Article Text

Abstract
Objective Diet and physical activity modifications are prescribed to women with polycystic ovary syndrome (PCOS). This study aimed to evaluate the correlation between physical activity and nutrition-related knowledge, attitudes and practices with obesity indices in young women with PCOS.
Design A cross-sectional study.
Setting Universities located in Shiraz.
Participants 308 young college women (age: 21.51±0.82 years, body mass index (BMI): 23.78±4.36 kg/m2) with PCOS who studied in several universities in Shiraz from February to August 2023 participated in the study voluntarily.
Methodology Participants filled out a modified Wellness Knowledge, Attitude and Behaviour Instrument, performed the step test to measure their maximum rate of oxygen consumption (VO2max), and their weight, height and waist circumference were measured to estimate their BMI and waist-to-height ratio (WHtR). Pearson product moment correlation and linear regression tests were used for data analysis.
Results No significant correlation was found between physical activity knowledge and both attitudes (r=0.014, p=0.804) and practices (r=0.49, p=0.399). However, a significant correlation was observed between physical activity attitudes and practices (r=0.125, p=0.028). In terms of nutrition, there were significant weak correlations between nutrition knowledge and attitude (r=0.228, p<0.001) as well as moderate correlations between nutrition attitude and practices (r=0.456, p<0.001), while no significant correlation was found between nutrition knowledge and practices (r=0.093, p=0.102). Additionally, significant negative weak correlations were noted between WHtR and VO2max (r=−0.178, p=0.003), and between BMI and VO2max (r=−0.211, p<0.001), while regression analysis indicated that VO2max is a stronger predictor of WHtR than physical activity practices and significantly predicts BMI.
Conclusion Nutrition and physical activity knowledge were not correlated with practices, while attitude was positively correlated with practices. VO2max demonstrated a stronger association with obesity indices compared with physical activity practices, although further research is warranted to confirm these findings.
- Health
- Physical Fitness
- NUTRITION & DIETETICS
- Attitude
- Knowledge
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available on request from the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The study examines the relationship between physical activity, nutrition knowledge, attitudes and practices with obesity indices in women with polycystic ovary syndrome (PCOS), providing data on an understudied population.
The use of maximal oxygen consumption as an objective measure of cardiorespiratory fitness strengthens the validity of the physical activity assessments.
Stringent eligibility criteria, including age restrictions (19–29 years) and health status, reduce confounding variables and enhance internal validity.
The cross-sectional design limits the ability to infer causal relationships between the studied variables.
Self-reported data on nutrition and physical activity may introduce bias, and the lack of a PCOS-specific questionnaire could affect measurement precision.
Introduction
Polycystic ovary syndrome (PCOS) is the most common endocrine reproductive disorder affecting 4–20% of women of reproductive age worldwide.1 Weight gain in patients with PCOS is linked to increased metabolic dysfunction, disruptions in menstrual periods, hormonal imbalances, ovulation issues, fertility problems and higher risks of diabetes, cardiovascular disease and cancer.2 3 Women with PCOS are prone to changes in eating habits and a sedentary lifestyle.4 Studies show that the risk of obesity in patients with PCOS is four times higher than in healthy individuals. Approximately 60% of women with PCOS are either overweight or obese due to a combination of genetic and epigenetic influences, mitochondrial dysfunction, alterations in protein and miRNA profiles, and environmental factors contributing to obesity.5 Research suggests that a 5–10% reduction in body weight can significantly reduce the complications of PCOS, but achieving this goal is often challenging due to various obstacles to weight loss and maintenance.6 Successful weight loss requires following a proper diet, avoiding inactivity and engaging in regular exercise.7
Despite the importance of nutrition and physical activity in managing PCOS, evidence indicates that women with PCOS generally have lower diet quality, poorer dietary intakes (higher cholesterol, lower magnesium and zinc) and lower levels of physical activity compared with women without PCOS.8 The reasons for these differences are not well understood based on available studies.
