Article Text

Abstract
Objectives To investigate temporal trends in the geographical variation in oral anticoagulant (OAC) treatment of patients with atrial fibrillation, to evaluate the extent to which regional differences in patient populations may explain this difference and to explore whether patient predictors of adherence may have a different impact across regions.
Design Register-based cohort study from 1 January 2013 to 31 December 2022.
Setting The study used data from nationwide health registers to explore differences in OAC adherence across the five administrative regions in Denmark.
Participants Patients with atrial fibrillation and a CHA2DS2-VASc score ≥2 (n=291 666).
Outcome Population adherence to OAC treatment operationalised as the proportion of days covered (PDC).
Results A continuous rise in overall adherence (PDC) from 53% to 78% was observed during the study period. Concurrently, the predominant treatment shifted from vitamin K antagonists to direct OACs with a preference for rivaroxaban and apixaban. The adherence variation between the highest-performing and lowest-performing regions decreased from 18% in 2013 to 9% in 2022, whereas the relative between-regions rankings remained unchanged. Applying multivariate Poisson models adjusting for patient demographics, health status and socioeconomic factors did not substantially change the inter-regional variations; this suggests that different compositions of patient populations cannot explain these variations. However, the impact of socioeconomic factors and comorbidities among patients was unequal across regions. In regions with the lowest overall adherence, a higher risk of non-adherence was seen among patients having mental health disorders, low income and living alone.
Conclusions The geographical variation in OAC adherence decreased over time as the overall adherence improved. However, substantial variation remained.
- CARDIOLOGY
- Thromboembolism
- Medication Adherence
- EPIDEMIOLOGY
- Observational Study
- Quality in health care
Data availability statement
Data may be obtained from a third party and are not publicly available. The data used in this study are available to authorised research institutions through collaborative agreements. Access to the Danish registers is granted by Statistics Denmark and the Danish Health Data Authorities. More information can be found on the website of Statistics Denmark (www.dst.dk/en/TilSalg/Forskningsservice).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study presents comprehensive analyses of the impact of patient determinants on geographical variation in the adherence to oral anticoagulant therapy for atrial fibrillation.
The Danish national registers offer high-quality data with near-complete population coverage, and the systematic collection of real-world data provides valuable insights into treatment patterns and adherence reflecting actual clinical practices and patient behaviours.
Routinely collected data, however, are restricted to predefined parameters, meaning that key determinants of adherence may not be captured. Unmeasured variables, such as patient preferences and clinical decisions on anticoagulant therapy made in guideline grey areas, may contribute to residual confounding.
Dependence on administrative codes and electronic health records may introduce bias due to regional variations in IT systems or registration practices, which could have affected data consistency and comparability.
Introduction
Atrial fibrillation (AF) is the most common cardiac arrhythmia worldwide, and it is becoming increasingly prevalent due to the ageing population.1 Oral anticoagulant treatment (OAC) is essential to reduce the risk of stroke in patients with AF.2 3 However, despite the widespread guideline recommendation of using OAC for AF,4 5 approximately 20% of patients are still left untreated.6 7 This reveals a persistent gap between optimal care and real-world clinical practice, which holds a risk of potentially preventable strokes.
In healthcare, unwarranted variation refers to treatment differences driven by disparities in healthcare provider practice or healthcare system factors, rather than patient needs or preferences.8 Identifying unwarranted variation may uncover areas where clinical practice deviates from evidence-based guidelines, thereby providing valuable insights into potential inefficiencies or inequalities in care delivery.8–11 Denmark offers an ideal setting for such investigations due to its comprehensive nationwide healthcare registers12 that enable longitudinal analyses of OAC usage.
Geographical variation in OAC usage has been demonstrated across and within countries.13–20 In Denmark, geographical variation in OAC initiation and persistence has been demonstrated across municipalities16 and administrative regions.16 18 19 21 Additionally, a lower prevalence of ischaemic stroke, major bleeding and all-cause mortality has been observed in regions with high rates of OAC initiation with no corresponding increase in haemorrhagic stroke.16 18 This suggests that increasing OAC usage could enhance patient outcomes in low-use regions. Variations in OAC usage across the five Danish administrative regions have been shown to decrease as the overall OAC usage increases.21 Nevertheless, notable differences still exist, and the underlying drivers for this geographical variation remain poorly understood.
Factors at the patient, provider and healthcare system levels affect the adherence to OAC treatment guidelines.22 To better understand the clinical implications of the persisting geographical disparities, this study explores temporal trends and the current status of anticoagulant treatment variation in AF patients across Denmark and assesses how much of this variation can be explained by differences in patient health and socioeconomic status.
Methods
Design
We conducted a nationwide registry-based cohort study in Denmark from 1 January 2013 to 31 December 2022. To allow for analyses of temporal trends in OAC use, we established ten open cohorts including prevalent and incident patients with AF, each cohort representing a calendar year in the 10-year study period.
