Article Text

Abstract
Introduction Physical activity (PA) is crucial for older adults’ well-being and mitigating health risks. Encouraging active lifestyles requires a deeper understanding of the factors influencing PA, which conventional approaches often overlook by assuming stability in these determinants over time. However, individual-level determinants fluctuate over time in real-world settings. Digital phenotyping (DP), employing data from personal digital devices, enables continuous, real-time quantification of behaviour in natural settings. This approach offers ecological and dynamic assessments into factors shaping individual PA patterns within their real-world context. This paper presents a study protocol for the DP of PA behaviour among community-dwelling older adults aged 65 years and above.
Methods and analysis This 2-week multidimensional assessment combines supervised (self-reported questionnaires, clinical assessments) and unsupervised methods (continuous wearable monitoring and ecological momentary assessment (EMA)). Participants will wear a Garmin Vivosmart V.5 watch, capturing 24/7 data on PA intensity, step count and heart rate. EMA will deliver randomised prompts four times a day via the Smartphone Ecological Momentary Assessment3 application, collecting real-time self-reports on physical and mental health, motivation, efficacy and contextual factors. All measurements align with the Behaviour Change Wheel framework, assessing capability, opportunity and motivation. Machine learning will analyse data, employing unsupervised learning (eg, hierarchical clustering) to identify PA behaviour patterns and supervised learning (eg, recurrent neural networks) to predict behavioural influences. Temporal patterns in PA and EMA responses will be explored for intraday and interday variability, with follow-up durations optimised through random sliding window analysis, with statistical significance evaluated in RStudio at a threshold of 0.05.
Ethics and dissemination The study has been approved by the ethical committee of Hasselt University (B1152023000011). The findings will be presented at scientific conferences and published in a peer-reviewed journal.
Trial registration number NCT06094374.
- Aging
- Exercise
- Digital Technology
- Methods
- Behavior
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The study captures large-scale, temporally sensitive data on physical activity (PA) behaviours in real-world settings.
The hybrid data collection approach combines supervised (eg, self-reporting, clinical assessments, ecological momentary assessment (EMA)) and unsupervised (eg, continuous wearable monitoring) methods, providing a comprehensive view of PA.
Supervised data collection methods, including self-reporting and EMAs, may face challenges with participant compliance and higher attrition rates.
Unsupervised wearable monitoring and clinical assessments reduce participant burden but require robust backend infrastructure and technical support.
Digital literacy and access disparities among older adults may affect data representativeness.
Introduction
The global increase in life span is accompanied by an important rise in age-related impairments,1 often referred to as the non-communicable disease (NCD) pandemic.2 Regular physical activity (PA) has been shown to enhance overall well-being and significantly reduce the likelihood of experiencing adverse health outcomes, in particular chronic or NCDs (eg, coronary heart disease, stroke, certain cancers, diabetes mellitus type 2, obesity, hypertension, osteoporosis, falls and mortality).3–5 PA is recognised as a key component of a healthy lifestyle.6 Although older adults (often categorised as those aged 65 years and above) are more susceptible to these NCDs and thus truly benefit from preventive measures, they rank among the least physically active age groups. They devote a significant portion of their daily routine to sedentary behaviours, which