Article Text

Abstract
Introduction Diet and nutrition play a vital role in all stages of chronic kidney disease (CKD) prevention, treatment and management. In particular, dietary interventions are essential to manage hyperphosphataemia, a common metabolic complication in CKD consistently associated with an increased risk of cardiovascular disease and all-cause morbidity and mortality. Unfortunately, dietary management of any kind in this cohort of patients also comes with the added challenge of limited and variable access to renal dietitians, logistical difficulties and multiple medical appointments. Given the complexity of managing diet in patients on dialysis, there is a need for novel interventions that not only help patients navigate daily challenges but could also be integrated into clinical practice to support the work of dietitians. We are testing if the use of digital health (via a new, specifically designed smartphone App) plus standard care compared to standard care alone is a feasible and effective method of delivering nutritional advice to patients with elevated phosphate levels undertaking dialysis.
Methods and analysis This is a multicentre codesigned randomised controlled trial (RCT) that will recruit individuals aged 18 years or over on maintenance dialysis for a minimum of 3 months who have a serum phosphate level of ≥1.6 mmol/L. Participants will be recruited from 23 different dialysis sites across Australia. They will be block randomised into two groups in a 1:1 ratio that will either be the intervention group (receive the TeleKinesis App for 3 months in addition to standard care) or the control group (standard care alone). The primary outcome of the study is to assess the effect of this intervention on the change in patients’ serum phosphate levels. The RCT will assess the effectiveness of the programme by comparing serum phosphate at baseline, 3 months and follow-up at 6 months. A total recruitment target of n=180 participants is expected.
Ethics and dissemination Ethics approval was received from the Sir Charles Gairdner and Osborne Park Health Care Group Human Research Ethics Committee on 5 December 2022 (reference RGS0000005559). Informed consent will be given by participants once they have read and signed the patient information and consent form. The results are expected to be published in scientific journals and presented at clinical research conferences and to the consumers who have taken part in the trial. This is protocol 1.0 dated 10 November 2024.
Trial registration number ACTRN12621000746831.
- Dialysis
- Digital Technology
- NUTRITION & DIETETICS
- Health Education
- Biochemistry
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study. No data available as this is a protocol.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The intervention will be evaluated in a randomised controlled study with outcome assessors and a statistician blinded to participant allocation.
This is a multicentre trial across patient groups with diverse ethnicity and age, improving the generalisability of the study findings.
The ownership of mobile phones is high in patients with chronic kidney disease.
The use of consumer involvement in the development and study design will increase its acceptability, suitability and relevance to the target population.
The primary limitation of this study is the exclusion of patients with low digital literacy, insufficient English language skills or a poor internet connection.
Introduction
Hyperphosphataemia is one of the most prevalent metabolic complications in patients with chronic kidney disease (CKD), with elevated serum phosphate levels consistently associated with an excess risk of cardiovascular disease and all-cause morbidity and mortality.1 Reports indicate that over half of patients on haemodialysis have pre-dialysis hyperphosphataemia.2 3
Appropriate, timely and effective dietary interventions are recognised as an essential component to achieving normal serum phosphate.4 Traditionally, tight restrictions of dietary phosphorus have been considered the core strategy to avoid harmful elevated blood levels that are associated with poor clinical outcomes. However, dietary interventions to optimise phosphorus management in people with CKD remain a challenge due to the complexity of the diet, the risk of malnutrition and common comorbidities.
