Article Text

Abstract
Objectives Subanaesthetic doses of esketamine may attenuate the opioid-induced cough reflex and prevent intraoperative haemodynamic fluctuations. This study aims to evaluate the effect of subanaesthetic doses of esketamine on the quality of recovery in patients who underwent abdominal surgery.
Design Retrospective cohort study using propensity score matching (PSM) methodology.
Setting A tertiary academic hospital.
Participants Patients who underwent abdominal surgery under general anaesthesia with tracheal intubation between 20 December 2022 and 30 April 2023, were retrospectively reviewed. Patients were assigned to the esketamine or control group based on whether they received a subanaesthetic dose of esketamine.
Primary and secondary outcome measures The primary outcome was extubation time (T1). Secondary outcomes included post-anaesthesia care unit (PACU) observation time (T2), total PACU time (T3), postoperative pain at multiple time points and adverse events including respiratory depression, hypertension and others.
Results A total of 2177 patients underwent abdominal surgery. After PSM, 1196 patients were analysed, 598 in each group. Esketamine significantly reduced the extubation time compared with the control group (20.00 vs 23.00 min, p=0.001). Total PACU time was shorter in the esketamine group than in the control group (62 vs 66 min, p=0.015), although PACU observation time did not show a significant difference. Compared with the control group, the esketamine group had a lower incidence of severe postoperative pain immediately after extubation (0.33% vs 2.01%, p=0.007) and respiratory depression (2.68% vs 5.35%, p=0.027), but a higher incidence of hypertension (9.53% vs 6.35%, p=0.042). There were no other significant differences in adverse events between the two groups.
Conclusions The use of subanaesthetic doses of esketamine for induction of anaesthesia in patients undergoing abdominal surgery may shorten the extubation time and reduce the incidence of postoperative complications.
Trial registration number ChiCTR2300072154.
- ANAESTHETICS
- Adult anaesthesia
- Adverse events
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
Propensity score matching was used to minimise selection bias and to balance baseline characteristics between the groups of patients with and without esketamine.
A relatively large sample size from a real clinical setting was included, which increased the generalisability of the results.
As a single-centre retrospective study, the generalisability of the findings may be limited.
Residual confounding from unmeasured variables may still be present, potentially affecting the results of the propensity score analysis.
Sensitivity analysis was not performed, which may affect the robustness of the findings regarding residual confounding.
Introduction
Approximately 313 million people worldwide undergo surgery each year, and general anaesthesia with tracheal intubation is the most commonly used anaesthetic technique.1 2 Advances in medical technology have significantly reduced anaesthesia-related mortality rates.3 However, this approach can still lead to adverse events, such as intubation cough, intraoperative haemodynamic fluctuations, postoperative pain and postoperative cognitive dysfunction.4–7 These reactions can prolong hospital stay and increase healthcare costs. Therefore, improving the efficacy and comfort of general anaesthesia with tracheal intubation has become a pressing concern.
Esketamine is a modified version of the anaesthetic ketamine that acts primarily by inhibiting the N-methyl-D-aspartate (NMDA) receptor, resulting in sedative and analgesic effects. Compared with ketamine, esketamine has a higher potency, stronger analgesic and sedative effects, and fewer side effects.8 9 Previous research indicates that subanaesthetic doses of esketamine, administered intravenously at 0.1–0.3 mg/kg or by infusion at 0.1–0.3 mg/kg·h can effectively reduce cough reflexes caused by opioid induction,10 prevent intraoperative haemodynamic fluctuations11 and reduce the need for intraoperative propofol and opioid medications.12 13 However, it remains unclear whether subanaesthetic doses of esketamine in general anaesthesia affect patient recovery and the incidence of postoperative delirium and agitation.14 15
This study retrospectively analyses the effect of subanaesthetic doses of esketamine used for intubation of general anaesthesia on recovery quality, postoperative pain and adverse events in patients undergoing abdominal surgery. The objective is to provide clinical evidence regarding the effect of esketamine on recovery quality for abdominal surgery patients. Propensity score matching (PSM) was used to adjust pairs of patients with and without esketamine for potential confounders.