contrasts with the increased risk they face for developing such health conditions.7 8 Current evidence highlights the fact that a sedentary lifestyle correlates with the manifestation of up to 35 chronic conditions, thereby imposing a significant decline in the cumulative years of life and those lived in a state of high quality of life (QoL).9–13 In light of the ever-increasing awareness of the significance of PA and the adverse outcomes associated with a sedentary way of life, it remains concerning that a substantial 58.2% of the global population of older adults is falling short of the recommended guideline of engaging in at least 30 min of moderate-to-vigorous PA per day for a minimum of 5 days a week.14 15
As the proportion of older adults continues to rise, understanding the factors contributing to healthy ageing becomes increasingly critical.16 Moreover, the knowledge of the barriers and facilitators of PA among older adults is fundamental to designing interventions to promote an active healthy lifestyle.17
In recent years, the emergence of digital health technologies has ushered in a new era of monitoring, analysis and intervention in the domain of PA.18
Mobile health technologies (eg, wearable, portable, connected sensors) present a unique opportunity to capture and quantify a rich array of data concerning individuals’ daily movements and exercise routines. This technological advancement allows for a comprehensive exploration of the intricacies of PA behaviour, unveiling patterns that were previously difficult to discern using traditional self-report methods.19 The rise of these mobile health technologies equipped with sensors that measure motion, motor skills and mobility for unsupervised, real-world scenarios is becoming increasingly prominent as essential adjunctive tools in the conventional clinical evaluations.20 These technologies offer a breakthrough by addressing the limitations inherent in routine clinical tests.21 The data collected in ecologically valid and individual-relevant environments have the capacity to capture diverse and unforeseen events, potentially overcoming the constraints of conventional assessment methods.22 Furthermore, the continuous nature of data collection facilitates the identification of subtle changes in individuals’ status, enhancing the precision and sensitivity of outcome information. In essence, these advancements in technology pave the way for a more nuanced understanding of individuals’ PA patterns and contribute to more accurate and insightful clinical assessments.23–26
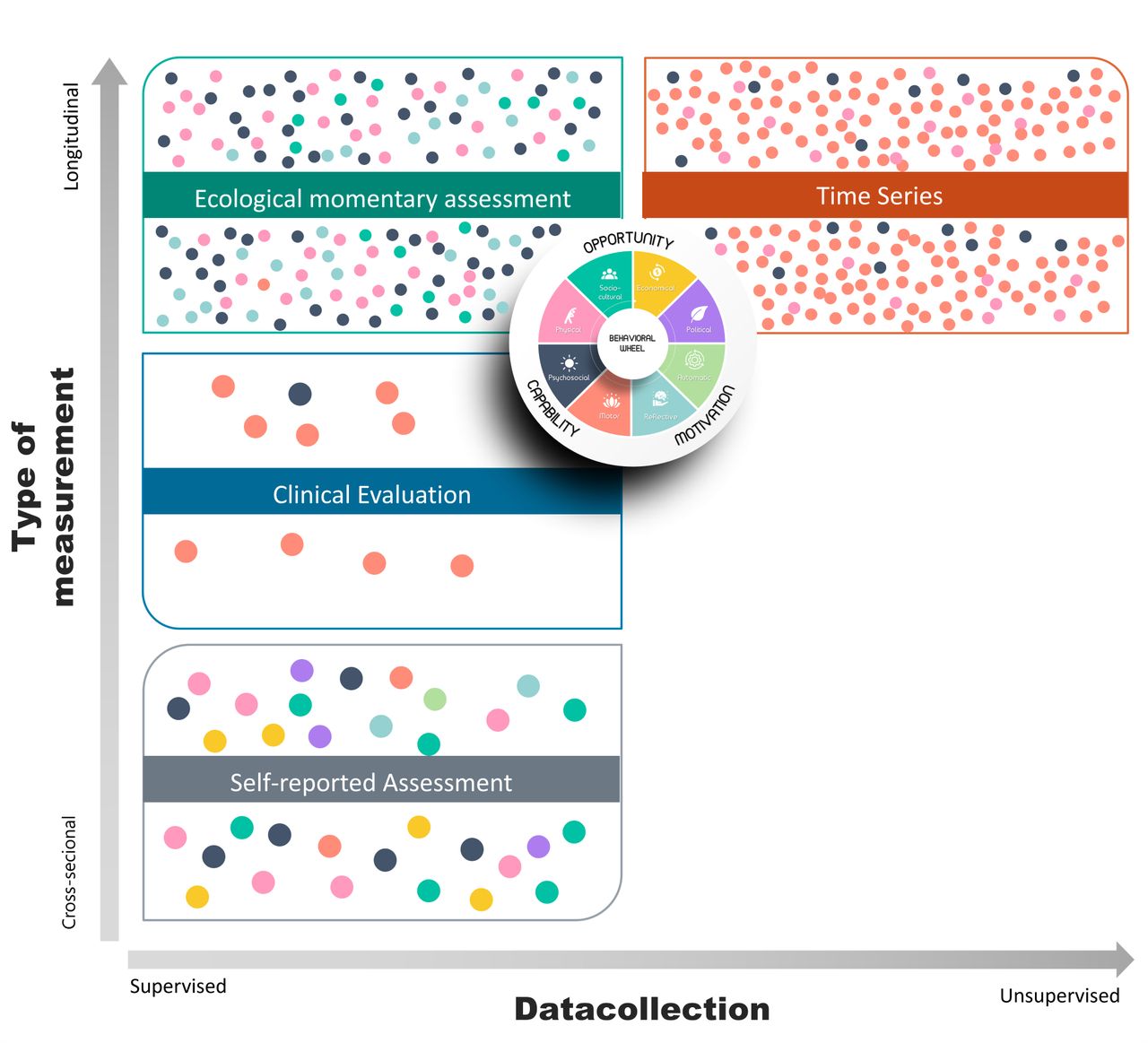
This evolution has given rise to a concept known as digital phenotyping (DP), which refers to the utilisation of data sourced from personal digital devices to swiftly quantify the individual human phenotype.27 DP achieves real-time, continuous quantification in an unsupervised way of an individual within their natural environment through the automated aggregation of data. The aim of DP is to measure human behaviour patterns and functioning in both health and disease on a moment-to-moment basis.28 In addition, other approaches such as ecological momentary assessment (EMA) can be used. EMA is designed to repeatedly and intensively sample individuals’ behaviour, cognition, affect, context and other experiences in real time and ecologically.29 It is a method that enables capturing time-dependent variations of behaviour and its determinants.30 The combination of traditional data collection methods, such as self-reported assessment and clinical assessment—latter named as supervised assessment with more dynamic and time-sensitive methods, such as time series assessment—referred to as unsupervised assessment—and EMA offers the promise to map and identify the crucial factors that influence PA behaviour. This information can then be used as the basis for the optimisation of, in this specific case, promoting PA in a precise, predictive and personalised manner.