As new guidelines, evidence and understanding of the bioavailability of this nutrient become clearer, there is a need for this to be translated effectively to the person with CKD.5 Evidence from observational studies has also shown more favourable outcomes with a more liberalised plant-based diet.6 This also supports dietary recommendations for healthy heart advice and reduction of gut issues (gut dysbiosis), both common in CKD.7
The recent Kidney Disease Outcomes Quality Initiative guidelines for management of nutrition in CKD4 recommend that adults with stage 3–5 CKD adjust their dietary phosphorus intake to maintain normal serum phosphate levels. For all adults with CKD or post-transplant, it is reasonable to consider the bioavailability of different phosphorus sources (such as animal, vegetable or additives) when making decisions about phosphorus restriction treatment. However, there is little high-quality evidence to guide clinical management of hyperphosphataemia or to indicate the recommended amounts of different dietary sources of phosphorus.8
Unfortunately, dietary management of elevated serum phosphate also comes with logistical challenges. Factors such as limited and variable access to renal dietitians,9 low patient-to-dietitian ratios, geography, complex and competing medical issues and multiple, overlapping medical appointments make it difficult to coordinate access with a renal dietitian. Tertiary outpatient services often lack the resources to provide the required frequent and intensive dietetic contact necessary to support the required sustained behavioural change.10–12
Given the complexity of managing diet in patients on dialysis, there is a need for novel codesigned evidence-based approaches that can help patients navigate daily challenges that can be integrated into routine clinical practice to support the work of dietitians while minimising face-to-face appointments.13–15
Digital health solutions are a promising approach to deliver timely evidence-based nutritional care, with the potential to complement in-person appointments which are hampered by long waiting times. Incorporating patient choice of intervention may also lead to improved engagement and clinical effectiveness.16 17 Digital health (also known as telemedicine, eHealth, eMedicine and virtual health care) has become an acceptable and effective method of communication and delivering health-related education resources following expanded use during the COVID-19 pandemic. Delivered via the web, telephone and text messaging, digital health has been promoted as a potential platform to meet increasing demands and deliver nutritional care. Its many advantages include an exceptional level of patients’ and providers’ convenience, a high level of efficiency, delivery of continuous and potentially updated information that is otherwise not possible and increasing use by dietitians including renal dietitians.18
Digital health interventions can also increase flexibility in access and improve patient engagement via personalised care options.19 Due to its accessibility and reach, digital health has the potential to engage with a more diverse group of patients.20 This includes rural and remote communities, the latter of which have almost no access to a renal dietitian. Other studies looking at patient readiness, interest and capability of using mobile health concluded that digital health could provide an important alternative and/or supplemental resource for patients and families.21–23