Recent research has shown that women’s knowledge, practices and attitudes significantly influence their body mass index (BMI) during reproductive years.9 Other studies have found associations between nutrition knowledge and attitude with nutrition practices in various populations, including Chinese adults10 and individuals with high-normal blood pressure.11 Additionally, studies have shown that while many working women in certain regions may have good basic nutrition knowledge and attitudes, they may not meet minimum dietary diversity score.12
In terms of physical activity, knowledge about the minimum frequency and duration needed to achieve health benefits is still lacking in some populations including educated persons.13 Sex-based differences in physical activity knowledge have also been observed.14 Poor physical activity knowledge has been identified as a barrier to physical activity practice among hospital staff.15 However, there is a lack of research on nutrition and physical activity, especially in women with PCOS. Therefore, this study aimed to assess the knowledge, attitudes and practices of nutrition and their association with BMI and waist-to-height ratio (WHtR) as obesity indices in young women with PCOS.
Methods
Study design and participants
The main objective of this study was to investigate the association between physical activity levels and nutrition-related knowledge, attitudes and practices with obesity indices in young women diagnosed with PCOS. Specific objectives included (1) assessing physical activity levels: to evaluate how these levels correlate with obesity indices; (2) evaluating physical activity related knowledge: to determine its relationship with physical activity attitude; (3) analysing attitudes towards physical activity: to explore how these attitudes may correlate with physical activity practices; (4) examining nutrition practices: to analyse their association with obesity indices; (5) assessing nutrition-related knowledge: to determine its relationship with nutrition attitude; (6) analysing attitudes towards nutrition: to find how these attitudes may correlate with nutrition practices.
This cross-sectional descriptive study was conducted in Shiraz, the capital city and fourth most populated city of Iran. To control the effect of age on the study variables, we selected our study subjects from university students. Participants of this study were 308 young collegiate female students aged 19–29 years selected by referring to different educational classes and dormitories at eight universities and explaining the study aims to students as well as through announcements. Inclusion criteria were: participation in a regular examination for their PCOS treatment in recent years, not suffering from any kind of cardiovascular disease or impairment that could impair their physical abilities and not being pregnant.
The sample size was calculated based on a similar study and proportion of girls affected with PCOS performed in Shiraz by Akbarzadeh et al.16 Using G*Power at 95% CI, a two-sided test, 5% significance level test (α=0.05) with 95% power, and correlation p H1 0.25, the required number of participants was estimated at 202. To prevent the effect of exclusions or dropouts during the performance, 308 participants were selected.
Anthropometric measurements
Sociodemographic data (age, race, education) were collected. The weight, height and waist of participants were measured in light clothing and barefoot position. Height and weight were measured using a digital stadiometer (Seca 284, Germany) to the nearest weight of 0.1 kg and height of 0.5 cm. BMI was calculated by weight (kg)/height (m)2. The waist circumference was measured at the level of the iliac crest using a flexible tape (made in Iran). Waist-to-height ratio (WHtR) was calculated through waist circumference (cm)/height (cm).
Physical activity and nutrition measurements
Participants completed demographic and physical activity/nutrition questionnaires under the supervision of the researcher. Demographic questions included 13 questions regarding age, education, ethnicity, economic status, health conditions (including any kind of current disease and treatment methods), marital status, number of children or previous pregnancies, weight loss methods (such as diet, supplement and exercise) and any physical problems affecting physical activity. Physical activity and nutrition were measured using the Persian version of the modified form of the Wellness Knowledge, Attitude and Behaviour Instrument (WKABI) originally developed and tested by Dinger, Watts and Barnes.17 The validity and reliability of the original questionnaire were previously confirmed by Woomer.18 The WKABI included 53 questions.
The original English version of the WKABI was translated into Persian by two independent bilingual translators who are fluent in both languages and familiar with the subject matter. The questionnaire was translated into Persian and back-translated into English to ensure linguistic accuracy. The Persian version of the questionnaire was reviewed and approved by five experts in nutrition, physical activity and public health to ensure item relevance and appropriateness for the target population. A pilot study was conducted with 30 university students to assess cultural relevance and comprehensibility. Feedback from participants led to minor adjustments in item wording to enhance clarity and contextual appropriateness. The mean internal consistency of the questionnaires of knowledge, attitude items of nutrition and physical activity categories was evaluated and approved (Cronbach’s alpha was 0.78).
