Article Text

Abstract
Introduction Systemic racism exposes Black and Latinx adolescents to a range of traumatic stressors that increase the risk for long-term emotional and behavioural health (EBH) problems. Researchers have theorised that critical consciousness (CC)—awareness of societal inequities and engagement in action to promote social justice—may serve as a protective factor that promotes youth well-being. There are few rigorous longitudinal research studies, however, that examine the development of CC among adolescents, the association over time of CC with EBH and the potential of CC to protect against harmful effects of race-related stress. This longitudinal study, Resilience in a Stressful Era (RISE), addresses these gaps using a mixed methods approach with Black, Latinx and White adolescents in Baltimore.
Methods and analysis We plan to enrol up to 650 Black, Latinx and White adolescents ages 14–19 who reside in Baltimore, Maryland. The recruitment will include outreach through youth-serving organisations, community events, youth networks, social media, snowball sampling and re-contacting adolescents who participated in a prior study (R01HD090022; PI: Mendelson). Participants will complete online questionnaires assessing exposure to pandemic- and race-related stress, CC and EBH twice per year over 4 years as they transition into early adulthood. Using an explanatory sequential mixed methods approach, in-depth interviews exploring the development and impact of CC will be conducted with a subset of participants selected based on their CC scores and, separately, their caregivers. A Youth Advisory Board comprised of adolescents who are representative of our target study population will be developed to provide input on the study and its implementation. Growth mixture modelling and latent variable modelling will be used to analyse quantitative data. Themes identified through qualitative analyses will expand the understanding of quantitative findings.
Ethics and dissemination All study procedures were approved by the Johns Hopkins Bloomberg School of Public Health Institutional Review Board. Findings will be disseminated through publications in peer-reviewed journals and presentations at academic conferences. We will also communicate research findings with study participants and disseminate findings to the Baltimore community, such as developing briefs for the Baltimore City Health Department and/or hosting a town hall meeting for Baltimore families.
- Adolescents
- MENTAL HEALTH
- Community Participation
- Health Equity
- Risk Factors
- Stress, Psychological
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Quantitative and qualitative data collection at multiple assessment points across a 4 year period when participants are becoming young adults will provide insights into an important developmental transition with implications for adult emotional and behavioural health.
The study’s rigor and potential to advance the field are enhanced by the recruitment of a racially and ethnically diverse adolescent sample, mixed methods with sequential explanatory analyses and the assessment of three domains of emotional and behavioural functioning, including emotional well-being.
Partnership with youth-serving community agencies and guidance and implementation support from a study Youth Advisory Board increases our capacity to engage the adolescent population and represent their perspectives authentically.
Like the vast majority of observational studies, our study will not use a random sample of youth, and the results will not be weighed to represent Baltimore or national adolescent populations.
While our study is focused on Black, Latinx and White youth, many other racial/ethnic groups experiencing racism are not part of this study (eg, Asian and Native youth).
Introduction
Adolescence is a key developmental period that influences long-term health and well-being.1 Cumulative risk models indicate that adolescents who experience additive stress are at risk for developing emotional and behavioural problems (eg, depression, substance use) with negative consequences for the transition into adulthood2 3 and adverse impacts over the life course and inter-generationally. Systemic racism, the oppression of specific racial or ethnic groups at a structural or policy level,4 disproportionately exposes marginalised adolescents to acute and chronic stressors, including poverty and violence.5 Thus, for Black and Latinx adolescents in low-income, often segregated, settings, experiencing racism and discrimination during a critical developmental period creates a significant risk for current and future emotional and behavioural problems.6–9
In times of general societal stress, such as the COVID-19 pandemic and its aftermath, systemic racism further exacerbates hardships for Black and Latinx adolescents, resulting in high levels of family financial strain, food insecurity, disruption in education, and illnesses and deaths of loved ones.10–14 Compounding these issues, Black and Latinx adolescents continue to be exposed to publicised instances of police brutality, stressful personal interactions with police and oppressive anti-Latinx immigration policies.15–17 Data are lacking, however, on the impact of the current social climate18 on these young people. Gaps include the lack of longitudinal data on multiple race-related stress exposures, the assessment of multiple emotional and behavioural health (EBH) domains, including both mental and behavioural health problems (eg, depressive, anxiety and post-traumatic stress symptoms, problematic substance use) and a dearth of studies that involve Black, Latinx and White adolescents in an urban context as participants. In addition, it is important to acknowledge and examine how Black and Latinx adolescents experience racism differently and how multiple identities (eg, identifying as Latinx and Black) intersect. Such data are critical for understanding current and prospective trends in adolescent EBH and particularly identifying how differing experience of racism may lead to specific stressors for Black, Latinx and White youth.
