Article Text

Abstract
Introduction Early and accurate diagnosis of tuberculosis (TB) is central to ensuring the proper treatment and curbing the transmission of the disease. Despite the significant burden, the diagnosis of peripheral lymph node(LN)TB, the most prevalent form of extra pulmonary tuberculosis (EPTB), has been challenging in low resource settings. To meet the existing needs, the Mobile-TB-Lab study set out to evaluate two innovative approaches, including thermal imaging and recombinase-aided amplification assay (RAA) in Minoo for point-of-need diagnosis of LNTB. The synergy of these index tests is expected to pave the way for rapid detection of EPTB in resource-constrained settings.
Methods and analysis Mobile-TB-Lab is a multicountry diagnostic evaluation study to be performed in Bangladesh and Uganda. Under this protocol, a total of 200 suspected EPTB patients with cervical lymphadenitis will be enrolled from tertiary healthcare facilities in Bangladesh and Uganda. Each participant will be subjected to laboratory investigations including microscopy, real-time PCR, cytology, culture and Xpert MTB/RIF Ultra with the tissue sample following fine-needle aspiration (FNA). As the index tests, thermal imaging will be performed before performing the FNA, and the leftover aspirate will be used to perform RAA in the Minoo device. The diagnostic efficiency of the index tests will be determined against a composite reference standard based on the laboratory methods. Besides, latent class analysis will be performed to assess the diagnostic accuracy of the index tests. Finally, health economic evaluation will be performed to determine the cost-effectiveness of the investigative methods.
Ethics and dissemination The study protocol (PR-23031) has been approved by the research review committee (RRC) and the ethical review committee (ERC) under the institutional review board (IRB) of icddr,b in Bangladesh. In Uganda, the study protocol has been approved by the Research Ethics Committee of the Infectious Diseases Institute of Makerere University under reference number IDI-REC-2023–62 and approval from the Uganda National Council for Science and Technology (UNCST) under reference number HS3494ES. All the study materials and procedures to be used for the enrolment of the participants have been approved by the ethical review committee. The study will be performed according to the declaration of Helsinki and the International Council for Harmonisation–Good Clinical Practice to ensure the participants’ rights, safety and well-being. The findings from this study will be submitted to peer-reviewed journals and presented at relevant national and international meetings.
- Artificial Intelligence
- BACTERIOLOGY
- Clinical Protocols
- Diagnostic Imaging
- Diagnostic microbiology
- Molecular diagnostics
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Artificial Intelligence
- BACTERIOLOGY
- Clinical Protocols
- Diagnostic Imaging
- Diagnostic microbiology
- Molecular diagnostics
STRENGTHS AND LIMITATIONS OF THIS STUDY
The key strength of the study lies in the introduction of two point-of-need techniques in diagnosing extra pulmonary tuberculosis.
This multicountry study will give a projection on the diagnostic efficiency of the index methods across the continents.
The accuracy of the methods will be determined against a composite reference standard.
Cost-effectiveness of the index methods will be determined, which will facilitate their eventual implementation.
The inadequate volume of the tissue aspirate might influence the analysis with recombinase-aided amplification assay in Minoo.
