Article Text

Abstract
Objectives This study aims to investigate the relationship between the triglyceride-glucose (TyG) index in patients with early sepsis-associated acute kidney injury (SA-AKI) and the risk of in-hospital mortality.
Design Secondary data analysis.
Setting This study analysed secondary data from the Medical Information Mart for Intensive Care (MIMIC) 2008–2022.
Participants A total of 1632 participants were enrolled in the final analysis.
Primary and secondary outcome measures A secondary data analysis study was conducted using data from the MIMIC IV 3.0 database. Participants were divided into four groups based on the quartiles of the TyG index. The primary outcome was all-cause in-hospital mortality. The association between the TyG index and in-hospital mortality among SA-AKI patients was assessed using multivariate COX proportional hazards regression analysis and restricted cubic spline regression analysis. Subgroup and sensitivity analyses were performed to verify the robustness of results.
Results A total of 1632 patients were included in the study. The in-hospital mortality rate was 31.13%, and the intensive care unit (ICU) mortality rate was 25.25%. Multivariate COX regression analysis showed that the TyG index was independently associated with an increased risk of in-hospital mortality (HR 1.14 (95% CI 1.02 to 1.27); p=0.02) and ICU mortality (HR 1.17; (95% CI 1.04 to 1.32); p=0.01). The restricted cubic spline regression model indicated that the risk of in-hospital and ICU mortality increased linearly with the increase in the TyG index. Sensitivity analysis demonstrated that the effect size and direction were consistent across different subgroups, and the results were stable.
Conclusion A high TyG index is associated with increased mortality during hospitalisation in patients with SA-AKI. Larger-scale prospective studies are needed to confirm these findings.
- Intensive Care Units
- Acute renal failure
- Mortality
- INTENSIVE & CRITICAL CARE
Data availability statement
Data are available in a public, open access repository. The datasets generated and/or analysed during the current study are available in the MIMIC-IV repository, https://physionet.org/content/mimiciv/3.1/.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The extensive Medical Information Mart for Intensive Care-IV database was used, enhancing the generalisability of the findings.
Employed rigorous statistical methods, including multivariate and spline regression analyses, to ensure result reliability.
Focused on the under-researched early-stage sepsis-associated acute kidney injury, potentially aiding in early identification of high-risk patients.
Only the baseline triglyceride-glucose index was considered, omitting its temporal changes that could affect outcomes.
The generalisability of the findings may be limited due to the data being sourced from a single medical centre.
Introduction
Sepsis is a life-threatening organ dysfunction caused by a dysregulated response to infection, which typically includes acute kidney injury (AKI).1 Previous studies have shown that approximately 60% of AKI cases in critically ill patients are associated with sepsis, hence referred to as sepsis-associated acute kidney injury (SA-AKI).2–4 SA-AKI is common in critically ill patients and is closely associated with adverse outcomes, including prolonged hospital stays and increased risk of death.5 6 SA-AKI can be divided into early or late stages. Early SA-AKI is mainly caused by SA-AKI, while late SA-AKI is usually an indirect result of sepsis treatment, with early and late SA-AKI showing phenotypic and prognostic differences.7 Moreover, studies have indicated that most patients are diagnosed with AKI on the same day as sepsis diagnosis.8 Therefore, identification and intervention of early SA-AKI can better improve patient outcomes.
Insulin resistance (IR) is characterised by reduced effectiveness of insulin in promoting glucose uptake and utilisation, playing a crucial role in the deterioration of conditions in patients with SA-AKI.9 10 The triglyceride-glucose (TyG) index, due to its easier and more convenient acquisition compared with IR, has become an alternative biomarker for IR.11 In recent years, multiple studies have shown a significant association between the TyG index and all-cause mortality in critically ill patients with conditions such as sepsis, ischaemic stroke and chronic kidney disease (CKD).12–15 Additionally, the TyG index has demonstrated good predictive value in long-term major adverse cardiovascular events among patients with high cardiovascular risk.16 17 Several studies have demonstrated that the TyG index correlates with the advancement of metabolic disorders.18 19 The extensive release of inflammatory factors and unbalanced oxidative stress may be the chief culprit in inducing IR and aggravating renal function damage in sepsis.20 Moreover, IR contributes to kidney injury through multiple mechanisms, including endothelial dysfunction, oxidative stress and inflammatory responses, all of which are closely related to the occurrence and progression of SA-AKI. 21 Currently, there is a lack of research on the relationship between the TyG index and outcomes in patients with early SA-AKI. Therefore, this study aims to explore the relationship between the TyG index and clinical outcomes in patients with early SA-AKI, which may help us identify high-risk patients and potentially contribute to the development of new strategies to improve patient outcomes.
