Article Text

Abstract
Introduction Postoperative sleep quality is generally impaired in elderly patients undergoing total knee arthroplasty. Decreased postoperative sleep quality seriously affects postoperative recovery. Both esketamine and dexmedetomidine have been individually demonstrated to have the potential to enhance postoperative sleep quality. However, the effectiveness of mini-dose esketamine–dexmedetomidine supplemented intravenous analgesia on postoperative sleep quality remains to be elucidated.
Methods and analysis 110 elderly patients undergoing total knee arthroplasty will be randomly assigned to different regimens of patient-controlled intravenous analgesia with a total volume of 100 mL in either the experimental group (sufentanil 1.5 µg/kg+esketamine 25 mg+dexmedetomidine 100 µg) or the control group (sufentanil 1.5 µg/kg+equal vol of placebo, ie, saline). The primary outcome is the subjective sleep quality score on the night of surgery, assessed using the Richards–Campbell Sleep Questionnaire. The secondary outcomes are the Richards–Campbell Sleep Questionnaire scores on the first and second postoperative nights. Patients’ pain scores, Richmond Agitation-Sedation Scale scores, analgesic medication usage and incidence of nausea and vomiting are documented two times per day for two postoperative days. The Montreal Cognitive Assessment score is assessed on the day of discharge. Regarding other outcomes, telephone follow-up will be performed at 30 days postoperatively to assess the Pittsburgh Sleep Quality Index score and identify and document major complications within 30 days. Safety outcomes encompass not only the monitoring of basic vital signs such as hypotension, hypertension, tachycardia, bradycardia and low peripheral oxygen saturation but also psychiatric symptoms, including nightmares, hallucinations, restlessness, confusion, diplopia and blurred vision. The analysis will be conducted according to the principle of intention-to-treat.
Ethics and dissemination The study protocol has been approved by the Medical Research Ethics Committee of Weifang People’s Hospital (KYLL20240523-1). The results of the study will be published in peer-reviewed journals and scientific conferences.
Trial registration number ChiCTR2400085253.
- Anaesthesia in orthopaedics
- Sleep medicine
- Pain management
- ANAESTHETICS
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study investigates the impact of mini-dose esketamine–dexmedetomidine combination analgesia on sleep quality in elderly patients, using acute-phase changes measured by the Richards–Campbell Sleep Questionnaire and systematic psychiatric symptom monitoring to ensure safety and validate efficacy.
Clinical trials adhere to rigorous methodological standards, such as the randomised double-blind placebo-controlled design and the intention-to-treat method, which help minimise bias and enhance the reliability of the research results.
Mini-dose of esketamine–dexmedetomidine is used for postoperative intravenous analgesia to reduce the incidence of drug-related side effects.
The study does not clarify the mechanism by which the combination therapy affects sleep quality.
This is a single-centre trial, and further validation at other institutions is necessary.
Introduction
As the main method for the treatment of end-stage knee diseases, total knee arthroplasty (TKA) has been widely used in clinical practice. Feng et al 1 have found that the number of TKA cases in China has surged, with an increase of about 600% from 2011 to 2019. Impaired sleep quality is prevalent among patients undergoing TKA,2 3 especially for an ageing population.4 Compared with other age groups, elderly patients (≥65 years), who constitute the majority of TKA recipients, face elevated risks of postoperative complications due to age-related physiological decline and comorbidities. Among these, impaired sleep quality is particularly concerning, with studies reporting patients experiencing poor sleep on the night of surgery3 5—a risk factor linked to heightened pain sensitivity,6 7 higher incidence of delirium,8 9 promotion of depression,10 reduced long-term quality of life11 and cardiovascular adverse events.12 Given that anaesthesia and analgesic strategies directly influence sleep regulation, optimising perioperative management to address sleep disturbances is crucial for enhancing postoperative outcomes in this vulnerable population. Therefore, how to improve the problem of impaired sleep among elderly patients undergoing TKA has become an important factor in optimising their recovery process.