Introduction
Tuberculosis (TB) is a chronic infectious disease caused by bacilli of Mycobacterium tuberculosis complex (MTBC). It has long been regarded as the leading cause of death in adults globally despite the remarkable progress in TB control, with 122 million disability-adjusted life years (DALYs) attributed to disease episode and post-TB.1–3 According to the WHO Global TB Report (2024), Bangladesh ranked seventh out of the eight topmost countries with a high TB burden, contributing to 3.5% of TB incidences globally.4 The burden of this disease follows a similar trend in Africa as well as in Asia. Without exception, the burden of the disease is also high in Uganda, which has been enlisted as one of the 30 high-burden TB–HIV countries in the world.5 Although M. tuberculosis mostly affects the lung, it can also disseminate to extrapulmonary organs via the blood or lymph, resulting in extrapulmonary TB (EPTB). In 2019, EPTB accounted for 16% of the total 7.5 million TB cases globally, whereas the percentage was 18.19% of total TB cases in Bangladesh, with 3.65% mortality as reported by the Annual TB Report 2020.6 7 Likewise, around one fourth of the TB patients is diagnosed as EPTB in Sub-Saharan Africa where the prevalence of TB lymphadenitis is 24%.8 Most cases of EPTB in adults are frequently found in the extrathoracic lymph nodes (LN), especially the cervical areas. Effective treatment regimens, ensuring early and confirmed diagnosis, remains the major challenge towards proper and timely management of TB and EPTB cases.6 9 10
Diagnosis of EPTB, especially LNTB, is often challenging, given the lack of reliable diagnostics to distinguish these forms of TB, even in high-income countries.7 11 12 The classical method of diagnosis by isolating the bacteria by culture has been considered as the confirmatory test. However, the procedure takes several weeks and is only possible in a few specialised laboratories.11 Cytology and conventional smear microscopy for acid-fast bacilli (AFB) are used as the initial diagnostic tools for LNTB in resource-poor settings.13 Fine needle aspiration cytology (FNAC) is a simple and rapid diagnostic technique, but cytomorphological features of LNTB can overlap with other non-TB lesions.11 14 Conventional smear microscopy for AFB lacks sensitivity due to the paucibacillary nature of FNA.14 Lateral flow and antigen detection assays have limited sensitivity and specificity.11
With the advent of PCR-based molecular diagnostic methods, detection of TB and the treatment procedure has become faster. However, PCR-based assays are not suitable for on-site screening. In developing countries, the necessary equipment for diagnosis is only available in a few central laboratories, with less accessibility and limited capacity to test large numbers of incoming samples.11 Moreover, the transport conditions of samples are often not well maintained, which leads to unreliable results. Therefore, portable, accurate, simple and rapid tests, which are independent of climatic conditions, are needed to detect TB at the point-of-need.
Like other diagnostic approaches, radiology-based and ultrasound-based methods have been exploited towards improved diagnosis of EPTB. However, these advanced techniques are resource demanding and require significant technical expertise. Therefore, there is still a need for imaging techniques with improved accuracy and low training requirements to detect TB. In recent years, thermal imaging has gained popularity for the diagnosis of chronic diseases with genetic predisposition and screening of infectious diseases.15–20 This portable diagnostic modality has been successfully applied in the field of tumour diseases, especially in the detection of LN metastases.21 This technique can now be applied with little training using a standalone thermal camera which makes it rapid and cost-effective. While the thermal imaging approach has already been tested under difficult climatic conditions,22 it is yet to be investigated for the diagnosis of EPTB, especially LNTB. Until now, most LNTB patients are diagnosed at later stages due to the lack of reliable tools for early screening.23 The thermal imaging-based approach is therefore particularly promising for the screening of early and elusive LNTB cases. Moreover, this imaging system can support the process of FNA towards obtaining LN aspirate containing the Mycobacteria in the absence of ultrasound imaging devices. Thus, targeted invasive sampling could potentially be feasible in resource-limited settings, while ensuring patient safety and better outcomes.
Considering the resource constraints, isothermal molecular techniques such as loop-mediated isothermal amplification, recombinase polymerase amplification (RPA), rolling circle amplification, and nucleic acid sequence-based amplification have become popular in detecting infectious pathogens.24 RPA/recombinase aided amplification assay (RAA) is an isothermal probe-based nucleic acid detection method that requires neither template denaturation nor primer annealing steps. The low reaction temperature (close to ambient in parts of tropical countries) for the polymerase (42.0°C), the assay’s robustness and the detection device’s compactness make it an optimal technique for rapid molecular diagnosis at the point of care/need settings.25 RPA’s success in diagnosing virus infections has been proven through the development of standard assays for detecting many emerging and neglected diseases, most successfully in the Ebola outbreak in Guinea 2014–16.26–31 The assay is currently operated in a pocket-sized portable device (Minoo) linked to a smartphone app,32 see figure 1A.

