Article Text

Abstract
Objective This study aims to synthesise evidence on the pooled level of exit knowledge among outpatients served in public hospital pharmacies and private pharmacies in Ethiopia and to identify the associated factors associated with medication knowledge by conducting a systematic review and meta-analysis of primary articles focused on this area.
Design This systematic review and meta-analysis study employed the GRADE (Grading of Recommendations Assessment, Development and Evaluation) approach.
Data sources Three electronic databases—MEDLINE, Scopus and Google Scholar—were searched for all English-language articles published from 2010 until 18 December 2024.
Eligibility criteria of selected studies The review exclusively included studies that reported original data, were freely accessible in full text and were written in English, as well as those investigating the level of knowledge among outpatients and associated factors, irrespective of study design. Studies lacking abstracts and full texts, reports, qualitative research, and conference summaries were excluded from the analysis.
Data extraction and synthesis Data from selected studies were extracted by three independent reviewers using a standardised data extraction format created using Microsoft Excel. Their results were cross-checked by two additional reviewers for consistency.
Results Of the 521 identified studies, 9 met the inclusion criteria. The overall pooled knowledge level was 45%. Factors associated with knowledge included residence (OR=0.67, 95% CI: 0.27 to 0.71), adequacy of information provided (OR=0.87, 95% CI: 0.24 to 0.90), education level (OR=0.70 CI: 0.39 to 0.89), clarity of instructions (OR=0.80 CI: 0.14 to 0.99) and pharmacist politeness (OR=0.72 CI: 0.46 to 0.77).
Conclusion The systematic review and meta-analysis showed that pooled patient knowledge regarding their dispensed medications in Ethiopia is about 45%. Key determinant factors of knowledge included education level, quality of pharmacist communication, urban versus rural residence and pharmacist politeness. Recommendations for improvement include enhancing pharmacist training, developing educational materials in local languages, outreach programmes for rural areas and implementing patient-centred care policies.
PROSPERO number: CRD42024560816
- Ethiopia
- Patients
- Drug Utilization
- Drug Therapy
- Health
- Health & safety
Data availability statement
All data relevant to the study are included in the article.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The strength of this study lies in its rigorous adherence to Preferred Reporting Items for Systematic Review and Meta-Analysis guidelines.
Inclusion of studies with diverse geographical locations within Ethiopia.
The limitation of this study, including heterogeneity among studies, was notable despite subgroup analyses and meta-regression attempts to explore sources.
Publication bias, evident from funnel plot asymmetry, may have affected results despite statistical adjustments.
The reliance on cross-sectional studies limits insights into temporal changes in knowledge levels.
Background
Rational use of drugs has become an important concern for the WHO and many countries in recent years.1 This is because the inappropriate use of medicines is a prevalent problem, particularly in developing countries.2 The irrational use of medications is often expressed in terms of polypharmacy, incorrect use of antibiotics, excessive use of injections, not following clinical guidelines when prescribing, inappropriate self-medication, including prescription drugs, and not sticking to prescribed dosages.3 A recent systematic review of primary studies in Ethiopia examined these different forms of drug misuse across various healthcare settings in the country. The study found that the prevalence of injectable drugs exceeding the WHO recommended standards was notably high, with Soddo Christian Hospital in the Southern Nations, Nationalities, and Peoples’ Region (SNNPR) having the highest rate at 57.2%, followed by Debremarkose referral hospital in the Amhara region at 48.36%. The review found that Bahir Dar Hospital in the Amhara region had the lowest percentage of drugs prescribed from the essential drugs list or formulary, at 81.4%, which is lower than a review of primary healthcare centres across 11 African countries, where 88.0% of prescribed drugs were from the essential drug list.4 Another systematic review study showed that the prevalence of self-medication is 44.0% with the highest being observed in Addis Ababa (62%).5
Previous studies also showed that factors that lead to irrational drug utilisation in Ethiopia were found to include pharmacists’ practices such as limited dispensing time, insufficient counselling and inadequate labelling.6 7 Another factor could be the physician–pharmacist relationship. A previous study in Jigjiga town, Ethiopia, reported that the collaboration between the physicians and pharmacists was suboptimal.8 Additionally, the educational and cultural backgrounds of patients, physical factors during dispensing like noise, the prevalence of comorbid conditions leading to polypharmacy and the lack of proper rational drug utilisation training for prescribers all play a role.5 9 10 These factors must be addressed as irrational drug utilisation could impose detrimental health and economic burdens on developing countries like Ethiopia. It may lead to drug resistance, longer periods of hospitalisation and increased morbidity and mortality.4 9 11
