Article Text

Abstract
Objective With the increasing prevalence of antimicrobial resistance (AMR), the rational use of antibiotics is crucial. This study aimed to evaluate the antibiotic use patterns and influencing factors of compliance in Shanxi Province Hospitals between 2015 and 2021 and provide data support for the management of antibiotics.
Design This was a retrospective observational study of trends in antibiotic use and data reporting trends in the context of antimicrobial stewardship (AMS).
Data sources The analysis involved annual antibiotic data from hospitals covered by China’s National Clinical Improvement System (NCIS). We obtained information on hospital characteristics (eg, city, a deidentified hospital code and hospital level) from Shanxi Provincial Pharmaceutical Quality Control Centre.
Eligibility criteria Our study included Shanxi hospitals that reported annual antibiotic data to the NCIS system in any year between 2015 and 2021.
Results The number of hospitals reporting antibiotic data has increased annually. Between 2015 and 2021, a total of 221 hospitals in 11 cities were analysed. The proportion of patients undergoing clean surgical procedures with prophylactic antibiotic prescriptions decreased from 45.08% to 40.0% between 2019 and 2021, with a compound annual growth rate (CAGR) of −5.80 (p=0.103). The intensity of antibiotic treatment among inpatients was from 42.00 to 39.70 daily defined dose between 2017 and 2021, with a CAGR of −1.40 (p=0.015). The proportion of inpatients with antibiotic prescriptions decreased from 51.42% to 47.14% between 2015 and 2021, with a CAGR of −1.44 (p<0.001), and the proportion of inpatients with special-grade antibiotic prescriptions decreased from 0.74% to 0.49% between 2016 and 2021, with a CAGR of −2.56 (p=0.998). The multivariable logistic regression analysis showed that public hospitals, hospitals with prescription automatic screening system (PASS), hospitals with AMS, City A, City G and City I were independently associated with the proportion of patients who used prophylactic antibiotics for patients undergoing clean surgical procedures. Hospitals with PASS and AMS, and hospitals in City A, City D, City E and City I were independently associated with the antibiotic use density. Tertiary hospitals and City C were independently significantly associated with the proportion of inpatients with antibiotic prescriptions. Hospitals with AMS and City D were independently significantly associated with the proportion of inpatients with special-grade antibiotic prescriptions (all p<0.05).
Conclusions Antibiotic consumption in inpatients decreased during the study period. However, we need to take more measures to reduce patients undergoing clean surgical procedures with prophylactic antibiotic prescriptions and inpatients with special-grade antibiotic prescriptions. Antibiotic use was associated with various hospital characteristics and geographic locations. While the provincial efforts in controlling antibiotic use show some efficacy, further enhancement of surveillance programmes and targeted interventions at the hospital level are necessary to mitigate the escalation of AMR and ensure adequate antibiotic supply for emerging infectious diseases.
- Antibiotics
- Retrospective Studies
- PUBLIC HEALTH
- Quality Improvement
- Quality in health care
- Organisation of health services
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Antibiotics
- Retrospective Studies
- PUBLIC HEALTH
- Quality Improvement
- Quality in health care
- Organisation of health services
STRENGTHS AND LIMITATIONS OF THIS STUDY
Our study utilised the NSIC database, which includes a vast number of hospitals in Shanxi, China, enhancing the generalisability of findings.
We employed CAGR to assess antibiotic utilisation trends, providing more accurate long-term insights than traditional methods.
This study is among the first to examine city-level variations as a key determinant of antibiotic compliance rates.
Due to the retrospective nature of the study, missing records might affect outcomes.
While we focused on standardised antibiotic management, future studies should explore clinical appropriateness in depth.
Introduction
The irrational use of antibiotics has driven the emergence of antimicrobial resistance (AMR), resulting in the proliferation of multidrug-resistant and pan-drug-resistant bacterial strains.1–3 This escalating crisis poses a significant global public health threat, as it significantly extends hospital stays, increases healthcare costs and exacerbates morbidity and mortality rates. The review on AMR projected that 10 million deaths caused by AMR could occur by 2050.4 5 In response, international organisations have intensified efforts to combat bacterial resistance. On World Health Day in 2011, the WHO issued an urgent call to action against drug resistance, emphasising the stark warning: ‘No action today, no cure tomorrow’. In 2015, the WHO launched the ‘Global Action Plan on Antimicrobial Resistance’. Furthermore, in 2016, the United Nations General Assembly convened a high-level meeting to address the issue of bacterial resistance. Concurrently, international bodies such as the G20 and G7 have advanced coordinated strategies to mitigate the spread of bacterial resistance.5
China also needs to address the growing public health challenges posed by AMR.6 7 In response to this critical public health challenge, the Chinese government has implemented a series of comprehensive, multifaceted interventions over the past several decades, aimed at optimising antimicrobial usage and controlling the proliferation of AMR. The Chinese Health Ministry formulated the Guiding Principles for Clinical Use of Antibiotics in 2004 and revised them in 2015. The Health Ministry established the Centre for Antibiotic Surveillance in 2005.8 The Expert Committee on Rational Drug Use of the National Health Commission (NHC) of China compiled national guidelines on antimicrobial therapy in 2012 and revised them in 2017 and 2023.9 The NHC of the People’s Republic of China organised a special campaign to rectify the clinical use of antibiotics across the country in 2013. This special campaign established the goals for antibiotic application in the hospital10: (a) the number of antibiotics in use was reduced to 50 kinds in each hospital; (b) the use of antibiotics in patients who undergo clean surgical procedures should not exceed 30%; (c) the antibiotic use in inpatients in general hospitals should not exceed 60%; (d) and the antibiotic use density should be controlled below 40 daily defined doses (DDDs) per 100 people per day.
