Article Text

Abstract
Background Few studies have investigated the prevalence of chronic wounds and the clinical and sociodemographic characteristics of hospitalised patients affected by them. Understanding these characteristics within the inpatient setting can support improved follow-up, inform care strategies, enhance quality and safety and reduce associated healthcare costs. This study aimed to determine the prevalence and the sociodemographic profile of adult inpatients with chronic wounds admitted to the eight hospitals of the Catalan Institute of Health between 2016 and 2020.
Methods A descriptive, observational, cross-sectional and retrospective multicentre study was conducted using routinely collected clinical data from 1 January 2016 to 31 December 2020. The study encompassed hospital wards, step-down units and home hospitalisation services across eight public hospitals managed by the Catalan Institute of Health, the main public healthcare provider in Catalonia, Spain. The study included all patients aged 18 years or older who were hospitalised with chronic wounds during the study period. The main variables were nursing diagnoses of chronic wound types: pressure injuries (PIs), arterial ulcers (AUs), venous ulcers (VUs), mixed ulcers and diabetic foot ulcers (DFUs), as recorded in nursing electronic health records. Secondary variables included age, sex, reason for admission, unit of admission, hospital type, source of admission and discharge destination. A descriptive and comparative analysis was performed.
Results Among 796 698 hospitalised patients, 16 935 (2.1%) presented with at least one chronic wound. The most common types of chronic wounds were PIs and AUs. A slight decline in the prevalence of chronic wounds was observed over the study period. Cardiovascular and respiratory conditions were the leading causes of admission among these patients. AUs and DFUs were more prevalent in men, whereas VUs were more frequently observed in women. Patients with PIs had longer hospital stays, higher rates of intensive care unit admissions and increased in-hospital mortality. In contrast, patients with vascular ulcers more often required continued care after discharge (p<0.001).
Conclusions Chronic wounds continue to represent a significant healthcare challenge. It is essential to consider the clinical characteristics and health outcomes of hospitalised patients with chronic wounds in order to improve care quality and safety. Further research is warranted to explore the relationship between patient care complexity and the type of chronic wounds present.
- Prevalence
- Wounds and Injuries
- Hospitalisation
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. All relevant data are available in the article or the supplementary materials.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This multicentre study included a large number of patients.
Electronic nursing data are recorded voluntarily, and the nursing registry of chronic wounds may be associated with under-registration.
The results of this study only apply to adult inpatients.
Background
Chronic wounds (CWs) represent a heterogeneous group of lesions that include vascular ulcers (venous and arterial), diabetic foot ulcers (DFUs) and pressure injuries (PIs), among others.1–4 Sibbald et al have proposed that wounds persisting for more than 6 weeks should be considered chronic in nature.1
Multiple general and local factors contribute to delayed healing in CWs. These include advanced age, pharmacological treatments, malnutrition, comorbidities, social and familial context and inadequate wound management.5 The increasing life expectancy observed in recent decades is closely linked to a rising prevalence of chronic conditions, including CWs. It is estimated that between 1% and 1.5% of the population in high-income countries are affected by some type of wound, and in Europe, wound care accounts for approximately 2%–4% of total healthcare expenditure.3 6 7
According to the National Consensus Conference on Lower Extremity Ulcers,8 75%–80% of lower extremity ulcers are of venous origin, with a population prevalence of 0.5%–0.8%. In contrast, arterial ulcers (AUs)—those of ischaemic aetiology—have a prevalence ranging between 0.2% and 2%. Ulcers of neuropathic origin, typically associated with diabetes mellitus, are clinically categorised under the broader concept of diabetic foot. Epidemiological data suggest that diabetes mellitus affects 7%–7.5% of the general population, and it is estimated that 15%–25% of individuals with diabetes will develop a foot ulcer during their lifetime.8