Data sources
The study was based on data records in the Danish national health registers from 2001 to 2022.12 Data on diagnoses and clinical procedures were obtained from the Danish National Patient Register (LPR), which holds continuously updated information on all contacts to the secondary healthcare sector.23 Information on redeemed prescriptions was extracted from the Danish National Prescription Registry (DNPR).24 Information on socioeconomic status and place of residence was obtained from the annually updated registers at Statistics Denmark.25 The data were linked at the individual level through the unique personal identification number in the Danish Civil Registration System,26 which also provided information on sex, vital status and migration for all Danish residents.
Study population
Inclusion criteria: The study included patients aged ≥18 years and an AF diagnosis recorded in the LPR (International Classification of Diseases (ICD)-10: DI48*, including all subdiagnoses). 5 years of consecutive residence in Denmark was required before inclusion to ensure comprehensive follow-up and data availability. Additionally, a CHA2DS2-VASc (congestive heart failure, hypertension, age 75+ years, diabetes mellitus, prior stroke or transient ischaemic attack or thromboembolism, vascular disease, age 65–74 years and female sex) score of ≥2 was required to ensure that all participants had an indication for OAC according to guideline recommendations4 (online supplemental table 1).
Supplemental material
Exclusion criteria: Participants were excluded from the study if undergoing a left atrial appendage closure procedure (OPCS-4: KFFW9*, including all subcategories). Although atrial appendage closure is not recommended in guidelines as a substitute for OAC, it is frequently offered to patients in or outside clinical trials when OAC is poorly tolerated.27
Within each calendar-year cohort, eligible participants were followed from 1 January, or from the first day of the calendar year on which they fulfilled all inclusion criteria, until reaching one of the following endpoints: undergoing a left atrial appendage closure procedure, death, emigration or 31 December of that year, whichever came first. Patients whose follow-up ended due to the conclusion of a calendar year were included in the cohort for the following year. Consequently, participants could be followed for a maximum of 10 years and be represented in up to 10 subcohorts.
Exposure
The exposure was the geographical area of residence, defined by the five administrative regions in Denmark. The regions are responsible for organising hospital care, general practice and specialised healthcare services.28 Each region serves as an administrative entity, allowing for potential regional variation in healthcare quality and access, which may influence OAC adherence. The exposure variable was operationalised as the participant’s region of residence on the day when entering the cohort and was updated annually on 1 January throughout the study period.
Outcome
The main outcome was OAC adherence defined as the proportion of days covered (PDC)29 with OAC. Adherence was assessed at the population level by comparing the total time covered by treatment with the total time at risk in a specified population.30 As the study populations comprised both prevalent and incident patients, this approach provided a composite measure of the three phases of adherence: initiation, implementation and persistence.29 31
Covariates
Participant demographics included age group, sex, country of origin, education, employment status, household income and cohabitation status (online supplemental table 2). The health status of the participants was assessed using the Danish Multimorbidity Index32 (online supplemental table 3). This index provided information on 38 long-term physical and mental conditions (AF was excluded from the original index).
Determining the PDC
OAC included medications approved for the prevention of stroke and systemic embolism in AF: vitamin K antagonists (VKAs), that is, warfarin and phenprocoumon, and direct OACs (DOACs), that is, edoxaban, rivaroxaban, apixaban and dabigatran. For DOACs, the daily dose was determined by multiplying the dose of the prescribed pill by the recommended number of daily dosages for the specific DOAC. For VKAs, we used the model developed by Skeppholm and Friberg33 to estimate age-adjusted and sex-adjusted daily dosage for each prescription.34 The duration of each redeemed prescription was determined by dividing the dispensed medication amount by the estimated daily dosage. All prescriptions were given a grace period of 20%, that is, the prescription duration was extended by 20% beyond the dispensed amount. Additionally, a stockpiling interval of 30 days permitted patients to carry over a maximum of a 30-day supply of medication from one prescription to the next.
The PDC was calculated by dividing the cumulated time covered by redeemed OAC prescriptions by the total time at risk in the relevant population.
Statistical analyses
Temporal trends in OAC adherence were assessed by determining the PDC by year and geographical region. Adherence rates were standardised by age group and sex and were presented graphically. Temporal trends in the use of OAC subgroups were evaluated by calculating the proportion of dispensed daily doses for each medication group relative to the total of dispensed daily doses. The distribution of OAC subgroups was evaluated annually at national level and stratified by region. The results were presented graphically.
We used multivariate Poisson regression models to examine the extent to which variations in patient sociodemographics and health status across geographical regions could explain any observed variance in OAC adherence. We constructed three models adding patient determinants of OAC adherence sequentially. Model 1 adjusted for sex and age. Model 2 also adjusted for health status using the Danish Multimorbidity Index32 (online supplemental table 3). Model 3 additionally adjusted for patient origin and socioeconomic status (online supplemental table 2). The three models were applied sequentially in the full study population, the 2013 cohort and the 2022 cohort, respectively, thereby providing incidence rate ratios (IRRs) of adherence between regions. All models accounted for time at risk. Robust 95% CIs were reported for analyses of individual subcohorts, while cluster-robust CIs were employed when subcohorts were combined. The fully adjusted model 3 was applied to each of the 10 subcohorts, thereby providing annual IRRs and robust 95% CIs of adherence between regions. The results were presented graphically.