Methods
Patient and public involvement
Patients or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Study population
This is a secondary data analysis study with longitudinal follow-up of patients. The Medical Information Mart for Intensive Care IV (MIMIC-IV-3.0) is a freely accessible database that includes 94 458 ICU admissions from Beth Israel Deaconess Medical Center in Boston, Massachusetts, spanning from 2008 to 2022.22 The MIMIC-IV database contains a wealth of information, including demographic data, vital signs, laboratory results and diagnostic information classified using International Classification of Diseases, Ninth Revision (ICD-9) and Tenth Revision (ICD-10) codes. To access the database, one of the authors (Chengyi Feng) obtained the necessary certification (MIMIC-IV database authorised use certificate number: 58286177).
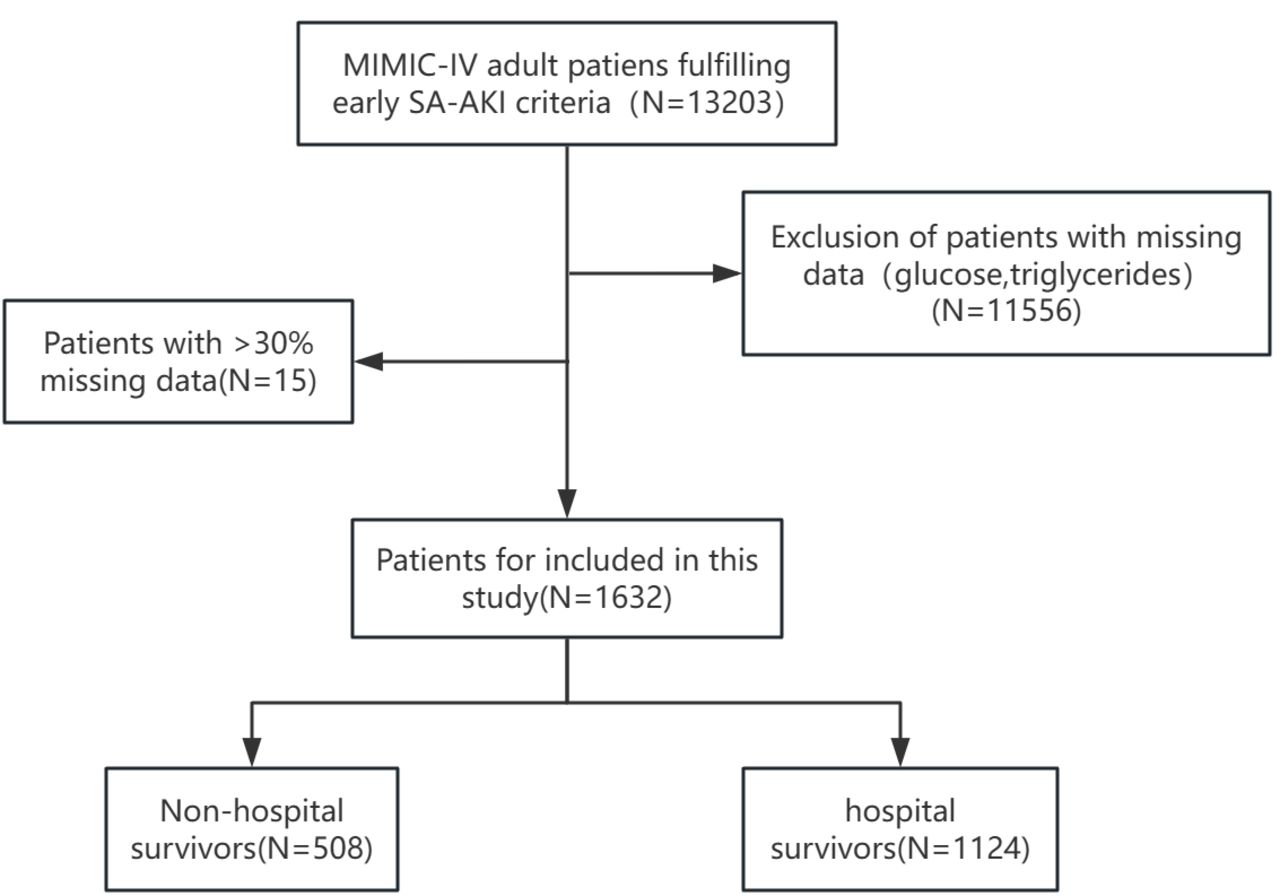
In this study, early SA-AKI is defined as AKI occurring within 48 hours after the diagnosis of sepsis, according to the 28th Acute Disease Quality Initiative Task Force consensus report. Sepsis diagnostic criteria are defined according to Sepsis-3 standards as patients having an infection and a Sequential Organ Failure Assessment (SOFA) score of ≥2.23 The diagnosis of AKI is defined according to the Kidney Disease: Improving Global Outcomes (KDIGO) criteria as either an increase in Serum Creatinine (SCr) of ≥1.5 times the baseline within 7 days, an increase in SCr of ≥0.3 mg/dL within 48 hours or a urine volume of <0.5 mL/kg/hr within 6 hour.24 The inclusion criteria were as follows: (1) diagnosis of sepsis that met the Sepsis-3 criteria; (2) development of AKI within 48 hours after the diagnosis of sepsis. The exclusion criteria were as follows: (1) age <18 years; incomplete data (eg, missing triglycerides and fasting blood glucose) or missing values exceeding 30% (figure 1).

Flow chart of patient selection.
Variable extraction