Physical activity knowledge refers to participants’ understanding of concepts related to exercise, fitness and physical activity guidelines. This construct was assessed using 11 multiple-choice questions covering topics such as knowledge across various domains, including exercise types (aerobic and anaerobic), fitness goals (eg, flexibility, cardiorespiratory fitness, strength training) and practical recommendations (eg, target heart rate (HR), reducing soreness). They also emphasise understanding exercise intensity, health benefits and proper techniques for improving physical fitness. Each question had one correct answer and three distractors, and scoring was based on the total number of correct responses (maximum score=11). Nutrition knowledge refers to participants’ understanding of dietary principles, healthy eating guidelines and the relationship between diet and health. This construct was assessed using 13 multiple-choice questions covering topics such as calorie content, weight loss methods and the nutritional composition of foods. Topics covered the caloric content of fat, macronutrient contributions, protective factors against heart disease and osteoporosis, and behaviours for disease prevention. Each question had one correct answer and three distractors, and scoring was based on the total number of correct responses (maximum score=13).
Physical activity attitudes refer to individuals’ beliefs, feelings and perceptions regarding the importance, benefits and enjoyment of engaging in physical activity. These attitudes were assessed using six items scored on a 5-point Likert scale, where participants rated their agreement with statements about their views on the belief that exercise is beneficial for weight control, health maintenance, increased energy, stress reduction and improved self-esteem, contributing to overall well-being and longevity. Higher scores indicated more positive attitudes towards physical activity (maximum score=30 (6 items×5 points)). Nutrition attitudes were defined as individuals’ beliefs, feelings and perceptions regarding the importance, benefits and enjoyment of adhering to healthy eating habits. These attitudes were measured using five items scored on a 5-point Likert scale, where participants rated their agreement with statements about their views on nutrition concern and awareness about eating habits, the importance of nutrition labels, weight management, staying informed on nutrition information and the role of dietary supplements in dietary choices. Higher scores reflected more positive attitudes towards healthy eating (maximum score=25 (5 items×5 points)).
Physical activity practices refer to self-reported behaviours related to engagement in physical activities, or other forms of physical movement. Participants rated their agreement with statements about habitual physical activity on a 5-point Likert scale, covering domains such as recreational sports, stretching, strength training, weekend leisure activities and household/occupational tasks. Higher scores indicated more frequent or consistent engagement in physical activity behaviours (maximum score=45 (9 items×5 points)). Nutrition practices were defined as self-reported dietary behaviours, including food choices, meal patterns and adherence to healthy eating guidelines. Nutrition practices were assessed through self-reported behaviours, including health-based and taste-based food choices, fat intake moderation, label reading, fast food consumption and adherence to vegetable/fruit intake guidelines. The items also evaluated meal skipping due to work obligations and alignment with dietary pyramid recommendations. Higher scores reflected healthier or more consistent dietary behaviours (maximum score=45 (9 items×5 points)).
Scores for each construct were categorised into three levels: high, moderate and low, based on the 33rd and 66th percentiles. Scores falling within the top 33% of the distribution were categorised as high, those between the 33rd and 66th percentiles as moderate, and those in the bottom 33% as low.
Maximal oxygen consumption assessment
A step test was used to measure Maximal oxygen consumption (VO2max) due to its feasibility in any gymnasium and the ability of participants with similar conditions and diseases to perform it.19 A 3-min step test was conducted using a 42-cm (16.25 inches high) step. Participants performed 22 complete steps per minute regulated by a metronome set at 88 beats per minute. The test was performed after a brief demonstration and practice by participants. Immediately after completing the test, the participant’s pulse rate was measured in a standing position for 15 s by the researcher and converted to beats per minute (15 s HR×4). The following equation was used to predict VO2max (mL×kg−1×min−1) from the step test pulse rate (ST pulse).
VO2max = 65.81 − (0.1847 − ST pulse (beat × min−1)).20
Statistical analysis
Descriptive statistics (mean, SD and frequency) were used to present variables. The Kolmogorov-Smirnov test assessed data distribution normality. Due to the normal distribution of findings, the Pearson product moment correlation (two-tailed) test was used to examine relationships between knowledge, attitude and practices scores. Regression models were constructed to evaluate the relationships, and collinearity statistics (variance inflation factor (VIF) and tolerance) were checked to ensure model validity. Linear regression analysis evaluated the relationship between nutrition practices, physical activity practices and VO2max with BMI and WHtR. An alpha level of p<0.05 was considered statistically significant. Data analysis was performed using SPSS (V.26.0) software.