We applied Poisson regression models, including region of residence as an interaction term, to assess whether the association between patient determinants and OAC adherence differed across geographical regions. The exposure variables included country of origin, household income, cohabitation, physical health status and mental health status. The exposure variables were derived from patient covariates (online supplemental tables 2 and 3). These variables were further collapsed into dichotomous categories (online supplemental table 4).
Separate models were applied for each exposure variable. All models adjusted for sex, age and the comorbidities defined in the Danish Multimorbidity Index.32 The model assessing physical health status adjusted only for mental health conditions. Similarly, the model assessing mental health status adjusted only for physical health conditions. Participants with unknown household income were excluded from the analysis of income effect (n=1261). Each model estimated the region-specific IRRs for OAC adherence by comparing the exposed group to the unexposed group within each region. A reference model without the interaction term for region was used to estimate the overall IRR across all regions. All estimates were presented with cluster robust 95% CIs and displayed in a forest plot. Wald tests were used to evaluate the interaction effects, and statistical significance was assessed at the 0.05 level.
Sensitivity analyses
We performed sensitivity analyses by applying 10% and 30% grace periods and allowing stockpiling for 0 and 60 days, respectively. When assessing regional interaction on income effect, we performed sensitivity analyses including the patients with unknown household income in the low-income to middle-income group and the high-income group, respectively.
All analyses were performed in Stata V.18.35 Results were reported according to the Strengthening the Reporting of Observational studies in Epidemiology guidelines.36
Patient and public involvement
No patients or public stakeholders were involved in the design, conduct or reporting of this study.
Results
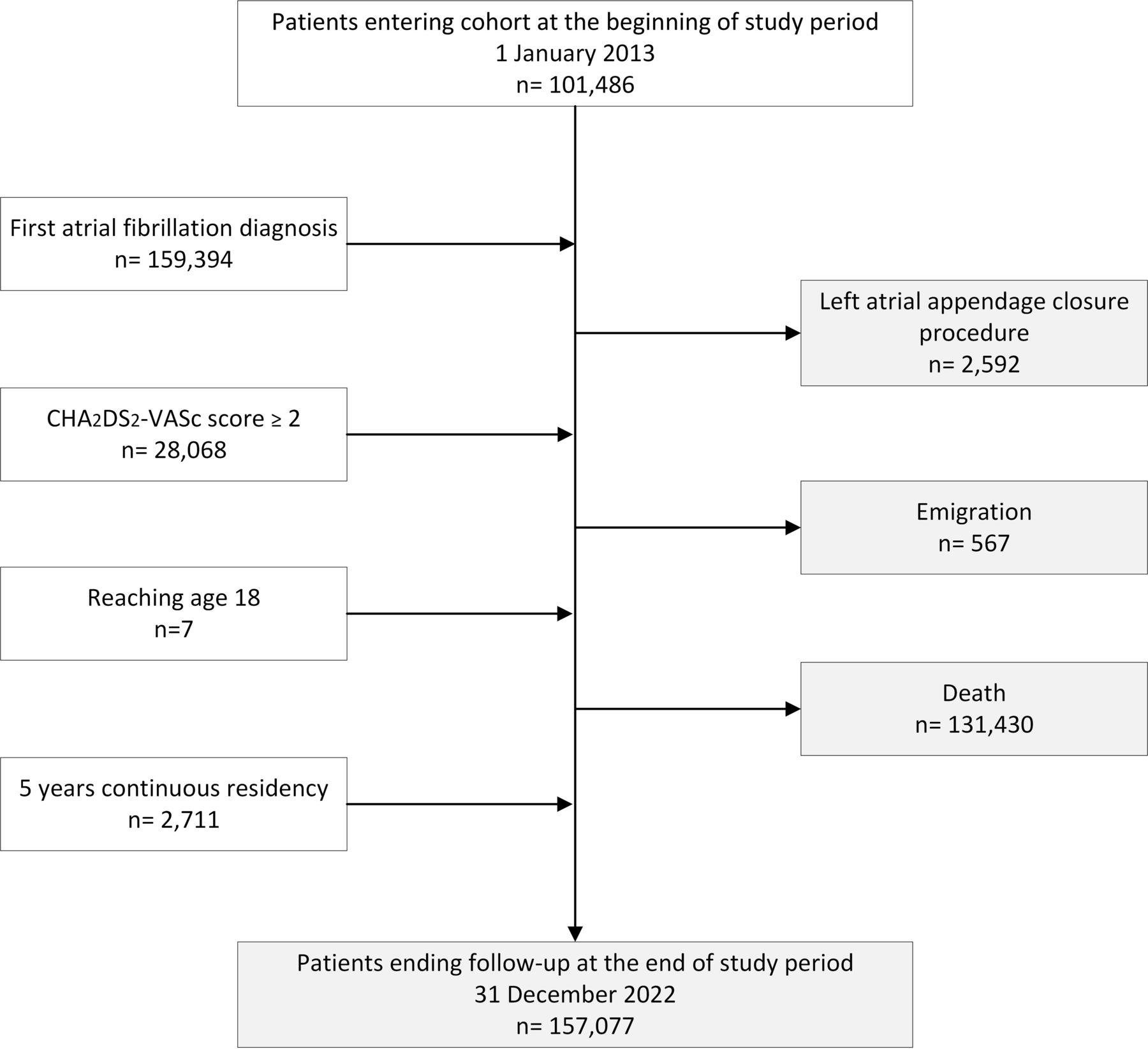
A total of 2 91 666 patients with AF were included in the study. Of these, 101 486 patients entered the study at the beginning of the study period on 1 January 2013, while 190 180 were included during the study period. 157 077 patients ended follow-up at the end of the study period on 31 December 2022, while 134 589 had left the cohort during follow-up due to death, left atrial appendage closure procedure or emigration (figure 1). The median follow-up time was 3.8 years (IQR 1.4–7.3).