To prevent irrational drug utilisation, pharmacy professionals take the highest responsibility as they involve providing the right drug, dosage, quantity and package, to the right patient, along with clear instructions and counselling the patient regarding the administration and appropriate follow-up, although other health professionals including nurses and doctors, and the patient himself are also responsible.12 Addressing factors that impact the dispensing practices of pharmacists, such as communication barriers, dispensing facilities, high workloads and pharmacists’ skills, knowledge and dedication, is crucial to ensuring patients have sufficient knowledge about their prescribed medications.7 This is because successful management of a disease is possible when patients have a good understanding of their disease and its treatment.13 One of the factors contributing to medication errors and poor drug safety in patients is a lack of patient knowledge about their dispensed medications.14 Patient medication knowledge refers to the information that patients need to possess to properly use the medications that have been prescribed to them.15 This includes knowledge about the purpose of the medication, the dosage instructions, how to administer it, the expected duration of treatment, potential side effects, precautions to take, contraindications, interactions with other drugs and the effectiveness of the medication.16 Inadequate patient knowledge about their medications can lead to incorrect use, resulting in treatment failure and putting the patient’s health at risk.17 Furthermore, a lack of medication knowledge may cause unintentional overdosing or non-adherence to the prescribed regimen, ultimately leading to poor health outcomes for the patient.18 On the other hand, evidence from previous studies suggests that improved knowledge regarding their disease condition, drug regimen and potential side effects could positively impact patient disease control.19
Findings regarding patient understanding of medications provided in developing nations vary widely, likely due to differences in dispensing practice observed and varying literacy levels across different studies.18 Previous studies conducted in Ethiopia and other parts of the world have shown that various factors can determine a patient’s knowledge about their medication. These factors include the quality of communication between the doctor and patient,20 the interaction between the pharmacist and patient21 as well as the patient’s age,22 gender, education level,23 income, primary language24 and the nature of their illness.7 Despite this evidence, the pooled level of knowledge regarding their medications among ambulatory patients in Ethiopia is not known. Its predictor factors are also diverse across the studies, and their combined effect is not understood. So, by observing this gap, the objective of this systematic review and meta-analysis is to synthesise evidence on the pooled level of knowledge and the associated factors.
Methods
Design
This study adhered to the guidelines outlined in the Cochrane Handbook for Systematic Reviews of Interventions, and the results are reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.25 We conducted a meta-analysis on the systematic review, ensuring key conditions for validity and reliability were met. These include study homogeneity, availability of quantitative data, high study quality and the use of an appropriate statistical approach. The protocol for this review has been registered in advance with the International Prospective Register of Systematic Reviews (PROSPERO) under registration number CRD42024560816. It includes all studies investigating the level of knowledge among outpatients and its determinant factors with consideration of study design. The study’s inquiry was structured around the population (outpatients in Ethiopia), intervention (evaluating outpatient knowledge of dispensed medication at pharmacies), comparison groups (none) and outcome (patient knowledge about their dispensed medications, including dosage, administration, side effects and other relevant medication information) components and aimed to answer the question: ‘Which factors predict outpatients’ knowledge about their medications served both in public hospital pharmacies and private pharmacies?’
Search strategy
We searched three different electronic databases for all English-language articles published from 2010 until 18 December 2024. A comprehensive search strategy was carried out, employing three digital databases including MEDLINE, Scopus and Google Scholar. Searching terms for the technique were “level of knowledge”, “Dispensed medications”, “Medications”, “Associated factor”, “Predictor factor”, “Determinant factor” and “Outpatients”. The initial search strategy was adapted in the MEDLINE database by blending HeadingsMeSH (Medical Subject Headings) terms, text words and BOOLEAN operators (OR, AND). It was then adjusted for use in various databases between 15 September 2024 and 18 December 2024. Further information was gathered by consulting subject matter experts, reviewing pertinent literature and manually compiling a reference list of the selected papers.