Methods
Study design and patient population
This retrospective, single-centre study was conducted at the First Affiliated Hospital, Zhejiang University School of Medicine (Hangzhou, China). It was registered in the Chinese Clinical Trial Registry (www.chictr.org.cn, ChiCTR2300072154, 05/06/2023). The medical records used in this study were obtained from the medical database of the First Affiliated Hospital, Zhejiang University School of Medicine.
From 20 December 2022 to 30 April 2023, patients who had abdominal surgery under general anaesthesia with tracheal intubation were included in the study. Inclusion criteria included an American Society of Anesthesiologists (ASA) physical status of I to III and concurrent routine induction (sufentanil) with or without a subanaesthetic dose of esketamine for general anaesthesia. Exclusion criteria were age <18 years or >80 years, hepatic or renal dysfunction, severe pulmonary disease, severe cardiac dysfunction (New York Heart Association Classification 3–4), central nervous system disorders, psychiatric disorders, severe preoperative anaemia, intraoperative bleeding ≥500 mL or severe intraoperative haemodynamic fluctuations with markedly unstable vital signs caused by massive bleeding, duration of surgery >240 min, postoperative intensive care unit admission and patients not transferred to the postanaesthesia care unit (PACU) after surgery.
Anaesthetic procedure
All patients underwent preoperative fasting. On admission to the operating room, patients were monitored with ECG, non-invasive upper arm blood pressure, pulse oxygen saturation (SpO2), respiratory rate, partial pressure of end-tidal carbon dioxide (PetCO2), body temperature and bispectral index. Invasive continuous arterial pressure monitoring and central venous pressure monitoring were performed as needed.
Patients in the control group received midazolam (0.04 mg/kg), propofol (1.0–2.0 mg/kg), rocuronium (0.6 mg/kg) and sufentanil (0.3–0.5 µg/kg). The esketamine group received subanaesthetic doses of esketamine (0.2 mg/kg) in addition to the above induction agents. During surgery, 0.8–1.5 minimum alveolar concentration sevoflurane, 4–6 mg/kg·h propofol and 0.1–0.3 µg/kg·min remifentanil were maintained. After surgery, 4 mg ondansetron and 50 mg flurbiprofen axeyil were administered intravenously. Postoperative analgesia was achieved with 0.375% ropivacaine for nerve block (transversus abdominis plane block, TAP) or local wound infiltration anaesthesia.
Patients were transferred to the PACU after surgery, and endotracheal tubes were removed as soon as certain criteria were met (patients were awake, respiration rate >10 breaths per minute and tidal volume >5 mL/kg). Inadequate muscle strength was treated with 0.04 mg/kg neostigmine and 0.02 mg/kg atropine intravenously. Supplemental oxygen at a rate of 2 L/min was administered via nasal catheter after extubation. Pain was assessed using the Numeric Rating Scale (NRS) immediately, 15 min and 30 min after extubation. Hydromorphone (0.01 mg/kg) was administered for pain relief if the NRS score exceeded 4 points. A jaw thrust or positive pressure ventilation with a face mask was used to treat respiratory depression. For dysphoria or delirium, propofol 0.5 mg/kg was used for sedation. If hypertension is diagnosed, intravenous amlodipine 5 mg is recommended. If hypotension occurs, ephedrine 6 mg should be administered. If shivering occurs, intravenous tramadol 50 mg is recommended. Discharge from the PACU was assessed using the modified Aldrete score, with a score ≥9 indicating readiness for discharge.16 17
Data collection
Demographic and perioperative data were collected from the clinical information system (Seenew, Hangzhou, China) and institutional electronic Anaesthesia Data System (Medical System, Suzhou, China), including: (1) preoperative data: gender, age, body mass index (BMI), medical history, and ASA classification; (2) intraoperative data: type of surgery, surgery duration, anaesthesia duration, intraoperative blood loss and use of the patient-controlled analgesia (PCA); (3) PACU data: heart rate, blood pressure, oxygen saturation, extubation time, PACU observation time, the total PACU time, postoperative pain (NRS score), analgesic use, incidence of hypertension, hypotension and medication use. Additionally, the modified Aldrete score, respiratory depression, delirium and agitation, nausea/vomiting, shivering and other PACU adverse events (eg, reintubation) were recorded.