Factors that affect the decline in sleep quality among patients in the perioperative period of TKA are not only related to their age and surgical trauma degree, but also affected by their preoperative basic conditions (including gender, comorbidities, preoperative sleep disorders, preoperative anxiety and depression), postoperative triggers (including pain, ward environment, anxiety and depression) and the use of intraoperative anaesthesia and analgesics.13–15 Anaesthetic analgesics can not only ensure the smooth progress of TKA but also effectively alleviate patients' postoperative pain, which is an indispensable part of TKA treatment. However, studies have shown that there are common pathways between general anaesthesia and physiological sleep.16 Traditional opioid anaesthetics can effectively reduce postoperative pain, but they have side effects of disrupting sleep regulation, which in turn can lead to sleep disorders.17 18 The combination of new anaesthetic drugs can provide important insights for solving the above problems.
Ketamine, a non-competitive antagonist of the N-methyl-d-aspartate (NMDA) receptor, is recognised for its potent analgesic characteristic as an anaesthetic, featuring some adverse side effects, such as psychiatric symptoms, tachycardia and high blood pressure. Recent studies have shown that ketamine can improve sleep.19 More importantly, it can prolong the average duration of deep sleep.20 Esketamine, the dextrorotatory isomer of ketamine, boasts a stronger effect and a lower incidence of adverse psychiatric reactions.21 Wang et al have demonstrated that the intraoperative administration of esketamine can enhance sleep quality in patients undergoing thyroidectomy on the first postoperative night.22 Qiu et al have suggested that the intraoperative use of esketamine primarily enhances postoperative sleep quality in patients undergoing gynaecological surgery by inhibiting inflammation, regulating the circadian rhythm system and reducing opioid consumption.23 Accumulating data demonstrate that both ketamine and esketamine may improve sleep architecture during surgical recovery through NMDA receptor modulation and anti-inflammatory effects, offering a dual-target strategy for perioperative care.23 24 Dexmedetomidine is a highly selective α2-adrenoceptor agonist with sedative, analgesic and anxiolytic effects. It distinguishes itself from traditional sedatives by improving sleep quality through the activation of natural sleep-inducing mechanisms.25 Evidence suggests that dexmedetomidine enhances GABA signalling in the hypothalamic ventral lateral preoptic area through indirect activation of α2A receptors within the nucleus accumbens, thereby inducing a sedative effect.26 However, it is not an effective analgesic that restricts its utilisation in painful procedures. Moreover, it affects haemodynamics and may lead to bradycardia or hypotension in many cases.
In the previous treatment of sleep impairment among patients undergoing TKA, drugs (alprazolam, zolpidem, melatonin) or non-pharmacological measures are usually used to improve the sleep quality of patients, thereby reducing the degree of postoperative pain and promoting postoperative rehabilitation.3 27 Ketamine, which stands apart from the aforementioned sleep-promoting drugs, is an intravenous analgesic that has been recommended for postoperative analgesia.28 The use of its dextrorotatory isomer, esketamine, is anticipated to minimise psychotropic side effects and has advantages of a shorter recovery period, faster recovery of cognitive function and less postoperative pain. Additionally, dexmedetomidine, which possesses intrinsic analgesic properties, is often recommended in combination with opioids for postoperative analgesia, particularly in the elderly. Emerging evidence demonstrates that patient-controlled analgesia with mini-dose dexmedetomidine enhances analgesia and preserves sleep architecture while avoiding excessive sedation.29 30 Notably, its intrinsic sedative properties may counteract ketamine/esketamine-induced psychoactive adverse reactions through α2-adrenoceptor-mediated neuromodulation.31 32 At the same time, esketamine demonstrates efficacy in mitigating dexmedetomidine-induced bradycardia and hypotension.32 Thus, a promising multimodal analgesic strategy by combining esketamine and dexmedetomidine could be beneficial to patients. Recently, it has been found that mini-dose esketamine (5.5 µg/kg/hour) combined with dexmedetomidine (0.02 µg/kg/hour) for intravenous analgesia in postoperative spinal orthopaedic surgery can significantly improve sleep quality and analgesic effect without increasing side effects in young people aged around 35 years.33 The aforementioned study elucidates the impact of mini-dose esketamine–dexmedetomidine as a supplement to intravenous analgesia on enhancing the sleep quality of postoperative patients. However, its specific effect on improving sleep in elderly postoperative patients remains unexplored. Based on the above research, we propose a hypothesis that mini-dose esketamine–dexmedetomidine, when used to supplement intravenous analgesia, can potentially improve postoperative sleep quality in elderly patients who will undergo TKA.
