Article Text

Abstract
Background Cardiovascular disease (CVD) is a major cause of death globally. In advanced stages, patients with CVD often require palliative care due to reduced health-related quality of life from physical, psychological and spiritual symptoms, along with physical disability.
Objectives To investigate (1) the symptom and function burden of patients with CVD on their first admission to specialist palliative care services and (2) how these care burdens, and other clinical characteristics, affected patients’ utilisation of community-based versus inpatient services.
Design A national population-based observational study using point-of-care outcomes sourced from the Australian palliative care outcomes and collaboration (PCOC).
Settings Community-based and inpatient Specialist palliative care services across Australia registered in the PCOC.
Participants Patients who required specialist palliative care principally for CVD, and whose death occurred between 1 January 2013 and 31 December 2022.
Methods Five validated clinical instruments were used to collect point-of-care outcomes on each individual’s function (Resource Utilisation Groups - Activities of Daily Living (RUG) & Australia-modified Karnofsky Performance Status (AKPS)), symptom distress (Symptoms Assessment Scale & Palliative Care Problem Severity Score) and other clinical characteristics (Palliative Care Phases). Multivariable logistic regression was applied to evaluate how patients’ functional and symptom burden influenced their use of inpatient versus community-based palliative care services.
Results Our analysis included 17 002 patients with CVD, with 7539 (44.3%) receiving community palliative care services and 9463 (55.7%) accessing inpatient palliative care services. On admission to palliative care services, patients often exhibit significant physical functional impairments and substantial symptom burdens, particularly related to fatigue and breathing difficulties. In comparison, patients accessing inpatient services tended to have greater functional impairment (p<0.001) but commonly reported lower symptom burdens (p<0.001). Our analysis indicated that greater functional impairment (ORs ranged from 2.53 to 6.02, p<0.001 for RUG; ORs ranged from 1.72 to 5.02, p<0.008 for AKPS), poorer overall health condition (OR ranged from 1.28 to 17.60, p<0.001) and referrals by a community service (OR=0.16, 95% CI: 0.14 to 0.18, p<0.001) were a negative predictor of inpatient services use. Surprisingly, higher levels of symptom distress and challenges in symptom management were associated with a decreased likelihood of using inpatient services compared with community-based services.
Conclusion Patients with CVD frequently require support to manage decreased functional abilities, as well as symptoms like fatigue and breathing difficulties. With greater investment in community-based supportive services and a skilled palliative care workforce, more individuals with advanced CVD could potentially receive palliative care in community settings.
- PALLIATIVE CARE
- Cardiovascular Disease
- Health Services
Data availability statement
Data may be obtained from a third party and are not publicly available. All our data are from Australian Palliative Care Outcomes and Collaboration (PCOC), which could be applied for access through their website: PCOC Research Data. (https://www.uow.edu.au/australasian-health-outcomes-consortium/pcoc/research-data/).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study is the first large-scale, national investigation in Australia that specifically focuses on the clinical characteristics and care needs of patients with cardiovascular disease receiving palliative care.
It offers a comprehensive analysis of the factors influencing the utilisation of various palliative care services by integrating diverse clinical characteristics, including functional impairment, symptom burden, referral patterns and overall health condition.
The multivariate models did not include other significant clinical factors (eg, the need for management of oedema and cognitive impairment) or social factors, which could influence the use of various types of palliative care services.
The higher rate of proxy-reported assessments in the inpatient group, as compared with the community group, may have introduced discrepancies that affect the reliability of the data.