Primary outcome
The primary outcome was extubation time (T1), defined as the time from discontinuation of anaesthesia to extubation (minutes).
Secondary outcome
Secondary outcomes included postoperative pain immediately after extubation, at 15 min and at 30 min, and analgesic use. The modified Aldrete score at PACU discharge and the incidence of PACU adverse events including respiratory depression, hypertension, hypotension, delirium, agitation, nausea/vomiting, shivering, reintubation and use of symptomatic treatment were recorded.
Respiratory depression was defined as respiratory rate falling below eight breaths per minute or SpO2<90% for more than 1 min.18 19 In addition, the comparison of PACU observation time (T2), defined as the time from extubation to PACU discharge, total PACU time (T3), defined as the interval from PACU admission to discharge, and PACU discharge delay rate, defined as the percentage of patients with a PACU time greater than 120 min, were analysed.
Patient and public Involvement
Patients or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Propensity score matching
PSM analysis was performed using R Project for Statistical Computing (V. 4.2.3, Lucent Technologies, Reston, USA) and the matchIt package to reduce differences between the two groups based on the esketamine administration to minimise confounding factors. It is generally accepted that a standardised mean difference (SMD) of less than 0.1 for all variables indicates a good fit.20 For binary variables, the SMD is the difference in event rates between the treatment and control groups divided by the pooled SD, where the p is the weighted average of the event rates in both groups. For multicategory variables, the variable is split into several binary dummy variables, and the SMD is calculated separately for each dummy variable, taking the maximum absolute value. Nearest-neighbour matching method was used in a 1:1 ratio, with a calliper value of 0.05. Matching variables were selected based on prior literature where there was evidence of being potential confounders21 and included age, gender, BMI, chronic disease, ASA physical status classification, surgical category, surgery duration, anaesthesia duration, intraoperative blood loss and PCA use. The absolute SMDs are less than 0.1 for all variables. Multiple linear regression analysis was used to complete the matching process.
Statistical analysis
Sample size was calculated using PASS statistical software (NCSS LLC, Kaysville, USA). This was a retrospective case–control study. In the preliminary study, we included 20 patients in each group, and the mean extubation times for the two groups were 19.00±11.52 min and 22.15±14.42 min, respectively. A two-tailed test with α set at 0.05, 90% power and a sample size of 1:1 indicated that a minimum sample size of 361 participants per group was required. As PSM will be used for case selection, we included a larger sample size to ensure that the final number after PSM met the required threshold.
All quantitative data were assessed for normality using the Shapiro–Wilk test. Normally distributed continuous data were presented as mean (SD), and differences between groups were analysed using t-tests or analysis of variance (ANOVA). Skewed data were presented as median (25th–75th percentile) and were analysed using the nonparametric Mann–Whitney U test. Categorical data were analysed using the χ2 test or Fisher’s exact test. Ordinal data were analysed using the Wilcoxon rank-sum test. All statistical analyses were performed with the SPSS software 22.0 (IBM Corp., NY, USA). Statistical significance was defined as P <0.05.