Eligibility criteria
Inclusion criteria
The review exclusively included studies reporting original data, freely accessible in full text and written in English, and those investigating the level of knowledge among outpatients and associated factors, irrespective of study design.
Exclusion criteria
Studies lacking abstracts and full texts, reports, qualitative research and conference summaries were excluded from the analysis.
Study selection procedures
EndNote X9 citation manager was employed to import studies from various sources and eliminate duplicates. After removing duplicates, five reviewers (DG, TTA, GT, EG and GL) independently screened the inclusion of all potential studies identified through the search process based on the title and abstract. An additional six reviewers (DG, HSA, ANY, ATB, AAL and GAK) assessed the entire text of the papers to determine eligibility for inclusion in the study. Any discrepancies were resolved through discussion. Ultimately, all eligible papers with complete content underwent review.
Quality appraisal
The quality of these articles was assessed by four reviewers (DG, HSA, ANY and ATB) using a 14-item checklist derived from the criteria outlined in the National Institutes of Health (NIH) Quality Assessment Tool for Cohort, Cross-Sectional Studies and Case Series available at https://www-nhlbi-nih-gov.ezproxy.u-pec.fr/health-topics/ study-quality-assessment-tools. If an item was answered ‘NO’ or ‘UNCLEAR’, it received a score of ‘0’, while a response of ‘YES’ was scored as ‘1’. The overall quality score for each article was determined by summing the scores for all 14 evaluation criteria. Articles were classified as low quality if their scores ranged from 1 to 5, moderate quality between 6 and 10 and high quality if scores fell within the range of 11–14. Studies scoring 6 or more based on the NIH criteria were deemed good quality and included in the review. Any discrepancies in the quality assessment were resolved by consulting with the first author.
Data extraction process
Data from selected studies were extracted using a standardised data extraction format created using Microsoft Excel. The format included categories such as author details (name and year of publication), the town in which the study is conducted, pharmacy type, knowledge measuring tool used, medications about which knowledge is measured, dosage form, sample size, level of knowledge (%) and NIH score. Three independent reviewers (HSA, ANY and ATB) performed the data extraction, and their results were cross-checked by two additional reviewers (AAL and GAK) for consistency. In cases of discrepancies, the articles were thoroughly reviewed by the involvement of another two reviewers (EG and GL), and any disagreements were addressed through further discussion.
Operational definitions
Good knowledge: According to most of the studies included in this review,21–24 26 patients who respond correctly to at least two-thirds of knowledge-related questions are considered to have good knowledge.
Poor knowledge: According to most of the studies included in this review,21–24 26 patients who respond correctly to less than two-thirds of knowledge-related questions are considered to have poor knowledge.
High education: Patients who have a diploma or above are considered to have a higher education.
Low education: Patients having less than a diploma are considered to have low education.
Statistical analysis and data synthesis
After being retrieved using Microsoft Excel 2016, the data were exported to Stata V.17 for further analysis. A descriptive analysis and report on the features of the included studies’ summary tables and narrative text were completed. Forest plots were used to show the overall level of knowledge or effect sizes and to identify factors that may determine the observed patterns. The presence of heterogeneity between studies was checked by using the Cochrane Q statistics. This statistical heterogeneity between studies was examined using I2. Using a funnel plot and the statistical tests developed by Egger and Begg, the existence of publication bias was examined. The authors conducted a subgroup analysis to identify potential moderating factors that could explain the variations in effect sizes among the primary studies, based on characteristics such as sample size. Additionally, a meta-regression model was used to investigate the sources of heterogeneity, by considering factors like the study area and publication year of each included study. The p values reported for these analyses were calculated using Wald tests.
As the analysis revealed significant heterogeneity among the included studies, the pooled effects were estimated using a random-effects meta-analysis approach, as proposed by DerSimonian and Laird. To determine how each study affects the overall estimate of knowledge, we conducted a leave-one-out sensitivity analysis. This approach involves removing one study at a time and recalculating the estimate for each iteration.
The degree of certainty of the evidence for the outcome was assessed using the GRADE (Grading of Recommendations Assessment, Development and Evaluation) tool. Observational studies started with low-quality evidence, which could be downgraded to very low based on five factors: risk of bias, inconsistency, indirectness, imprecision and publication bias. Evaluations were performed for each domain, and the evidence quality was adjusted accordingly.