Flow chart of the study cohort. Patients were included in the cohort on fulfilling all inclusion criteria: age ≥18 years, residing in Denmark for at least five consecutive years, diagnosed with atrial fibrillation and with a CHA2DS2-VASc score of ≥2. Patients were excluded if they had a history of left atrial appendage closure procedure. During the study period, patients entered the cohort once all inclusion criteria were met. The last criterion fulfilled is depicted in the flow chart. Patients were followed until they reached one of the following endpoints: undergoing a left atrial appendage closure procedure, death, emigration or end of study, whichever came first. The white boxes indicate patients entering the cohort, and the grey boxes indicate patients leaving the cohort.
Sociodemographic and health characteristics of the full cohort (2013–2022), the 2013 cohort and the 2022 cohort are presented in table 1.
Demographic and clinical characteristics of the study cohort
Temporal development in OAC treatment
During the study period, overall adherence to OAC therapy increased from 53.1% (95% CI 53.1% to 53.1%) in 2013 to 78.0% (95% CI 78.2% to 78.2%) in 2022 among patients with AF. Adherence improved throughout the study period across all regions, and the relative rankings of regional adherence levels remained stable (figure 2). In 2013, adherence ranged from 60.4% (95% CI 60.4% to 60.4%) in the highest-performing region to 50.4% (95% CI 50.4% to 50.4%) in the lowest-performing region, representing a regional difference of 10.0%. By 2022, these values had risen to 82.8% (95% CI 82.8% to 82.9%) and 75.3% (95% CI 75.3% to 75.3%), respectively, reducing the regional difference to 7.6%. Overall improvement and regional convergence in adherence were most pronounced during the early years of the study, with adherence showing signs of stabilisation in the later years (figure 2).

Temporal development in adherence to oral anticoagulant treatment in 2013–2022. Adherence to anticoagulant treatment by year for the full cohort and individual administrative regions, standardised by age and gender. PDC, proportion of days covered.
Concurrently, a substantial shift in anticoagulant usage was observed for patients with AF. In 2013, VKAs (primarily warfarin) accounted for 80.4% of usage, which had declined to 15.8% by 2022, with increasing usage of DOACs accounting for the remaining 84.2%. In 2013, DOAC usage was primarily driven by dabigatran which accounted for 14.5% of the total OAC usage. Rivaroxaban and apixaban showed the greatest increase during the study period; these drugs accounted for 32.2% and 40.4%, respectively, of the total anticoagulant usage in 2022 (figure 3A). Across regions, a largely parallel transition from VKA to DOAC was observed. However, DOACs accounted for a larger proportion of OAC use in the Capital Region of Denmark compared with the other regions throughout the study period. Additionally, the distribution of DOAC subtypes varied across regions. In all regions, the most frequently used DOACs were rivaroxaban and apixaban, though with a greater preference for rivaroxaban in the North Denmark Region and for apixaban in the Capital Region of Denmark and the Region of Southern Denmark (figure 3B).

Changes in usage of oral anticoagulants for atrial fibrillation in 2013–2022. Distribution of dispensed oral anticoagulant agents among patients with atrial fibrillation. Stacked-area plot shows the relative contribution of each subgroup by year. (A) Nationwide distribution; (B) regional distributions. OAC, oral anticoagulant treatment.
Regional variation in OAC adherence adjusted for differences in patient populations
Sequential adjustments for patient demographics, health status and socioeconomic factors had little impact on the regional adherence variation in the 2013 cohort, 2022 cohort and full cohort. The fully adjusted model 3 showed a slight convergence of IRRs and reduced regional variation. The greatest difference was observed in 2013, where adjustments for patient characteristics reduced the adherence gap between the highest-performing and lowest-performing regions from 21% to 18%. However, most estimates remained consistent despite adjustments for patient characteristics (table 2).