Subsequently, the NHC issues documents every year, requiring the health commission of every province, based on the ‘Special Campaign in 2013 Nationwide,’ to adopt methods such as data monitoring, supervision and inspection, and undercover visits, to evaluate the clinical application of antibiotics in all levels and types of medical institutions and continuously improve the management work. A significant milestone was achieved in 2015 with the establishment of the National Clinical Improvement System (NCIS) by the NHC of the People’s Republic of China, creating a comprehensive surveillance network to monitor dynamic patterns of antibiotic utilisation.11 12 This network has demonstrated remarkable expansion, growing from an initial cohort of 2969 participating hospitals to over 11 691 institutions currently engaged in the surveillance system.13 14 The implementation of antibiotic management work is promoted through the efforts of the Provincial Pharmaceutical Quality Control Centre.
This study leverages data from NCIS to analyse temporal trends in antibiotic consumption, compare variations in antibiotic use across hospitals with distinct characteristics and assess compliance with national guidelines, and also to identify strengths and weaknesses in antibiotic management practices within Shanxi Province and uncover disparities in implementing antimicrobial stewardship (AMS) programmes among hospitals of different tiers and geographic regions. Furthermore, this research serves as a model for other regions to evaluate the impact of national surveillance systems on antibiotic use patterns, contributing to global efforts to combat antimicrobial resistance. The findings from this study will provide critical insights for healthcare policymakers, hospital administrators and clinicians, enabling them to optimise infection treatment strategies while addressing the pressing need to mitigate antimicrobial resistance.
Methods
Study design
This study was a retrospective study from 2015 to 2021. In this study, we included hospitals that met the following criteria: Inclusive criteria: (1) hospitals that reported antibiotic use data to the NCIS in any 1 year from 2015 to 2021 in Shanxi Province. Exclusive criteria: (1) hospitals without information on four indicators of antibiotic use for any 1 year, (2) hospitals with absurd and censored data and (3) hospitals that became non-functional.
This study didn’t require ethical approval since it involved the analysis of data collected by a regulatory organisation.
Patients and public involvement
There was no direct public or patient involvement in the design and implementation of this study.
Data collection and definition
Data collection
The data of antimicrobial use patterns are based on the actual consumption of antimicrobials used by hospitalised patients, which included: (1) the proportion of inpatients prescribed antibiotics, (2) the intensity of antibiotic treatment among inpatients, (3) the proportion of inpatients undergoing clean surgical procedures with prophylactic antibiotic prescriptions, (4) the proportion of inpatients using special-grade antibiotics. These data were obtained from China’s NCIS. Additionally, the following information was collected from the Shanxi Provincial Pharmaceutical Quality Control Centre: (1) the type of hospitals (hospital levels, hospital locations, hospital ownership categories and whether it is a quality control sentinel hospital), (2) the management of antibiotic use in the hospital (presence or absence of an antimicrobial stewardship (AMS) programme and a prescription automatic screening system (PASS)) and (3) the use of special-grade antibiotics. We conducted data cleaning on the antimicrobial use patterns, excluding data that did not make logical sense. For example, we excluded data where the proportion of inpatients prescribed antibiotics or the proportion of inpatients undergoing clean surgical procedures with prophylactic antibiotic prescriptions exceeded 100%.
Definition
The proportion of inpatients with antibiotic prescriptions (%): the proportion of inpatients who used antibiotics to the total inpatients in the medical institution during the same period. The proportion of inpatients who used antibiotics=the number of inpatients who used antibiotics / the total number of inpatients in the medical institution for the same period ×100%. The number of inpatients who used antibiotics and the total number of inpatients were calculated based on the number of discharged patients.
The intensity of antibiotic treatment among inpatients: the amount of antibiotic consumed by 100-bed inpatients per day=the amount of antibiotic used by inpatients (cumulative DDD number)/the number of bed days of inpatients for the same period ×100. Bed days of inpatients=average hospitalisation days×total number of discharged patients in the same period.