Introduction
Cardiovascular disease (CVD) is a leading cause of death in Australia and worldwide.1 Individuals with severe stages of CVD often experience a diminished health-related quality of life due to physical, psychological and spiritual symptoms, as well as physical disability.2–4
Palliative care is a patient- and family-centred approach aimed at optimising patients’ quality of life by anticipating, preventing and treating suffering in all its forms.5 It is recommended for integration into the management of all chronic illnesses and can complement curative treatments.2 6–8 Robust evidence demonstrates that palliative care significantly enhances patient satisfaction and overall quality of life.2 9–11 Palliative care should be accessible in all settings where patients require it, with a primary focus on both community and hospital environments.5 6 12 Community-based and inpatient palliative care differ in their structure and processes, yet both are essential for delivering comprehensive care.13–15 Different types of palliative care are integral to ensuring patients receive the necessary support tailored to their specific needs and circumstances.5 15
Despite the significant disease burden similar to that of cancer patients, palliative care is currently underutilised in patients with advanced CVD.3 16 17 Addressing this disparity and ensuring that CVD patients receive ‘the right care, in the right place, at the right time’' presents a significant challenge in optimising palliative care for this group.17 18 Previous research has predominantly focused on understanding the palliative care needs of this patient group.19 However, there is a notable gap in exploring their patterns of palliative care utilisation, particularly how clinical characteristics and specific palliative care needs influence the use of different types of palliative care services. This area warrants further investigation to better tailor palliative care services to the unique requirements of this group.
Therefore, our study used a nationwide sample of deceased cardiovascular patients to investigate: 1) patients’ symptoms and functional burden on their first admission to specialist palliative care services, and 2) how patients’ symptoms and functional burden and other clinical characteristics affected their utilisation of community-based versus inpatient palliative care services. Our findings have the potential to guide policy development, optimise resource allocation and enhance the training of healthcare professionals to improve the delivery of palliative care services tailored to the needs of patients with CVDs.
Materials and methods
Data source
Our study used anonymised patient outcome data from the Australian palliative care outcomes collaboration (PCOC), a national, government-funded initiative by the Australian Health Services Research Institute.20 The PCOC aims to enhance the quality of palliative care through a systematic process involving routine assessments, measurement, reporting of patient outcomes and benchmarking. The palliative care services registered with PCOC assess clinical outcomes of their patients using validated and standardised tools (refer to data collection tools below).
Inpatient palliative care services conduct these assessments at admission, every 24 hours thereafter and at discharge to guide patient care. Community-based palliative services perform assessments on admission, during each subsequent patient contact and at discharge. These assessment results are submitted to PCOC biannually, and PCOC processes these data for validation and quality assurance. Based on this data, the PCOC national office generates biannual reports on clinical performance for each participating service. These services can then benchmark their performance against national averages and industry-agreed standards, fostering an environment of continuous improvement in palliative care.
Study population and settings
This study included individuals who satisfied the following criteria: (1) accessed specialist palliative care from Australian services registered with PCOC; (2) had CVD identified as the primary life-limiting condition necessitating palliative care; (3) their initial palliative care episode and death occurred between 1 January 2013 and 31 December 2022. The study specifically focused on the initial assessment conducted at the admission to the first episode of palliative care for each patient. An ‘episode of care’ is defined as a continuous period of care provided to a patient in a single care setting. The study examined patients from two categories of episodes: those in community-based settings and those in inpatient facilities. ‘Inpatient episodes’ document one of the overnight admitted options: designated palliative care beds or non-designated palliative care beds. ‘Community episodes’ document one of the community options: private residences or residential aged care facilities.
Variables and data collection tools
The palliative care services registered with PCOC evaluate patients’ clinical outcomes using five standardised and validated tools:
PCOC symptom assessment scale (PCOC SAS): an 11-point scale ranging from 0 (absent) to 10 (worst possible), used to measure distress from common symptoms requiring palliative care, such as sleep difficulties, appetite issues, nausea, bowel problems, breathing difficulties, fatigue and pain.21 This assessment is preferably done by patients; however, proxy assessment is also acceptable when direct patient reporting is not feasible.
Palliative care problem severity score (PCPSS): clinicians use this tool to assess the global severity and complexity of patients’ palliative care problems, including pain, other symptoms and psychological/spiritual and family/carer issues.20 PCPSS is a 4-point scale where 0 indicates absence and three signifies severe problems.