Patient and public involvement
No patients and/or the public were involved in the design, conduction, reporting or dissemination of this research.
Results
Description of the study subjects
Out of 460 young women diagnosed with PCOS who volunteered for this study, 308 met the inclusion criteria. The study included 308 young female college students, aged 19–29 years (18–19 years: 13%, 20–21 years: 34.7%, 22–25 years: 38.3% and 26–30 years: 14%). In terms of the education level, participants held bachelor’s degrees (71.4%), master’s degrees (20.1%) and doctorate’s degrees (8.4%) in various fields excluding sports sciences, medical sciences and nutrition sciences due to potential influence of their academic knowledge on responses. Considering economic status or family income, they were ranked as: very low (0%), low (1.6%), average (71.8%), high (22.4%), very high (4.2%). The majority of participants (85.4%) were single with the minority (14.6%) being married.
Considering participants’ BMI (kg/m2), 9.7% were underweight (BMI<18.5), 55.2% were normal weight (BMI: 18.5–24.9), 24% were overweight (BMI: 25.0–29.9) and 8.8% were obese (BMI>30).
Regarding physical activity knowledge, most participants (55.4%) demonstrated low knowledge, while 23.4% and 21.2% had moderate and high knowledge, respectively. Similarly, low nutrition knowledge was prevalent (49.2%), with 22.0% demonstrating moderate and 28.8% high knowledge. In terms of physical activity attitude, a larger proportion of participants exhibited a high attitude (40.3%) compared with low (36.0%) and moderate (23.7%) attitudes. Conversely, for nutrition attitude, most participants had a low attitude (43.8%), while 33.5% had a high attitude and 22.7% a moderate attitude. Physical activity practices were more evenly distributed: 34.4% (low), 37.3% (moderate) and 28.3% (high). Nutrition practices showed a similar distribution: 34.1% (low), 34.7% (moderate) and 31.2% (high).
In terms of VO2max (mL/kg/min), participants were classified as 0% poor (VO2max≤23.9), 0.6% fair (VO2max: 24–30.9), 55.2% average (VO2max: 31–38.9), 35.7% good (VO2max: 39–48.9) and 0% excellent (VO2max: ≥50). Their frequency of regular aerobic exercise participation varied, with some as always (9.4%), usually (17.5%), sometimes (26.9%), seldom (23.4%) and never (22.7%).
VO2max could only be estimated for 282 participants as some did not meet the required criteria for the test due to reasons such as inability to follow the test rhythm (n=3), fatigue (n=4), pain during performance (knee, back or other n=5) or unwillingness to participate in the test (n=14). Detailed descriptions of participants and study variables are presented in table 1.