PIs are defined as localised damage to the skin and underlying tissue, usually over a bony prominence, resulting from prolonged pressure and subsequent occlusion of the microcirculation. This process leads to tissue hypoxia and rapid degeneration.9 In Spain, recent studies have shown that PI prevalence has remained relatively stable in recent years, with the most recent data from 2022 indicating a prevalence of 0.043%.10 11 However, due to demographic trends and the rising incidence of chronic diseases such as diabetes and obesity, the incidence of CWs is expected to increase over the next decade.3 4 12 13 Over the past 15 years in Catalonia, nurses working in public hospitals under the Catalan Institute of Health, as well as other healthcare providers, have systematically documented the nursing care process and outcomes using the ATIC (Architecture, Terminology, Interface and Knowledge) standardised interface terminology within electronic health record (EHR) systems.14 More than 200 000 care episodes are recorded annually. These records include patient assessments, care plans (nursing diagnoses and interventions) and continuous monitoring of patient progress. Nurses routinely document wound types, care interventions based on wound assessment, and the use of specific wound care products.15
While several studies have assessed the prevalence of specific types of CWs, few have examined their overall prevalence or described the characteristics of hospitalised patients with CWs. A clearer understanding of the patient profile in our healthcare setting may contribute to improved clinical follow-up and the development of targeted strategies for managing these patients. This, in turn, can enhance the quality and safety of care while helping to reduce healthcare costs.
Therefore, the objective of this study was to determine the prevalence and sociodemographic characteristics of adult patients hospitalised with CWs at the eight hospitals of the Catalan Institute of Health between 2016 and 2020.
Methods
Setting and study design
A descriptive, observational, cross-sectional and retrospective multicentre study was conducted using routinely collected clinical data from 1 January 2016 to 31 December 2020. The study encompassed hospital wards, step-down units and home hospitalisation services across eight public hospitals managed by the Catalan Institute of Health, the main public healthcare provider in Catalonia, Spain. These centres were classified into hospitals of high and low complexity (A1, A2 and A3 for high complexity; B1, B2, B3, B4 and B5 for low complexity). The study included all patients aged 18 years or older who were hospitalised with CWs during the study period, in wards, step-down units and home hospitalisation services at eight public health hospitals. Excluded from the study were adult patients hospitalised in critical care units, short-stay units or emergency observation units. Patients identified as close to the end of life were also excluded. The sampling technique used was non-probabilistic consecutive sampling.
Patient and public involvement
Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Data collection
The data source used was Business Objects and the Minimum Basic Data Set (MBDS), the data warehouse of EHR systems in centres under study. For nursing record data, the extraction was performed annually from 2016 to 2020, by unit, centre and in aggregate. The data were pseudo-anonymised. These data were coded and reviewed to detect potential inconsistencies in a data collection sheet created with Microsoft Excel 2010. In the database, no identifying data of all included patients was present, as a consecutive numerical code was used to identify each patient. Study approval was granted by the institutional research ethics committee (PR185/21). Informed consent was waived due to the study’s retrospective design.
Variables
The main variables of the study were nursing diagnoses for the types of CWs: PIs, AUs, venous ulcers (VUs), mixed ulcers (MUs) and DFUs, recorded at the nurse’s electronic healthcare records. PIs were considered both hospital-acquired and community-acquired. In our study, community-acquired pressure ulcers were those recorded at the nursing station within the first 24 hours of admission. Hospital-acquired pressure ulcers were considered as those recorded after the first 24 hours of the patient’s hospitalisation. Secondary variables collected included age, sex, reason for admission (diagnosis-related groups), admission unit, type of hospital, source of admission and discharge destination (continuity of care).
Statistical analysis
The analysis strategy primarily included descriptive statistics, using the mean, SD and minimum and maximum values for variables that follow a normal distribution, while for variables that do not follow a normal distribution, the median, 25th and 75th percentiles and minimum and maximum values were used for analysing the sociodemographic characteristics of the study population and the prevalence of CWs. For the comparative analysis of sociodemographic differences according to the types of CWs, to detect significant differences between the types of CWs, the χ2 test or Fisher’s exact test was used for categorical variables and the t-test or Mann-Whitney U test for continuous variables. Statistical significance was established at a bilateral p<0.05. This analysis was conducted using SPSS statistical software V.23 (Chicago, Illinois).