The present study addresses those gaps using a strength-based approach. A strength-based approach is well-suited to identifying and valuing (and later expanding through intervention) the inherent talent and potential of marginalised youth who have been denied equitable opportunities. Unlike much of the prior research on adolescent mental health, this study employs a positive youth framework to assess emotional wellness as a core EBH domain, including flourishing, hope and resilience. The aims and design are informed by a positive youth development framework and resiliency theory. The former emphasises the inherent potential in all young people and promote youth assets,19 whereas the latter highlights internal assets and external resources that protect against the negative effects of adversity.
The study also explores the development and impact of critical consciousness (CC), which has emerged as a competency associated with positive developmental functioning, especially for marginalised adolescents. CC is comprised of three components: (1) awareness of unjust social systems (critical reflection), (2) a belief that communities can resist these systems (critical motivation) and (3) engagement in anti-oppressive actions (critical action).20 21 Evidence suggests that CC may promote positive youth development22 and youth empowerment23 through the development of social justice activism and leadership. CC is also associated with other positive aspects of youth functioning, such as career development, community engagement, civic participation and academic achievement. Some studies suggest that aspects of CC are also linked to overall mental health, including lower depressive symptoms24 and positive emotional development.22 25 26
There are few longitudinal studies concerning CC, however, and we know little about how the development of CC over time may differ for minoritised youth.21 Relatedly, the development of CC among adolescents with privileged identities (eg, White youth) is poorly understood.21 Research on associations between CC and mental health is also scarce, particularly studies examining a range of emotional and behavioural outcomes among youth of different racial and ethnic groups longitudinally.21 Addressing these gaps is critical to our understanding of when and how CC develops, whether it is associated with mental health for young people, and distinct developmental pathways of CC for different racial and ethnic groups can help lay the groundwork for the development of tailored interventions to promote CC among diverse young people.
Positive adaptation, or resilience, occurs when protective factors at the individual and/or contextual levels buffer a person against the harmful effects of stress exposure over time and across contexts.19 27–29 Consistent with a strength-based approach, CC has been proposed as a potentially important protective factor for youth exposed to oppressive systems. Specifically, CC is hypothesised to mitigate the harmful effects of racism and associated stressors.20 No prior studies to our knowledge, however, have explicitly tested whether CC has protective effects in the context of race-related stress. This study will investigate CC as a protective factor that reduces harmful links between trajectories of race-related stress and EBH and will evaluate these associations for Black, Latinx and White adolescents.
To address the gaps outlined above, we are conducting a mixed-methods longitudinal study titled RISE (Resilience in a Stressful Era) Baltimore. We are currently recruiting Black, Latinx and White adolescents aged 14–19 residing in Baltimore and will follow their development for 4 years as they transition into early adulthood. Specifically, the study will assess adolescents’ stress exposures (including race-related stressors such as police interactions and immigration policies), adolescents’ development of CC, the prospective associations of stress exposures and CC with EBH and the potentially protective influence of CC.