The aim of this paper is to develop and present a comprehensive and exhaustive methodology to dynamically capture and characterise PA behaviour of community-dwelling older adults. This novel approach combines different types of evaluation (ie, supervised and unsupervised) as well as different timeframes (ie, cross-sectional and continuous data collection) within a single protocol. This research project has three core objectives, which are to enhance our understanding of PA behaviour in older adults, refine DP methodologies and optimise the use of wearable technology in clinical trials.
Methods
Study status
Participant recruitment began in October 2023, with data collection initiated in March 2024. Data collection is still ongoing at the time of this report.
Study setting and design
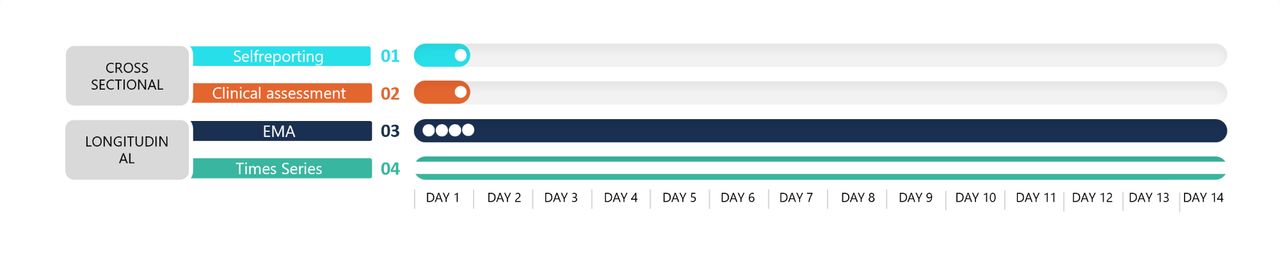
An observational study will be conducted to gather data on multiple levels using a hybrid approach combining supervised and unsupervised data collection methods. This integrated strategy will be complemented by four distinct measurement approaches, ensuring a comprehensive assessment of the research objectives, which are visualised in figures 1 and 2.

The spectrum of data collection explored for defining digital phenotypes in PA behaviour. EMA, ecological momentary assessment; PA, physical activity.

Meta view of the integrated data collection.
The complete methodology of data collection is presented in online supplemental table 1.
Supplemental material
Participants and public involvement
Participants and the public were not engaged in the design or development of this study protocol. However, direct participant involvement is a key component of the research process, which includes participation in structured interviews, completion of assessments and standardised questionnaires at scheduled study visits and contributing to continuous digital data collection over 2 weeks. Additionally, the protocol will be tested for feasibility in a pilot phase to ensure its practicality and participant compliance before the full study is implemented. This preliminary step allowed us to refine the methodology and address potential data collection and participant engagement challenges.
Participants
Participants include older adults aged 65 years and above with no severe illness introducing a loss of mobility or function or a reduction in cognitive functions preventing the proper understanding of instructions. Individuals with a remote history of coronary artery disease or diabetes will also be excluded to reduce potential confounding factors, as these conditions can influence PA patterns and introduce variability related to cardiovascular or metabolic limitations. They will be recruited via social media reach, newspaper advertisements and pitches at several senior citizen organisations, through the local community services. No financial compensation will be offered; however, participants will receive non-monetary incentives, such as detailed individualised feedback and advice on their physical health status and health-related behaviour. Additionally, participants will have the opportunity to try out a wearable activity tracker with personalised guidance from researchers, which has been identified as a key motivator during preliminary recruitment efforts. To be eligible for participation, individuals must meet the inclusion and exclusion criteria fully described in box 1.