Methods and analysis
Study design and patients
This randomised, double-blind, placebo-controlled trial will be conducted at Weifang People’s Hospital. The study flow chart is presented in figure 1. Our study protocol is reported following the Standard Protocol Items: Recommendations for Interventional Trials statement (figure 2). The research protocol has received approval from the local biomedical research ethics committee on 23 May 2024 and registered with the Chinese Clinical Trial Registry on 4 June 2024 (ChiCTR2400085253). The study commenced with the enrolment of the first patient on 6 June 2024 and is projected to conclude by 6 June 2026. All participants will sign a written informed consent prior to their inclusion in the trial (see online supplemental file 1).
Supplemental material

The schematic flow chart for this study. MoCa, Montreal Cognitive Assessment; NRS, Numeric Rating Score; PSQI, Pittsburgh Sleep Quality Index; RASS, Richmond Agitation-Sedation Scale; RCSQ, Richards–Campbell Sleep Questionnaire.

{kind=link}
{kind=link}
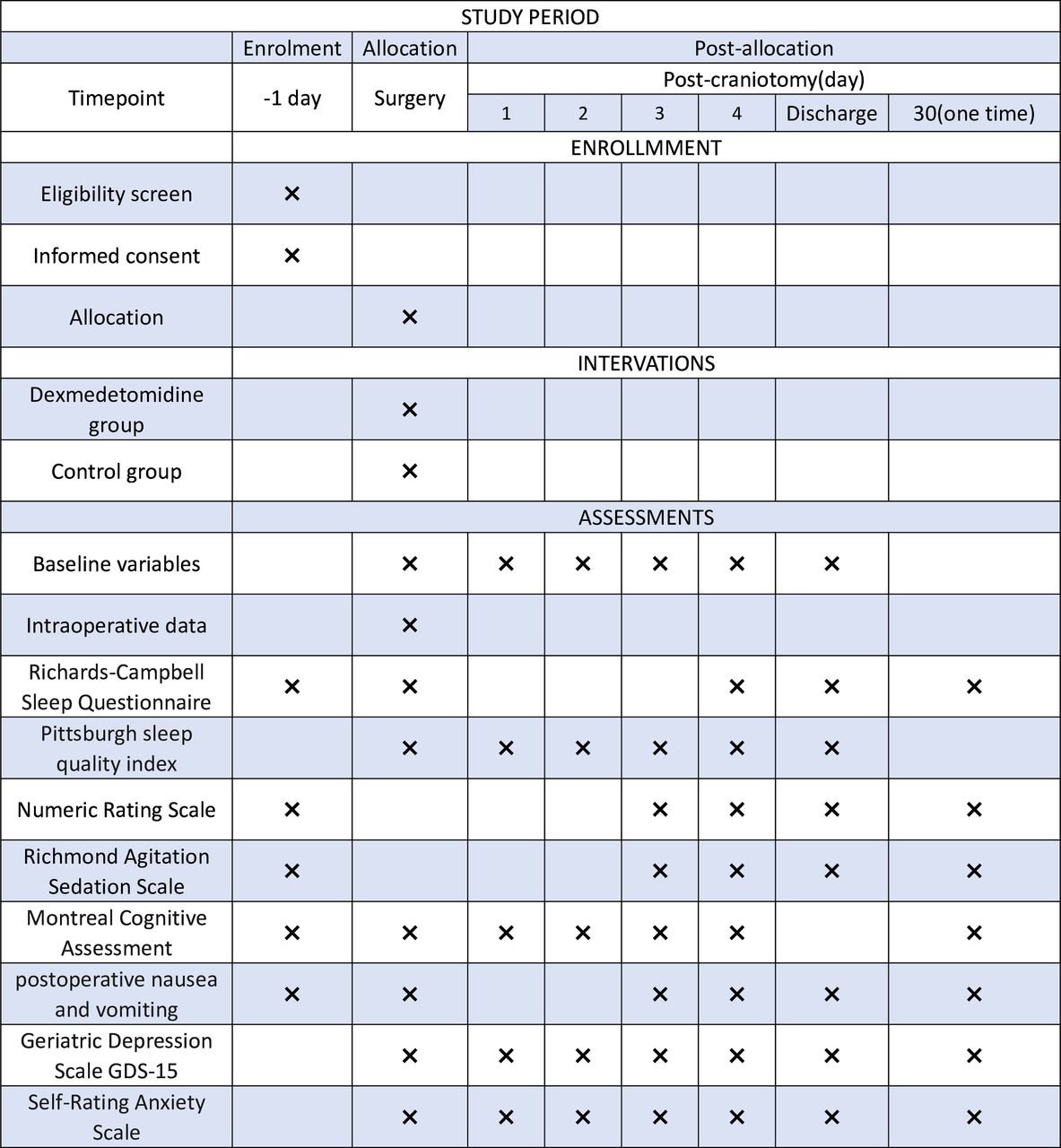
Schedule of enrollment, main intervention and assessment (Standard Protocol Items: Recommendations for Interventional Trials figure). GSD-15, Geriatric Depression Scale .