(A) Smartphones presenting three possible outcomes of the recombinase polymerase amplification assay in Minoo (Source: Dr Ahmed Abd El Wahed, doi: 10.1007/s15010-024-02179-z); (B) Thermal imaging device (camera) presenting with a thermography (Source: Dr Sophie Schneitler).
Considering the unmet needs and current gaps, the research team set out this diagnostic evaluation study with an overarching goal to evaluate the diagnostic efficiency of the thermal imaging system and a pocket-sized isothermal amplification device operated via smartphone for detecting LNTB. This proposed study aims to establish a simplified point-of-need diagnostic algorithm for LNTB detection in resource-limited settings.
Methods and materials
Study sites and population
This multicountry diagnostic evaluation study will involve multiple implementation partners. The study activities will be conducted in Bangladesh and Uganda. In Bangladesh, icddr,b will conduct the study in collaboration with Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka. In Uganda, Makerere University will conduct the study in collaboration with Mulago National Referral Hospital, Kampala. The suspected tuberculous lymphadenitis (cervical lymphadenitis) patients will be enrolled in the study.
Inclusion/exclusion criteria
Any individual suspected as a case of tuberculous lymphadenitis (cervical LN measuringn ≥1 cm in the short axis diameter) will be included in the study. Cases diagnosed as malignancies will be excluded from the diagnostic analysis.
Study design and sampling
This will be a diagnostic evaluation study where a case–control design will be followed to determine the diagnostic efficacy of the index methods. The study procedure will involve patient enrolment, clinical sample collection, patient data collection and analysis, laboratory analysis, result delivery to the patient, referral of the confirmed patients to the treatment centre, and follow-up of the treated patients. For outcome analysis, the suspected patients will be stratified into two groups (case and control) based on the operational definition below.
Case
Any person whom clinicians suspect as having tuberculous lymphadenitis and positive through AFB microscopy and/or histopathology and/or culture and/or real-time PCR and/or Xpert MTB/RIF Ultra.
Control
Any person suspected by the clinicians as a case of tuberculous lymphadenitis but turns out to be negative through all the methods (AFB microscopy/culture/histopathology/real-time PCR/ Xpert MTB/RIF Ultra).
Study procedure
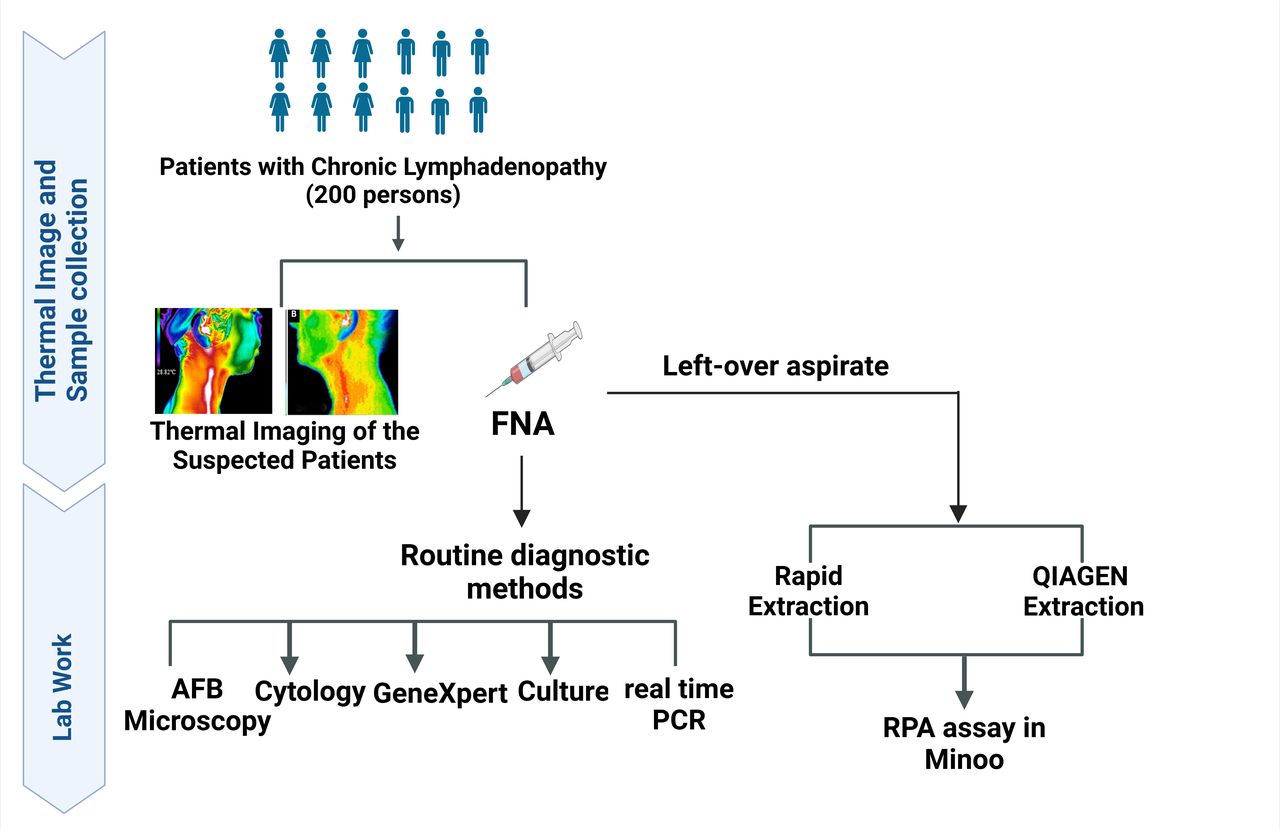