Results
Prevalence
Between 2016 and 2020, 796 698 patients were admitted to the participating centres. Of these, 16 935 had some type of CW, meaning a global incidence of CWs of 2.1%: 9667 (1.21%) pressure ulcer episodes, 5080 (0.64%) AU episodes, 1167 (0.15%) generic ulcer episodes, 1139 (0.14%) VU episodes, 1105 (0.14%) DFU episodes and 190 (0.02%) MU episodes. When analysing pressure ulcers according to the stage, the results were as follows: 34.6% in stage I, 64.1% in stage II, 17.7% in stage III and 7.2% in stage IV, with stage II pressure ulcers being the most prevalent.
Regarding the global incidence by centre, we can observe that high-complexity hospitals have a prevalence of 2.39%, compared with 1.81% in low-complexity hospitals. The centres with the highest prevalence are centres A1 (3.57%), B5 (3.25%), A2 (2.69%) and B2 (2.40%), while those with the lowest incidence are centres B3 (2.03%), B4 (1.94%), A3 (1.58%) and B1 (0.82%).
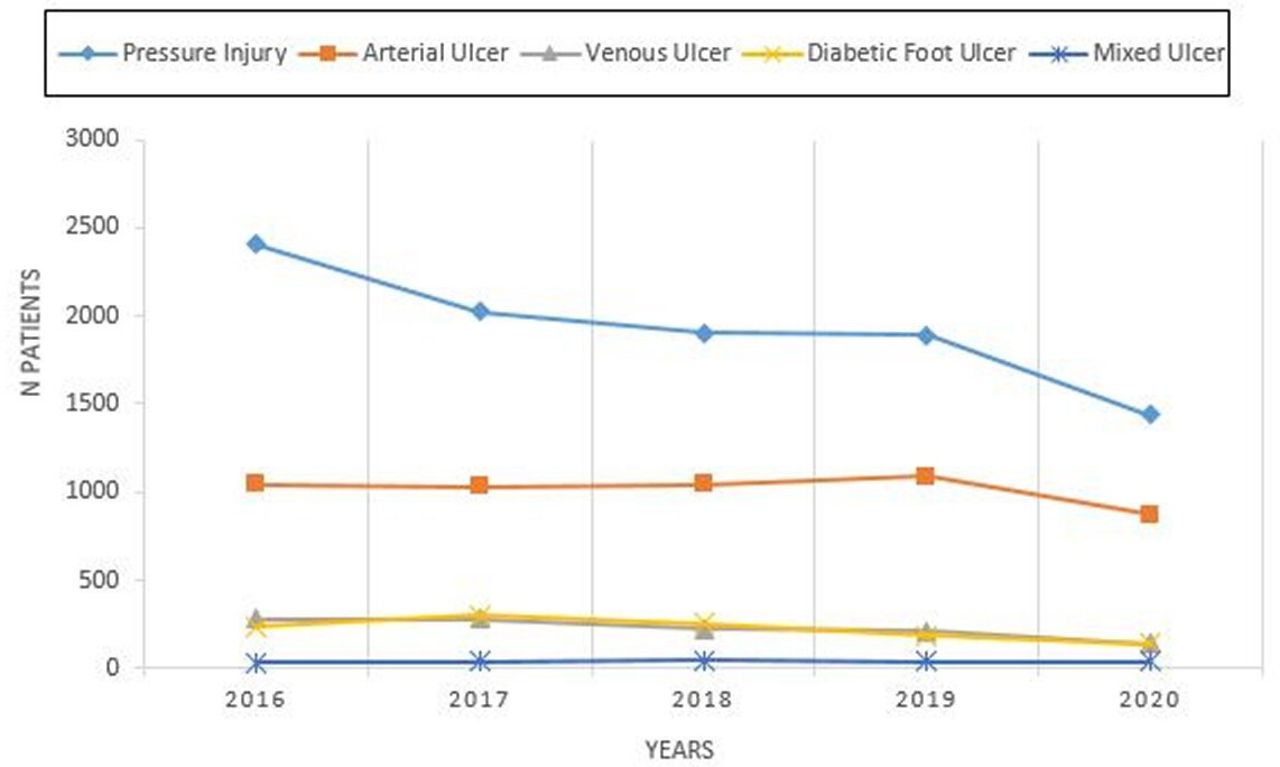
The prevalence during the study years of the different types of CWs showed a downward trend in PIs, VUs and DFUs. However, MUs and AUs remained stable over the 5-year study period (figure 1)

{kind=link}
Distribution of chronic wounds by year.