In this study, information was extracted using Structured Query Language (SQL) with PostgreSQL software (version 16.4) and Navicat Premium software (version 16). If a patient had multiple ICU admissions, only data from the first admission were selected. Data extracted from the MIMIC-IV database within 24 hours of patient ICU admission included demographic information such as age, gender and race; comorbidities including chronic kidney disease (CKD), chronic obstructive pulmonary disease (COPD), cerebrovascular disease (CVD), liver disease, diabetes, cancers, congestive heart failure (CHF), myocardial. infarction (MI), sequential organ failure assessment (SOFA) score and laboratory indicators (white blood cell (WBC), haemoglobin, platelets, albumin, blood urea nitrogen (BUN), creatinine, calcium, potassium, neutrophils, lymphocytes, fasting blood glucose and triglycerides). If a variable was recorded more than once in the first 24 hours, we used its average value. Data on the use of nephrotoxic drugs, vasopressors and diuretics within the first 2 days of ICU admission were also extracted. The extraction of insulin usage data is based on information recorded within the first 24 hours after ICU admission. Follow-up began on the date of ICU admission and ended on the date of death. The TyG index was calculated using the formula ln (fasting triglycerides (mg/dl) × fasting blood glucose (mg/dl)).2 The NLR index is defined as the neutrophil-to-lymphocyte ratio. All laboratory variables, excluding those with missing values exceeding 30%, were included to reduce potential bias. For variables with missing values of less than 30%, multiple imputation was performed using the ‘miceforest’ package in Python software. The dataset with the smallest normalised root mean square error compared with the original data was selected for model construction (see online supplemental tables S1 and S2).
Supplemental material
Supplemental material
Primary outcome and secondary outcome
The primary outcome of the present study was in-hospital all-cause mortality, and the secondary endpoint was ICU mortality.