Patient and public involvement
Patients and the public were not involved in the design, conduct, reporting or dissemination of this systematic review and meta-analysis.
Results
Search outcomes
The databases of MEDLINE, Scopus and Google Scholar were used for a comprehensive search, resulting in the identification of 521 published papers until 18 December 2024. Following the elimination of duplicates across databases, 147 articles underwent screening. Among these, 119 articles were excluded based on irrelevant titles and abstracts. Further assessment resulted in the exclusion of 15 articles due to different settings, study time and methodology. The remaining 13 articles underwent quality appraisal, and 4 articles were excluded due to low quality as they were found to have less than a 6 NIH score. Finally, the review incorporated nine papers, three of which had moderate quality and six had high quality, meeting the inclusion criteria. The PRISMA diagram in figure 1 below illustrates the stepwise study selection procedure.

Diagram of study selection according to the Preferred Reporting Items for Systematic Review and Meta-Analysis guidelines.
Characteristics of included studies
Two of the studies in this systematic review and meta-analysis were done in Harar Town (Harari region),23 24 two in SNNPR,7 12 one in Adulala (Oromia region),27 one in Mekelle (Tigray region),21 one in Ambo (Oromia region),22 one in Bahir Dar city (Amhara region)26 and one in Jimma city (Oromia region).28 The sample sizes across 9 studies totalled 3493 individuals, with Jimma town having the largest sample size of 426 and Adulala the smallest with 302 participants. The highest level of knowledge of dispensed medications was observed in Mekelle, reaching 81%, while the smallest was in southwest Ethiopia, which is 13.2%. All studies employed a cross-sectional design and were conducted between 2014 and 2024 (see table 1 for detailed characteristics of the studies included in this review). The studies focused on patients’ knowledge regarding the medication’s name, dosage, administration frequency, administration route, treatment duration, potential side effects, possible interactions with other medicines or foods, proper storage conditions and what actions to take if a dose is missed.
Characteristics of the studies included in the systematic review and meta-analysis of level exit knowledge and associated factors among outpatients in Ethiopia (2014–2024)
Certainty of evidence
The certainty of evidence of the included studies was assessed using the GRADE approach. Given the nature of observational studies, the initial level of certainty in the evidence was rated as low. Several factors were considered in the assessment of the overall quality of the evidence. First, the risk of bias was considered serious, primarily due to the limited number of studies and the use of cross-sectional methods, which are inherently prone to bias. Second, inconsistency was also rated as serious, as there was significant heterogeneity observed among the included studies, suggesting variability in the results. On the other hand, the evidence did not exhibit indirectness, as all studies measured the outcome variable objectively and were directly relevant to the review question. Imprecision was also rated as not serious, given that the studies had adequate sample sizes and produced narrow CIs, indicating precise estimates. Furthermore, there was no indication of publication bias, as evidenced by the results of Egger’s and Begg’s tests. Considering all these domains, the overall certainty of the evidence was rated as low.
Meta-analysis
Pooled level of knowledge of dispensed medications
The combined knowledge of dispensed medications across the nine studies was 45%, with a 95% CI ranging from 28% to 63% using the random effect model. The forest plot in figure 2 below depicts the pooled level of knowledge.

Forest plot showing the pooled level of knowledge regarding dispensed medications among outpatients in Ethiopia.
Publication bias
A visual assessment of the funnel plot was conducted to explore publication bias, and the notable asymmetry observed suggests the presence of such bias. Furthermore, Egger’s and Begg’s tests were performed to provide an objective evaluation. Despite the funnel plot visual inspection showing asymmetry, inferring the presence of publication bias, Egger’s test (p=0.200) and Begg’s test (p=0.175) did not show publication bias. The funnel plot is shown below in figure 3.

Funnel plot showing the pooled level of knowledge regarding dispensed medications among outpatients in Ethiopia.