Description of participants and variables
Physical activity
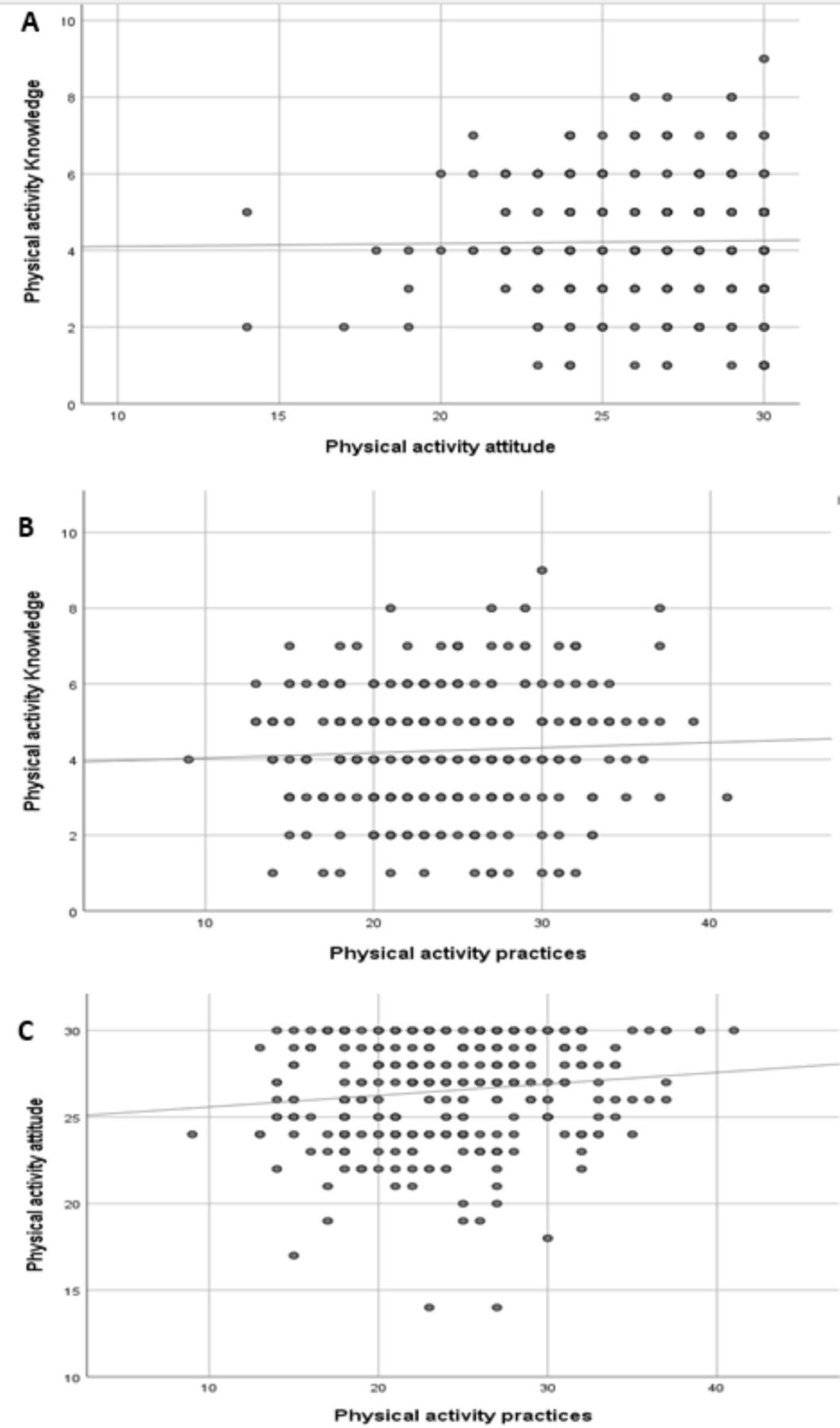
Based on the questionnaire information regarding physical activity knowledge, attitude and practices, as shown in figure 1, the study’s findings revealed no significant correlation between physical activity knowledge and physical activity attitude (r=0.014, p=0.804) or physical activity practices (r=0.49, p=0.399). However, a significant correlation was found between physical activity attitude and practices (r=0.125, p=0.028). Partial analysis of this study indicated a significant, positive and weak correlation between Vo2max and physical activity practices (p=0.03, r=0.176).

Correlation between physical activity knowledge, attitude and practices.
Nutrition
Regarding nutrition, the findings in figure 2 showed a significant weak correlation between nutrition knowledge and attitude (r=0.228, p<0.001) as well as significant moderate correlations between nutrition attitude and practices (r=0.456, p<0.001). There was no significant correlation between nutrition knowledge and practices (r=0.093, p=0.102).

{kind=link}
{kind=link}
Correlation between nutrition knowledge, attitude and practices.
Prediction of body mass index and waist-to-height ratio
Regression models were constructed to evaluate the relationships, and collinearity statistics (VIF and tolerance) were checked to ensure model validity. The regression analysis yielded the following collinearity statistics and regression coefficients across four models for BMI and WHtR.
Collinearity statistics revealed that all VIF values remained below 2.8, and tolerance values were acceptable, confirming that multicollinearity was not a concern in any of the models, thus validating the stability of the regression analyses.
Body mass index
Model 1 established that VO2max was a significant predictor of BMI (p=0.001, β=−0.193), indicating a strong negative relationship whereby increased cardiovascular fitness is linked to lower BMI. The model demonstrated an adjusted R² of 0.044, suggesting that approximately 4.4% of the variance in BMI can be explained by VO2max alone. Physical activity practices approached significance (p=0.094, β=−0.110), while nutrition practices did not show a significant relationship (p=0.371, β=0.057) (see online supplemental etable 2).