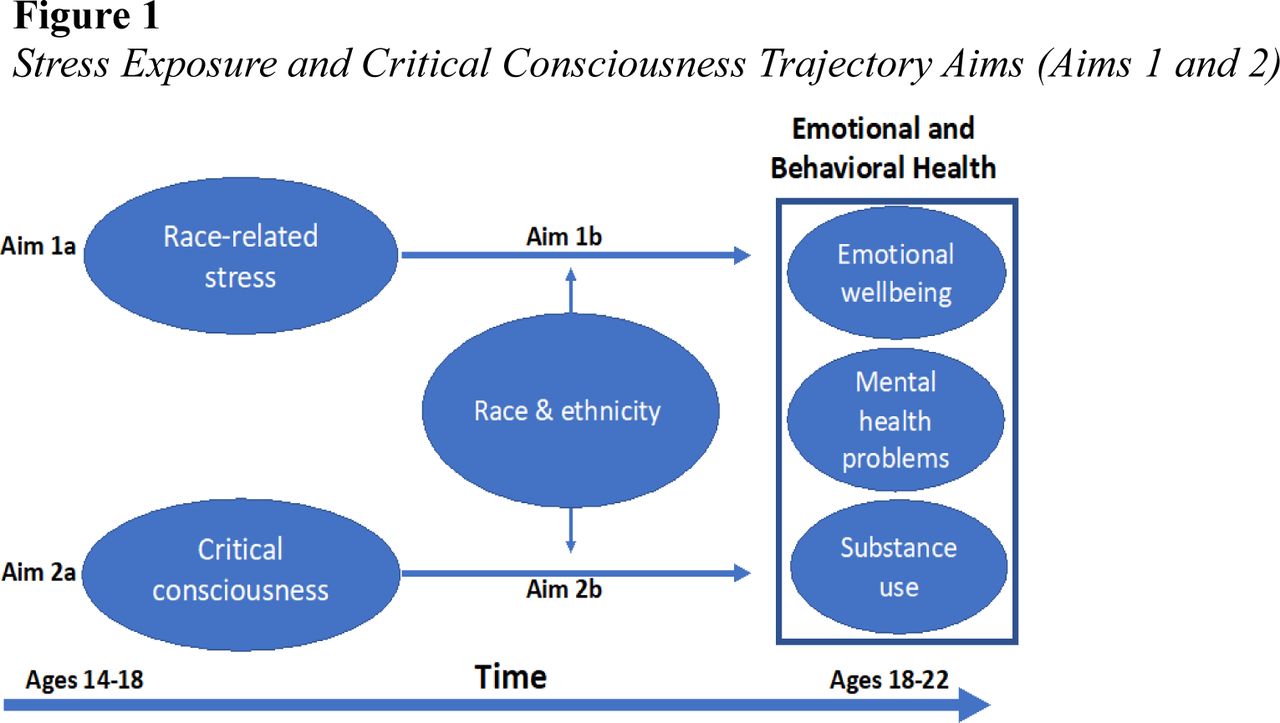
The three study aims are illustrated in figures 1 and 2. First, as shown in figure 1, we will identify trajectories of adolescent stress exposures (Aim 1a) and assess the trajectories’ associations with EBH outcomes (Aim 1b). Second, we will identify trajectories of adolescent CC (Aim 2a) and assess the trajectories’ associations with EBH outcomes (Aim 2b; see figure 1). For each component of Aims 1 and 2, we will test how trajectories and associations may differ for Black, Latinx, and White youth.

Stress exposure and critical consciousness trajectory aims (Aims 1 and 2).

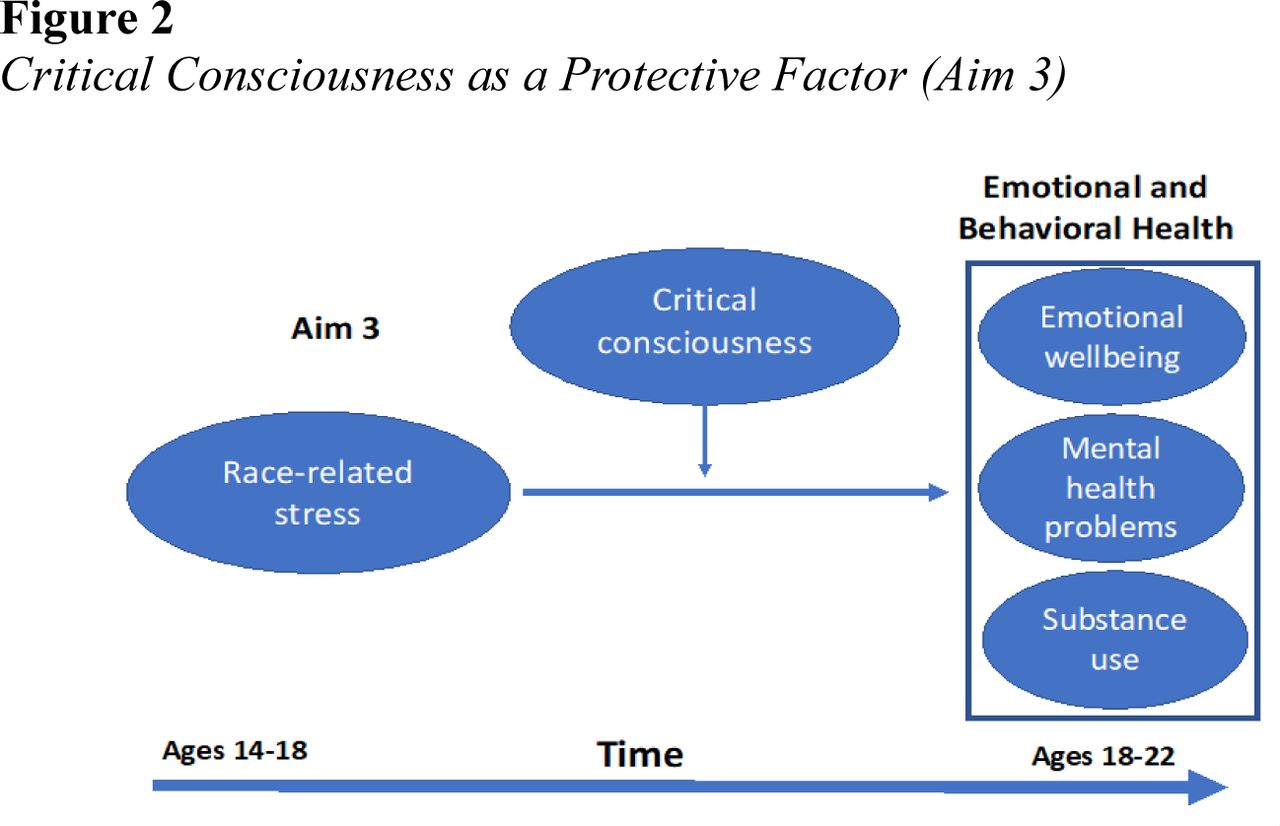
Critical consciousness as a protective Factor (Aim 3).
Third, as shown in figure 2, CC will be evaluated as a protective factor that may reduce harmful links between stress exposures and EBH (Aim 3). We will assess whether these relationships may differ for Black, Latinx and White youth. For each aim, qualitative data will be used to contextualise and expand survey findings.
Methods and analysis
Study design
This is a mixed-methods longitudinal study, with an explanatory sequential design.30 Participants will complete two self-administered online questionnaires per year over a 4 year period, for a total of eight waves of survey data collection. In-depth qualitative interviews will be conducted with a subset of participants, some with high scores on CC and some with low scores on CC and, separately, with their parents or caregivers. Interviews will be conducted one-on-one virtually or over the phone annually for four total qualitative time points. The goal of these interviews is to explore the development and mental health impacts of CC and potential differences between young people with high and low levels of CC.
Patient and public involvement: the Youth Advisory Board (YAB)