Resource Utilisation Groups–Activities of Daily Living (RUG-ADL): this tool evaluates patients’ functional dependency levels in activities such as eating, toileting, bed mobility and transfers. Eating was assessed on a 3-point scale (1 for independent or supervision only, 3 for total dependence/tube fed) and the other activities on a 4-point scale (1/2 for independent and monitor, 5 for assistance from two or more persons).22
The Australia-modified Karnofsky Performance Status (AKPS) Scale evaluates a patient’s performance in terms of activity, work and self-care. Clinicians assign a single score ranging from 0 to 100, based on their observations of the patient’s ability to perform typical tasks related to these dimensions. A score of 100 represents normal physical abilities with no signs of disease, while lower scores indicate diminished performance. A score of 0 signifies that the patient has died; however, this score is not used in the PCOC because no further assessments are conducted after a patient’s death.20
PCOC palliative care phases: the non-sequential PCOC palliative care phases which describe four distinct, clinically meaningful phases of palliative care (ie, stable, unstable, deteriorating and terminal) were determined by clinicians based on comprehensive clinical assessments of the patient and their family. The palliative care phase identifies a clinically meaningful period in a patient’s condition and serves as the foundation for developing palliative care casemix classification. Detailed definitions of each phase can be found in the study by M. Masso et al20
Other variables included in this study involved demographic data such as sex, age group, country of birth, preferred language, referral source, year of admission, episode length, phase length, Socio-Economic Indexes for Areas (SEIFA) and place of death. SEIFA is a summary measure of social and economic conditions developed by the Australian Bureau of Statistics.23
Statistical analysis
We described the characteristics of patients, their care episodes and clinical measures using frequency distributions and percentages. Differences between the two groups (inpatient vs community) were assessed using Pearson’s χ2 tests.
To investigate the impact of patients’ functional and symptom burden, and other clinical characteristics on the utilisation of inpatient versus community palliative care services, we employed multivariable logistic regression models. Significant factors associated with the utilisation of different specialist services were identified through backward stepwise regression procedures. Due to substantial multicollinearity among elements of the RUG-ADL scale, only the ‘total RUG-ADL’ score was included in these stepwise analyses. The criteria for inclusion and exclusion in the models were set at significance levels of 0.05 and 0.10, respectively. The model’s fit was evaluated using the C-index, and p values for trend were calculated. In our analyses, patients admitted to community-based services served as the reference group.
In our regression analyses, scores on the PCOC SAS, total RUG-ADL and AKPS were reclassified as categorical variables as follows: PCOC SAS: since <11% of patients had scores >1 on four PCOC SAS symptom scores, the PCOC SAS was categorised into 0=absent (PCOC SAS=0), 1=mild (PCOC SAS=1–3), 2=moderate (PCOC SAS=4–7) and 3=moderate (PCOC SAS=8–10). AKPS: the categorisation for AKPS was 1=normal activity (AKPS=90–100), 2=symptomatic and ambulatory (AKPS=70–80), 3=occasional assistance required (AKPS=60), 4=increasingly limited mobility (AKPS=30–50) and 5=completely bedfast (AKPS=10–20). RUG-ADL: the categories for RUG-ADL were defined as RUG-ADL: 0=independence or supervision only (total RUG-ADL=4–5), 1=limited physical assistance (RUG-ADL=6–13), 2=one assistant plus equipment (RUG-ADL=14–17) and 3=two assistants for full care (RUG-ADL=18).
We also fitted Kaplan-Meier curves and performed log-rank tests to compare survival time after the first episode of palliative care admission for the two groups.
Patient and public involvement statement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Results
The characteristics of the study cohort and the community and inpatient episodes are shown in online supplemental table 1. The study cohort comprised 17 002 patients, of which 51.8% were male, and 57.1% were aged 85 years or older. Additionally, 61.6% of patients were referred from a hospital, followed by 33.0% referred from a community service. At the time of accessing palliative care, nearly half (49.8%) of patients were in the deteriorating phases.