Statistical analysis
Continuous variables are expressed as mean±SD or median (Q1,Q3) according to data distribution, while categorical variables are expressed as proportions. The Kolmogorov–Smirnov test is used to assess the normality of continuous parameters. If normally distributed, t-tests or analysis of variance are used for continuous variable analysis; if not normally distributed, Mann–Whitney U tests or Kruskal–Wallis tests are used for continuous variable analysis. The HR and 95% CI between the TyG index and endpoints are calculated using the Cox proportional hazards model, with adjustments made to certain models. Confounding variables included in the multivariate logistic analysis are selected based on P values <0.05, and factors that may affect prognosis as suggested by clinical physicians and clinical experience are used as independent variables in the multivariate COX regression analysis. Specifically, Model 1: unadjusted; Model 2: adjusted for age, gender and race; and Model 3: adjusted for age, gender, race, CHF, diabetes, CVD, CKD, use of nephrotoxic drugs, use of vasopressors, use of diuretics, SOFA, WBC, BUN and NLR. We also used a four-knot restricted cubic spline regression model to analyse the association between baseline TyG index and all-cause mortality in hospital and ICU. Additionally, subgroup analyses were conducted to verify the correlation between the TyG index and mortality rates in the hospital and ICU for each subgroup. The COX proportional hazards model was also used for sensitivity analysis to confirm the robustness and stability of the results. All statistical analyses were performed using R (version 4.2.2), with statistical significance defined as a two-sided p value <0.05.
Results
Baseline characteristics
Based on the inclusion and exclusion criteria, this study enrolled 1632 patients with early SA-AKI from the MIMIC-IV database, with an in-hospital mortality rate of 31.13% and an ICU mortality rate of 25.25%. The baseline characteristics of early SA-AKI patients categorised by the quartiles of TyG index are shown in table 1. Patients were divided into four groups based on the admission TyG index levels (Q1: 6.19–8.80; Q2: 8.80–9.28; Q3: 9.28–9.86; Q4: 9.86–13.49). The median TyG index values for each quartile were 8.49 (Q1, Q3: 8.24, 8.65), 9.02 (Q1, Q3: 8.91, 9.15), 9.55 (Q1, Q3: 9.41, 9.71) and 10.38 (Q1, Q3: 10.10, 10.82). In table 1, using Q1 as the reference group, it was found that younger diabetic patients were more likely to have higher TyG