The care-seeking suspected tuberculous lymphadenitis patients in BSMMU and Mulago National Referral Hospital will be invited by the study physician to get enrolled in the study. After obtaining the informed consent, the study team will collect the demographic and clinical metadata from the individual patient following the routine physical examination. Then the patient will be examined through the portable imaging systems and subsequent laboratory procedures, as delineated in figure 2. The study physician will take images of the infected area likely to harbour tubercular infection. Following the thermal imaging, ultrasound-guided FNA will be performed under the supervision of a radiologist. Then the LN aspirates from the patient will be subjected to AFB microscopy and cytology. The remaining sample will be used for culture, real-time PCR and Xpert MTB/RIF Ultra. The leftover LN aspirate will be neutralised by tissue lysis buffer (ATL buffer), and DNA will be extracted from the aspirate to perform RAA assay in Minoo. Both bead-based and QIAGEN kit-based DNA extraction methods will be performed to extract DNA. Based on the routine diagnostic findings, physicians from the healthcare facilities will give standard treatment advice to the patients, such that this study will not interfere with the regular treatment. The study team will follow up a subset of the patients after 6 months of treatment. During the follow-up, the study team will perform thermal imaging of the patients.

{kind=link}
{kind=link}
Schematic diagram of the study procedure and laboratory investigations.FNA,fine-needle aspiration; RPA, recombinase polymerase amplification.
Clinical and laboratory methods
Clinical examination
General examination with special emphasis on LN (cervical chain) will be conducted by the expert pathologists. Being a suspect, the individual will be enrolled. Then the study physicians from icddr, b will collect the necessary information in the case report form and perform thermal imaging before FNA.
Thermal imaging
Three standardised images of the cervical region (right and left cervical-lateral as well as one image of the cervical region from the ventral side) are taken of each of the study participants using the FLIR C5 thermal camera and saved as JPG files. The image sections are selected such that participants in these images cannot be identified. Artificial intelligence will be trained on the data set. For this purpose, a neural network is first trained on the thermographic images, and in a second step, the additive anamnestic data are included. For this purpose, Python is used as the programming language and software libraries such as TensorFlow and Keras. The model’s parameters are optimised using cross-validation, and the final performance is determined on a hold-out test dataset.
LN ultrasound
The LN ultrasound will be performed according to the method described by Ying et al.33 An expert radiologist will perform the ultrasound prior to FNA to detect the LN with potential tubercular infection. The ultrasound report of the participants will be collected by the icddr, b study team for research purposes.