Supplemental material
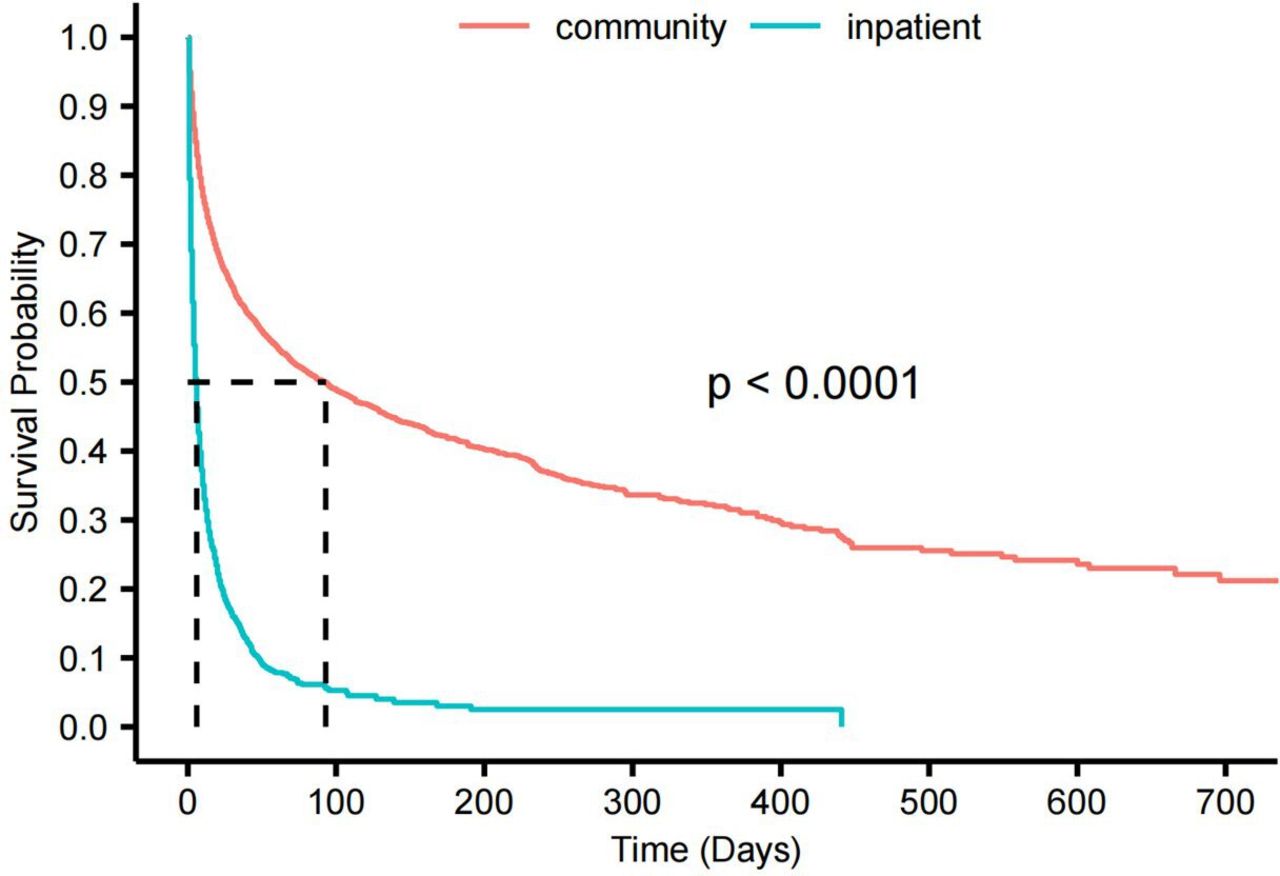
Within this cohort, 44.3% were from community-based palliative care services and 55.7% were from inpatient palliative care services. Compared with the inpatient group, patients in the community group were more likely to be female (p<0.001) and older than 85 years (p<0.001). A significantly higher proportion of patients in the inpatient group had an episode length of less than 1 week (p<0.001) and were referred from a hospital. Patients in the community group were predominantly assessed as being in the deteriorating (56.9%) and stable (29.5%) phases, while the inpatient group was predominantly assessed as deteriorating (44.1%), followed by terminal (22.6%) and unstable (20.3%) phases (p<0.001). The survival curves indicate that the community group had a significantly longer survival time compared with the inpatient group, suggesting that community episodes of palliative care services were initiated much earlier than inpatient episodes (figure 1). Clinical outcome measures for both groups of patients are shown in online supplemental table 2. Overall, patients in both groups exhibited high levels of functional and performance impairment, with one-third being completely bedfast (AKPS score=10–20) and requiring two assistants for full care (Total RUG-ADL scores=18). Significant differences in function and performance impairment were observed between the two groups. The proportions of patients in the inpatient group requiring two assistants for full care (43.30% vs 20.25%) or being completely bedfast (46.91% vs 20.59%) were more than double those of the community group (p<0.001). Regarding the SAS assessments, severe levels of distress were uncommon across all symptoms. Fatigue and breathing problems were the top two sources of distress, causing moderate and severe levels of distress in more than one-third of patients. In terms of assessments for PCPSS, approximately one-third of patients experienced moderate and severe levels of problems related to other symptoms and family issues, compared with nearly 15% for psychological problems and pain. A significant disparity in symptom burden was observed between the two groups. Most often, the inpatient group had higher proportions of absent category, fewer mild category, and equivalent moderate category across all symptom assessments (p<0.001 for each). The differences in the severe category between the two groups were not evident due to the small proportion of this category for both groups.