Subgroup analysis
Subgroup analysis was carried out based on the type of pharmacy, region and sample size as the studies showed the presence of heterogeneity identified by the I2-test (I2=95.62%, p<0.001). Subgroup analysis took the mean sample size (388) as a cut-off point. Studies with sample sizes below the mean of the combined sample sizes were classified as Group One, while those above the mean were classified as Group Two. The pooled level of knowledge was then assessed for each group. The analysis showed that the heterogeneity is not due to sample size difference, as the pooled level of knowledge in group one was 37.7% with a CI range of 8.8% to 84.2% and p=0.701. In comparison, that of group two was 47.6% with CI 28.1% to 67.1% and p=0.701. Further subgroup analysis was carried out to find out the source of heterogeneity, taking public pharmacies as group one and private pharmacies as group two. The result showed that the heterogeneity is not due to the type of pharmacy, as the pooled level of knowledge in group one was 50% (95% CI: 31 to 69%, p=0.287). In comparison, group two’s was 29% (95% CI: 3 to 62%, p=0.287). Subgroup analysis, treating studies from different regions as independent groups, revealed that the observed heterogeneity can be attributed to regional variations. The SNNPR region exhibited the lowest level of knowledge, at approximately 21% (95% CI: 3% to 37%, p=0.001). Studies conducted in the Amhara and Tigray regions were single studies. The overall results of subgroup analysis are presented in table 2 below.
Subgroup analysis of the level of knowledge about dispensed medications among outpatients in Ethiopia by region, sample size and pharmacy type of primary studies focused
Meta-regression and sensitivity analysis
Meta-regression
A random-effects meta-regression was conducted, considering sampling size and publication year as covariates. The results showed that neither sample size (p=0.692) nor publication year (p=0.134) significantly impacted the outcome. Further meta-regression based on region showed that the heterogeneity among the studies could be attributed to region differences in which studies were conducted (p=0.001). Table 3 presents the covariates, their beta-coefficients, 95% CI and p values.
Meta-regressions of the level of knowledge regarding dispensed medications among outpatients in Ethiopia
Sensitivity analysis
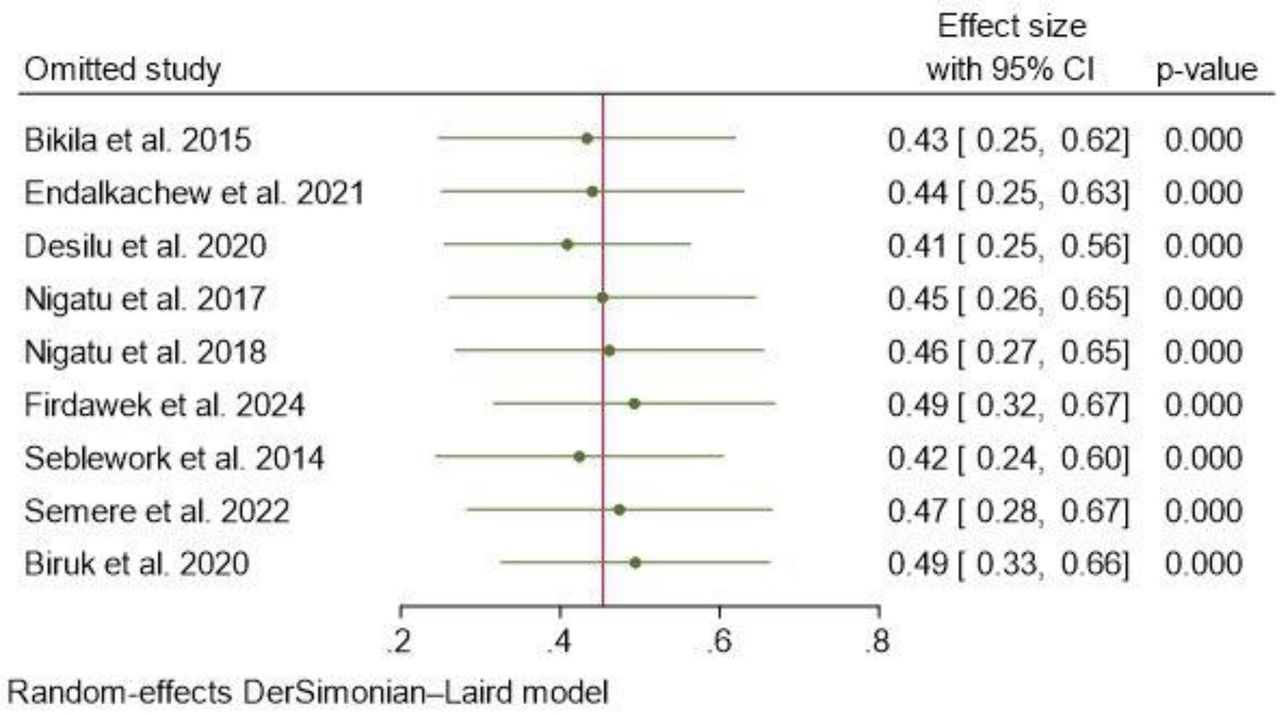
Results of the leave-one-out sensitivity analysis of the pooled exit knowledge for each excluded study remained within the CI (ranging between 41% and 49%) of the analysis that combined all the studies as presented in figure 4. This suggests that the overall estimate is robust and not significantly affected by any single study.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Results of a leave-one-out sensitivity analysis of the level of knowledge regarding dispensed medications among outpatients in Ethiopia.