Supplemental material
In Model 2, VO2max remained a significant predictor (p=0.001, β=−0.193), reaffirming its role in predicting BMI. Physical activity practices continued to trend towards significance (p=0.103, β=−0.108), and nutrition practices remained non-significant (p=0.384, β=0.056). Additionally, age was not found to significantly predict BMI (p=0.906, β=0.007) (see online supplemental etable 2).
Model 3 reiterated the significance of VO2max (p=0.001, β=−0.194), while physical activity practices approached significance (p=0.079, β=−0.117) and nutrition practices remained non-significant (p=0.358, β=0.059). The education level was also found to be non-significant regarding BMI (p=0.522, β=−0.038) (see online supplemental etable 2).
Finally, Model 4 confirmed the significance of VO2max (p=0.001, β=−0.192) and noted physical activity practices trending towards significance (p=0.102, β=−0.108), while nutrition practices and economic status remained non-significant predictors (p=0.378, β=0.057; p=0.785, β=0.016, respectively) (see online supplemental etable 2).
Waist-to-height ratio
The regression analyses for WHtR were similar to those conducted for BMI. In Model 1, VO2max was again a significant predictor (p=0.009, β=−0.156), indicating a negative relationship with WHtR. The model yielded an adjusted R² of 0.046, highlighting that approximately 4.6% of the variance in WHtR is accounted for by VO2max. Physical activity practices approached significance (p=0.051, β=−0.128), while nutrition practices did not show significant predictive value (p=0.674, β=0.027) (see online supplemental etable 3).
Supplemental material
In subsequent models, Model 2, Model 3 and Model 4 consistently confirmed the significance of VO2max (p values of 0.009, 0.009 and 0.011, respectively). Physical activity practices approached significance in Models 2 (p=0.062) and Model 3 (p=0.044), indicating a potential beneficial effect on WHtR. However, nutrition practices and the confounding factors of age, education and economic status were not significant across all models, indicating the need for further investigation into these relationships (see online supplemental etable 3).
Discussion
The aim of this study was to examine the relationships between knowledge, attitude and practices of lifestyle (nutrition and physical activity) with obesity indices and VO2 max in young women with PCOS. The findings revealed no significant correlation between physical activity knowledge and physical activity attitude and practices. However, there was a significant correlation between physical activity attitude and practices. Additionally, there was a significant correlation between nutrition knowledge and attitude as well as between nutrition attitude and practices, but not between nutrition knowledge and practices. Furthermore, a significant negative correlation was observed between WHtR and VO2max and physical activity. The negative correlations between VO2max and BMI and WHtR reflect small-to-medium effect sizes. These findings suggest that cardiorespiratory fitness has a modest but clinically relevant correlation with body composition in women with PCOS. No significant correlation was found between WHtR as well as BMI with nutrition practices and between physical activity and BMI.
The significant relationship between VO2max with BMI and WHtR found in this analysis supports the hypothesis that cardiovascular fitness is a crucial factor in body weight regulation. As VO2max increases, BMI tends to decrease, suggesting that interventions aimed at improving cardiovascular fitness could effectively promote weight management.
Although physical activity practices showed a promising trend towards significance, further research is warranted to explore specific types and intensities of physical activity that may influence BMI more directly. Interestingly, nutrition practices did not significantly contribute to BMI and WHtR prediction, suggesting that the assessment methods may need refinement or that other dietary factors may play a more critical role.
To the best of our knowledge, this is the first study to investigate the relationship between knowledge, attitude and practices of nutrition and physical activity with obesity indices (BMI and WHtR) and Vo2max in collegiate aged females with PCOS. Descriptive study of physical activity and nutrition knowledge, attitude and practices revealed a notable discrepancy between knowledge, attitudes and practices related to physical activity and nutrition among young women with PCOS. While a majority of participants demonstrated low-to-moderate knowledge in both domains, attitudes toward physical activity were more positive compared with nutrition, where low attitudes predominated. Practices for both physical activity and nutrition were relatively evenly distributed across low, moderate and high levels, suggesting that despite suboptimal knowledge and mixed attitudes, some participants engaged in healthier behaviours. These results highlight the need for targeted interventions to bridge the gap between knowledge and practices, as well as to foster positive attitudes, particularly in nutrition, to improve health outcomes in this population.