Impact of adjusting for patient characteristics on regional differences in adherence to oral anticoagulant therapy in Denmark
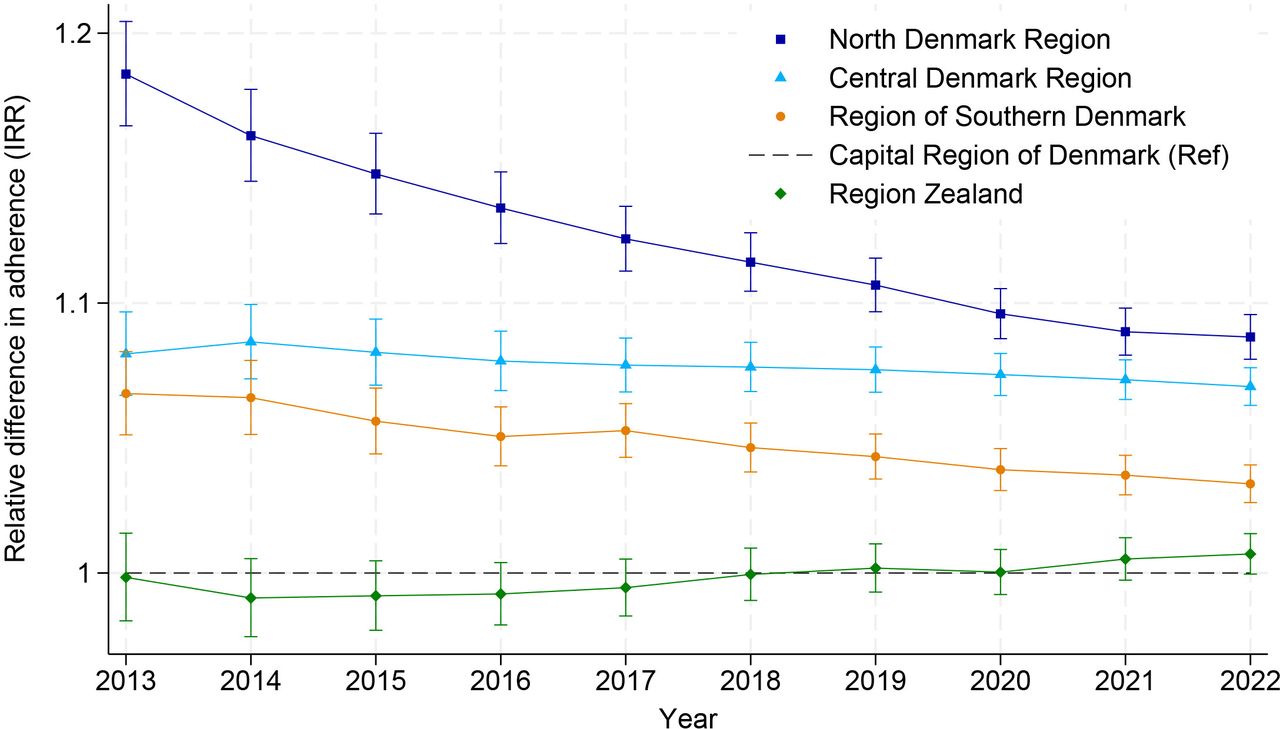
The North Denmark Region had the highest adherence levels across all periods compared with the Capital Region of Denmark (reference group). However, the relative difference decreased during the decade from 18% higher adherence in 2013 to 9% in 2022. Similarly, the Central Denmark Region and the Region of Southern Denmark consistently had higher adherence levels compared with the Capital Region of Denmark throughout the study period (2013–2022). The difference remained stable at 7%–8% in the Central Denmark Region, while a decrease from 7% to 3% was observed in the Region of Southern Denmark. No significant difference in adherence levels was observed between Region Zealand and the Capital Region. The relative ranking of regions in terms of adherence remained consistent throughout the study period (table 2 and figure 4).

Temporal development in the variation of adherence to anticoagulant therapy across geographical regions. Fully adjusted IRRs of adherence across the Danish administrative regions (adjusted for patient age, gender, health status, 38 long-term conditions defined in the Danish Multimorbidity Index (online supplemental table 2) and patient’s socioeconomic characteristics (origin, education, employment, income, cohabitation). IRR, incidence rate ratio.