Clinical and sociodemographic characteristics
The clinical and sociodemographic characteristics of the study populations were analysed and are presented in online supplemental table 1. The mean age was 75.5 years, and 61.8% (10 472) were male. Regarding clinical characteristics, the mean length of stay was 13 days (IQR: 7–16). Regarding the type of admission, 78.2% (13 243) were episodes admitted via emergency, while 21.8% (3692) were scheduled patients. Of the patients’ episodes treated with CWs, 76.2% (12 900) came from their homes or social residences, 10.8% (1833) were referred from acute hospitals and 9.4% (1591) were referred from primary care centres. The main reasons for admission of the studied patients were cardiocirculatory disease (34.5%), musculoskeletal/connective tissue (15.2%) and respiratory disease (12.5%). Only 12.1% (2050) required admission to the intensive care unit (ICU), and 53.6% (9083) were discharged home, 27.3% (4626) to another hospital, 11.3% died (1906) and 7.5% (1272) were admitted to home hospitalisation.
Supplemental material
Analysing the relationship between the types of wounds and the sociodemographic characteristics of studied patients, we can observe that the mean age was significantly higher in patients with PIs and VUs (p<0.001). Additionally, differences in gender were observed, with a higher frequency of men among patients with AUs (74.2% vs 25.8%) and DFUs (70% vs 30%) compared with the total study population (p<0.001). In contrast, VUs were more prevalent in women, significantly increasing compared with the prevalence in the studied population (p<0.001).
Regarding the length of stay, a longer hospital stay was observed in patients with pressure ulcers compared with the global study population (median: 16 vs 13 days), while it was slightly lower in patients with VUs (median: 10 vs 13 days). It was also observed that among patients with AUs, the frequency of scheduled admissions was higher than in the overall population (30.5% vs 21.8%) (p<0.001). Regarding the source of studied episodes, no differences were observed among the different types of wounds.
However, it was identified that patients with PIs had a higher frequency of ICU admissions (17.9% vs 12%) (p<0.001). In terms of discharge destination, the mortality rate was higher in patients with PIs than in the overall study population (15.2% vs 11.3%), whereas the mortality rate was lower in patients with AUs (5.2% vs 11.3%) (p<0.001). Additionally, patients with VUs, AUs and DFUs required greater care continuity from primary care (p<0.001).
Finally, it is worth noting that although the main reason for admission among the studied patients was cardiovascular problems, this reason was more prevalent among patients with AUs than in the overall study population (65.7% vs 34.5%) (p<0.001). Additionally, a higher frequency of admission due to respiratory problems was observed in patients with PIs (18.2% vs 12.5%) (p<0.001).
Discussion
This study identified a 2.1% prevalence of CWs in hospitalised patients. The main chronic lesions were PIs and AUs. A slight downward trend in the prevalence of CWs was observed during the period 2016–2020. The main reasons for the admission of patients with CW were related to cardiovascular and respiratory diseases. AUs and DFUs were more prevalent in men, whereas VUs were more frequently observed in women. Additionally, patients with PI had longer hospital stays, a higher frequency of ICU admission and mortality during their hospital stay, whereas patients with vascular ulcers required more continuous care after discharge than the rest of the CW. These results help highlight that CW remains an important health problem, so it is important to consider the characteristics and health outcomes of hospitalised patients with CWs to establish improvements in the quality and safety of care.