Nutrition education via a smartphone application (Apps) has been shown to be effective in improving outcomes in patients with diabetes, weight management and smoking. A systematic review of evidence suggests that digital health tools can positively influence dietary sodium intake and fluid management among individuals with CKD by promoting behavioural changes. However, the quality of the studies was low, and the effectiveness of these interventions remains uncertain due to methodological shortcomings and the wide variety of digital health approaches and intervention types.24 Participants in studies of digital interventions report high satisfaction levels with digital health interventions based on them being informative, with low user burden, and easy to understand. Furthermore, a recent qualitative systematic review concluded that patients felt that digital health interventions were an important way of accessing lifestyle services.25 However, people with CKD and healthcare professions both report a major knowledge-practice gap regarding ‘how these interventions can be implemented into everyday use.’26
While text messaging is readily available, the potential of a targeted phosphate App for education and behaviour change has not been fully evaluated. The ability to incorporate visual elements such as pictorial messages, infographics, visual food swaps and food information could enhance its impact27 and thus reduce serum phosphate.
The primary aim of this study is to assess the effect on serum phosphate of a novel codesigned smartphone App (The TeleKinesis App) that delivers nutritional education plus standard care compared to standard care alone.
Methods and analysis
Study design
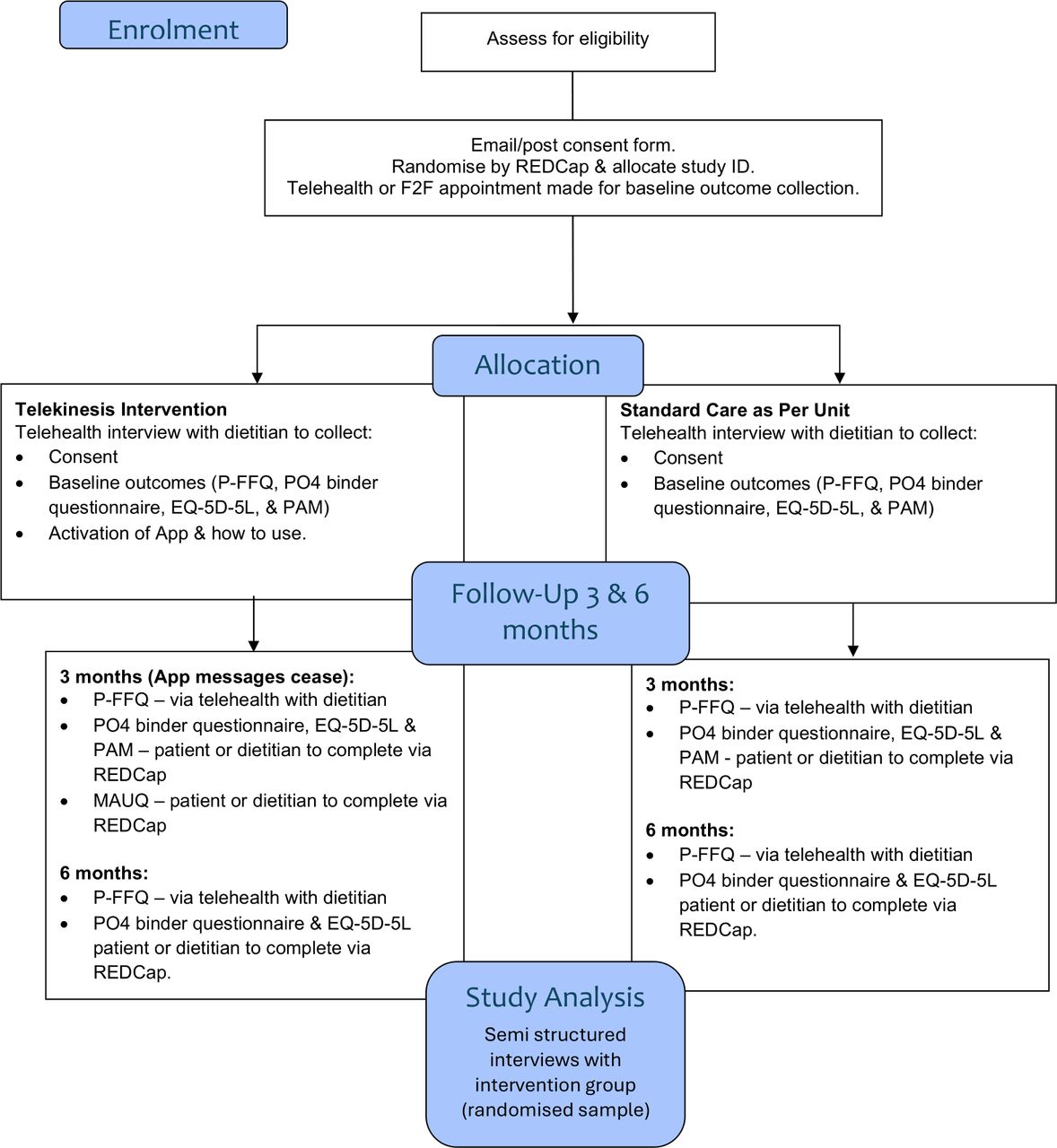
The TELEnutrition and KIdNey hEalth is a randomised controlled trial comparing the effect of digital health to standard care on serum phoSphate control in patients on dIalysiS (The TeleKinesis Study). It includes a 3-month period of intervention with a 6-month follow-up. Patients will be randomised to either TeleKinesis App plus standard care (intervention group) or standard care alone (control) in a 1:1 ratio. The intervention group will receive biweekly dietary phosphorus education via smartphone App for 3 months (figure 1). This protocol uses the Standard Protocol Items: Recommendations for Interventional Trials reporting.28

The TeleKinesis Study design and flow. REDCap, Research Electronic Data Capture; ID, unique number assigned to participant; F2F, face to face; P-FFQ, phosphate food frequency questionnaire; PO4, serum phosphate; EQ-5D-5L, quality of life questionnaire; PAM, patient activation measure; MAUQ, mHealth App usability questionnaire.
Study setting
The study is being conducted in 23 dialysis units throughout Australia, in both the hospital and satellite setting, that serves ethnically, culturally and socioeconomically diverse populations (figure 2). Recruitment (metro, rural and remote) commenced in July 2023 and concluded in December 2024. The final 6-month follow-up expected to be completed by the end of June 2025.

Map of recruiting sites.
Recruitment
Patients receiving maintenance haemodialysis or peritoneal dialysis will be identified in nephrology outpatient clinics and satellite/hospital dialysis units. A recruitment target of 180 participants (90 per group) includes an expected loss of 10% drop-out over the first 3 months of the trial. This is set to achieve the sample size calculation of 166 (83 per group) completing 3-month assessments. The original recruitment target of 200 was updated to 180 after it was recalculated at 12 months of active recruitment. This was based on the anticipated dropout rate being reduced to 10%. This was not preplanned but was used to inform the research team of an estimated time to end recruitment.
Eligibility criteria include receiving maintenance dialysis for at least 3 months, being aged 18 years or over, having a serum phosphate level >1.6 mmol/L (this will be based upon the average of a minimum of two measurements over the previous 3 months), having sufficient English language skills to read and understand App messages and having access to a smart mobile phone for the duration of the study.