Results
Demographic and patient characteristics
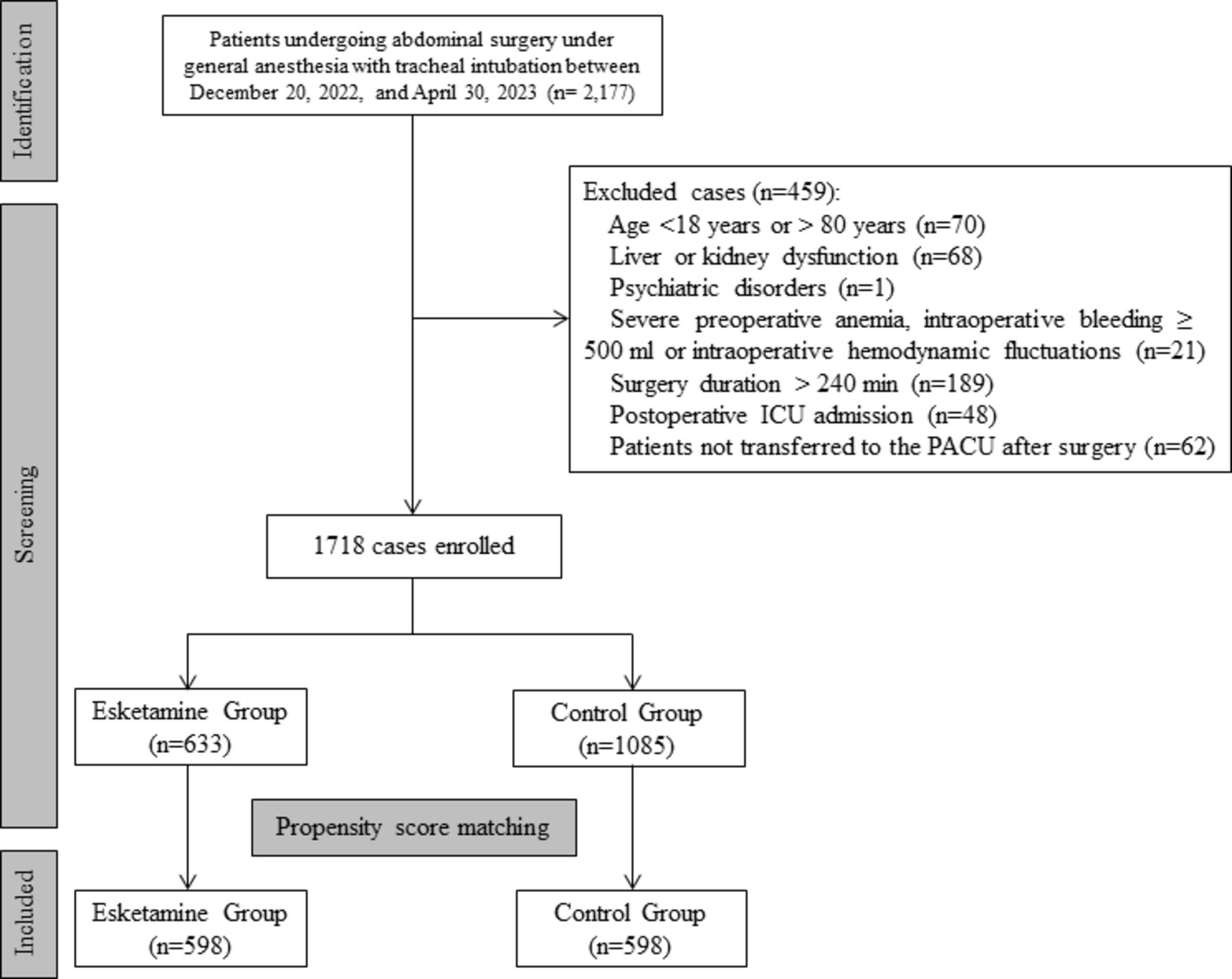
A total of 2177 patients with ASA physical status of I to III under sufentanil anaesthesia underwent abdominal surgery, including hepatobiliary, gastrointestinal and colorectal surgery, at the First Affiliated Hospital, Zhejiang University School of Medicine. Based on the inclusion and exclusion criteria, a final of 1718 patients were enrolled, with 633 patients in the esketamine group and 1085 patients in the control group. PSM successfully matched 598 patients in each group, achieving the required sample size (figure 1). The use of PSM ensured that the baseline characteristics were similar between the two groups (figure 2). The distribution of the propensity scores and the SMD of the covariates were well balanced after PSM adjustment (figure 3).

Flowchart of patient selection. ICU, intensive care unit; PACU, post-anaesthesia care unit.

Standardised mean differences (SMD) of covariates after propensity score matching. ASA, American Society of Anesthesiologists; BMI, body mass index; COPD, chronic obstructive pulmonary disease; PCA, patient controlled analgesia; PSM, propensity score matching.

{kind=link}
{kind=link}
{kind=link}
Distributions of propensity scores after propensity score matching.