It is estimated that 1%–2% of the population in developed countries will have CWs during their lifetime,16 slightly below the global prevalence results of this study. It should be noted that there are few similar studies in hospitalised patients with which to compare the global prevalence data obtained. Ahmajärvi et al, in their 2016 study, observed a prevalence of 0.08% of CW in hospitalised patients.17 Three studies in Spain show a prevalence of chronic CW ranging between 0.11% and 7.8%18–20 but do not include the hospitalised population. Regarding the downward trend observed in the prevalence of CWs over the years studied (2016–2020), there are national prevalence studies that inform us of a sustained trend, although only in PI and dependency-related injuries.10 21 This data concurs with our results. Conversely, a previous study by Yao et al, analysing the trend over 5 years (2014–2018), as in the present study, shows an upward trend of CW in China.22 It is possible that these results are related to the improvement in the quality of care in the different centres in our study and strategies introduced at the Catalan Institute of Health, such as the dissemination of the clinical practice guideline for lower extremity wounds in 2018.23 In addition, several studies were published regarding the progressive improvement in staffing levels during the studied years.24 Furthermore, in 2020, the trend was more pronounced due to the fact that it coincided with the COVID-19 pandemic. This had a significant impact on the hospitals included in the study, as the patients’ profile admitted throughout most of the year was different from the usual. The care intensity required at the time may have caused CW under-recording.
According to the aetiology of CW in this study, PIs are the most prevalent (1.21%). Previous studies conducted in hospitalised patients show similar results.25 26 Reviews conducted in Europe show a 10.8% prevalence of PI, with a wide variability depending on the countries, between 1.1% and 27.2%.27 28 Another systematic review conducted demonstrated a 0.2%–29.6% prevalence of PI.29 The last national prevalence study conducted in Spain in 202221 established a 7.7% prevalence of PI in hospitalised patients. In the field of primary care, previous studies show a prevalence of approximately 0.1%,18–21 quite below the results obtained in studies of hospitalised patients, which may be due to the fact that hospitalised patients are more at risk of developing PI due to compromised mobility.27 As for the stage of PI, the most prevalent in our study were stage II PIs, which is consistent with the fifth national prevalence study in hospitalised patients.10 Amir et al, in 2016, observed an 8% prevalence of PI, of which 42.3% were stage III–IV.30 The prevalence of VUs was estimated at approximately 0.09%. Internationally, other studies establish a 0.05% prevalence of VU in hospitalised patients.21 In primary care, the result was 0.04%.18 19 Both studies are consistent with the results obtained in our study. According to DFUs, our study shows a prevalence of 0.09% in hospitalised patients. Internationally, we find that the range of prevalence is wide, between 1.2% and 20.4%.28 A systematic review conducted in Australia established a 2.6% prevalence of DFU. Other studies in primary care show a prevalence of 0.01%.18 19 As for AUs, which in our study accounted for 0.42%, in a previous systematic review, the prevalence of AU was estimated between 0.7% and 10.9%.29 Graves et al, in their narrative review, found that data on AU prevalence are scarce, and those that they found concluded a prevalence of 0.01% in primary care services.27 This is consistent with the prevalence of other studies (0.012%–0.005%),18 19 probably because they are studies in the field of primary care.