A significant but weak correlation was observed between physical activity attitudes and practices representing a small effect size. This suggests that while positive attitudes towards physical activity may encourage engagement, other factors likely play a larger role in determining physical activity behaviours. A weak but significant correlation was found between nutrition knowledge and attitudes, indicating a small effect size. This suggests that higher nutrition knowledge is modestly associated with more positive attitudes towards healthy eating.
A moderate correlation was observed between nutrition attitudes and practices, representing a medium effect size. This indicates that positive attitudes towards nutrition are significantly associated with healthier dietary behaviours. This also suggests that to improve physical activity and nutrition practices, knowledge alone is not sufficient and attitude must also be addressed.
A previous study found a significant correlation between knowledge, attitude and practices in reproductive-age women in marginalised areas in Sri Lanka.9 In contrast, a pilot study with athletes indicated that nutrition knowledge predicted dietary practices.21 The disparity between our findings and those of the mentioned studies may be attributed to the education level of the participants. Our study participants were college students with similar academic backgrounds, potentially limiting the correlation between knowledge and practices. The relationship between knowledge, attitude and practices is often analysed in public health and social science research. Effective factors that influence this relationship include: education, cultural beliefs and norms, socioeconomic status, access to information, personal experience, social support, psychological factors, motivation, self-efficacy and health literacy.22–26
In addition, factors like culture, exercise facilities, motives and barriers may have a stronger relationship with physical activity practices compared with knowledge and attitude. A previous study identified several common motivations for engaging in physical activity and sports, including health benefits, overall well-being, enjoyment, social interaction and support from others. Conversely, prevalent obstacles have been noted including time constraints, fatigue, low energy levels, financial limitations, health issues, lack of motivation and adequate facilities.27 Health status can also influence physical activity practices,28 which may be another cause of differences between present and previous findings.
Other findings of the study were related to obesity indices, indicating a significant negative correlation between WHtR and VO2max (as an index of physical activity) as well as WHtR and physical activity. VO2max and physical activity, by priority, were the most important predictor of WHtR while VO2max was the only predictor of BMI. The participants had an average BMI of 23.78±4.367 kg/m2 and a healthy WHtR of 0.456±0.0570.29 55.2% of participants had an average VO2max (31–38.9), while 35.7% had good VO2max (39–48.9). 45% of participants had higher physical activity practices levels than the mean score (24.00±5.660). According to a study, there was a low association between VO2max and physical activity when adjusted for age and body fat percentage.30 However, we found a high association between VO2max and physical activity (r=−0.177, p=0.001). Therefore, VO2max emerged as the most significant predictor of obesity indices, reflecting its role as an indicator of daily physical activity and related physiological adaptations. Nutritional practices were not significant predictors of obesity indices. VO2max can be influenced by various aspects of physical activities, including daily activities, sports and recreational activities, as well as genetics. Regular participation in aerobic exercise varied among participants: always (9.4%), usually (17.5%), sometimes (26.9%), seldom (23.4%) and never (22.7%).
No studies were found regarding the correlation of cardiorespiratory fitness or VO2max with obesity indices in patients with PCOS. While a study reported a reduction in cardiorespiratory fitness in patients with PCOS,31 our study showed that participants had a VO2max of 38.319±3.407(mL/kg/min) which is within the normal range for their age group and sex. Several studies have explored the effects of exercise training on obesity and anthropometric indices in women with PCOS. A recent meta-analysis review suggested that regular exercise could improve cardiorespiratory fitness and waist circumference in women with PCOS.32 Another study indicated that high-intensity interval training and continuous moderate-intensity training could benefit some anthropometric indices and aerobic capacity in patients with PCOS.33 Additionally, the aerobic exercise programme was found to reduce BMI in women with PCOS.34
Reducing obesity is possible through two methods: dietary modification and increased energy expenditure (ie, exercise). In this study, energy expenditure and physical activity were found to be correlated with obesity indices. Similar to our findings, previous research has shown that low physical activity levels can predict abdominal fat in individuals of all weight categories.35 Controversies between our findings and similar studies may be attributed to differences in physical activity intensity. For example, one study found that regular aerobic exercise can slightly decrease waist circumference and visceral adipose tissue, while high-intensity exercise may offer more benefits compared with moderate intensity.36
Nutrition practices were identified as a potential factor affecting obesity indices. We found that 49% of participants reported higher nutrition practices compared with the mean score (27.17±4.59). In contrast to our findings, a recent study suggested that adherence to recommended diets was associated with lower central fat accumulation in women with PCOS.37 Another study indicated that planning a diet programme and changing eating habits played a significant role in reducing BMI in obese patients with PCOS.38 Differences in study design, such as interventional or descriptive mode, may contribute to varying results. Similar to our findings, a study by Bruner et al found no significant differences in body weight or BMI following nutritional counselling.39 The lack of correlation between nutrition practice and anthropometric indices in our study may also be due to the participants’ similar diets, as they were all university students who consumed similar foods from the university restaurant.