Impact of patient-level determinants across regions
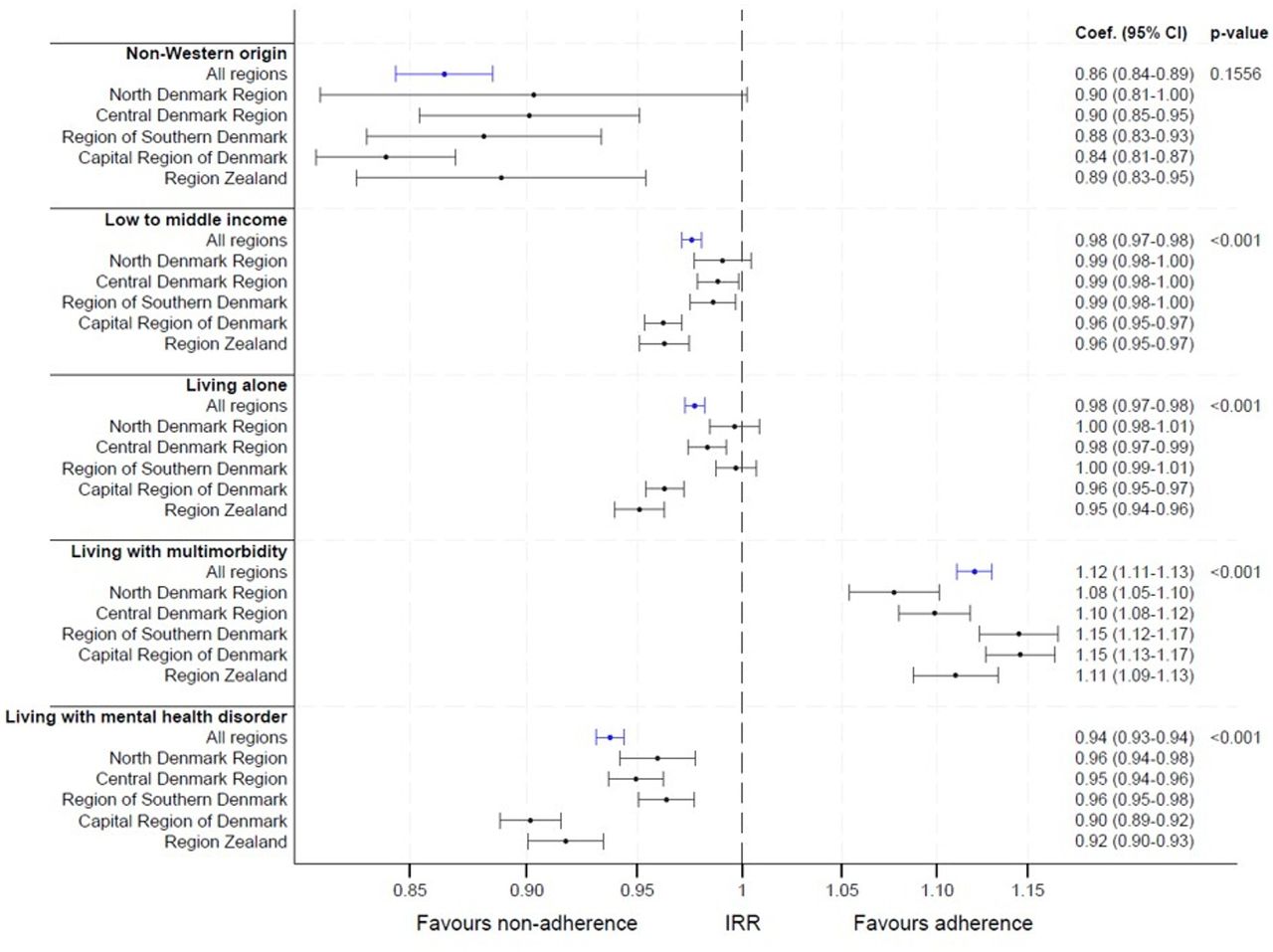
Patients of non-Western origin had reduced adherence across all regions, with an overall IRR of 0.86 (95% CI 0.84 to 0.89) compared with patients of Western origin. This association was most pronounced in the Capital Region of Denmark (IRR 0.84, 95% CI 0.81 to 0.87), while the association was less pronounced in the North Denmark Region (0.90, 95% CI 0.81 to 1.00).
Similarly, patients with mental health disorders had an increased risk of non-adherence (IRR 0.94, 95% CI 0.93 to 0.94), and the associations were stronger in the Capital Region of Denmark (IRR 0.90, 95% CI 0.89 to 0.92) and Region Zealand (IRR 0.92, 95% CI 0.90 to 0.93) compared with the other regions.
The overall impact of low income and living alone on OAC adherence also showed a trend towards non-adherence. In line with our findings for mental health status, the associations were stronger in the Capital Region of Denmark and Region Zealand compared with the other regions. However, the overall impact of income and cohabitation was small (IRR 0.98, 95% CI 0.97 to 0.98 for both).
In contrast, multimorbidity was associated with improved adherence in all regions, with an overall IRR of 1.12, 95% CI 1.11 to 1.13. The strongest association was observed in the Region of Southern Denmark (IRR 1.15, 95% CI 1.12 to 1.17) and the Capital Region of Denmark (IRR 1.15, 95% CI 1.13 to 1.17), while the association was less pronounced in the North Denmark Region (IRR 1.08, 95% CI 1.05 to 1.10).