Inclusion criteria
Patients who meet the following criteria will be recruited: (1) age 65 years or older, but younger than 90 years; (2) conform to the American Society of Anesthesiologists grades I–III; (3) scheduled for elective TKA under general anaesthesia; (4) transferred to a general ward before 19:00 on the day of surgery and (5) consente to patient-controlled intravenous analgesia (PCIA) for postoperative pain management.
Exclusion criteria
In this protocol, patients will be excluded based on the following criteria: (1) emergency surgery; (2) a diagnosis of sleep apnoea syndrome or a STOP-Bang score≥3; (3) severe cardiac dysfunction (preoperative Left Ventricular Ejection Fraction <30% or New York Heart Association class IV), severe liver dysfunction (Child–Pugh class C) and severe renal dysfunction (necessitating preoperative dialysis); (4) expected to be transferred to the intensive care unit (ICU) after surgery; (5) allergy to any components of ketamine, esketamine and dexmedetomidine, as well as currently undergoing treatment with these medications; (6) sleep disturbances within the past month requiring medical intervention, such as the use of hypnotic drugs; (7) preoperative conditions, including sick sinus syndrome, severe sinus bradycardia with a heart rate<50 beats per minute, atrioventricular block of second degree and higher without the presence of a pacemaker; (8) an inability to communicate and cooperate with the study due to severe dementia and language barriers; and (9) a preoperative history of schizophrenia, epilepsy, parkinsonism and myasthenia gravis.
Randomisation and blinding
Random numbers are generated using SAS V.9.3 software (SAS Institute, Cary, North Carolina, USA) with a 1:1 allocation ratio and block sizes of 4. Throughout the study, the research coordinator (CL) will be responsible for assigning enrolled patients to one of the two groups randomly and preparing the study medications—both the test drug and the placebo—20 min before the end of surgery. Both the test drug and the placebo are stored in 5 mL syringes from the same brand and batch. The syringes are labelled only with random identifiers (eg, ‘STUDY-001’) and expiration dates, without any indication of group assignment (eg, ‘Group A’ or ‘Group B’). The test drug and placebo are both colourless and odourless transparent liquids. The PCIA pump, a drug infusion device, consists of a pump unit (including a display screen, driving device, processing module, battery), a liquid storage bag, a pipeline and a self-control drug administration button. The PCIA pump is driven by a micro-motor to ensure accurate drug delivery, with the infusion rate adjustable within a specified range. Apart from variations in patient demographic information, the appearance of the prepared PCIA pumps is consistent. A strict blinding protocol is implemented, in which the preoperative visit is conducted by the anaesthesiologist (YL), while anaesthesia is administered by another two anaesthesiologists (XW and JL) according to the established protocol. The postoperative assessment is performed by the anaesthetic nurse (XJ), who is blinded to the research protocol and is solely responsible for postoperative follow-up. All the participating patients, healthcare team members and research personnel, except the research coordinator (CL), are unaware of the trial group assignments. Group assignments will be announced by the coordinator (CL) at the end of the trial. In the event of an emergency, such as the occurrence of a serious adverse event or when guidance is needed for subsequent treatment steps based on the blinding results, researchers have the option to reveal the group allocation or to halt medication administration. Any such instances will be meticulously documented and securely preserved.