Inclusion and exclusion criteria
Inclusion criteria
Participants are 65 years and above
Participants are competent to give informed consent
Participants are able to actively participate in the study
Participants are community dwelling (living independent at home or in a service apartment)
Without a severe illness
Dutch language proficiency as native speaker
Exclusion criteria
Current neurological disorder such as Parkinson’s disease, multiple sclerosis, cerebrovascular accident, etc
Current cardiovascular disorder such as stroke, acute myocardial infarction, coronary artery bypass grafting, percutaneous coronary intervention less than 5 years ago
Current respiratory disorder, such as chronic obstructive pulmonary disease, pneumonia, pulmonary fibrosis, asthma, etc
Current severe metabolic disorder, such as diabetes types 1 and 2, severe osteoporosis, etc
Current severe cognitive disorders, such as Alzheimer’s disease, vascular dementia, Lewy body dementia, frontotemporal dementia
Sample size
Due to the innovative and exploratory character of this study, involving the utilisation of emerging technologies previously unexplored for this specific purpose, formal sample size calculations were deemed unattainable. Because of the lack of accessible prior studies that could provide foundational information, a sample size calculation was impossible. Therefore, a convenient sample of 200 healthy older adults was opted for this trial.31
Supervised versus unsupervised data collection
Supervised data collection
Self-reported assessment
At the baseline assessment (T0), participants will be asked to complete a comprehensive series of standardised and validated questionnaires in Dutch, as presented in online supplemental table 2 (English translations of these questionnaires are also presented in online supplemental appendix 1).
Supplemental material
Supplemental material
Clinical assessment
Additionally, at baseline (T0), participants will undergo a thorough clinical assessment, consisting of balance testing, muscle strength evaluation, cardiovascular examination and cognitive analysis. The complete psychometric characteristics of the clinical assessments are summarised in online supplemental table 3.
Supplemental material
Ecological momentary assessment (EMA)
Participants will receive four random prompts daily (time random (TR)) over a 2-week period on their mobile phones via auditory signal. The Smartphone Ecological Momentary Assessment3 (SEMA3) application32 will be installed on the participant’s smartphone and will be used to trigger the EMA Questionnaire.
To ensure adequate spacing across the day, four timeframes, each of 2 hours, will be constructed between 8:00 and 20:00, in which one trigger will be randomly given. They will be instructed to halt their ongoing activities and promptly complete the EMA Questionnaire, which typically will take two to 3 min. In cases where participants are driving or engaged in activities incompatible with questionnaire completion, they are strictly advised to disregard the prompt. If a participant fails to complete the EMA Questionnaire following the initial prompt, the phone will emit a maximum of three reminder signals at 5 min intervals. After the third reminder, access to the EMA Questionnaire will be temporarily suspended until the subsequent scheduled questionnaire.
Unsupervised data collection
Time series data collection
Finally, participants will be invited to wear a monitoring device continuously for 2 weeks (24/7) to record their activity data (time continuous (TC)). The device will collect detailed, continuous data across several parameters, including PA metrics (eg, step count and activity intensity categorised as light, moderate or vigorous), physiological metrics (eg, heart rate, calorie expenditure and stress levels) and additional indicators (eg, floors climbed, sleep duration and quality, and the ‘body battery’ metric, which estimates overall energy levels based on activity and stress). Walking cadence will be used to classify PA intensity: moderate intensity is defined as activity exceeding three metabolic equivalents (METs), corresponding to a cadence of at least 100 steps per minute. In contrast, light intensity ranges between 1.6 and 2.9 METs. Movements below 20 steps per minute will be categorised as incidental and classified as sedentary behaviour. Data for all variables will be collected in 15 min intervals. The GARMIN Vivo smart V.5 was selected for its established accuracy, high user acceptance and ability to provide unprocessed data specifically for research purposes through the manufacturer’s research portal. A user-friendly, personalised manual was prepared for all participants, providing clear guidance on using the Garmin Vivosmart V.5, including detailed instructions to charge the device every 3 days to ensure continuous data collection. Additionally, participants will be provided with a diary to log the dates and times they will charge the device (online supplemental appendix 2). These features make it a robust and reliable tool for capturing multidimensional PA data in older adults.33–35
Supplemental material
Measurements
All measurements are based on the Behaviour Change Wheel (BCW),36 which finds its theoretical foundation in Michie’s COM-B framework (Capability, Opportunity and Motivation Model of Behaviour).37 It represents a comprehensive theoretical structure that dissects behaviour into three essential components (as illustrated in figure 3):
Opportunity pertains to the external conditions enabling or hindering the behaviour.
Capability refers to the individual’s psychological and physical ability to engage in the behaviour.
Motivation encompasses the internal processes driving the inclination to perform the behaviour.

Theoretical framework used to develop study protocol based on the Behaviour Change Wheel.
By adopting this framework, the study tends to embrace a multifaceted and dynamic approach for analysing and understanding the complex interplay of these elements that shape observed behaviours in PA. A summary of all included measurements on the different levels can be found in detail in online supplemental table 1. We are now going to discuss the three subcomponents of the BCW, which are elaborated in detail.
Opportunity
The opportunity of the BCW includes aspects of the physical, sociocultural, economic and political environments that can influence behaviour at the micro, meso or macro level.38 Influences can arise from concrete settings in which the behaviour occurs or from broader systems that influence behaviour indirectly. To gauge these components, self-reporting measurements and EMA will be employed.