Patient characteristics in the esketamine group and control groups before and after PSM are shown in table 1. After PSM, there were no significant differences (p>0.05) in the patient characteristics in gender, age, BMI, medical history, ASA classification, type of surgery, surgery duration, anaesthesia duration, intraoperative blood loss and use of the PCA between the two groups.
Comparison between the esketamine and control groups before and after propensity-score matching
Primary outcome
The results showed that the extubation time (T1) in the esketamine group was 20 (11, 32) minutes, while the T1 in the control group was 23 (13, 37) minutes (p=0.001), indicating that patients induced with subanaesthetic doses of esketamine had faster recovery in the PACU (table 2). Multiple linear regression suggests that ketamine is an independent protective factor for extubation time (online supplemental table 1).
Supplemental material
Recovery time after surgery.
Secondary outcome
The number of patients with severe postoperative pain immediately after extubation was significantly higher in the control group (12, 2.01%) than that in the esketamine groups (2, 0.33%) (p=0.007). In addition, the number of patients requiring additional hydromorphone for postoperative pain during PACU treatment was significantly higher in the control group (94, 15.72%) than in the esketamine group (70, 11.71%) (p=0.044). However, there were no statistically significant differences in the number of patients with postoperative pain between the two groups at 15 and 30 min after extubation, as shown in table 3.
Postoperative pain scores and analgesic requirements.
During the PACU period, the number of patients with respiratory depression in the control group was 32 (5.35%), significantly higher than the 16 (2.68%) cases in the esketamine group (p=0.027). The esketamine group had a significantly higher rate of hypertension than the control group (9.53% vs 6.35%, p=0.042). There were no significant differences in hypotension, delirium and agitation, nausea and vomiting, or shivering between the two groups. There were no emergencies requiring reintubation in either group. There were also no statistically significant differences in the modified Aldrete scores between the two groups when patients left the PACU (table 4).
Postoperative adverse events and the modified Aldrete score
In addition, the total PACU time (T3) was also shorter in the esketamine group (62.00 vs 66.00, p=0.015). However, there was no significant difference in the PACU observation time (T2) between the two groups, with median times of 38 min in the control group and 37 min in the esketamine group (p=0.738). The number of patients with delayed discharge from the PACU was 30 (5.02%) in the esketamine group and 38 (6.35%) in the control group, respectively (p=0.318) (table 2).
Discussion
The results of the current study indicate that the use of subanaesthetic doses of esketamine can effectively reduce the postoperative extubation time in the PACU for patients undergoing abdominal surgery. In addition, esketamine was found to reduce postoperative pain without increasing postextubation side effects.
Previously, it was thought that combining different mechanisms, such as esketamine with midazolam, propofol or sevoflurane, could deepen the level of anaesthesia and influence patient recovery.22 23 However, recent studies have shown that esketamine not only increases the depth of anaesthesia but also accelerates recovery from anaesthesia.24 Animal studies have shown that ketamine, the parent compound of esketamine, can shorten the peak activation time of the glutamatergic neurons, particularly those in the paraventricular thalamus, thereby reducing extubation time. Clinical studies have also shown that patients who received subanaesthetic doses of esketamine intraoperatively had faster and better recovery of postoperative respiratory rate and tidal volume.25 The current study supports these findings and suggests that the use of subanasthetic doses of esketamine may accelerate patient recovery.