Study intervention
Based on the results of the randomised group, interventions will be carried out according to the research plan. Patients in the experimental group receive a 2 mL test solution, consisting of esketamine 25 mg, dexmedetomidine 100 µg and sufentanil 1.5 µg/kg, which is diluted to a final volume of 100 mL with normal saline. Patients in the control group are given a placebo of 2 mL normal saline along with sufentanil at the same dosage, which is also diluted to 100 mL with normal saline. The treatment regimen involves an initial loading dose of 2 mL, followed by a continuous infusion at a rate of 1 mL per hour. A single top-up dose of 2 mL is permitted, with a lockout interval set at 15 min. The primary objective of this protocol is to maintain the Numeric Rating Score (NRS) for pain within or below the threshold of 3 points, ensuring effective postoperative analgesia.
Rescued analgesia protocol
In the recovery room, patients with an NRS pain score of 4 or higher are enabled to press the PCIA pump. If additional analgesia is required and the PCIA is insufficient, a single dose of sufentanil will be administered to alleviate symptoms until the NRS score is reduced to 3 or below. It is important to note that the use of esketamine and dexmedetomidine is prohibited in this context.
Perioperative management
Standard preoperative fasting and water deprivation are conducted for all patients the evening prior to surgery. On their arrival in the operating room, peripheral venous access is established immediately. Comprehensive monitoring, including ECG, non-invasive blood pressure, pulse oxygen saturation (SpO2), bispectral index and end-tidal carbon dioxide partial pressure (PetCO2), is initiated. Invasive arterial blood pressure monitoring is selectively deployed according to patient-specific needs. Before induction, patients will undergo routine ultrasound-guided adductor canal block with 30 mL of 0.33% ropivacaine to optimise comfort and analgesia.
The anaesthetic regimen employed is total intravenous anaesthesia, in accordance with the standard practice of our unit. For the induction of anaesthesia, patients receive an intravenous bolus injection of sufentanil at a dose of 0.3 µg/kg, propofol at 2 mg/kg or etomidate at 0.3 mg/kg, rocuronium bromide at 0.6 mg/kg and dexamethasone at 5 mg. Throughout the surgery, anaesthesia is sustained via a continuous intravenous infusion of propofol and remifentanil. The objectives of our anaesthesia management include maintaining BIS within a range of 40–60, keeping heart rate and blood pressure fluctuations within 20% of the patient’s baseline values, and regulating the core body temperature between 36°C and 37°C. PCIA pump is connected 20 min before the end of surgery. With the absence of any contraindications, ondansetron at a dose of 8 mg and flurbiprofen axetil at 50 mg are administered intravenously. Ondansetron will be administered as a prophylactic measure against postoperative nausea and vomiting, and flurbiprofen axetil will be used for patient analgesia. Lornoxicam (8 mg) is administered routinely by orthopaedic surgeons postoperatively for 2 days, two times per day. No other pharmacological or non-pharmacological treatment measures are used for sleep disorders that occurred during the postoperative period in the ward.
Additionally, vasoactive medications, including ephedrine, atropine, norepinephrine, nitroglycerin and esmolol, are made available during the surgery as necessary based on the patient’s condition.
Vital signs, including blood pressure, heart rate and pulse oximetry, are closely monitored in the anaesthesia recovery room for a minimum of 30 min prior to the patients being transferred back to the ward. On the patient’s return to the ward, continuous cardiac monitoring is maintained, and blood pressure assessments are conducted every 30 min to an hour, based on the individual’s condition, until 08:00 the following day after surgery or until the patient’s condition is deemed stable by the clinical team. At that point, a long-term medical prescription is issued by the clinician and executed by the nurse on the ward.