Fine Needle Aspirate
FNA will be conducted by trained pathologists working in BSMMU and Makerere University using aseptic procedure. The sample will be collected in a 3-cc syringe. After collecting the sample, two slides will be prepared with Ziehl–Nelsen (ZN) stain for identifying AFB. Another two slides will be prepared using H&E stain for conducting cytopathology tests. After the preparation of the slides, the rest of the samples will be transferred to the microbiology lab in BSMMU under aseptic precautions.
Chest X-ray
A chest X-ray will be done to exclude pulmonary TB.
Xpert MTB/RIF Ultra
The Xpert MTB/RIF Ultra assay will be conducted following the previous literature with minor improvisation.34 In the BSL-2 lab, the LN aspirate will be mixed with phosphate buffer saline (PBS) using the sterile transfer dropper to have a final volume of 0.7–1.0 mL in a 15-mL sterile falcon tube. The closed specimen container will be manually agitated twice 15 min apart at room temperature. The inactivated sample will be transferred into the test cartridge and dispensed slowly to minimise the risk of aerosol formation. The subsequent processing is fully automated in the Xpert MTB/RIF Ultra system. The results will be available in electronic version through the computer.
Real-time PCR
Real-time PCR will be done by GENMARK MTB/NTM Detection Kit for Real-Time PCR (www.genmark.com.tr) following instructions of the manufacturer. GENMARK MTB/NTM Real Time PCR Detection Kit is designed for the detection of MTBC and NTM by targeting IS6110 (MTBC) and 16S RNA (pan-Mycobacterium) genes.
Microscopy for AFB
Microscopy will be done according to the methods as per Uddin et al.35 Slides will be prepared with ZN stain and microscopic examination will be done by expert microbiologists.
Cytopathology
Cytopathology of LN aspirates will be performed following methods from previous literature.36 37 The slide will be kept under air for 15 min for drying, followed by washing under tap water. Then it will be deepened in haematoxylin for 4 min and briefly rinsed in tap water. Then lithium carbonate will be added to the slide and again washed under tap water. At this point, the slide will be rinsed with 95% alcohol twice. Then it will be stained in eosin azure for 2 min. Again, it will be rinsed with 95% alcohol for 2 min and then it will be rinsed with 100% alcohol for a couple of minutes. After clearing in xylene two times, the slide will be prepared for microscopic examination. A pathologist of BSMMU and Makerere University will examine the slide and a second opinion will be taken from another pathologist. When two pathologists agree on the examination’s outcome, the result will be informed to the patient and then recorded by the research team. If there is disagreement between the two pathologists, the slide will be examined by the third pathologist to resolve the discrepancy.
Culture
Culture will be performed in accordance with the methodology described previously.35 38 The aspirate will be decontaminated prior to culture. 4% sodium hydroxide and 2.9% sodium citrate containing 0.5% N-acetyl-L-Cysteine will be used to decontaminate the sample. Then it will be mixed properly with a vortex mixer. After ensuring proper mixing, the sample will be incubated at room temperature inside the biosafety cabinet for 15 min. Then PBS (pH 6.8) will be added to make the volume up to 40 mL. The sample will be centrifuged at 3000 rpm for 15 min to get the concentration. The pellet will be collected after discarding the supernatant very carefully. Then the pellet will be resuspended with 1.5 mL of PBS. One loop full of samples will be inoculated on a Löwenstein–Jensen slant for culture.
RAA in Minoo
The RAA assay will be performed with the extracted DNA samples following the previously published method.32 39 In brief, the assay will be performed in a 50 µl volume using the RAA kit (Jiangsu Qitian Gene Biotechnology Co., Ltd, China). The master mix will be prepared in a tube with 420 nM of RAA primer, 120 nM of RAA Probe, and 1 x rehydration buffer will be added to the RAA lyophilised pellet. Then, 14 mM magnesium acetate will be pipetted into the tube lids. Thereafter, template DNA will be added to the tube and the reaction mixture will be mixed by pipetting. The tube will be then incubated in the Minoo device (midge medical GmbH, Berlin, Germany) for amplification at a constant temperature of 42°C for 15–18 mins. The Minoo device is wirelessly (Bluetooth) connected with a smartphone for operation. The device is controlled from an authorised application, which transfers the relevant data to the backend via the internet (Wi-Fi) for analysis and usage monitoring. Kassandra, a proprietary Python-based algorithm, is used to analyse the fluorescence amplification signal. After analysis, the result of the test (positive, negative or inconclusive) is directly displayed on the smartphone application (see figure 1A).