The differences in the impact of origin between regions were not statistically significant (p=0.16). However, in the remaining analyses, the interaction between region of residence and patient exposure variable was considered statistically significant, showing p values <0.001 (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Impact of patent determinants on adherence to oral anticoagulant treatment stratified by region in 2013–2022. For all estimates, the reference group (IRR=1) is the unexposed group in the same region (full cohort in reference model). The results are presented as IRRs with 95% CIs. All models were adjusted for sex, age and comorbidities defined in the Danish Multimorbidity Index (online supplemental table 1). Origin, income and cohabitation were adjusted for all conditions; multimorbidity only for mental health conditions, mental health status only for non-mental health conditions. P values are provided for no interaction between exposure variable and region of residence. IRR, incidence rate ratio.
Sensitivity analyses
Sensitivity analyses did not lead to any substantive changes in the results (online supplemental figures 1 and 2).
Discussion
Principal findings
A substantial increase in overall adherence to OAC for patients with AF was observed during the study period, rising from 53% in 2013 to 78% in 2022. Adherence improved consistently across all five Danish regions, without notable changes in the relative rankings of the regional adherence levels. By 2022, the absolute adherence difference between the highest-performing and lowest-performing regions was 7.6%. Concurrently, a significant shift in treatment patterns was observed, characterised by a transition from VKAs to DOACs, with a preference for rivaroxaban and apixaban. The sequential adjustments for patient demographics, health status and socioeconomic factors had little impact on the IRRs of OAC adherence across regions. The greatest impact of adjusting for patient characteristics was observed in 2013 when the adherence gap between the highest-performing and lowest-performing regions was reduced from 21% to 18%. When applying the fully adjusted regression model, the variation in adherence between the highest-performing and lowest-performing regions decreased from 18% in 2013 to 9% in 2022. However, the relative rankings of regions remained unchanged. Low socioeconomic status and the presence of psychiatric comorbidities were associated with reduced adherence to OAC, with the impact being more pronounced in regions characterised by lower overall adherence. Conversely, patients with multimorbidity showed higher adherence across all regions, with the highest impact in the Region of Southern Denmark and the Capital Region of Denmark.
Strengths and limitations
The nationwide Danish registers provide comprehensive, high-quality data on health and sociodemographic characteristics with near-complete population coverage,23 thereby minimising selection bias and enabling robust and representative analyses. Health data are systematically collected over time from routine care settings, which allows the study of treatment patterns that reflect real-life practices and patient adherence. However, the use of routinely collected data inherently limits the depth of available information, as it is restricted to pre-existing data fields. Key clinical factors, such as patient-reported adherence barriers, physician rationale for treatment decisions and lifestyle factors, are not systematically recorded. As a result, important determinants of adherence remain unmeasured, potentially introducing residual confounding. Furthermore, despite systematic data collection, variations in coding practices over time and across administrative settings with different IT systems may introduce bias and lead to misclassification. The DNPR24 records all medication prescriptions redeemed at any pharmacy in Denmark. This ensures consistent, population-wide monitoring of medication reimbursement. However, as only data on redeemed prescriptions are available (not records of prescribed medications), the study relies on estimated daily doses. Furthermore, it cannot determine whether non-adherence was due to medications not being collected or never prescribed.
Comparison with existing literature
Our study demonstrated a substantial restructuring of anticoagulant treatment in Denmark over the past decade; this restructuring was characterised by significantly improved adherence and effective DOAC implementation. These findings are consistent with previous studies.6 7 18 19 However, our incorporation of recent data further highlighted the trends. During the study period, adherence increased consistently across all regions, and the absolute difference in adherence rates across regions decreased slightly, from 10% in 2013 to 7.6% in 2022. Furthermore, the adoption of DOACs followed a uniform pattern across regions. Such uniform development could be explained by the context of the Danish tax-funded healthcare system with free and equal access.37 Additionally, widely accepted international guideline recommendations exist for OAC.4 5 These guidelines have been translated and adapted to the Danish setting by the Danish Society of Cardiology and are updated annually (nbv.cardio.dk). They are widely implemented across geographical regions and healthcare sectors, thereby facilitating consistent treatment practices.
Although the implementation of DOACs was uniform across regions, variations in the preference for specific DOAC subtypes were observed. Rivaroxaban and apixaban were the predominant DOACs in all regions, but their distribution varied. Previous research has shown that once-daily dosing regimens are associated with improved adherence.38 39 In this study, DOACs with a once-daily dosing schedule (rivaroxaban and edoxaban) accounted for a larger proportion of dispensed prescriptions in regions with higher adherence rates, potentially contributing to regional variations in adherence.