Data collection and outcome assessment
Baseline variables, including demographic data, comorbidities and major laboratory tests, will be collected. Based on exclusion criteria, these tests include assessment of liver and kidney function, cardiac assessments such as ECG and echocardiography, and other routine laboratory tests such as complete blood count, electrolyte levels, blood glucose and coagulation. Sleep quality within the recent 1 month is evaluated using the Pittsburgh Sleep Quality Index (PSQI), which ranges from 0 to 21, with higher scores indicating poorer sleep quality.34 Pain intensity, both at rest and during movement, is assessed using NRS (an 11-point scale, where 0 indicates no pain and 10 represents the most severe pain). Depressive symptoms are assessed with the Geriatric Depression Scale (GDS-15), which ranges from 0 to 15 (a score of 1–4 indicating no depression, 5–9 suggesting possible depression and 10 or above indicating depression). Anxiety levels are evaluated using the Self-Rating Anxiety Scale (SAS), which ranges from 20 to 80, with higher scores indicating greater anxiety.35 Cognitive function is assessed using the Montreal Cognitive Assessment (MoCA). Intraoperative data such as the amount of anaesthesia administered, duration of anaesthesia, length of the surgical procedure, use of tourniquets, fluid infusion rates, estimated blood loss and transfusion requirements, and the use of any vasoactive drugs during surgery will also be collected.
Primary outcome
The primary outcome measure is the subjective sleep quality on the night of surgery, which is assessed by the Chinese version of the Richards–Campbell Sleep Questionnaire (RCSQ) between 08:00 and 10:00 on the first postoperative morning.36 37 Five domains, including sleep depth, sleep latency, number of awakenings, ability to return to sleep and overall sleep quality, are encompassed in RCSQ. The overall RCSQ sleep score, calculated as the mean of these five domains, is categorised into four groups: very poor sleep (scores of 1–25), poor sleep (scores of 26–50), good sleep (scores of 51–75) and very good sleep (scores of 76–100). The Chinese version of the RCSQ has demonstrated good reliability and validity in evaluating sleep quality for patients in the ICU and elderly inpatients.38 In addition, to ensure the consistency of sleep assessments, the investigators for the RCSQ evaluation will receive training twice prior to and during the study.
Secondary outcomes
The RCSQ on the first and second postoperative nights will be evaluated according to the primary outcome measures. Pain intensity assessed using the NRS and the consumption of analgesic medications, along with the Richmond Agitation-Sedation Scale (RASS), are monitored during 0.5 hours after surgery and the first two postoperative days at specific times (08:00–10:00 and 16:00–17:00). The NRS includes both movement pain and resting pain. The total 48-hour analgesic consumption via the PCIA pump is also recorded. The incidence of nausea and vomiting within the first 24 hours and between 24 and 48 hours postoperatively is also recorded. Additionally, the MoCA is assessed on the day of discharge to evaluate cognitive function, and the PSQI will be used to measure sleep quality at 30 days following surgery.
Other outcomes
Self-administered attempts and total self-administered dose of PCIA in postoperative 48 hours. The duration of postoperative in-hospital stay is defined as the period spanning from the day of surgery to the day of hospital discharge. Major complications necessitating medical interventions, such as those classified as Clavien–Dindo grade 2and above,7 within the 30-day postoperative period will also be collected.
Safety outcomes
We conducted surveillance for hypotension defined as a systolic blood pressure<90 mm Hg or a decrease exceeding 30% from the baseline, hypertension indicated by a systolic blood pressure>180 mm Hg or an increase of more than 30% from the baseline, bradycardia characterised by a heart rate falling below 45 beats per minute or a reduction surpassing 30% from the baseline, tachycardia with a heart rate>100 beats per minute or an increase exceeding 30% from the baseline and pulse oxygen saturation<90%. These vital signs are monitored from the onset of anaesthesia until 08:00 the following day after surgery or until the patient reaches a stable condition.