Safety measures
Good Clinical Practice as required by the two Research Ethics Committees in Bangladesh and Uganda will be followed while enrolling the participants and personnel safety will be ensured. The trained pathologists at BSMMU and Makerere University will conduct FNA, and the samples will be handled and tested in BSL-2 labs by the trained lab technician of the project. Moreover, the FNA aspirate will be neutralised with ATL buffer prior to performing the bead-based DNA extraction.
Health economic evaluation
Test results and all available cost data will be used for the health economic evaluation. On the cost side, all resources will be included to measure the effort required for the different testing methods, including the reference tests. For this, information on expenses for laboratory materials (chemicals, materials, equipment, protective gear and test cartridges) will be documented. The amount of time (time required to take thermal images and to collect specimens, the time needed to perform the analyses) will be recorded to measure the costs for staff salary. Finally, potential challenges and obstacles experienced when performing the reference tests and the new technologies will be documented to assess and compare the feasibility of the different tests in a real-world healthcare setting.
The economic value of thermal imaging and the rapid extraction test will be evaluated against the regular course of diagnostics. Costs will be calculated from the health system perspective. Effectiveness will be measured by assessing the accuracy of each diagnostic strategy, namely the true-positive (TP), true-negative (TN), false-positive (FP), and false-negative rate (FN). Each outcome is then translated into DALYs. (TP=2.39, TN=0, FN=16.99, FP=0.1 DALYs). A cost-utility analysis will be conducted. The incremental cost-effectiveness ratio and incremental cost-utility ratio will be assessed for each strategy compared with the standard procedure. A willingness-to-pay threshold is set based on the gross domestic product per capita of Bangladesh (USD 2,529) for 2023, in line with WHO guidelines.
Sample size calculation
With an assumption of 90% sensitivity of the new test, a lower limit of the CI of at least 75% and a one-sided α level of 0.05, 120 samples are adequate to determine the performance of the index methods with approximately 78% power. However, considering a dropout rate of approximately 20%, a total of 200 participants will be recruited (100 participants at each site) in the study.
Data analysis
Parametric and non-parametric tests will be performed based on the distribution of data. Standard statistical methods, including contingency tests and binomial confidence intervals, will be followed to determine the sensitivity and specificity of the index methods with 95% CI. A composite reference standard based on the laboratory methods (Xpert MTB/RIF Ultra, microscopy, cytology, culture and real-time PCR) will be taken as the benchmark to evaluate the test accuracy, that is, to compute sensitivity and specificity. According to the composite reference standard, any case being positive through AFB microscopy and/or histopathology and/or culture and/or real-time PCR and/or Xpert MTB/RIF UltraGeneXpert will be considered as TP, whereas any case being negative through all of these cases will be considered as TN. Cohen’s kappa coefficient (k) and McNemar’s test will be performed to determine the concordance and discordance between diagnostic methods. To increase the rigour of the diagnostic analysis, in addition to the binomial approach, the sensitivity and specificity of each test will be estimated using a Bayesian latent class modelling framework. Data collection, preparation and analysis will be performed using Stata, R and Microsoft Excel. A p-value <0.05 will be considered statistically significant.