indices, and patients with higher TyG indices exhibited increased WBC counts, BUN, creatinine, sodium, NLR and SOFA scores. Additionally, longer hospital and ICU stays were observed in groups characterised by higher TyG indices. In online supplemental table S3, the comparison between hospital survivors and non-survivors showed that age, haemoglobin, platelets, WBCs, albumin, BUN, calcium, serum creatinine, sodium, NLR, SOFA, TyG and NLR were associated with in-hospital mortality. Non-surviving patients were also more likely to have a history of heart failure, malignant tumours and nephrotoxic drug and vasopressor use.
Supplemental material
Baseline characteristics according to TyG index quartiles
Associations between the TyG index and all-cause mortality
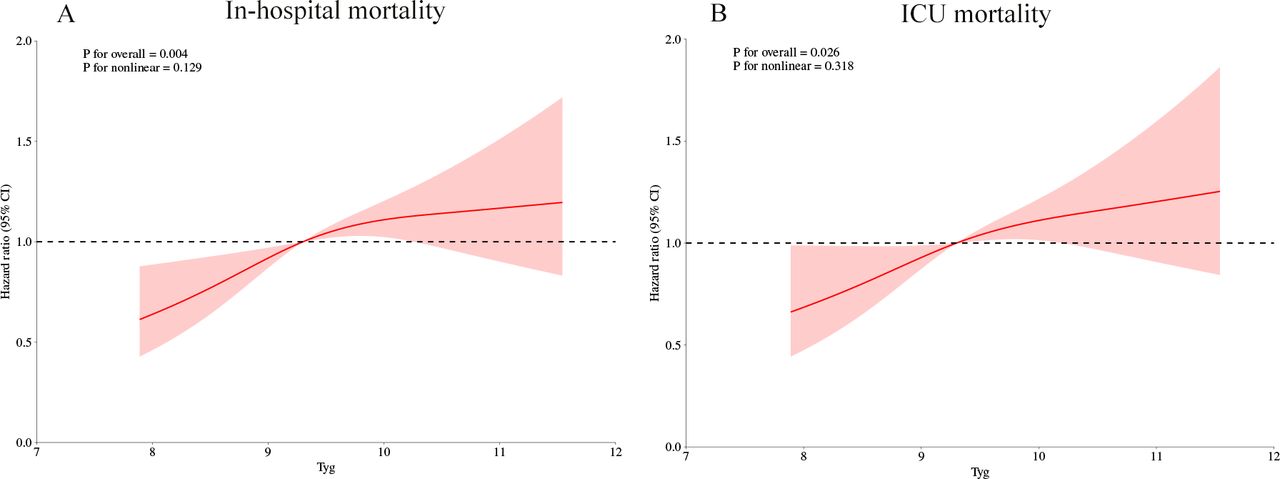
Online supplemental table S4 shows that multivariate logistic regression analysis indicates that the TyG index is independently associated with an increased risk of in-hospital mortality (OR 1.23 (95% CI 1.08 to 1.40); p=0.002). Table 2 uses the Cox proportional hazards analysis method to analyse the correlation between the TyG index and in-hospital mortality. The results show that when the TyG index is a continuous variable, it is a significant risk factor for in-hospital patient death in the unadjusted model (HR, 1.19 (95%CI 1.07 to 1.31) P<0.001), partially adjusted model (HR, 1.15 (95%CI 1.04 to 1.28) p=0.006) and fully adjusted model (HR, 1.14 (95%CI 1.02 to 1.27) p=0.023). When the TyG index is a categorical variable, in the four established COX proportional hazards models, the higher quartile group of early SA-AKI patients with a higher TyG index is significantly associated with a higher risk of in-hospital death: unadjusted model (HR, 1.54 (95%CI 1.20 to 1.98) P<0.001), partially adjusted model (HR, 1.46 (95%CI 1.12 to 1.91) p=0.005) and fully adjusted model (HR, 1.37 (95%CI 1.04 to 1.81) p=0.025). Similar results were observed in the multivariate COX proportional hazards analysis of the TyG index and ICU mortality (table 2). In addition, the restricted cubic spline regression model suggests that the risk of hospital mortality and ICU mortality increases linearly with the increase in the TyG index (nonlinear p=0.129 and nonlinear p=0.318, respectively) (figure 2A,B).
Supplemental material
Cox proportional hazard models for In-hospital and ICU all-cause mortality

Restricted cubic spline curves for TyG index and HR
ROC curve of TyG