The proportion of inpatients with special-grade antibiotic use (%): special-grade antibiotic use was defined according to Guidance for Clinical Application of Antibiotics (2015 Edition). The proportion of inpatients with special-grade antibiotic use accounted for the total antibiotic use in inpatients for the same period. The proportion of special-grade antibiotic use in inpatients=the amount of special-grade antibiotic used in inpatients (cumulative DDD number)/amount of total antibiotic use in inpatients for the same period (cumulative DDD number) × 100%.
The proportion of inpatients undergoing clean surgical procedures with prophylactic antibiotic prescriptions (%): The proportion of the patients who used prophylactic antibiotics for clean surgical procedures accounted for the total number of patients with clean surgical procedures for the same period. The proportion of inpatients undergoing clean surgical procedures with prophylactic antibiotic prescriptions (%) = the number of inpatients who used prophylactic antibiotics for clean surgical procedures/the total number of inpatients with clean surgical procedures in the same period ×100%.
To reduce the overuse of antibiotics in the hospital, the management of the four antibiotic indicators relies on setting targets (table 1).
Targets of the antibiotic indicators
Special-grade antibiotics are defined as those that meet any of the following criteria: (1) they have obvious or serious adverse reactions and should not be used casually; (2) they have strong antibacterial effects and broad antibacterial spectra, and their frequent or excessive use can lead to rapid development of resistance in pathogenic bacteria; (3) they have limited clinical data on efficacy and safety and are not superior to currently available drugs; (4) they are newly launched drugs that require further verification regarding indications, efficacy or safety, and are expensive. This classification ensures that the use of these antibiotics is strictly regulated to optimise patient outcomes and minimise potential risks. The health commission of each province, taking into account local medical needs and antimicrobial management policies, will publish a list of special-grade antibiotics specifically tailored for hospitals within its jurisdiction for their reference.
Sentinel hospitals were identified by the NHC for the hospital’s data quality recognition. The hospital stewardship programme team mostly included infectious disease specialists, infectious disease consultants, medical directors, pharmacy directors, lab directors, quality control directors, hospital infection control directors, clinical pharmacists, microbiology lab technicians, public relations staff and information technology directors.
To derive a comparable metric of antibiotic use across time, a compound annual growth rate (CAGR) for antibiotic use was calculated as follows.

where CX was the total antibiotic use by inpatients in year X, CY was the total antibiotic use by inpatients in year Y and n was the number of years.
Statistical analysis
The statistical analysis was performed using SPSS Statistics version 21.0 (IBM, Armonk, NY, USA). Continuous data with a normal distribution were presented as means±SD and analysed using Student’s t-test and ANOVA; otherwise, they were presented as medians (IQR, IQR) and analysed using the Mann–Whitney U and Kruskal–Wallis H test. Categorical data were described as n (%) and analysed using the χ2 test or Fisher’s exact test. The scatter plot was drawn. Line graphs were drawn to show the change over the years. A two-sided p value <0.05 was considered statistically significant. We used a multivariable logistic regression model to examine the relationship between hospitals' characteristics and the compliance rate of various antibiotic indicators.
Results
Current status and trend of antibiotic-related indicators in Shanxi province
NCIS began to monitor antibiotic-related indicators in 2015, encouraging participating hospitals to complete data reporting on time, but it is not mandatory. If a hospital cannot accurately obtain monitoring data, it may not report relevant indicators. NCIS initially monitored only one antibiotic-related index, that is, the proportion of inpatients with antibiotic prescriptions. The proportion of inpatients with special-grade antibiotic use (%) was monitored in 2016. In 2017, the intensity of antibiotic treatment among inpatients was included. The proportion of inpatients undergoing clean surgical procedures with prophylactic antibiotic prescriptions (%) was included in 2019. At present, there are four monitoring indicators related to antibiotic drugs. A total of 221 hospitals reported data on antibiotics over the 7 years.
The number of hospitals that reported the proportion of inpatients undergoing clean surgical procedures with prophylactic antibiotic prescriptions increased from 176 in 2019 to 190 in 2021, and the proportion of inpatients undergoing clean surgical procedures with prophylactic antibiotic prescriptions decreased continuously from 45.08% to 40.0% between 2019 and 2021, with a CAGR of −5.80 (p=0.103). The number of hospitals reporting the antibiotic use density in inpatients increased from 147 in 2017 to 199 in 2021, and the antibiotic use density in inpatients was 42.00 and 39.70 DDD in 2017 and 2021, respectively, with a CAGR of −1.40 (p=0.015). The number of hospitals reporting the number of inpatients who used antibiotics increased from 119 in 2015 to 203 in 2021, and the proportion of inpatients who used antibiotics decreased from 51.42% to 47.14% between 2015 and 2021, with a CAGR of −1.44 (p<0.001). The number of hospitals reporting special-grade antibiotic use increased from 144 in 2016 to 199 in 2021, and the proportion of special-grade antibiotic use decreased from 0.74% to 0.49% between 2016 and 2021, with a CAGR of −2.56 (p=0.998) (table 2, online supplemental figures 1 and 2). Changes across different types of antibiotic are shown in online supplemental figure 3. The consumption of antibiotics according to the Anatomical Therapeutic Chemical (ATC) methodology in DDDs per hospital from 2015 to 2021 is shown in online supplemental table 1 .