Patients will be ineligible if they have been hospitalised within the last month, have had a serious intercurrent illness within the last month, if the patient is not expected to remain on dialysis for the duration of the study or if they have significant cognitive impairment or intellectual disability that would inhibit their understanding of the App messages and infographics. A screening log will be kept of patients who were approached but were deemed ineligible or declined to participate (and the reason) for final data capture which will be presented in a Consolidated Standards of Reporting Trials diagram. All participants will give informed consent via the patient information and consent form (PICF) (online supplemental file 1).
Supplemental material
Randomisation
Randomisation will be conducted via Research Electronic Data Capture (REDCap) using a computer-generated block randomised sequence. Participants will be notified of their allocation at the baseline digital health appointment. They will be asked not to disclose their allocation to any other study personnel or other patients. The participants in the intervention arm will also be instructed not to disclose the contents of the TeleKinesis App for the duration of the 6-month trial to ensure that those randomised to the control arm are not unduly influenced.
Intervention
The control group will continue to receive standard care (eg, nutritional assessment and education or review assessment and counselling on request of the renal team) as per normal procedure for their treating unit for the duration of the study. The TeleKinesis intervention group will receive standard care plus education on reducing phosphorus intake via biweekly targeted App messaging, infographics and visual animations over the 3-month intervention period (figure 3). For instance, as part of their first message, their baseline serum phosphate will be uploaded onto the App with the target levels displayed in a graph. After the 3-month intervention phase, all participants will go to standard care for the remaining 3 month-follow-up phase of the 6-month study.

{kind=link}
{kind=link}
{kind=link}
The TeleKinesis Study dashboard page and sample messages (a) Home page. (b) Sample of infographic. (c) Weekly summary from the renal dietitian. (d) Weekly quiz from the nephrologist.
The messages/infographics will be unidirectional and will be delivered on Monday and Thursday every week. This mode of communication has been shown to be an effective, timely and low-cost strategy in improving general dietary behaviours in patients with CKD and end-stage kidney failure.15 The intervention is aimed at supporting a healthy dietary pattern that includes modification of highly bioavailable dietary sources of phosphorus and phosphate binder education, as well as simple swaps, eating out, safe snacks and understanding food labels. This intervention will be in addition to standard care.
TeleKinesis messaging development
A series of messages and infographics has been developed based on evidence-based guidelines on the management of hyperphosphataemia.4 The message development was completed using the behaviour change framework and included peer review by renal dietitians, nephrologists and renal nurses and was granted ethics in December 2022. It was also assessed for readability using the Flesch-Kincaid reading scale. The final draft of all messages was reviewed by people with lived experiences and/or carers.
Patient and public involvement
In 2022, we collaborated with individuals with experience of kidney disease to explore their perspective of current dietary advice and their experience using telehealth technology to access their medical team or other uses.20 Three focus groups and three individual telephone interviews with 22 patients (including five carers) with kidney failure maintained on haemodialysis and peritoneal dialysis were conducted. We sought their experiences on receiving dietary advice, the timing, type and the use of digital health as an option to receive nutritional education, prompts and information. The findings have been published and informed the design and development of the TeleKinesis App into a 12-week programme delivering biweekly messages in the form of words, infographics and quizzes. Once developed, patients were asked to review a draft of the programme and inform us of its acceptability before finalising it and uploading it onto the App. There was no patient or consumer involvement in the trial management. At the completion of the trial, we will disseminate deidentified findings from the trial to the study participants and the dialysis units that completed the trial.
Outcome measures
The primary outcome will be measured as the change in serum phosphate levels between baseline and at 3 months. Serum phosphate levels will be retrospectively collected from routine care measurements taken pre-dialysis session over the 2 months prior to the baseline digital health appointment. Further serum phosphate levels will be obtained at baseline, 1, 2, 3, 4, 5 and 6 months (as part of routine care). The primary outcome will be the difference between the two groups in the change in serum phosphate at baseline compared to follow-up. This will equal the average of the 1-, 2- and 3-month serum phosphate minus the average baseline serum phosphate (baseline, −1 and −2 months).
Alongside the primary outcome, comparisons will also be made between groups with respect to serum phosphate levels at the following:
Baseline versus month 1; month 2; month 3; month 4; month 5; month 6; average of months 1 and 2; average of months 2 and 3.
Month 6 and month 3; month 6 and baseline.
Average of months 4 to 6 and average of months 1 to 3.