The receiver operating characteristic (ROC) curve for the TyG index (online supplemental figure S1) was plotted to predict in-hospital mortality in SA-AKI patients. The area under the ROC curve (AUC) of TyG was 0.764 (95% CI: 0.740 to 0.788), indicating a reasonably good predictive performance of TyG.
Supplemental material
Subgroup analysis
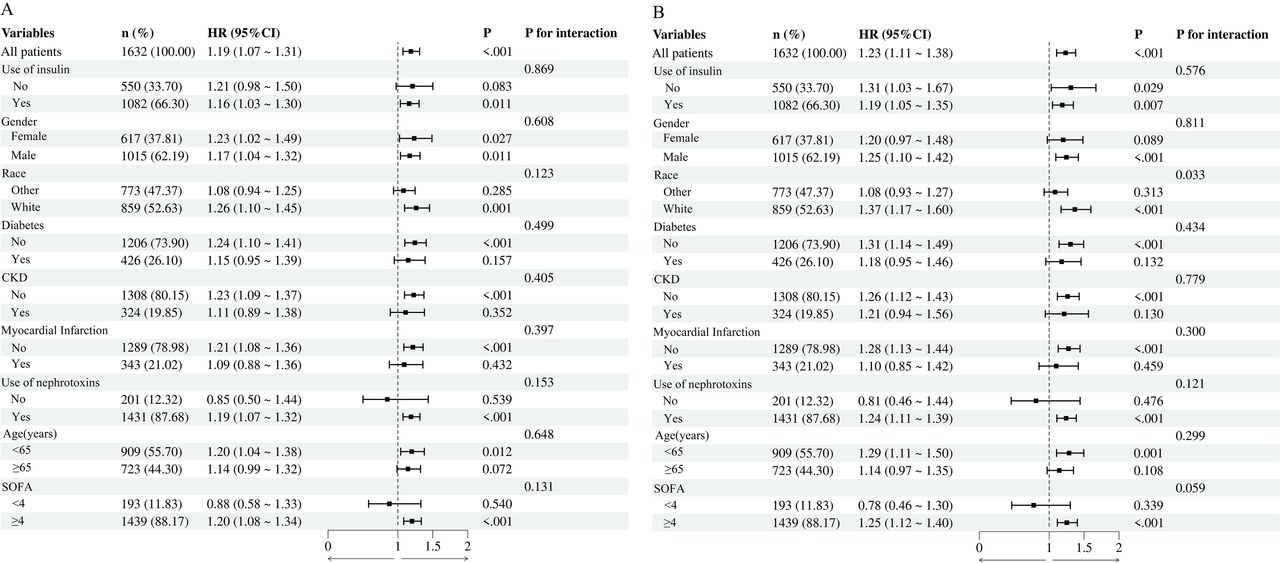
Additionally, to confirm the relationship between the TyG index and in-hospital and ICU mortality, subgroup analyses were conducted based on age, gender, race, SOFA score, history of CKD, use of nephrotoxic drugs and CHF. In figure 3A, the TyG index is significantly associated with in-hospital mortality in patients who are ≤65 years old (HR=1.19, 95%CI 1.04 to 1.37), Caucasian (HR=1.26, 95%CI 1.09 to 1.45), without CKD (HR=1.23, 95%CI 1.10 to 1.38), without diabetes (HR=1.24, 95%CI 1.10 to 1.41), without CHF (HR=1.22, 95%CI 1.09 to 1.37), using nephrotoxic drugs (HR=1.19, 95%CI 1.07 to 1.31) and with a SOFA score of >4 (HR=1.20, 95%CI 1.08 to 1.33). Additionally, the TyG index is significantly associated with in-hospital mortality in both male (HR=1.17, 95%CI 1.04 to 1.32) and female (HR=1.24, 95%CI 1.03 to 1.50) patients. In the subgroup analysis for the secondary outcome of ICU mortality, the results were consistent with the primary outcome in all respects, except for gender, indicating that the TyG index has similar correlations in most subgroups (figure 3B).

{kind=link}
{kind=link}
{kind=link}
Subgroup analyses for the association of TyG index with in-hospital mortality and ICU mortality.
Sensitivity analysis
Oline supplemental table S5 provides detailed results of the sensitivity analysis. After excluding patients with CKD, diabetes mellitus, using high-risk nephrotoxic agents, using high-risk nephrotoxic agents and those using insulin, the association between the TyG index and in-hospital mortality and ICU mortality among early SA-AKI patients remained stable. These results are consistent with the initial findings that included all patients.
Supplemental material
Discussion
In this study, we assessed the correlation between the TyG index and clinical outcomes in early SA-AKI patients based on the MIMIC database. We found a significant correlation between elevated TyG index and increased all-cause in-hospital mortality and ICU mortality in early SA-AKI patients. This association remained even after adjusting for various confounding factors. Therefore, the TyG index has potential value in assisting clinical physicians in making treatment decisions for early SA-AKI patients.