{kind=link}
Survival curves for patients with cardiovascular disease referred to inpatient versus community palliative care services. Comparison between the two groups was performed using log-rank tests.
Online supplemental table 3 presents the adjusted and unadjusted OR for predictors of inpatient service utilisation, using community-based services as the reference group, as determined by a multivariate logistic regression model with a c-statistic of 0.89. Only the adjusted ORs are reported here. Among sociodemographic factors, higher SEIFA scores (adjusted OR ranged from 1.34 to 2.18; p<0.001) are positively associated with using inpatient services. Conversely, female patients (adjusted OR: 0.82; 95% CI: 0.73 to 0.91; p<0.001), older age (adjusted ORs ranged from 0.52 to 0.81; p<0.001), being born in a country other than Australia (adjusted ORs ranged from 0.58 to 0.88; p<0.001), and years closer to 2022 (adjusted ORs ranged from 0.42 to 0.85; p<0.001) were negatively associated with accessing community-based services. As indicated by the p values for trend, dose-response associations were observed for the factors of ages (p<0.001), SEIFA (p<0.001) and years of admission (p<0.001).
In terms of clinical characteristics, the most significant factor predicting the use of inpatient services was patients being assessed in the unstable phase (adjusted OR: 17.60; 95% CI: 14.15 to 21.90; p<0.001). Higher scores on RUG-ADL and lower scores on AKPS were linked to an increased likelihood of entering inpatient services. Regarding symptom burden, moderate (adjusted OR: 1.20; 95% CI: 1.02 to 1.40; p=0.024) and severe (adjusted OR: 1.74; 95% CI: 1.32 to 2.29; p<0.001) breathing problems assessed by PCOC SAS, as well as severe bowel problems (OR: 1.72; 95% CI: 1.03 to 2.86; p=0.038), positively predicted use of inpatient services compared with absence of these symptoms. Conversely, from mild to moderate levels, symptoms such as insomnia, fatigue and family issues assessed by PCPSS were consistently associated with lower odds of using inpatient services. Additionally, dose-response associations were identified for all symptom and function-related factors, with a p value for the trend of less than 0.001 for each.