Secondary outcomes
Feasibility of the study will be assessed using acceptability of the intervention, assessment of implementation, adherence to dietary and medication recommendations, recruitment and retention rates. Other validated questionnaires will capture different aspects of self-management, lifestyle behaviours and quality of life. Data will be collected using the following:
Acceptability: Acceptability will be measured using the mHealth App Usability Questionnaire.29 This validated measure (online supplemental file 2) will only be conducted in the intervention group and will be collected at the end of the 3-month intervention. Additional semi-structured interviews (online supplemental file 3) will be conducted in approximately 20% of the intervention group to further determine acceptability and undertake a process evaluation.
Adherence to dietary recommendations: This will be measured using the validated Phosphate Food Frequency Questionnaire (P-FFQ).30 Dietary phosphorus intake will be measured at baseline and after the 3-month intervention phase and compared between groups. A similar analysis will be performed comparing dietary intake at 6 months versus 3 months and 6 months versus baseline (online supplemental file 4).
Adherence to medication recommendations: Phosphate binding medication-taking behaviour will be measured using a phosphate binder questionnaire. The difference in ‘actual number’ of phosphate binders at 3 months versus baseline, 6 months versus 3 months and 6 months versus baseline (online supplemental file 5).
Quality of life: Quality of life will be measured using the quality of life questionnaire (EQ-5D-5L).31 Differences between groups will be assessed based upon the change in scores at 3 months versus baseline (online supplemental file 6).
Patient knowledge and ability to self-manage: This will be assessed using the PAM-13,32 the most widely used instrument for measuring patient activation and has been validated and recommended for use in those with kidney disease. The PAM-13 assesses patients’ knowledge, skills and confidence in managing their own health. This will be measured at baseline, 3 months and 6 months (online supplemental file 7).
Assessment of implementation fidelity: The engagement, usage, quiz completion and infographic downloads will be monitored, recorded and assessed as part of the App analytics provided by App consultants.
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Exploratory outcomes
Interdialytic weight gains (average of the previous three haemodialysis sessions): This will be measured at baseline, 3 months and 6 months.
Cost analysis: A cost-effectiveness evaluation from a health system perspective with a 12month- time horizon will be undertaken comparing costs of the intervention with standard care. The analysis will be undertaken and reported in accordance with the Consolidated Health Economic Evaluation Reporting Standards33 and include the following:
Cost of the intervention. This will include the development costs, costs associated with sending messages and costs to administer the app (including web hosting, support and maintenance). The time required to administer the app by the dietitians and the training time required for dietitians unfamiliar with the use of the app will also be recorded.
Cost of standard care including dietitians’ time (salary) and cost of traditional education materials.
Estimate of costs associated with healthcare resource use over the duration of the trial for the intervention and control groups.
Quality-adjusted life years (QALYs) will be calculated using quality of life information from the EQ-5D-5L.31 The EQ-5D-5L will be conducted at baseline, 3 months and at completion (month 6).
The cost-effectiveness will be assessed based on incremental cost-effectiveness ratios calculated as the incremental cost to achieve a clinically meaningful change in the primary outcome and to achieve one QALY.
Other outcome measures
Semi-structured interviews (with approximately 20% of the intervention participants or until theme saturation) will be conducted by the principal investigator. The aim of these interviews will be to explore perspectives on trial participation, use and acceptability of the intervention (App) and thoughts on future app development. See table 1 for study time points and data collection timing.
Study timepoints and data collection timing
Dietary analysis
Dietary intake will be measured using the P-FFQ.30 Nutrient analysis will be conducted using FoodWorks V.10 (Xyris Software (Australia) Pty).
Statistical analysis
A minimum sample of n=166 (n=83 per group) has 80% power to detect an effect size of 0.19 in a linear mixed model comparing two groups across two timepoints, with alpha=0.05. This effect size is based on a mean phosphate level decrease of 0.24 mmol/L (minimal clinically important difference) in the intervention group from a minimum mean phosphate level of 1.40 mmol/L in the control group, with a pooled SD of 0.63 mmol/L. These values are derived from summary measures in a recent systematic review8 of phosphorus-specific diet therapy in phosphate levels in adults on maintenance haemodialysis. To attain a sample size of n=166 to complete the study follow-up, it is anticipated that at least n=180 participants are required to account for 10% expected loss to follow-up in the cohort (G*Power 3.1.9.7).