In recent years, the TyG index, as a novel surrogate marker for IR, has been proposed as a potential marker for the occurrence and progression of various disease types, including mainly atherosclerotic diseases, cardiovascular diseases and metabolic syndrome.25–28 Blood glucose levels hold significant prognostic importance in critically ill patients. Some studies have demonstrated that blood glucose levels are significantly correlated with in-hospital mortality in patients with cardiogenic shock.29 30 Furthermore, as research deepens, the relationship between the TyG index and sepsis has been widely discussed, with elevated TyG associated with the risk of sepsis across different population groups. For instance, a study by Xin Wang et al based on the eICU Collaborative Research Database (eICU-CRD) demonstrated that an elevated TyG index is independently associated with an increased risk of sepsis.31 In addition, some studies have shown that the TyG index can predict adverse outcomes in sepsis patients. A study by Rui Zheng et al, which included 1257 critically ill patients with sepsis, found that the risk of in-hospital and 28-day mortality in patients increased linearly with the increase in the TyG index.13 Moreover, a recent study indicated a non-linear increase in the relationship between the TyG index and 28-day mortality in non-diabetic critically ill sepsis patients.32
In the field of kidney disease, Yang Zewen et al found that a higher TyG index is linearly associated with an increased risk of AKI in patients with CHF.33 Another study indicated that the TyG index is non-linearly correlated with the risk of AKI in patients with acute myocardial infarction, with a 34.4% increase in the risk of AKI for every one-unit increase in TyG level.34 Furthermore, Liangjing Lv’s research team discovered that in critically ill patients, when the TyG index exceeds 10.014, the risk of mortality is positively correlated with the increase in the TyG index.35
Previous studies have shown that early SA-AKI is associated with a higher disease severity, a greater need for renal replacement therapy and a lower renal recovery rate at discharge.36 Moreover, the TyG index has been used as a predictor and risk-stratification tool for SA-AKI.20 However, to date, no study has clarified the relationship between the TyG index and the adverse outcomes of early SA-AKI. Our research results indicate a correlation between a high TyG index and adverse outcomes in SA-AKI. Current research shows that various mechanisms can lead to SA-AKI injury, including systemic and renal inflammation, complement activation, renin-angiotensin-aldosterone system (RAAS) dysregulation, mitochondrial dysfunction, metabolic reprogramming, microcirculatory dysfunction and macrocirculatory abnormalities. Several other processes may indirectly lead to SA-AKI, such as exposure to nephrotoxic drugs, hyperchloraemia and abdominal compartment syndrome.7 37 38 The TyG index is now considered a reliable and convenient indicator for evaluating IR, which has been widely confirmed to be closely related to endothelial dysfunction, oxidative stress, immune imbalance, coagulation imbalance and inflammatory responses, factors that are also closely related to the occurrence and progression of SA-AKI.11 39–41 Studies have shown that IR may lead to a reduction in nitric oxide (NO) synthesis and an increase in NO oxidative destruction, changes that could ultimately lead to the occurrence of endothelial cell dysfunction. At the same time, IR associated with oxidative stress may also cause glomerular endothelial cell injury, mesangial cell proliferation and basement membrane thickening.42 Additionally, IR may lead to elevated levels of catecholamines and dysregulation of pro-inflammatory and adipokines, which could result in chronic hypercatecholaminaemia and inflammation, thus adversely affecting kidney function.43 44 Furthermore, IR is closely associated with abnormal activation of the sympathetic nervous system and the RAAS, which could lead to increased levels of angiotensin II. Angiotensin II can increase systemic blood pressure, glomerular pressure and urinary albumin excretion, leading to early glomerular hyperfiltration and damage to the glomeruli during renal insufficiency.45 46
Our findings demonstrate a significant graded association between TyG index quartiles and multiorgan dysfunction severity. The progressive elevation of SOFA scores across TyG quartiles (7.0 (4.0–10.0) vs 10.0 (6.0–13.0), p<0.001) suggests a relationship between IR and systemic organ failure. This pattern aligns with three interrelated pathophysiological mechanisms: fFirst, elevated triglyceride levels promote ectopic lipid deposition in vital organs, particularly the liver and kidneys, disrupting cellular energy metabolism.47 Second, IR potentiates systemic inflammation through NLRP3 inflammasome activation, creating a pro-oxidative state that amplifies organ injury.48 This is corroborated by the parallel increase in NLR values across TyG quartiles (10.75 vs 12.43, p=0.008). Third, impaired glucose homeostasis directly compromises endothelial NO bioavailability, worsening microcirculatory perfusion in critically ill patients.49 Renal biomarkers also exhibited particularly significant trends: from Q1 to Q4, creatinine levels increased by 83% (1.2 mg/dL to 2.2 mg/dL) and BUN increased by 48% (23 mg/dL to 34 mg/dL), with both P values of <0.001. These changes suggest that the TyG index may serve as an early warning indicator for renal decompensation.