Self-reported assessment
Self-reported information on age, gender, height, smoking status, marital status, level of education, living arrangement, urbanisation level, participation status, self-rated health level39 and pain level40 will be collected. Participants will also be asked to indicate their retirement status, level of income, living status and access to facilities in the community. Their QoL level will be evaluated using the WHO Quality of Life Brief Version.41 These items will be collected using the online survey tool Qualtrics.42
Ecological momentary assessment (EMA)
Participants will rate their self-rated health, five physical complaints (ie, muscle stiffness, pain, dizziness, shortness of breath and fatigue), contextual factors and QoL using a 7-point Likert scale.43 The sequence of questions in the questionnaire will vary, with questions presented in a random order.
Capabilities
Capabilities refer to an individual’s capacity to effectively perform a specific behaviour. It encompasses a range of skills and abilities required for the successful execution of that behaviour. The significance of capabilities lies in its pivotal role; when individuals lack the necessary skills for a particular behaviour, the likelihood of them adopting and sustaining behaviour change diminishes.
Capabilities can be deconstructed into two primary categories, which are psychosocial and physical capability. Psychosocial skills pertain to an individual’s cognitive and emotional aptitude to engage in a given behaviour. It encompasses a spectrum of factors, including knowledge, skills, memory, attention and self-regulation. Physical capability refers to the physical capacity to carry out a behaviour. It includes factors such as physical strength, mobility, cardiovascular capacity and balance.44 45
The measurement instruments included to map the respective psychosocial and motor skills are summarised in online supplemental tables 2 and 3. They will be evaluated across the four distinct levels of measurement, encompassing self-reporting, clinical assessment, EMA and time series analysis.
Self-reporting assessment
Self-reported information on driving status, mobility issues, depression,46 stress,47 cognitive functioning,48 subjective well-being,49 anxiety,50 PA,51 sleep pattern52 and emotional loneliness53 will be collected.
Clinical assessment
Psychological and motor skills will undergo comprehensive evaluation through clinical assessments administered by experienced therapists. These assessments will encompass cognitive functioning, cardiometabolic health, muscle strength and balance, providing a holistic understanding of an individual’s overall health.
a. Cognitive functions
The assessment of cognitive functioning will be conducted using the SWAY (SWAY Medical in Tulsa, Oklahoma, USA).54 The cognitive performance segment of the application encompasses three modules grounded in sensory and neuromotor principles. These modules aim to assess stimulus recognition, cognitive processing speed, neuromotor response, working memory and reaction time. The cognitive testing segment, focusing on reaction time, has undergone clinical evaluation and demonstrated reliability and validity, comparing favourably to the standard Computerized Test of Information Processing assessment. However, the capacity of SWAY to function consistently across various mobile devices and operating systems is yet to be validated.55–57 Therefore it will be used to collect all the data.
b. Physical functioning
Walking performance
Gait analysis will be performed using the Six Minute Walking Test (6MWT). The 6MWT serves as a robust tool for evaluating exercise capacity at levels reflective of typical efforts exerted by the elderly during daily activities, as established by Lipkin et al in 1986.58 Additionally, it proves invaluable for assessing the progression of functional exercise capacity in diverse clinical intervention studies.59–62 The test demonstrates high reliability among healthy elderly individuals (intraclass correlation=0.93).63–65
During this test, diverse data will be gathered using specialised instruments. Gait speed, proven to be a robust predictor of adverse health outcomes, remains significant irrespective of the presence of common medical conditions and risk factors for diseases.66–68 Many studies demonstrated a strong association with incident disability, cognitive decline and dementia, falls and related fractures, mortality, and healthcare utilisation (eg, hospitalisation and institutionalisation). Although tested in very different populations, different walking distances and studied outcomes, the prognostic value is very consistent.69
Gait analysis will be performed using Digitsole insoles (Nancy, France) to quantify various parameters during walking. PODOSmart insoles, equipped with wireless sensors, can seamlessly fit into any shoe, enabling the measurement of spatial, temporal and kinematic gait parameters. These intelligent insoles feature multiple sensors to detect and record foot movements, alongside a microprocessor that computes biomechanical data related to gait.70 Additionally, potential gait deviations can be discerned through inertial measurement units (IMUs). These IMUs capture crucial gait parameters such as speed, cadence and biomechanical angles of motion during walking, interfacing with dedicated software on a tablet. The software facilitates the generation of comprehensive data reports, encompassing kinematic variables specific to an individual’s walking patterns.59 Notably, the validity and reliability of Digitsole have been studied in samples of healthy individuals over brief walking periods.70 71
Muscle strength
Muscle strength will be assessed using the Kinvent2016 handheld dynamometer. The test protocol involves consecutively evaluating the strength of different muscle groups of the lower extremities: abductors (side lying), adductors (supine), extensors (prone) and flexors (sitting). Each muscle group will undergo three tests, and the final result will be based on the best value obtained from these tests, following the protocol established by Thorborg et al.72
Additionally, hand grip force will be measured using the K-Force Grip (Kinvent, Montpellier, France). This measurement serves to evaluate overall strength, enabling comparisons of muscle function across populations and tracking the progression of conditions such as sarcopenia, while also identifying potential deficits.73 74 The dynamometer has been designed for assessing and rehabilitating handgrip strength. It provides real-time biofeedback on a tablet or smartphone. A study conducted by Nikodelis et al75 comparing Jamar and K-Force Grip found no fixed or proportional bias. Both groups exhibited high correlation coefficients, with the lowest correlation observed between the two instruments (r=0.90, p<0.05), indicating strong reliability.