Generally, in some obese women with PCOS, the progression of PCOS may be influenced by indirect mechanisms such as depression, reduced self-control and increased distress. These factors could decrease motivation to change lifestyle habits, including nutrition or physical activity leading to weight gain.40 Additionally, this study employed a cross-sectional design, which may be subject to various confounding factors that could influence our findings. Therefore, future interventional studies that more precisely control for nutritional and physical activity variables are recommended.
Our study had several strengths, including the evaluation of knowledge and attitude factors affecting physical activity and nutrition practices. We also assessed the relationship between physical activity and VO2max with obesity indices which can be influenced by lifestyle and genetic factors. These findings can be valuable for health policymakers, working with PCOS.
We acknowledge that the cross-sectional design of this study limits our ability to account for all potential confounding variables such as dietary intake, hormonal status and stress levels. Future research should consider incorporating the following elements. Additionally, the relatively small number of participants was due to the requirement of participants to undergo a stair test to measure cardiorespiratory fitness, limiting the sample size. Furthermore, the homogeneity of participants being university students may have impacted the generalisability of our findings due to similar nutrition and physical activity knowledge and habits among the participants. Potential for self-report bias in responding to questions may also influence findings. In addition, we used a general questionnaire to measure physical activity and nutrition knowledge and attitudes. It is recommended to provide a specific questionnaire for patients with PCOS in future studies. While the WKABI provided a broad assessment of adherence to healthy eating guidelines, it did not capture specific details about food choices, portion sizes or nutrient intake. This may have limited our ability to fully assess the impact of nutrition on obesity indices. Future studies should incorporate more comprehensive dietary assessment tools to explore the relationship between nutrition practices and obesity indices in greater detail.
Conclusions
We found no significant correlation between physical activity knowledge and attitudes or practices, but a positive correlation between physical activity attitudes and practices was evident, indicating that positive attitudes may encourage greater physical activity engagement. Thus, educational programmes with a focus on attitude and behavioural change must replace the traditional programme. For nutrition, significant weak correlations were found between nutrition knowledge and attitudes, along with moderate correlations between attitudes and practices. However, there was no direct relationship between nutrition knowledge and practices, suggesting that knowledge alone may not be enough to correlate with dietary behaviour. VO2max was identified as a significant predictor of both BMI and WHtR, reinforcing its important role in body composition. While physical activity practices showed potential associations, more research is needed to explore nutrition practices and the influence of other confounding factors such as psychological and detailed diet status. This study emphasises the importance of understanding the complex interactions between physical activity, nutrition and cardiovascular fitness and advocates for further research, especially as intervention or causal relationship research to enhance health promotion strategies. Also, considering that participants of this study were collegiate young women, extrapolating these findings to other subgroups must be done with caution.
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available on request from the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Shiraz University ethics committee, ID number: IR.US.PSYEDU.REC.1402.005. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We appreciate all participants and assistants who contributed to the study and universities for permitting us to perform the study.
Footnotes
Contributors MKJ and RH designed the research. MKJ supervised the study and RH performed it. RH provided the first draft of manuscript and MKJ revised it. MKJ performed statistical analysis. FE consulted in its methodology. All the authors reviewed and approved the final revision. MKJ is guarantor of this study.
Funding This work was supported by Shiraz University (postgraduate student grant, number: 1GCB2M1899).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.