Supplemental material
The CAGR of antibiotic use in Shanxi Province from 2015 to 2021
Decomposition of hospital characteristics-related antibiotic indicators
The median and interquartile intervals of the four indicators reported by all hospitals from 2015 to 2021 were calculated according to the different characteristics of the hospitals, and a statistical analysis was conducted. The overall proportion of patients undergoing clean surgical procedures with prophylactic antibiotics was 41.94% [28.13, 61.93], the intensity of antibiotic treatment among inpatients was 40.00 [34.23, 49.93] and the proportion of inpatients with antibiotics was 47.60% [40.98, 56.23]. The proportion of inpatients with special-grade antibiotics accounted for 0.39% [0.00, 1.49].
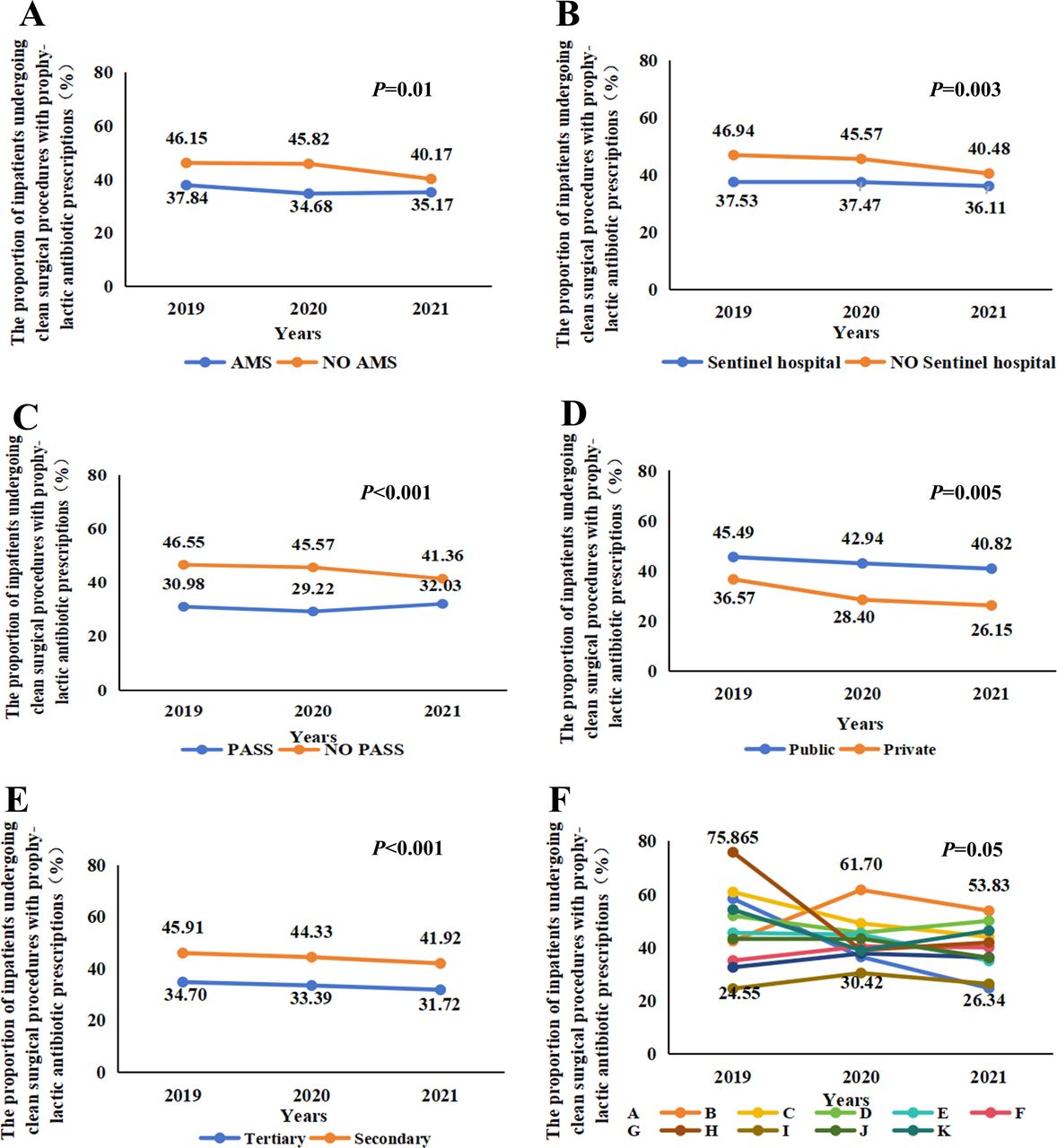
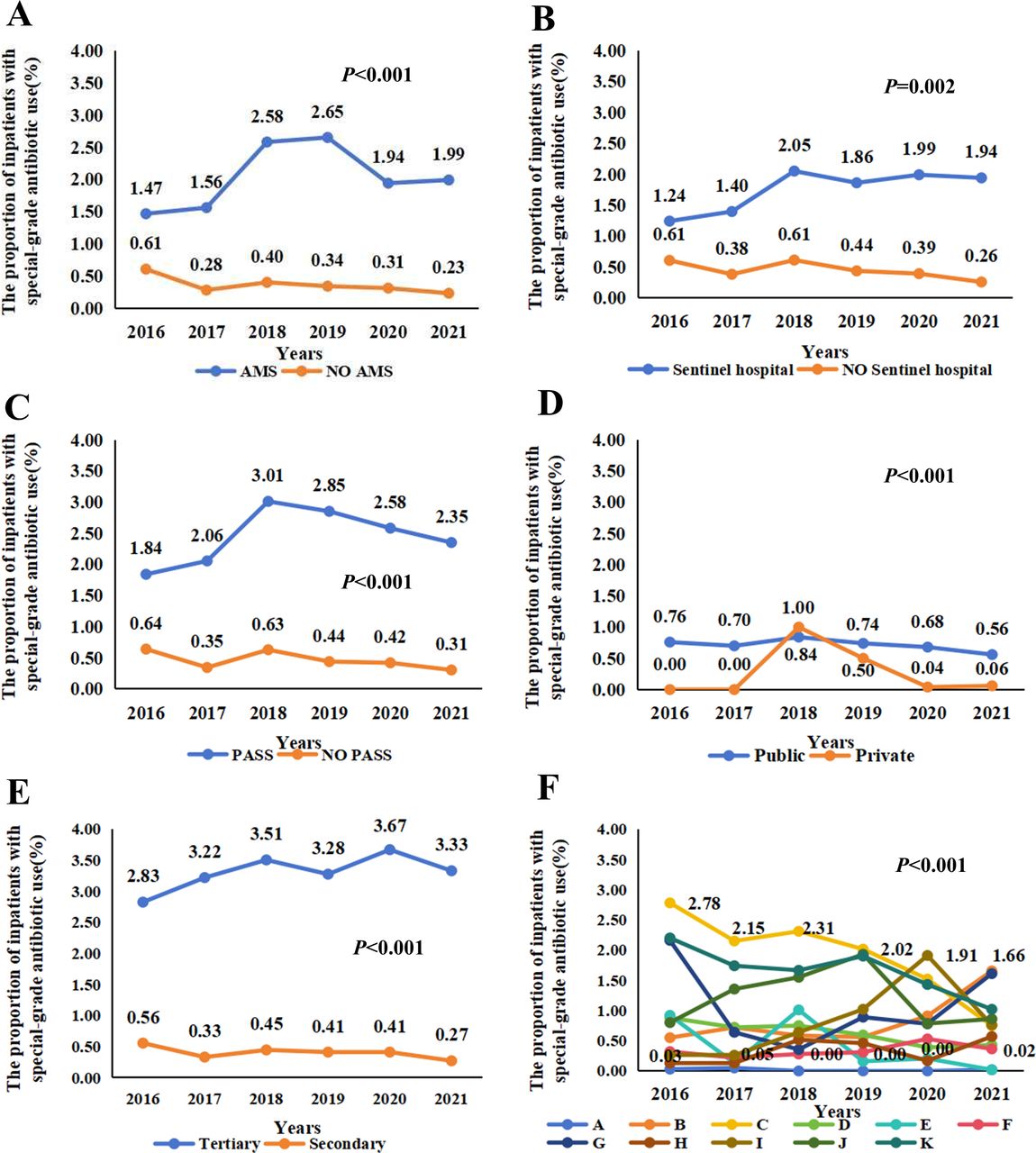
The values of variables relevant to antibiotic use were reported based on the characteristics of the hospitals, including hospital locations in the Shanxi province. The proportion of patients undergoing clean surgical procedures with prophylactic antibiotics was significantly higher in public hospitals, secondary hospitals, non-sentinel hospitals, hospitals without PASS and hospitals without AMS. The proportion of inpatients with antibiotic prescriptions and the intensity of antibiotic treatment among inpatients were significantly higher in public hospitals, secondary hospitals, non-sentinel hospitals and hospitals without PASS. The proportion of inpatients with special-grade antibiotic use was significantly higher in public hospitals, tertiary hospitals, sentinel hospitals, hospitals with PASS and hospitals with AMS. The differences were significant in these indicators in different cities (all p<0.05) (online supplemental table 2). We respectively drew the line charts of the changes of the four indicators in different types of hospitals over time, and the results showed that the differences of the indicators in the groups based on the city where the hospitals were located were greater than those in the other groups, as shown in figures 1–4.