Balance
Postural balance is crucial for maintaining a specific posture in response to external disturbances. Imbalances stemming from malfunctions in the visual, vestibular or proprioceptive sensory systems can lead to issues such as falls, injuries and instability in joints. To identify and address these concerns, clinical tests are essential.76 77 In this study, postural balance will be assessed using the Kinvent PLATES V.3 (Kinvent, Montpellier, France). Participants will undergo the single leg balance (SLB) test under various conditions: (1) three repetitions for each leg with open eyes on the PLATES and (2) three repetitions for each leg with eyes closed on the PLATES. The SLB test involves maintaining a stationary position on one leg for 10 s, focusing on a 0.5 m away, with hands on hips and the non-load-bearing leg slightly bent at the hip and knee.78 79 To facilitate a comprehensive comparison between open and closed eyes conditions, a 10 s test duration was chosen, aligning with norms established for the closed eyes condition during unipodal balance exercises (norm=9.4 s).80 Additionally, a second test, the single leg landing, will be conducted with three repetitions for each leg on the PLATES. This dynamic unilateral balance exercise requires participants to descend from a step positioned 19 cm above the force platform with a bounce, ensuring both feet are suspended before landing. Subsequently, participants must stabilise on one leg for 15 s, with hands on hips and their gaze fixed at a 0.5 m away.81 82
Functional capability
The Short Physical Performance Battery has emerged as one of the most promising tools to evaluate functional capability and provide a measure of the biological age of an older individual.83 It is an objective tool for measuring the lower extremity physical performance status. Three domains, which include balance, self-selected gait speed and lower limb strength, are assessed by a three-stage balance test (feet side-by-side, semitandem and tandem positions), a 3 or 4 m gait speed test (time spent to walk the course), and a repetitive chair stand test (five times chair sit-to-stand test), respectively. A 0–12-point scale is used to score the sum of the three assessments, with higher point values corresponding with greater levels of physical function and lower disability, whereas lower point values correspond with lower levels of physical function and higher disability, respectively.83 The timed results of each subtest are rescaled according to predefined cut points for obtaining a score ranging from 0 (worst performance) to 12 (best performance).84
Ecological momentary assessment
Participants will rate their stress, PA and sleep using a 7-point Likert scale. The sequence of questions in the questionnaire will vary, with questions presented in a random order.43
Time series data assessment
Throughout the 2-week trial, a continuous monitoring process (24/7) using Garmin Vivosmart V.5 activity tracker will collect various parameters, including stress levels, PA, step count, calorie expenditure, heart rate, the number of floors climbed, moderate-to-vigorous activity, cardiometabolic outcomes, body battery and sleep patterns.35 85
The continuous data contain data derived from a GARMIN wearable, capturing participants’ day-to-day activities through seamless, non-intrusive sensing.
Motivation
Clinical assessment
Motivators are the factors that guide or motivate a person’s behaviour from reflective or rational considerations or from automatic processes or factors such as needs, emotions and habits. Within the realm of motivation, two fundamental drives can be identified: automatic and reflective motivation. The first one is characterised by the emotional and instinctual triggers that shape our actions. This particular facet is gauged via self-reporting assessment by employing the Exercise Motivation Inventory-2.86
Another aspect is the reflective motivation, rooted in the cognitive and thoughtful aspects that steer behaviour transformation. This latter dimension encompasses factors such as beliefs, intentions and goal setting, all of which play pivotal roles in the journey towards change. To assess this aspect, both the Exercise Identity Scale87 and the Exercise Self-Efficacy Scale88 are being used.
The assessments will be administered at different significant time points, as depicted in figure 4.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Study outline. EMA, ecological momentary assessment.
Ecological momentary assessment (EMA)
Participants will rate their motivation level and intention to be physically active using a 7-point Likert scale.43 The sequence of questions in the questionnaire will vary, with questions presented in random order.
Statistical analysis
The assessment of data normality will be conducted using graphical techniques, including Q–Q plots, histograms and boxplots. Continuous data will be reported using the mean and SD or the median and IQR, depending on the distribution. Categorical data will be presented as frequencies and percentages.