This research shows that subanaesthetic doses of esketamine are effective in relieving immediate postextubation pain after extubation. Animal studies have suggested that the combining of NMDA receptor antagonists with opioids may result in synergistic or additive analgesic effects.26 Numerous clinical studies have supported this concept by demonstrating that administration of 0.15–0.5 mg/kg of esketamine reduces intraoperative opioid consumption and improves postoperative pain management.12 13 27 28 Consistent with these findings, the present study shows similar results. The subgroup that receiving subanaesthetic doses of esketamine reported significantly lower pain levels immediately after extubation. While there was no significant difference in pain scores between the two groups at 15 and 30 min postextubation, the PACU observation period showed a significant reduction in the number of patients in the esketamine group requiring additional analgesics for postoperative pain relief compared with the control group, indicating the beneficial effect of subanaesthetic doses of esketamine on overall postoperative pain relief. The major metabolite of esketamine is S-norketamine, which has approximately one-third the analgesic potency of esketamine and a longer elimination half-life. This may explain the prolonged analgesic effect of esketamine in the PACU.25
The results of this study indicate that the incidence of respiratory depression was significantly lower in the esketamine group than that in the control group. Respiratory depression is a common adverse event in the PACU, with an incidence rate of approximately 5%,18 which is similar to the incidence observed in the control group of this study. Causes of respiratory depression during the anaesthetic recovery period include the use of opioids, residual effects of muscle relaxants and the incomplete recovery of the respiratory system after surgery. It’s worth noting that approximately 20% of cases of respiratory depression are associated with the use of opioid medications.29 Elevated carbon dioxide (CO2) levels can stimulate central chemoreceptors, leading to an increase in respiratory drive. However, the use of opioid medications attenuates this response.30 Both animal and clinical studies have shown that ketamine can enhance CO2 sensitivity and provide moderate protection against respiratory depression and bronchoconstriction.31 32 Research by Jonkman et al also suggests that low-dose esketamine may counteract the respiratory depressant effects of opioid drugs.33 This suggests that the use of subanaesthetic doses of esketamine to induce anaesthesia may not only reduce opioid consumption but also stabilise respiration, thereby reducing the likelihood of fatal events.
The most common adverse events associated with esketamine primarily are psychological symptoms such as delirium, agitation, nightmares and dissociative phenomena, which often follow a dose-dependent pattern.34 35 Bornemann-Cimenti H et al have confirmed that subanaesthetic doses can reduce the incidence of psychological symptoms associated with esketamine.36 Our study supports this view and shows that subanaesthetic doses of esketamine do not increase the incidence of delirium or agitation. In addition, there is no effect on the incidence of nausea and vomiting. The sympathomimetic effects of esketamine manifest as increased blood pressure and heart rate.11 37 The incidence of hypertension was higher in the esketamine group than in the control group. This may be due to the increased blood pressure induced by esketamine.
The primary goal of the PACU is to improve turnover efficiency between surgical procedures and to increase patient satisfaction. Factors such as delirium, agitation and postoperative pain can prolong the PACU stay.38 However, the current study shows that the use of a subanaesthetic dose of esketamine doesn’t increase the incidence of these complications. Furthermore, the total PACU time for the esketamine group is shorter than that of the control group, suggesting that the use of esketamine may improve the efficiency of the PACU.
There are several limitations to this study. First, it is a single-centre, retrospective study, which may limit the generalisability of the findings. Although the two groups were matched on several demographic factors, there remains the potential for residual confounding due to unmeasured variables affecting the propensity score analysis. In addition, the lack of sensitivity analysis may affect the robustness of the results. Second, the dose of esketamine is subanaesthetic, and the study did not investigate potential problems associated with other doses. Finally, this study focuses exclusively on patients undergoing abdominal surgery and does not include other types of surgery. Therefore, further research should include large, multicentre, prospective studies to fully address these limitations.
Conclusions
Subanaesthetic doses of esketamine have been shown to be effective in reducing the extubation time in patients undergoing abdominal surgery under general endotracheal anaesthesia, without compromising the overall quality of recovery. In addition, the use of subanaesthetic doses of esketamine has the potential to reduce the incidence of severe postoperative pain, thereby reducing the need for analgesia in the PACU. This approach also helps to reduce the incidence of respiratory depression, resulting in a shorter overall PACU time, and ultimately contributing to the overall recovery process for patients.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the Clinical Research Ethics Committee of the First Affiliated Hospital, Zhejiang University School of Medicine (IIT20230403A) and registered in the Chinese Clinical Trial Registry (www.chictr.org.cn, ChiCTR2300072154).
References
Footnotes
Contributors DW, XF and YJ contributed to the study design. MW, KC, XW, YX, YW, MQ and ZL contributed to data acquisition. DW contributed to data analysis and drafting of the paper. XF and YJ contributed to manuscript revision. YJ contributed to final approval of the version. All authors read and approved the final version. YJ is the guarantor.
Funding This work was supported by the National Natural Science Foundation of China (82372159 and 82230074).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.