Discussion
Our population-based national study examined the symptom and functional burden of CVD patients on their first admission to specialist palliative care services, as well as how these burdens and other clinical characteristics influenced their use of different types of specialist services in Australia. Compared with the community group, the inpatient group exhibited significantly greater dependency and poorer performance, yet reported higher proportions of absent symptom burden and fewer instances of mild symptom burden. An unstable palliative phase, along with greater dependency and poorer performance, predicted the use of inpatient services. Surprisingly, increased symptom burden was often associated with a lower likelihood of using inpatient services compared with community services.
Previous studies have extensively documented that fatigue, breathing problems and functional disabilities are common among palliative care patients with CVD.4 19 24–26 In our study, patients reported higher levels of distress from fatigue and breathing problems compared with other symptoms. These two symptoms, which are often prevalent and concurrent, pose significant management challenges and are closely linked to impaired quality of life in CVD patients. For instance, a 2019 multicentre study in the US involving 1801 palliative care patients with CVD found that the most common symptoms were tiredness (50.3%), anorexia (35.7%) and dyspnoea (27.9%).26 Additionally, 38.9% of these patients were bedridden and fully dependent,26 a finding consistent with our study’s report of 35.17% of patients being completely bedfast. Beyond symptom management, our study also underscores the importance of addressing family needs and issues, a concern that has been increasingly emphasised in the international palliative care literature.
Our study compared the symptom burden and functional impairment between patients referred to community and inpatient services. We discovered that inpatient groups generally reported higher functional disability and lower symptom burden than their community counterparts. The findings regarding function were plausible, given that the inpatient group had a much shorter survival time and a significantly higher proportion of patients in the unstable and terminal stages compared with the community group. However, the findings that the inpatient group reported lower symptom burdens were unexpected and inconsistent with our previous studies focusing on the PCOC cohorts of lung cancer,27 dementia28 and stroke.29 One possible explanation relates to referral sources: 83.1% of inpatient group patients were referred from hospitals, while 56.5% of community group patients were referred from community services. It is likely that hospital-referred patients had better-managed symptoms before being referred to palliative care services. Nevertheless, given that palliative care focuses on symptom management, these findings necessitate further exploration of the determinants for patients accessing different types of palliative care services.
Our analyses contributed new insights by identifying the factors that predict the use of inpatient services compared with community-based services. We found that patients from areas with higher social and economic conditions were more likely to use inpatient services. This is likely attributable to the fact that most Australian palliative care workforce are employed in hospital settings in major cities.30 Additionally, our regression model indicated that community services were more widely used in most years between 2014 and 2022 compared with 2013, although the pattern did not persist after 2020, possibly due to the impact of COVID-19. This finding suggests that the efforts of advocacy for increased use of community services have been effective.31 32 Unsurprisingly, referrals from hospitals strongly predict the use of hospital palliative care services, given that many hospitals have palliative care units or designated palliative care beds. We also identified that being female and older age was associated with a higher likelihood of using community palliative care services. Further studies are needed to explore the underlying reasons for these associations.
Inpatient services, equipped to provide around-the-clock specialised care, can promptly address patients’ complex and urgent symptom management needs.15 However, our analysis showed that a higher symptom burden was not consistently linked to the use of inpatient services compared with community services. Instead, individuals with a higher symptom burden were more likely to access community services in most situations. These findings indicate that the delivery of palliative care services for patients with CVD could benefit from promoting a needs-based care model. However, consensus on need-based palliative care referral criteria in patients with CVD remains lacking.18 33 It should also be noted that the lower symptom burden observed in the inpatient group was likely due to decreased activity levels, given the substantially higher proportion of bedfast patients in this group compared with the community group. Elevated clinician-rated scores for family issues were also associated with a lower likelihood of using inpatient services in our study. This could be because community healthcare providers, who are more familiar with the family than hospital providers, tend to rate family burden and concerns higher.