The proportion of inpatients undergoing clean surgical procedures with prophylactic antibiotic prescriptions (%) (A) by with or without AMS; (B) by whether it is sentinel or not; (C) by with or without PASS; (D) by hospital ownership; (E) by hospital grade; (F) by the cities where hospital located. A–E: Cities where hospital located; A=Datong; B=Jincheng; C=Xinzhou; D=Taiyuan; E=Linfen; F=Yuncheng; G=Changzhi; H=Luliang; I=Yangquan; J=Jinzhong; K=Shuozhou. AMS, antimicrobial stewardship; PASS, prescription automatic screening system.

The intensity of antibiotic treatment among inpatients (A) by with or without AMS; (B) by whether it is sentinel or not; (C) by with or without PASS; (D) by hospital ownership; (E) by hospital's grade; (F) by the cities where the hospital is located. A–E: Cities where hospital located; A=Datong; B=Jincheng; C=Xinzhou; D=Taiyuan; E=Linfen; F=Yuncheng; G=Changzhi; H=Luliang; I=Yangquan; J=Jinzhong; K=Shuozhou. AMS, antimicrobial stewardship; PASS, prescription automatic screening system.

The proportion of inpatients with antibiotic prescriptions. (A) by with or without AMS; (B) by whether it is sentinel or not; (C) by with or without PASS; (D) by hospital ownership; (E) by hospital's grade; (F) by the cities where hospital located. A~E: Cities where hospital located; A=Datong; B=Jincheng; C=Xinzhou; D=Taiyuan; E=Linfen; F=Yuncheng; G=Changzhi; H=Luliang; I=Yangquan; J=Jinzhong; K=Shuozhou. AMS, antimicrobial stewardship; PASS, prescription automatic screening system.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The proportion of inpatients with special-grade antibiotics use. (A) by with or without AMS; (B) by whether it is sentinel or not; (C) by with or without PASS; (D) by hospital ownership; (E) by hospital's grade; (F) by the cities where hospital located. A~E: Cities where hospital located; A=Datong; B=Jincheng; C=Xinzhou; D=Taiyuan; E=Linfen; F=Yuncheng; G=Changzhi; H=Luliang; I=Yangquan; J=Jinzhong; K=Shuozhou. AMS, antimicrobial stewardship; PASS, prescription automatic screening system.
Multivariate logistic regression analysis between the compliance rate of various antibiotic indicators and the characteristics of different hospitals
Multivariable logistic regression analysis showed that public hospitals (OR=6.545; 95% CI: 3.177 to 13.485; p<0.05), hospitals with PASS (OR=0.409; 95% CI: 0.216 to 0.774; p<0.05), and hospitals with AMS (OR=0.537; 95% CI: 0.290 to 0.994; p<0.05), City A (OR=0.231; 95% CI: 0.059 to 0.908; p<0.05), City G (OR=0.247, 95% CI: 0.066 to 0.927; p<0.05) and City I (OR=0.120, 95% CI: 0.027 to 0.527, p<0.05) were independently significantly associated with the compliance rate of the proportion of patients undergoing clean surgical procedures receive prophylactic antibiotic prescriptions. The hospitals with PASS (OR=0.422; 95% CI: 0.291 to 0.611; p<0.05), City A (OR=0.268; 95% CI: 0.118 to 0.607; p<0.05), City D (OR=0.352; 95% CI: 0.169 to 0.733; p<0.05), City E (OR=0.296; 95% CI: 0.136 to 0.646; p<0.05) and City I (OR=0.297; 95% CI: 0.124 to 0.714; p<0.05) were independently significantly associated with the compliance rate of the antibiotic use density in inpatients. The tertiary hospitals (OR=0.396; 95% CI: 0.201 to 0.780; p<0.05) and City C (OR=6.522; 95% CI: 2.638 to 16.125; p<0.05) were independently significantly associated with the compliance rate of the proportion of inpatients who used antibiotics. The hospitals with AMS (OR=2.234; 95% CI: 1.088 to 4.58; p<0.05) and City D (OR=0.179; 95% CI: 0.047 to 0.679; p<0.05) were independently significantly associated with the compliance rate of percentage of special-grade antibiotic use (online supplemental table 3).