To answer the different research questions, different machine learning methods will be used and tested. We will first evaluate unsupervised learning with the use of hierarchical clustering, a well-established method in multivariate statistical analysis.89 The purpose of this approach is to reveal hidden patterns in how participants classify themselves, based on their self-reported adherence to the WHO’s recommendation of PA, and to identify participants with increased risk of falls. If the current strategy proves unsuccessful, alternative methods involving a random decision forest or gradient boosting algorithms will be tested.90 Ensemble learning methods, such as gradient boosting techniques, involve the integration of multiple weak predictors to form a more accurate one. This approach iteratively introduces decision trees to the model, with each new tree aiming to rectify the errors of its predecessors. Gradient boosting algorithms demonstrate notable effectiveness when dealing with intricate data, often achieving high accuracy across a diverse range of problems compared with stepwise linear regression.91 Nevertheless, the preference is to maintain a straightforward model, prioritising simplicity to facilitate clinical interpretation.
We will then evaluate supervised learning using (recurrent) neural network (RNN).92 Different models will be trained according to the research questions. The objective of this procedure is to identify distinctive variables that distinguish individuals who have experienced falls from those who have not and those who adhere to the WHO’s PA recommendations. The added value of RNN, in our context, is the ability to process time series input. Such kind of network possesses the capability to retain an internal memory of past inputs, leveraging it for predicting future inputs. RNNs excel in modelling intricate temporal interactions, demonstrating superior flexibility and robustness when handling sequential data.93 In comparison to stepwise regression, RNNs are adept at capturing complex temporal relationships and exhibit lower susceptibility to overfitting.
The significance threshold will be set at 0.05. Statistical analyses will be performed in R using RStudio (V.3.6.3).
Ethics and dissemination
This study was approved by the ethical committee of Hasselt University (B1152023000011) and registered at ClinicalTrials.gov (NCT06094374) on 17 October 2023. Participants will provide informed consent before any research activities, with a preview of the consent form available in online supplemental appendix 3. All collected data will remain confidential, with only de-identified data analysed.
Supplemental material
Data collection includes self-report questionnaires, clinical assessments and EMA tools, selected based on the BCW framework. A data integration platform will consolidate all collected data, applying pseudonymisation to protect participant privacy while ensuring compliance with data protection regulations. Standardised coding schemes will maintain consistency, and regular quality checks will identify discrepancies.
Data storage will follow legal requirements, with long-term curation strategies enabling future reuse. On study completion, raw data will be made available on reasonable request to support collaborative and reproducible research. The preregistration on ClinicalTrials.gov (NCT06094374) ensures transparency and accountability.
Findings will be disseminated through peer-reviewed publications, conference presentations and targeted knowledge translation activities for healthcare professionals, policymakers and participants.
Discussion
This research presents a novel protocol that enhances DP by employing a hybrid measuring methodology. The main aim of the protocol is to acquire a thorough comprehension of PA behaviour in the older adult population, ascertain the significant factors that influence this behaviour and develop DPs associated with PA behaviour. The innovative approach integrates both supervised and unsupervised data collection methods, combining self-reports, clinical assessments, EMA and continuous data from wearable devices. This protocol aims to capture the complex and dynamic nature of PA behaviour in older adults, with future research focused on validating its effectiveness.
Clinical relevance
Previous works demonstrate that data collected within an ecologically valid and individually relevant environment can surpass the limitations inherent in conventional clinical assessments or one-time self-reporting.19 21 94 The distinct advantage of unsupervised daily PA monitoring lies in its ability to detect more nuanced changes over time. Ultimately, through the utilisation of this methodology, our goal is to identify distinct DPs, enabling the tailoring of interventions to meet the unique needs of older adults. This personalised approach holds the potential to yield more effective and engaging interventions, finally enhancing their overall well-being and health.95 This initiative directly addresses a substantial public health concern.
Challenges
However, some potential pitfalls and challenges warrant careful consideration in this context. Technological adoption rates among community-dwelling older adults vary widely, and some individuals may lack the necessary technological literacy or access to digital devices.96 97 This may introduce selection bias into the study, and researchers must be mindful of the sample’s representativeness. Additionally, usability concerns surrounding digital tools such as wearables must be addressed. Older adults may struggle with complex interfaces or physical limitations that hinder their interaction with these devices.98
We acknowledge that DP traditionally encompasses a broader range of behavioural and physiological metrics beyond PA.99 Our decision to focus solely on PA as a component of the digital phenotype was intentional, given the novelty of this concept in PA research and the need for a practical, feasible starting point. Incorporating additional sensors, such as smartphone health kits, could enhance the scope of DP; nonetheless, this would have increased the study’s complexity and resource demands.100 This study serves as a foundational step, focusing on developing and validating methods specific to PA monitoring in older adults. Future research will build on this foundation by integrating broader data streams to capture a more holistic digital phenotype.