Meaningful inclusion of youth input in research and programming that affects adolescents and young adults improves the quality and outcomes of these processes and boosts youth engagement in resulting services.31–33 We will develop a YAB to guide study implementation, including measurement selection, recruitment strategies, assessments, interpretation of findings and next steps for shaping policies, practices and programming. We will also train YAB members to conduct qualitative interviews with adolescent participants to promote participant comfort and trust and provide research and professional development training for the YAB members.
The YAB will include 6–12 young people from Baltimore who are well-positioned to understand participant experiences, needs and perspectives. Recruitment and supervision of YAB members will be facilitated by our partnerships with HeartSmiles,34 a grassroots community organisation that trains Baltimore City youth in leadership and professional development (https://heartsmilesmd.com), and Centro SOL,35 a multidisciplinary organisation that serves Latinx youth and families (https://jhcentrosol.org). We will hold regular YAB meetings at convenient times for members and will pay them for their time and contributions.
Participants and recruitment
We will enrol up to 650 young people who are between the ages of 14 and 19; identify as Black, Latinx, White or multiracial; reside in Baltimore; and currently or previously attended school in Baltimore. Within these parameters, there were no exclusion criteria. We selected this baseline age range as we are interested in young people’s stress, mental health and CC development across the transition from adolescence into emerging adulthood. With help from our YAB, participants will be recruited through the outreach to local youth-serving organisations, youth networks and social media posts on a study Instagram account. The study staff will also attend community events to distribute information about the project. In addition, we will use snowball sampling: young people will receive a $20 VISA gift card for each person they recruit who enrols in the study and completes the questionnaire.