Discussion
To effectively tackle the public health challenges posed by AMR, it is crucial to strengthen AMS programmes.15 16All countries, including China, must act to reduce antibiotic use and prevent AMR.17 18 Monitoring and analysis of antimicrobial-related indicators are of great significance for assessing the effectiveness and deficiencies of antimicrobial stewardship. This research reviews and examines the utilisation of antibiotic medications in 221 hospitals across Shanxi Province over the past 7 years, while also determining the CAGR for four associated metrics. It comprehensively evaluated the use of antibiotics in each hospital within our province and assessed whether the enhancements in antibacterial drug management implemented by provinces following the conclusion of the national 3 year (2011–2013) antibacterial drug rectification initiative are sustainable. During the study period, the number of hospitals reporting data relevant to antibiotic use to NCIS has been increasing. This can be attributed to two main factors: China’s expansion of the monitoring network to include more hospitals and the enhancement of informatisation levels across various hospitals.19 This also indicates that the supervision of the provincial quality control centre is effective because it is the provincial quality control centre that has promoted the data reporting of the NCIS since 2015. This aligns with the suggestion from the China Centre for Health Development at Peking University, which suggested the establishment of an effective integrated surveillance network to monitor the use of antibiotics and invited policymakers to enforce the rational use of antibiotics.20 However, the number of hospitals reporting complete statistics relevant to antibiotic use must be immensely increased since AMR is still a growing global threat.
On the CAGR of antibiotic analysis from this study, the proportion of inpatients receiving antibiotics, the antibiotic use density in inpatients, the proportion of patients using prophylactic antibiotics for clean surgical procedures and the proportion of special-grade antibiotics used by inpatients declined in recent years, but the decline was statistically significant only for the proportion of inpatients receiving antibiotics and the antibiotic use density in inpatients. Nevertheless, these trends are interesting since they suggest a more rational and appropriate use of antibiotics. Still, clean surgical procedures are considered clean incisions21 and should not require antibiotics, except in special circumstances and in selected patients, which is possibly why the difference was not statistically significant. A similar line of thought can be applied to special-grade antibiotics, and the room for improvement is limited. Such drugs are already used in specific patients under specific circumstances. The same study saw huge differences in the prophylactic antibiotic use density in 2010, 2015 and 2020. Still, in the present study, the prophylactic antibiotic use density was declining in 2019, 2020 and 2021, although the differences were not statistically significant.
We found that in Shanxi, 47.6% of inpatients used antibiotics, 41.94% of patients used prophylactic antibiotics undergoing clean surgical procedures, 0.49% of antibiotics used by inpatients were of special grade, and the antibiotics use density was 40 DDDs. In a previous study, 22%–76% of inpatients used at least one antibiotic drug during their hospital stay,22 agreeing with the percentage obtained in the current study. Wu et al23 also found a large variation in the prophylactic use of antibiotics for clean surgical procedures among various hospitals in Shanxi province, which was similar to the results of our study. It may have been related to the differences in the awareness of surgeons on the rational use of antibiotics during the perioperative period.
To optimise antibiotic use, the United States Centres for Disease Control and Prevention (CDC) encourages all hospitals in the United States to implement hospital-based ASP with the outlined core elements.24 AMS management was strengthened and fully promoted in China in 2017. Since 2017, hospitals in Shanxi Province have successively carried out AMS management. AMS work is carried out under the guidance of Shanxi Provincial Pharmaceutical Quality Control Centre to prevent the escalation of AMR and related untoward consequences. AMS workgroup investigated antibiotic use using a model and shared information on the right drug, right dose, right duration, right route and de-escalation concerning antibiotics with healthcare professionals.25 26 In our study, hospitals with AMS programmes had lower antibiotic use density and a lower proportion of patients who used antibiotics and a lower proportion of antibiotic prescriptions who underwent clean surgical procedures with prophylaxis. The same study showed that the AMS programme significantly reduced antibiotic consumption and improved the judicious use of prescription antibiotics and clinical outcomes.22 27–29 A pragmatic cluster randomised control trial involving four European countries found that antibiotic prescribing in older adults was reduced after a multifaceted AMS implementation.30 The proportion of use of special-grade antibiotics, antibiotic use density and antibiotic cost was reduced significantly in some studies when a hospital had an AMS multidisciplinary team.28 31 32 The AMS has significant reductions in readmissions, mortality rates and antibiotic prescriptions postintervention.33 A significant reduction was observed in the consumption of carbapenems and echinocandins (11.15% and 25.62%, respectively) when clinical symptoms and microbial culture results were used in confirmatory diagnosis. Therefore, it is highly necessary for countries and hospitals to continue implementing or strengthening AMS action plans.