Furthermore, it is imperative to acknowledge that the use of mobile technology and EMA can elicit modifications in behaviour, the Hawthorne effect, even in the absence of explicit feedback.101 Therefore, it is imperative to do research that investigates the circumstances in which user performance in unsupervised environments corresponds to that in supervised environments. To address this potential confounding effect, the EMA prompts have been carefully designed to minimise disruption by limiting their frequency to four times a day and integrating them seamlessly into participants’ routines, based on findings from previous research.102 103 Furthermore, it is necessary to investigate if the observed alterations in behaviour directly impact levels of PA.21 104
Additionally, only about 5% of health and performance technologies have been proven effective through rigorous, independent validation. Consequently, the value of these technologies remains a topic open to debate.105 106
Ethical considerations are paramount in the context of digital health interventions and data collection in older adults.107 Issues such as data privacy and security must be thoroughly examined to safeguard the rights and well-being of the study’s participants. Moreover, the success of the research heavily relies on translating complex data streams from wearable devices into actionable insights. The challenge lies in making this information understandable and beneficial for individuals and healthcare practitioners. Effective data interpretation and communication are critical components.108
The representativeness of the sample is another aspect that will require attention. The demographics and health status of the older adults participating should be carefully considered. A non-representative sample could limit the generalisability of the findings. Therefore, efforts should ensure a diverse and inclusive sample, capturing a broader spectrum of experiences and needs. Participants with a remote history of coronary artery disease and those with diabetes will be excluded to minimise potential confounding factors related to their conditions. These individuals often exhibit distinct PA patterns or limitations due to cardiovascular or metabolic conditions, which could introduce variability.109 110 Hence, this initial study focuses on ensuring that the methods are robust and feasible, as this approach has not been previously applied.100 111 Starting with a healthy older adult population allows for validation and refinement of the methodology before extending it to individuals with more complex health profiles. However, to achieve a more representative understanding of the population, it is essential to include individuals with coronary artery disease and diabetes in future studies.112 These conditions are prevalent among older adults, and their inclusion would provide a more comprehensive picture of PA and improve the applicability of findings to broader populations.113–116
To ensure a representative sample, diverse recruitment methods will be employed, tapping into various channels and establishing partnerships with relevant organisations. Stratification based on key demographics, including age, gender, ethnicity and socioeconomic status, will be implemented, focusing on oversampling underrepresented groups. Additionally, continuous monitoring of the demographic composition during recruitment will guide necessary adjustments based on feedback and observed trends. Although no financial compensation will be provided, participants will benefit from non-monetary incentives, such as receiving detailed, personalised feedback on their physical health and activity patterns. They will also have the opportunity to explore the use of a wearable activity tracker with tailored support from researchers. These incentives are emphasised in recruitment materials to engage participants and highlight the practical and educational benefits of their involvement.117
Longitudinal data collection, while beneficial, can be resource intensive and may pose difficulties in participant retention and compliance over an extended period.118 119 Strategies to minimise attrition and maximise engagement are necessary to ensure quality and completeness of the data. An extensive training on using the wearable and the SEMA³ application is recommended to obtain a high response rate. Additionally, regular check-ins and personalised feedback will be implemented to maintain participants’ motivation and compliance.120
At last, the use of machine learning and RNNs, while offering powerful tools for data analysis, can be complex and require expertise. Ensuring that the chosen algorithms are appropriate and well tuned is crucial for the study’s success. The algorithms used for defining the DPs need to undergo thorough validation. To enhance the effectiveness of unsupervised measures, there is a need for standardised reporting of parameters, such as establishing a core dataset across studies. This reporting should also encompass metadata, which includes data that accompanies and describes the primary data. Standardising the duration of unsupervised assessments and providing detailed information are additional requirements.21 121 122
Despite these challenges, the insights gained could inform targeted interventions and public health policies, addressing the unique challenges of an ageing global population. Integrating findings into clinical practices may lead to personalised strategies for promoting PA among older adults, positively impacting health outcomes and reducing healthcare costs. Ultimately, the research contributes to the broader fields of gerontology, public health and data science.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to acknowledge Dr Kirsten Quadflieg for her invaluable input during the discussions surrounding the revision process of this manuscript.
References
Footnotes
Contributors KD is the guarantor of the study and accepts full responsibility for the overall content of the manuscript. KD, SV and BB conceptualised the study. KD and BB developed the methodology. Resources and project administration were managed by KD, who also prepared the original draft and contributed to visualisation. All authors—KD, SV, JR, AS, DH and BB—reviewed and edited the manuscript. Supervision was provided by AS, DH and BB. KD led the funding acquisition. All authors have read and agreed to the published version of the manuscript and are accountable for its integrity and accuracy.
Funding This work was supported by PXL University of Applied Sciences and Arts (2/DWO/2021/HC/P133) and by Agentschap Innoveren en Ondernemen (2/DWO/2022/HC/VL041).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.