Factors associated with the level of knowledge
Residence, the sufficiency of pharmacists’ information provided to patients, the patient’s education level, the clarity of pharmacist instruction to patients and the politeness of pharmacists were identified as factors significantly associated with the combined level of knowledge among outpatients served in public hospital pharmacies and private pharmacies.
The odds of having sufficient knowledge were about 32.7% (OR: 0.67, 95% CI: 0.27 to 0.71 p=0.03) lower for patients living in rural areas than those in urban areas. Those who got insufficient information had a 12.9% lower likelihood of having sufficient knowledge (OR: 0.87, 95% CI: 0.24 to 0.901, p<0.001) than those who received adequate information. Patients with lower education levels had 30.5% lower odds of having sufficient knowledge (OR: 0.70, 95% CI: 0.39 to 0.89, p=0.025) than those with higher education. Additionally, patients who did not receive clear instructions from pharmacists had 20.3% lower odds of having sufficient knowledge (OR: 0.80, 95% CI: 0.14 to 0.99, p=0.04) compared with those who did receive clear instructions. Lastly, patients served by pharmacists who did not respond politely had 27.8% lower odds of having sufficient knowledge (OR: 0.72, 95% CI: 0.46 to 0.77, p=0.029) than those served by polite pharmacists. Table 4 below summarises this.
The pooled ORs of factors associated with the level of knowledge
Discussion
This research used a systematic review and meta-analysis approach to analyse data from nine studies. The goal was to estimate the overall percentage of outpatients who had adequate knowledge regarding their dispensed medication in Ethiopia by analysing primary study results. This review showed that the combined level of knowledge among outpatients in Ethiopia regarding their dispensed medications is about 45%. This result is nearly in line with the study results in Nigeria and Lebanon, which showed that patients’ knowledge regarding their dispensed medications was 38.2% and 38.8%,15 29 respectively. These figures indicate that patients in these countries may share similar challenges in accessing information, understanding their medications and receiving adequate counselling from healthcare providers. In comparison, the study’s findings are higher than those reported in Australia, Gambia and Portugal, which were 28%, 16.1% and 17.5%,14 30 31 respectively. This disparity could be attributed to several factors. One key difference is the number of studies conducted in each country. In Ethiopia, nine studies were conducted regarding the current review title, which offers a more comprehensive picture of the knowledge level of outpatients, whereas the other nations have only one study each. Additionally, the timing of these studies may play a role, as most of the Ethiopian studies are recent, with five published after 2020. On the other hand, the studies in Australia, Gambia and Portugal were conducted several years earlier (2016, 2014 and 2015). Another critical factor creating the differences in results could be the dispensing practice. The dispensing time in the Gambia was reported to be 37 s,14 which is lower than the reported mean dispensing time in Ethiopia, (78 s).32 Dispensing time is an important indicator of how adequately pharmacists support patients. When this time is brief, pharmacists are likelier to leave the patient without providing sufficient information about their medications.