The comparative analysis revealed significant disparities in antimicrobial stewardship indicators among hospitals in different cities, likely attributable to varying levels of enthusiasm and rigour in implementing pharmaceutical quality control measures by management teams across regions. Established in 2009, the Shanxi Provincial Pharmaceutical Quality Control Centre prioritised guiding primary hospitals in the judicious use of antibacterial drugs as one of its key missions. This finding underscores that proactive oversight of antimicrobial use can have a profound and positive impact on optimising antibiotic management. These results not only provide robust evidence for the critical role of quality control in enhancing medical quality and ensuring patient safety but also offer clear guidance for future efforts. Specifically, by strengthening pharmaceutical quality control, we can continuously refine AMS practices, thereby reducing the misuse and irrational use of antibiotics, curbing bacterial resistance and safeguarding public health. It is important to note that Shanxi Province is geographically divided into 11 prefecture-level cities, each with a similar proportion of urban to rural hospitals. Therefore, the urban-to-rural hospital ratio is unlikely to be a contributing factor to the observed disparities in antimicrobial stewardship indicators.
The proportion of inpatients with antibiotic prescriptions, undergoing clean surgical procedures with prophylactic antibiotic and special-grade antibiotic use was significantly lower in private hospitals compared with public hospitals. These results suggest that it may be caused by the relatively serious condition of the patients admitted to these hospitals, and the number of difficult and infected cases was relatively high. These proportions (except special-grade antibiotic use) were significantly lower in tertiary hospitals and hospitals with monitoring systems. In addition, the proportions of all variables except special-grade antibiotic use showed a slight decreasing trend from 2019 to 2021, with or without statistical significance. It illustrates that hospitals with strict surveillance systems that promote the rational use of antibiotics seem efficient in using antibiotics when they are stringently needed. PASS is a core strategy within an AMS programme to reduce the irrational use of antibiotics in hospitals.34 It is widely adopted with the antibiotic management plan in hospitals in developed countries but not in developing countries. Digital interventions can improve antibiotic prescribing and monitoring antibiotic use in hospitals, but the degree of improvement by different types of digital interventions is yet to be elucidated.35 A previous study showed that the absence or minimal auditing of antibiotic prescriptions in the AMS programme in Tanzania weakened the programme.36 Digital interventions in the administration of antibiotics in hospitals improved the appropriate use of antibiotics in patients.35 A multifaceted computerised-AMS programme was effective and safe in reducing inappropriate antibiotic use in surgical settings.37
Some limitations were seen in this current study. The use of antibiotics must have been influenced by many factors, including the type of diseases treated, the severity of patients when admitted and the microbial examination performed, which were not analysed in this study. The NCIS data only provides aggregate antimicrobial-related indicators for hospitals, precluding the acquisition of specific metrics such as the average number of antibiotic types per prescription and the average DDD for each antibiotic category. The data reported by the hospitals may not have been 100% accurate. It may have influenced the outcome of this study. Not all the hospitals in the Shanxi province were reported to the system. Therefore, the outcome may not reflect the exact antibiotic used in the Shanxi province. We only obtained the information on whether the hospitals have AMS and PASS. The specific implementation degree and method of AMS and PASS in each hospital are uncertain. However, this study focused only on the standardised management of antibiotics as the first step, and our next work will focus on the rational use of antibiotics.
Conclusion
Based on the antibiotic data analysis of the NCIS and the Shanxi Provincial Pharmaceutical Quality Control Centre in the last 7 years, the proportion of inpatients using antibiotics and antibiotic use density showed a downward trend each year. The usage of antibiotics and compliance vary across hospitals with distinct characteristics. While the provincial efforts in controlling antibiotic use show some efficacy, further enhancement of surveillance programmes and targeted interventions at the hospital level are necessary to mitigate the escalation of AMR and ensure adequate antibiotic supply for emerging infectious diseases. In particular, it is necessary to supervise grass-root hospitals because compared with tertiary hospitals, secondary hospitals face more problems in antibiotic drug management. The effective management measures are to carry out a PASS and establish an AMS team.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
The data for the study were obtained from the National Clinical Improvement System (NCIS) and did not involve human participants or human material, so ethics approval and consent to participate were not applicable. Data were anonymised prior to being accessed by the study authors. According to the "Ethical Review Measures for Life Science and Medical Research involving Human Beings" issued by the Department of Science Education of the National Health Commission of the People's Republic of China in February 2023, it does not need to pass the approval of the ethics committee.
Footnotes
DY and YT contributed equally.
Contributors DY: conceived the research topic and led the literature search, data synthesis and writing of the manuscript; YT, SoW: data synthesis, edited the tables and figures. ShW: reviewed and edited the manuscript; JR, RZ, SY: were all involved in the different aspects of data collection. RH: served as scientific advisors; JD, ZR: critically reviewed the study proposal, reviewed and edited the manuscript. All authors were involved in data verification. ZR is the guarantor.
Funding The authors extend their appreciation to the Shanxi Pharmacy Administration & Quality Control Center. This study was funded by the Health Commission of Shanxi Province (2023XG032), (2023XG071), Natural Science Foundation of Shanxi Province (202303021222336).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.