There was a higher utilisation of inpatient services associated with higher levels of dependency and lower functional performance status. Relocating these individuals to an inpatient setting and abruptly altering their living environments may cause increased distress, confusion, and a heightened risk of falls and injuries. For most people in our study without severe or complex symptoms, a more patient-centred management model, based in their usual residence and involving highly trained staff to support families and caregivers, would be optimal. Therefore, a community-based model is suitable for patients with major functional disabilities but not experiencing severe symptoms.
Moreover, community-based palliative care services have gained popularity not only because they are more cost-effective compared with inpatient services,34 but also because they facilitate continuity of care by maintaining connections with the patient’s regular care providers and enabling patients to stay and die at their preferred place.34 However, it is important to note that home-care arrangements demand significant physical, emotional and financial commitment from families and caregivers. Many families and caregivers may become fatigued and overwhelmed or feel unsafe as the patient’s condition worsens or if unexpected health changes occur. A common reaction in these situations is to seek institutional care. This aligns with our findings, which indicate increased access to inpatient services for individuals in non-stable (especially unstable) palliative care phases compared with the stable phase. Enhanced support for carers and families of people with CVD tends to facilitate longer periods of home care.25
Strengths and limitations
To our knowledge, this is the first large-scale, national study that comprehensively examines the clinical characteristics, care needs, and their associations with the use of different types of palliative care services specifically for people with CVD in Australia. While the analyses were enhanced by the use of standardised and validated instruments at the point of care, several limitations should be acknowledged. First, some bias may have been introduced by the criteria used for disease classifications in these data. Given that the PCOC only captures the primary diagnosis that necessitates the episode of palliative care, patients included in this study may also have other common comorbidities except for CVD, such as diabetes and dementia. Second, our multivariate models focused on palliative care needs related to symptom and functional burden, but did not include other clinical factors (eg, need for management of oedema and cognitive impairment, etc) or social factors (eg, availability of informal carers). These significant and unique characteristics of advanced CVD are important considerations in decisions about the types of services to use. Third, the inpatient groups likely had a higher rate of proxy-reported SAS assessments compared with the community groups, given that more patients in the inpatient group were at a later stage of life. The potential discrepancies between patient-reported and proxy-reported outcomes may have introduced bias into our data. Given these limitations, the symptom outcomes reported in this study should be interpreted with caution.
Conclusion
On admission to specialist palliative care services, patients with CVD exhibit high degrees of physical impairment and distress associated with fatigue and breathing problems. Comparatively, patients entering inpatient services required higher levels of physical assistance but often reported lower levels of symptom burden. Our most notable finding is that elevated symptom distress and difficulties in managing these symptoms unexpectedly predicted a decrease in the utilisation of inpatient services compared with community services. Based on these findings, we concluded that there is a significant need to develop a CVD-specific palliative care pathway or referral guidelines to promote needs-based palliative care delivery models. Such a model could enable a larger number of people with advanced CVD to receive care and spend the end of life in their usual accommodations. Promoting these models would require greater investment in supportive services, such as skilled palliative care staff and support for carers, in the community.
Data availability statement
Data may be obtained from a third party and are not publicly available. All our data are from Australian Palliative Care Outcomes and Collaboration (PCOC), which could be applied for access through their website: PCOC Research Data. (https://www.uow.edu.au/australasian-health-outcomes-consortium/pcoc/research-data/).
Ethics statements
Patient consent for publication
Ethics approval
The PCOC programme has been approved by Human Research Ethics Committee (HREC) of the University of Wollongong (HE06/045) and this study was granted wavier of consent by The University of Western Australia HREC (RA/4/1/8365).
References
Footnotes
Contributors XQ conceived the concept, designed the study. ML drafted the manuscript, conducted data analysis and interpretation together with SQ and HL. YL conducted literature review. JD provided served as the guarantor, led the data application from the Palliative Care Outcomes Collaboration. XQ, ML, SQ, HL, YL, MT, HT, and JD critically reviewed and provided feedback on the manuscript. All authors approved the final version for submission.
Funding This study is supported by Hunan Provincial Natural Science Foundation of China (#2023JJ40791). The funder had no role in the conduct of the study.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.