On the other hand, the result of this study was lower compared with studies conducted in India, Iran, Saudi Arabia and Botswana which showed the level of patients’ knowledge to be 95%, 63%, 69% and 62.5%,1 2 20 33 respectively. These differences in knowledge levels could stem from several factors. First, healthcare infrastructure plays a significant role; countries like India, Saudi Arabia and Iran may have more established healthcare systems, with better access to medical education, resources and patient counselling, which could contribute to higher levels of patient knowledge. Second, socioeconomic factors, such as income, education and public health initiatives, likely impact the ability of patients to access information about their medications. Third, cultural differences and neighbourhoods may also affect how health information is communicated and received in different regions. Countries with higher knowledge levels may have more effective health education programmes and public awareness campaigns. Finally, differences in study designs and methodologies, such as sample size, population characteristics and types of medications studied, might also account for the variations observed across countries. This comparison underscores the need for improved healthcare education and resources in Ethiopia to elevate patients’ understanding of their medications.
The subgroup analysis revealed that the significant heterogeneity observed in the pooled knowledge levels could be largely attributed to regional variations. The SNNPR region showed the lowest level of knowledge at approximately 21%, indicating a notable disparity in patient understanding of dispensed medications in this region. This low knowledge level may reflect challenges specific to the region, such as limited access to healthcare resources, lower health literacy or inadequate patient counselling. The regional differences highlight the need for targeted interventions to address knowledge gaps and improve medication understanding in areas with lower levels of education and healthcare access. However, still the high I2 statistics for Oromia, Harari and SNNPR suggest significant heterogeneity between the studies, indicating that the variation is largely due to factors beyond chance. This could be attributed to differences in study populations, methodologies, regional factors, interventions or statistical issues, all of which may contribute to the observed variability in the results.
Concerning the determining factors, educational status, the adequacy of information provided by pharmacists, the clarity of their instructions, residence and the politeness of the pharmacists were all found to influence the overall level of knowledge significantly. Patients in rural areas had approximately 32.7% lower odds of possessing adequate knowledge than those in urban areas. This aligns with study results in Ambo, Ethiopia and eastern Ethiopia.22 24 This may be because people living in rural areas often travel longer distances to access care, have limited availability of healthcare services and providers and visit healthcare providers less frequently than those in other regions.34 Their counterparts, urban residents, have easier access to healthcare professionals for guidance when they have questions regarding their medications, which could be another reason for the difference.35 The odds of having adequate knowledge among patients who perceive they did not get sufficient information from pharmacists were 12.9% lower than those who perceive they get sufficient information from pharmacists. This result agrees with study results in Nigeria, Pakistan and Iran.15 17 35 This could be due to patients having received sufficient verbal counselling and written instructions, which would help them have a better understanding of treatment failure, potential drug adverse effects, and improvements in self-management of drug regimens.
The odds of having adequate knowledge among patients who did not have formal education were 30.5% lower than those with higher education. This is a critical finding because individuals with lower educational levels may struggle with reading and comprehending complex medication information, which is often provided in English or other formal languages that they may not be fluent in. This result corroborated with previous studies in India, Ghana, Gujarat, Lebanon, Nigeria, Pakistan and Sri Lanka.13 17–20 29 36 37 This may be due to the difficulty in reading and comprehending drug information provided in English and understanding the pharmacist’s instructions.19 20 Furthermore, patients who perceive they did not receive clear instructions from pharmacists had 20.3% lower odds of having adequate knowledge than those who perceive they receive clear instructions from pharmacists. Ambiguity in instructions can create confusion and mistrust, making patients hesitant to follow their prescribed regimens. Patients may feel unsure about the correct dosage, timing or side effects, leading to poor adherence. This result agrees with previous study results in Mekelle, Ethiopia, Ambo, Ethiopia and eastern Ethiopia.21 22 24 This could be because patients who did not receive clear instructions could face ambiguity and lack of confidence. Lastly, patients who perceived being attended by pharmacists who were not polite had 27.8% lower odds of having adequate knowledge than those who perceived being served by polite pharmacists. This may be due to the patients’ reluctance to ask questions or seek clarification if they feel the pharmacist is unapproachable or dismissive. This result agrees with the results of the study in Pakistan. It could be due to the patient’s hesitation to seek clarification or ask further questions of the pharmacists because they feared being insulted.17 Among the determinant factors significantly associated with the level of knowledge in primary studies but not significantly associated with the pooled knowledge is sureness about the sufficiency of information they got. The discrepancy in the association between sureness about the sufficiency of information and patient knowledge in individual studies versus the pooled analysis could be due to several factors. Variability in measurement methods may lead to inconsistent results when combining data. Additionally, smaller sample sizes in individual studies might show stronger associations, while pooling larger, more diverse samples can reduce statistical power.