This study also conducted a further analysis of risk stratification in various subgroups. Our subgroup analysis indicated that the value of the TyG index in predicting in-hospital mortality in SA-AKI patients is consistent between male and female patients. Additionally, we found that a higher TyG index is associated with prognosis in SA-AKI patients under the age of 65 years, but not in those over 65 years, which contradicts our everyday understanding but is similar to the results of a previous study.50 The attenuated association between the TyG index and SA-AKI risk in patients aged >65 years may reflect fundamental differences in age-related metabolic homeostasis. Ageing induces a unique ‘IR paradox’ characterised by baseline elevation of HOMA-IR indices even in non-diabetic populations.51 This phenomenon arises from multifactorial mechanisms: (1) sarcopenia-driven glucose disposal impairment, age-related loss of skeletal muscle mass reduces insulin-sensitive tissue volume, leading to chronic compensatory hyperinsulinaemia that may mask acute TyG fluctuations52 53; (2) mitochondrial redox imbalance, elderly patients exhibit diminished peroxisome proliferator-activated receptor gamma coactivator 1α (PGC-1α) activity, impairing fatty acid β-oxidation and amplifying lipid accumulation independent of acute illness54; these intrinsic alterations likely diminish TyG’s discriminative capacity in elderly SA-AKI. Similarly, we did not find a connection between the TyG index and in-hospital all-cause mortality in patients with a history of CKD or heart failure at baseline. The reason for this phenomenon may be reverse causality: patients diagnosed with these comorbidities are more likely to receive appropriate treatment or adopt healthy lifestyle habits. Moreover, although studies have shown that CKD does not increase the risk of death from SA-AKI, considering that TyG may be related to CKD and patients with CKD are more likely to progress to SA-AKI, we still conducted a sensitivity test for this risk factor.55 The results showed that the association between the TyG index and in-hospital all-cause mortality in SA-AKI patients without CKD is consistent with the main findings. Even in non-diabetic patients, stress-induced hyperglycaemia in the ICU may lead to insulin use, which could directly alter glucose levels.56 Our study further demonstrates that a subset of non-diabetic patients underwent insulin therapy following ICU admission. However, sensitivity analysis confirmed the robustness of our findings. Subgroup analysis further revealed a stronger association between the TyG index and in-hospital mortality in the insulin-treated group. This phenomenon may be attributed to the inherently higher baseline risk in this patient population, such as more severe underlying conditions, heightened systemic inflammatory responses and greater metabolic demands.57 58 In this study, we meticulously accounted for the utilisation of an array of medications, such as high-risk nephrotoxins, diuretics, vasopressors and additional agents, which were integrated into our analytical framework.
Our study still has certain limitations. First, our analysis is retrospective and, thus, cannot fully avoid some inherent biases. Although we have designed strict statistical methods to produce robust and credible results, some confounding factors not included may still affect the outcomes. Second, we only used the baseline TyG index and could not assess how the temporal changes in this biomarker affect the correlation with cause-specific mortality, which is also a direction we will explore further in subsequent studies. Third, although the MIMIC-IV database provides a vast amount of patient data, the generalisability of the findings may be limited due to the data being sourced from a single medical centre. Future research should further validate these findings in multicentre and more diverse patient populations. Lastly, to validate our findings, prospective cohort studies are necessary.
Conclusion
Our study found a significant association between the TyG index and in-hospital all-cause mortality in early SA-AKI patients, suggesting that the TyG index could serve as a potential predictive marker for in-hospital mortality in early SA-AKI, thereby enhancing risk assessment and guiding subsequent interventions. Future studies should validate these findings through prospective designs with serial TyG measurements, particularly evaluating whether dynamic TyG trajectories enhance risk stratification beyond single baseline assessments.
Data availability statement
Data are available in a public, open access repository. The datasets generated and/or analysed during the current study are available in the MIMIC-IV repository, https://physionet.org/content/mimiciv/3.1/.
Ethics statements
Patient consent for publication
Ethics approval
This study utilized exclusively secondary data from publicly available sources. As no human participants were directly involved in the research and all analyzed data were fully anonymized, ethical approval was not required for this work.
References
Footnotes
CF and XL contributed equally.
Contributors JD participated in concept design, CF drafted an early version of this manuscript, and XL substantially revised it and ZZ coordinated the editing of later drafts and revisions. All authors have been involved in refining the protocol. The guarantor of this manuscript is JD, who takes responsibility for the integrity of the work as a whole, from inception to published article.
Funding The project has been funded by a Young Talent Support Project for the Development of Hospital Infection Discipline of the Chinese Preventive Medicine Association (CPMA-HAIC-20240129001).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.