistical package STATA V.14.2 will be used for all statistical analyses.
The Δ saturation (difference between the highest and lowest value of SpO2) between COB and DODS 6MWT, along with its 95% CI, will be estimated as the primary analysis for the primary endpoint.
To investigate the association between baseline characteristics and the lowest value of SpO2, a subgroup analysis of patients with F-ILD or COPD will be performed, as well as a subgroup analysis with respect to disease severity and degree of desaturation.
Analysis pertaining to the secondary evaluation criteria
The same analysis used for the primary endpoint will be performed for the secondary endpoints.
Categorical variables will be compared using the McNemar test. Continuous variables will be examined for normality and analysed with either paired t-tests or mixed effects models (in case of normality) or Wilcoxon signed-rank test (in case of non-normality).
Interim analyses will not be performed.
The study protocol adheres to the Standard Protocol Items: Recommendations for Interventional Trials 2013 guidelines.
Data handling and storage
Data will be registered in REDCap. Correctness will be ensured by proofreading. Personal information will be treated in accordance with the General Data Protection Regulation. Source data related to standard clinical visits will be kept in the electronic patient files. Study-specific source data, such as patient questionnaires, will be typed directly into REDCap or recorded on paper documents, which will be stored in a secure area at the research department. All results will be kept for ten years after the end of the study, after which they will be destroyed.
Patient and public involvement
Patients currently being evaluated for AOT were consulted during the design of this study to ensure it is relevant and patient-centred focus. Their feedback helped shape the study.
Data monitoring committee
A data monitoring committee is not necessary due to the limited sample size, low risk of harm and the study’s straightforward design, which does not involve complex interventions or safety concerns that would require independent oversight.
Missing data
If patients do not complete both 6MWT, new patients will be included to reach the prespecified number of subjects.
Risk
Study participation is not related to any additional tests beyond what is planned from routine medical care, except for questions on patient preferences, HR-QoL and qualitative interviews. The 6MWT is carried out daily by experienced physiotherapists, and the inclusion and exclusion criteria select patients with minimal, if any, risks. However, any unexpected adverse events during the 6MWT will be carefully recorded.
Ethics and dissemination
Patients will only be included in this trial after providing written informed consent. The participant consent form is available in online supplemental materials. The study has been approved by The Central Denmark Region Committees on Health Research Ethics (1-10-72-115-24) and is registered at ClinicalTrials.gov (NTC06767904). Any important protocol modifications will be reported to The Regional Ethics Committee and at ClinicalTrials.gov. The study will be conducted in accordance with the Declaration of Helsinki and the Ethics Committee requirements.
Supplemental material
Patients may benefit individually by gaining knowledge about their oxygen need during exercise, and, as a group, contribute to increased knowledge about the effect of two different oxygen delivery systems during exercise in relation to specific pulmonary diseases.
The results of this trial will be submitted for publication in an international peer-reviewed journal.
Confidentiality
The study will be registered in the regional data agency records. Data will be handled according to Danish legislation. All original records will be archived at the trial site for 10 years.
Dissemination policy
The results of this clinical trial will be submitted as a paper in parallel with a presentation at a research conference. All coauthors will review and approve the content of the article before submission. All authors will adhere to the Vancouver recommendations on authorship guidelines.
Data statement
Full access to the protocol, participants dataset and statistical codes will be granted on reasonable request.
Discussion
The rationale behind this trial stems from clinical observations highlighting that many patients with F-ILD and COPD experience difficulty triggering DODS delivery. On the other hand, COB is heavier and more difficult to transport, especially when the patient is physically active. This challenge has posed practical issues in managing oxygen therapy for these patient groups, often leading to suboptimal outcomes in both clinical effectiveness and patient quality of life. Given these observations, we anticipate that this study will provide insights into how patients with F-ILD and COPD interact with oxygen delivery devices, potentially leading to more tailored and effective treatment strategies.
The primary objective of this trial is to build a robust, evidence-based understanding of the effectiveness and usability of oxygen concentrators within these patient populations. With the data, we expect to provide solid evidence that can directly inform clinical decision-making. Additionally, the inclusion of qualitative data, gathered through patient questions and interviews, will offer deeper insights into the subjective experiences of patients. These qualitative responses are essential for capturing the nuances of patient preferences, comfort and perceptions—elements that are often overlooked in clinical trials but play a pivotal role in device adherence and overall treatment success.
The findings from this study are expected to significantly enhance clinicians’ ability to make more informed decisions regarding the selection of oxygen delivery systems for patients with F-ILD and COPD. A better understanding of device effectiveness will also contribute to more judicious use of healthcare resources by reducing the need for unnecessary tests or trials that do not provide meaningful clinical benefit.
Moreover, the trial will address the practical burden of multiple walk tests, which are often required to assess the effectiveness of oxygen therapy but can be physically taxing for patients with F-ILD and COPD. The results from our trial could have significant implications for how healthcare providers assess oxygen therapy, potentially streamlining the process and making it less burdensome for patients.
From a broader healthcare perspective, the findings of this study have the potential to guide future practices in both clinical care and resource allocation. By identifying the oxygen systems that are most effective for specific patient populations, healthcare systems can allocate resources more efficiently, ensuring that patients receive devices best suited to their needs. Additionally, our findings could provide valuable information to device manufacturers, encouraging the development of more patient-centred designs that consider the practical limitations and preferences of individuals living with F-ILD and COPD.
It is important to note that the primary goal of this study is not to demonstrate the non-inferiority of one device over another, but rather to gather critical data that can help clinicians make better-informed decisions about which device will be most beneficial for specific patient populations.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors All four authors contributed to the design of the study and writing the protocol. SK-W is the guarantor.
Funding The study has received €13 500 from the Danish Lung Association.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.