Recommendations
Based on the findings and implications of the research on patients’ knowledge regarding dispensed medications, here are some recommendations:
Enhance pharmacist-patient communication
This study result showed that patients who did not receive clear instructions from pharmacists had lower odds of having sufficient knowledge about their medications. To improve medication knowledge, pharmacists must develop and implement simplified, patient-centred discharge instructions focusing on key medication information, side effects and adherence tips. These instructions should be designed in clear, concise language, free from medical jargon and supported by visual aids where applicable, such as pictorial guides or infographics. The instructions should also include easily accessible follow-up resources, such as contact numbers for pharmacists and healthcare providers for any medication clarification.38
Educational initiatives
Patient education
This study showed that patients without formal education had lower odds of having adequate knowledge about their medications than those with higher education. To mitigate this knowledge gap, healthcare systems establish a structured patient education programme that focuses on improving medication utilisation by providing clear, tailored information about the medications, their purpose, potential side effects and the importance of consistent use. This programme should involve multiple communication channels, including face-to-face counselling, educational pamphlets, videos and digital tools.39
Address urban–rural disparities
The study showed that rural residents had lower odds of possessing sufficient medication knowledge compared with their urban counterparts. To address healthcare access issues in rural areas of Ethiopia, telemedicine and mobile health platforms can be used to provide remote consultations and medication guidance, which is particularly beneficial for rural patients who may have limited access to healthcare facilities.40 Moreover, we recommend training and deploying community health workers in rural areas to provide medication education and support, bridging the gap between healthcare facilities and remote populations.41
Regulatory standards
Implement and enforce regulatory standards that require pharmacists to provide comprehensive medication counselling to every patient. Ensure adherence to these standards through regular audits and evaluations.
Strengthen the legal and regulatory framework for community pharmacies
Improve and standardise the legal and regulatory framework for community pharmacies across Ethiopia to ensure consistent and high-quality pharmacy services. This should include clear guidelines on pharmacist-patient communication, medication counselling and patient education.42
Research and collaboration
Continued Research: Support further research to explore factors determining patient knowledge about medications, such as cultural factors, economic status, and health literacy.43
Technology integration
Mobile Applications: Develop mobile applications that provide medication reminders, dosage instructions and educational content tailored to individual patient needs.44
It may be better if stakeholders implement these recommendations to improve patients’ knowledge about their dispensed medications, enhancing medication adherence and ultimately contributing to better health outcomes across diverse healthcare settings.
Conclusion
In summary, the systematic review and meta-analysis found that the overall level of patient knowledge about their dispensed medications in Ethiopia was approximately 45%. This was generally higher than some other countries; but lower than several others. The key determinants of adequate patient knowledge were educational status, the quality of information and instructions provided by pharmacists, residence in urban versus rural areas and the politeness of pharmacists. Targeted interventions to improve patient medication knowledge could include (1) enhancing pharmacist training on effective patient communication and counselling techniques, (2) developing educational materials in local languages and promoting their use during pharmacy visits, (3) implementing outreach programmes to improve medication knowledge in rural areas and (4) instituting policies and monitoring to ensure pharmacists provide a high standard of patient-centred care. Addressing these modifiable factors could help increase the level of patient knowledge about their dispensed medications in Ethiopia.
Data availability statement
All data relevant to the study are included in the article.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
The authors would like to extend their special thanks to the primary studies researchers.
References
Footnotes
X @ttuog19@gmail.com
Contributors DG, EG, GAK, GL, TTA, GT, ANY and AAL searched and extracted the articles. EG, AAL, HSA and GAK checked the quality of the articles. DG, EG, ATB, GL and GAK did the analysis part and wrote the result. EG, GAK, ATB and GL reviewed the manuscript. DG, EG, GT, HSA and GL revised the manuscript. Finally, all authors gave approval of the version to be published; agreed on the journal to which the article had been submitted; and agreed to be accountable for all aspects of the work. DG is the guarantor for this manuscript. I (DG) used AI only for correction of grammar error.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.