Participant data will be block randomised within sites. Descriptive summaries of baseline participant data will include means and SD for normally distributed continuous data and medians and interquartile ranges for non-normally distributed continuous data. Normality of data will be assessed graphically and with Shapiro-Wilk tests. Categorical data will be summarised using frequency distributions (n, %). Differences in longitudinal outcomes between control and intervention groups will be assessed using Generalised Linear Mixed Models (GLMM) with group-time interactions and nested random effects for participants and sites. Results will be summarised using marginal means and 95% CIs, with pairwise contrasts assessing differences between groups over outcome-specific time points. Models will be adjusted for covariates that have known associations or biological effects on outcomes. These include (but are not limited to) age, gender, dialysis vintage, type and medical history such as diabetes, coronary artery disease and cancer. Data will be analysed as per the intention to treat protocol using Stata 17.0 (StataCorp, College Station, Texas, USA).
The economic evaluation is to be conducted as a complete case cost-effectiveness analysis using a health system perspective for the analysis and a 12-month time horizon. Health outcomes in the economic evaluation will include QALYs and adherence to dietary recommendations. A generalised linear model will be used to calculate the marginal effects on cost of participant characteristics, QALYs, adherence to dietary recommendations and the intervention.
Risk mitigation
To minimise any safety concerns, the research team will ensure the treating team and haemodialysis unit are educated about the intervention. In particular, that this is supplementary to standard care. Normal referrals should still be made to the appropriate discipline as per site protocols and clinical need. Participants will be advised to avoid reading App messages while driving, operating machinery or conducting other activities in which normal safety measures should be followed.
Data management
All research files and data collected as part of the study from the App will be kept up to 7 years in a secure environment (eg, locked filing cabinet in the research office or equivalent) and password-protected electronic files, for example, REDCap. Each study site will have a copy of its own specific data management plan.
Ethics and dissemination
This study received full ethics approval from the Sir Charles Gairdner and Osborne Park Health Care Group Human Research Ethics Committee on the 5 December 2022 (reference RGS0000005559). Informed consent will be given by participants once they have read and signed the PICF (online supplemental file 1). The findings of this study will be disseminated via scientific forums including peer-reviewed publications and presentations at international conferences and to the consumers who have taken part in the trial.
Discussion
This study aims to evaluate the effectiveness of a novel smartphone app-based intervention to improve dietary adherence in a population of haemodialysis patients and reduce serum phosphate levels. The intervention will leverage widely accessible and user-friendly technology to complement existing dietary care, providing patients with consistent support, especially those residing in resource-limited or geographically isolated regions. It is noted that the study does have some limitations. Maintaining user engagement with an app can be challenging, possibly leading to lower adherence to dietary recommendations over time. Additionally, the exclusion of patients with low digital literacy, insufficient English language skills and poor internet connection may reduce diversity.
Key objectives include determining the optimal content, level of personalisation, frequency and timing of message notifications, as well as the extent of interaction required between healthcare professionals and patients. This will inform researchers on how to reduce limitations with future interventions. The TeleKinesis Study will generate robust evidence regarding the feasibility, effectiveness and cost-benefit ratio of an app-based intervention in enhancing dietary behaviours and clinical outcomes among haemodialysis patients. Given the critical role of dietary adherence in improving quality of life and clinical outcomes for this population, this intervention holds significant potential as a scalable and accessible approach to improving patient care.
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study. No data available as this is a protocol.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Sir Charles Gairdner and Osborne Park Health Care Group Human Research Ethics Committee (reference RGS0000005559). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors would like to thank the participants from the focus groups for their time and perceptions that helped develop the design of the intervention. The authors would also like to thank the following consumers and health professionals who assisted with the design and reviewed the content of the TeleKinesis App: Ellen Bettridge, Ruth Dumont, Hooi-Ling Fong, Catherine Keane, Katie Lenhoff, Kayla Palmer, Amy Thomson and Karen Walsh.
References
Footnotes
Collaborators N/A.
Contributors JB, AJ, KL, WL, MH and NB have all contributed to (1) designing the TeleKinesis Study and trial protocol and (2) revising it critically for intellectual content. JB is responsible for data collection. Analyses will be conducted by JB, AJ, KL, WL, MH and NB. JB is responsible for the overall content as the guarantor. All authors (JB, AJ, KL, WL, MH and NB) have (3) read and approved the final manuscript and (4) are accountable for all aspects of the work.
Funding This study is funded by a Sir Charles Gairdner Hospital Research Foundation Near Miss Award. The funder had no role in the study design; in the collection, analysis and interpretation of the data; in the writing of the report; and in the decision to submit the paper for publication. The funder did not influence the results/outcomes of the study despite author affiliations with the funder.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein) or of any geographic or locational references does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.