The risk of suboptimal treatment varies depending on the patients’ comorbidity40–42 and sociodemographic characteristics.43 44 Previous studies on geographical variation in OAC initiation and persistence in Denmark have mainly focused on accounting for physical comorbidity and not for sociodemographic factors or mental health disorders.16 18 19 21 We aimed to explore to what extent geographical variation can be explained by differences in population characteristics across regions. Therefore, we applied regression models that sequentially adjusted for patient demographics, health status and socioeconomics to examine whether accounting for specific patient characteristics significantly changed the relative differences in adherence across regions. As the relative differences remained stable across all adjustment models, this suggests that differences in patient populations across regions explained little of the observed regional variation.
When applying the fully adjusted model over 10 years, we observed that the relative differences across regions (figure 4) showed the same pattern as the absolute differences (figure 2). The relative rankings of the regions remained unchanged, and a 9% difference in relative adherence rates was seen between the highest-ranked region compared with the lowest-ranked region. The reduced relative difference over time (figure 4) appeared more pronounced than the change in absolute rates (figure 2). However, this can largely be explained by the overall increase in adherence over time, which inherently will reduce the relative difference.
The inability of the applied models to explain regional variation may be due to several factors. First, many patient-related factors are not captured in the register-based data used in this study, including health literacy and beliefs about medication. Second, regional variation may be driven by provider-level and system-level factors, including differences in physicians’ adherence to guidelines, shared decision-making practices and resource allocation. When assessing if OAC variation was explained by differences in patient populations, we assumed that the impact of patient determinants was uniform across the entire population. Importantly, many factors at provider or system level can influence whether patient risk factors are associated with reduced adherence. Therefore, we investigated whether the impact of comorbidity and socioeconomic status varied according to the patient’s region of residence.
In line with existing literature, we found that non-Western origin,43 low income,44 living alone44 and having a mental health disorder40 were associated with an increased risk of non-adherence. Furthermore, we found that the risk of non-adherence associated with low income, living alone and having a mental health disorder was increased in the regions with the lowest adherence rates. This might indicate systematic differences in the management of vulnerable patient groups, which could contribute to the persistent variation.
We found that adherence rates were consistently higher in patients with multimorbidity across all regions. This finding contrasts with evidence suggesting that the complexity of care associated with multimorbidity, including the burden of polypharmacy, may negatively impact adherence.42 45 46 However, in patients with AF, the risk of ischaemic stroke (and the net benefit of OAC) increases with greater comorbidity.4 5 This could explain the higher OAC adherence seen among patients with multimorbidity and AF. The impact of multimorbidity varies across regions. However, the direction of these differences does not explain the inter-regional variation.
Clinical implications and future research
The observed increase in overall adherence to OAC among patients with AF is encouraging. Adherence rates appear to stabilise at approximately 80%, suggesting that the target for optimal treatment coverage may be nearing. However, our findings highlight persistent regional adherence disparities that cannot be explained by population differences alone. In some regions, vulnerable patient groups seem to face an elevated risk of non-adherence, which may result from systematic variations at healthcare provider level or system level.
Future studies should aim to identify drivers of regional variation to pinpoint opportunities for improvement at both healthcare provider level and system level. The persistent unwarranted geographical variation in OAC usage suggests that there is still opportunity and need for improving the quality and equity of care for patients with AF.
Data availability statement
Data may be obtained from a third party and are not publicly available. The data used in this study are available to authorised research institutions through collaborative agreements. Access to the Danish registers is granted by Statistics Denmark and the Danish Health Data Authorities. More information can be found on the website of Statistics Denmark (www.dst.dk/en/TilSalg/Forskningsservice).
Ethics statements
Patient consent for publication
Ethics approval
Ethical approval and informed consent were not required, as the study was based on deidentified register data, which were encrypted, stored and anonymised by Statistics Denmark before analysis.
Acknowledgments
The authors thank Henrik Schou Pedersen for providing statistical advice.
References
Footnotes
Contributors IGL, ELG, AP, FB and AM designed the study. IGL and AP performed the statistical analyses and had full access to all data. All authors contributed to the analysis and interpretation of data. IGL drafted the first version of the manuscript, and all authors revised and contributed to the editing of the manuscript. All authors have read and approved the final version. AP is the guarantor of the study. ChatGPT (version 4.0) was used to improve the clarity and accuracy of the language in this manuscript. It was employed to correct spelling and grammar errors and to suggest synonyms or alternative phrasings where appropriate.
Funding This work was supported by the Foundation for Primary Health Care Research in the Central Denmark Region (Praksisforskningsfonden, file no. 1-30-72-112-16) and the Foundation for General Practice (Fonden for Almen Praksis, file no. A4105). The funding was granted based on peer review of the research proposal, with no involvement from the grant providers in any aspect of the study.
Competing interests The authors declare no competing interests related to this manuscript. Outside the submitted work, ELG has previously received speaker honoraria or consultancy fees from AstraZeneca, Bayer, Bristol-Myers Squibb, Pfizer, Novo Nordisk, Lundbeck Pharma and Organon. He is investigator in clinical studies sponsored by AstraZeneca, Idorsia or Bayer and has received unrestricted research grants from Boehringer Ingelheim.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.