The evaluation of the performance of thermal imaging involves several steps. At first, a subset of thermal images of the study participants (both case and controls as per the operational definition) will be used to develop and train the AI-based algorithm. For this purpose, a neural network model is first trained on the thermographic images, and in a second step, the additive anamnestic data are included. In this process, the Python programming language and the TensorFlow and Keras software libraries are used. The model’s parameters will be optimised using the cross-validation process. On determining the accuracy of the AI algorithm, the remaining raw images (hold-out data set) will be subjected to analysis through the AI-based algorithm. With the aid of the AI-based algorithm, the LNTB cases and controls will be predicted. Subsequently, the thermal images will be stratified as true cases and true controls against the operational definition for LNTB cases and controls to determine the sensitivity and specificity. Thus, the performance diagnostic efficiency of the thermal imaging will be evaluated for LNTB.
Discussion
In the wake of this diagnostic evaluation study, two innovative tools will be validated and evaluated, which will potentially pave the way for integration of the tools in healthcare facilities, both in Africa and Asia. Apart from the innovative tools, the design of the study will strengthen the outcomes as multiple diagnostic modalities will be used in parallel to evaluate the performance of the index tests. Notably, the latent class analysis will be performed to determine the diagnostic performance of the index tests, which will rule out the bias to any specific test as there is no reference test of diagnosis of EPTB. The addition of economic evaluation will help the policy makers and funders introduce the tool into healthcare systems, if the test proves more cost-effective.
Data management and confidentiality
During the recruitment, each individual participant will be assigned a unique identification number. Following enrolment, participants’ personal records (eg, name, address and telephone number) will be kept securely and will remain separate from any clinical/epidemiological data, laboratory samples or data resulting from laboratory analysis. Research data will be linked only to the study identification number. Thermal images of each participant will be kept in a unique folder with the identification number of that study participant. All data (clinical, epidemiological and thermal image) will be stored in a secure database. Data will be anonymised and stored according to the privacy and data protection regulations as indicated in the icddr, b institutional review board (IRB) guideline. Data collection and storage will be performed using Microsoft Excel.
Patient and public involvement
There has been no involvement of the patient in study design or conduct of the study. However, the study findings will be disseminated to study participants and their caregivers.
Ethics and dissemination
The study protocol (PR-23031) has been approved by icddr, b Research Review Committee and Ethical Review Committee of the Infectious Diseases Institute of Makerere University (IDI) (Ref. No. IDI-REC-2023–64) on 6 August 2023 and 24 August 2023, respectively. In addition, the study protocol has been approved by the Research Ethics committee of the Infectious Diseases Institute of Makerere University under reference number IDI-REC-2023–62 and the Uganda National Council for Science and Technology (UNCST) under reference number HS3494ES for Uganda. The study will be conducted in accordance with the Declaration of Helsinki and ICH-GCP. For recruitment, an eligible participant will be informed about the aim, outline and individual risk of the study. The study team will provide written informed consent to the participants/parents/legal guardians in their first language. The study participants/parents/legal guardians will be informed that they are under no obligation to be enrolled in the study and that they can withdraw at any time during the study, without giving a reason. The study procedures will have no influence on the treatment of the patients. The clinicians from the healthcare facilities will give the treatment advice to patients based on the existing diagnostic and treatment guidelines. The study findings will be disseminated through peer-reviewed publications, academic conferences and formal presentations to health professionals and practitioners. Findings will also be communicated to study participants and their caregivers.
Project status
Recruitment of the study participants started in January 2024. The recruitment and follow-up of participants is still ongoing. The protocol (V.2) has not been subjected to any modification to date.
Ethics statements
Patient consent for publication
References
Footnotes
X @jbokuni
Deceased AAS deceased
Contributors The study concept and design were conceived by KC, MS, SS, MW, AAEW, DM, SA and JBO. SS is the principal investigator for the Mobile-TB-Lab study. BB, BPD, AAS, CA, RMK and AC provided additional methodological and/ or clinical advice. FRL, SNM, LN, NTM, EE and MAAC will conduct screening and data collection. Analyses will be performed by PG and SEM. PG prepared the first draft of the manuscript and will assist with data analysis. All authors provided edits and critiqued the manuscript. SS acted as the guarantor.
Funding The study was funded by the Federal Ministry of Education and Research (BMBF) through the German Alliance for Global Health Research (GLOHRA). The grant number is 01KA2217A/B/C. The funder has no role in study design and implementation.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.