Focusing on sociodemographic characteristics and in line with other studies, the prevalence of CW increases with age, consistent with results obtained in previous research.10 19 20 Older people with chronic diseases and multiple comorbidities are at greater risk of developing CW. Age increases not only the risk of developing a wound but also the delay in its healing.17 Males predominate with 56% of cases, consistent with other studies in the hospital setting,10 20 unlike the results found in primary care, where females prevail.18–20 31 In terms of patient profiles, there are studies that coincide with ours25 in which the most common pathologies were cardiorespiratory. Finally, our study shows that ICU stays increase the prevalence of PI compared with the rest of the CW. These data are consistent with previous studies showing that prolonged ICU admission is associated with poorer health outcomes.32 Finally, regarding discharge destinations, it is observed that patients with vascular ulcers required more care from primary care. This may be due to the fact that many of these patients have a type of chronic injury that requires a multidisciplinary approach led by advanced practice nurses or expert nurses who are precise in the diagnosis and recording of the specificity of CW,14 improving their approach, management and follow-up. Standards and structured data allow better management of treatment, involve patients in their own care and reduce the possibility of omitting necessary parameters to describe and understand wound progression. Increasing comorbidities are variables that impact the complexity of patients treated in hospitals. Responding to this complexity requires significantly more dedication time and often causes a lack of time to address care,29 so the figure of the advanced practice nurse in CW in hospitalised patients could help reduce this omission. The incorporation of an advanced practice nurse could help improve the diagnostic accuracy of CW care. Professionals are trained to treat wounds such as pressure ulcers, vascular ulcers and diabetic ulcers and have good diagnostic accuracy, but there are rare wounds that may resemble these and lead to misdiagnosis. A misdiagnosis prolongs the patient’s suffering, delays healing, increases costs and can worsen the condition with inappropriate treatments.33 Studies focused on CW care recommend that professionals maintain a high level of awareness of potentially malignant lesions. This can help make a timely and accurate diagnosis and avoid the application of inappropriate treatments due to a misdiagnosis. It is crucial to emphasise the importance of a thorough evaluation before classifying a wound as chronic.34 For all the above reasons, it is important to research the standardisation of treatment and the outcome of CWs once diagnosed, as well as factors related to nursing care that predict a proper wound outcome.35 Research on tools that assist us in making both diagnostic and treatment decisions is needed, and AI (Artificial Intelligence) could be of great help in this regard.
Conclusion
This study identified a 2.1% prevalence of CWs in hospitalised patients. The main chronic lesions were PIs and AUs. A slight downward trend in the prevalence of CW was observed between 2016 and 2020. The main reasons for the admission of patients with CW were related to cardiovascular and respiratory diseases. AUs and DFUs were more prevalent in men, whereas VUs were more frequently observed in women. Additionally, patients with PIs had longer hospital stays, a higher frequency of ICU admission and mortality during their hospital stay, whereas patients with vascular ulcers required more continuous care after discharge. These results help highlight that CWs remain an important health problem. It is important to consider the characteristics and health outcomes of hospitalised patients with CWs to establish improvements in the quality and safety of care based on nursing diagnoses that allow us a high level of specificity.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. All relevant data are available in the article or the supplementary materials.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Clinical Research Ethics Committee of the Bellvitge University Hospital (PR185/21). Informed consent was waived due to the study’s retrospective design. Ethical and data protection protocols related to anonymity and data confidentiality (access to records, data encryption and archiving of information) were complied with throughout the study.
Acknowledgments
We thank the CERCA Programme/Generalitat de Catalunya for institutional support.
Footnotes
Contributors All authors had full access to all study data and took responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: MMLJ, JA and MG-S. Team coordination: MMLP and MG-S. Acquisition of data: MMLJ, MT-P, MP-P, TC-N, EZP and CB-M. Analysis and interpretation of data: MMLJ, MGS, JA and MR-G. Drafting of the manuscript: MMLJ, JA and MG-S. Critical revision of the manuscript for important intellectual content: MR-G, MT-P, MP-P, TC-N, EZP and CB-M. Statistical analysis: MMLJ and JA. Obtained funding: MMLJ. Administrative, technical and material support: MT-P, MP-P, TC-N, EZP and CB-M. Study supervision: MG-S and MR-G. MMLJ is responsible for the overall content as guarantor and accepts full responsibility for the finished work and/or the conduct of the study; he had access to the data and controlled the decision to publish.
Funding This study had been funded by the COIB—Nurse Research Projects Grants (grant PR-553/2022) and by the Agencia de Gestió d’Ajuts Universitaris i de Recerca (AGAUR) del Departament de Recerca i Universitats de la Generalitat de Catalunya (grant 2021SGR00929).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.