In addition, psychiatric symptoms, including nightmares, hallucinations, restlessness, confusion, diplopia and blurred vision, will be systematically monitored. Hallucinations and nightmares are documented through standardised self-report questionnaires incorporating structured prompts such as “Did you see or hear something that didn’t exist?” and “Did you have frightening dreams?” Restlessness is evaluated using RASS. Confusion assessment is examined using the delirium assessment scale. Specifically, confusion is assessed during the Post-Aanesthesia Care Unit (PACU) using the Confusion Assessment Method ICU, while assessments on the first and second postoperative days used the 3D Confusion Assessment Method for the Chinese population. For the evaluation of diplopia and blurred vision, a simplified bedside version of the Snellen visual acuity chart is employed for quantitative assessment of visual acuity, and the red glass test is used to determine the type of diplopia. All the aforementioned mental symptoms of the patients are evaluated at 30 min after admission to the PACU, as well as the first two postoperative days at specific times (08:00–10:00 and 16:00–17:00).
Sample size calculation
In a prior observational study of 20 elderly patients, the average RCSQ score on the night of surgery was 50, with an SD of 15.39 We hypothesise that the application of esketamine–dexmedetomidine in the PCIA will elevate the RCSQ score to 60 on the night of surgery. To achieve statistical significance at the 0.05 level and a power of 90%, the required sample size to detect this difference is calculated to be 49 patients per group using PASS 15.0 software. Accounting for a dropout rate of 10%, we aim to enrol 55 patients in each group.
Statistical analysis
Statistical analysis will follow the intention-to-treat (ITT) principle, where all randomised participants will be analysed according to their original group assignment, regardless of any protocol deviations or withdrawals after randomisation. For confirmation purposes, a per-protocol analysis will also be performed, but ITT analysis will serve as the primary analytical framework.
Data distribution normality will be evaluated through the Kolmogorov-Smirnov (α=0.05) and Q–Q plot visual inspection. Normally distributed data will be expressed as mean (SD) and compared between groups using an independent-samples t-test. Non-normally distributed data will be expressed as the median (IQR) and analysed using the Mann-Whitney U test. Categorical data will be shown as frequencies (percentages) and compared using the χ2 test or Fisher’s exact test.
The primary outcome measure is the total sleep score derived from the RCSQ on the day of surgery. This score will be evaluated by using either the inter-group t-test or the Mann-Whitney U test. Additional analyses, including the RCSQ score, RCSQ subitem scores, total sleep duration, sleep efficiency, sleep latency, wake time after sleep onset, pain scores at various postoperative time points, self-administered attempts and total self-administered dose of PCIA, postoperative hospital stay and inter-group comparisons, will also be analysed using either t-tests or the Mann-Whitney U test. Missing data will be processed by multiple imputation and maximum likelihood method. According to possible confounding factors (such as preoperative anxiety, depression, painful reaction), sensitivity analysis of the research results is carried out to ensure the stability of the research results. Repeated measurement data will be assessed using a mixed linear model. For ordinal data, the Mann-Whitney U test will be employed for inter-group comparisons, while mixed linear models will be used to analyse repeated measurements. Time-to-event data will be analysed using Kaplan-Meier survival analysis to compare postoperative hospital stays between groups. The log-rank test will be applied to determine the differences between groups. These differences will be quantified as hazard HRs and 95% CIs.
Ethics and dissemination
The study has been registered with the Chinese Clinical Trial Registry (online supplemental file 2). The study protocol, participant information sheet and consent form (online supplemental file 1), along with relevant materials, as well as the ethical aspects of this trial, have been approved by the Medical Research Ethics Committee of Weifang People’s Hospital, approval number KYLL20240523-1. Data collection for the study will use an electronic collection and management system, where data will be entered into the case report forms in a timely, complete, accurate and clear manner based on the original observations of the subjects. Data entry will be conducted using a dual-entry system on two separate computers, followed by two rounds of database comparison. Electronic data files will be categorised and stored with multiple backups to prevent loss. The results of this trial will be presented in peer-reviewed conference proceedings and publications.
Supplemental material
Ethics statements
Patient consent for publication
References
Footnotes
Contributors XW and JL contributed to the conception and design of the study. XW will contribute to the result collection. YL will contribute to the recruitment. CL will undertake the randomisation and allocation. XJ will conduct the follow-up. XW will write the manuscript. JL will revise and review the manuscript, and is the guarantor. All authors have agreed on the publication.
Funding This study was supported by the Medical and Health Science and Technology Project of Shandong Province (no. 202418000733).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.