We will also re-contact young people who participated in a previous study called Project POWER (Promoting Options for Wellness and Emotion Regulation; R01HD106654). The Project POWER sample consisted of 631 eighth graders across four cohorts (59% female, 74% Black, 15% Latinx, 7% White, 3% multi-racial and 1% other races/ethnicities) who are now 14–19 years old. Eligibility criteria for Project POWER were the same as those for RISE, except that Project POWER participants attended one of 29 participating Baltimore public schools. Inclusion of Project POWER participants will enhance the feasibility of recruiting our goal sample size due to our prior connection with those young people.
Consent and incentive procedures
Young people under age 18 will be required to provide signed parent permission and signed assent; those 18 or older will provide signed consent. The RISE Baltimore project website will include videos in English and Spanish in which YAB members will describe the study in a clear and engaging manner, as well as a link to REDCap, a secure web-based application hosted through Johns Hopkins University where adolescents can complete the eligibility screener questionnaire. Blank assent and consent forms will be available on REDCap for eligible youth to sign and upload. Eligible adolescents will be asked to provide their contact information; those under age 18 will also be asked to provide contact information for a parent or legal guardian. The study staff will follow up with parents to inform them about the study and guide them through providing signed permission through the portal.
The online questionnaire incentive, which is emailed to the youth after completing the questionnaire, is scaled to incentivise prompt response ($35 for completing within 24 hours of invitation and $25 if completed later than that). Electronic Mastercard gift card codes were chosen because they can be used in many locations and can be sent and received quickly after participants complete the questionnaire. Youth will receive an additional $25 gift card honorarium for each completed interview if they are selected for the qualitative subsample and agree to participate. Caregivers will also receive $25 for each interview they complete if they are contacted and choose to participate in the qualitative component.
Measures
Quantitative measures
Table 1 summarises the quantitative measures to be used in the study. Whenever possible, we selected measures that were developed or tested with young people of colour in urban contexts. The age of the participants will range from 14 to 19 years at baseline; for those participants who are under 18, we will use paediatric instrument versions when appropriate. Similarly, participants who are 18 years and older will complete the adult instrument version. We chose this option for instruments that were either specifically normed and/or developed for adolescents under 18 or for where it made sense to do so given the questions. We have noted which version we have used in table 1.
Measurement domains, constructs, variables and instruments
Descriptions of selected scales key to CC and race-related stress
Short-Form Critical Consciousness Scale36: A 13-item scale assessing adolescents’ views on race and class-based in equality (critical reflection), their self-efficacy to address these inequalities (critical motivation) and the socio-political actions they take in response to critical reflection and motivation (critical action). For adolescents who reported experiencing racial injustice, we developed questions to ascertain the type of discrimination experience, in what setting and how it affected them.
Perceived policy effects scale (PIPES)37 38: A 24-item scale that measures of the impact of immigration policies on Latino families. While it was originally developed and validated for use with parents, high reliability subscales of the measures have been used in a self-report format for adolescents.
Survey of the health of urban residents (SHUR)39: A subset of items from these measures assessing youth experiences with police brutality will be used, including questions about police cursing/harsh language, searching/frisking, threats and displays of force and the deployment of weapons against respondents (eg, stun gun, firearm).
Demographic characteristics
Questions assessing race and Latinx ethnicity will be based on the recommendations of the US Census.40 Adolescents who endorse Latinx ethnicity are asked about their country of origin. Gender classifications will include female (including cis and trans girls), male (including cis and trans boys) and non-binary. We expect the number of gender minority youth (ie, trans boys, trans girls and non-binary youth) to be small. We will also gather other relevant demographic data (see table 1).
Questionnaire development
Questionnaires will be pilot tested with members of our YAB to ascertain cultural and developmental appropriateness. For selected constructs that are particularly central to the study and have been less widely used and tested (eg, CC), we will conduct cognitive testing of the items with YAB members and will refine item wording based on their feedback. For a list of investigator-developed items, please see the online supplemental file 1.
Supplemental material
Qualitative measures
Interviews will explore adolescent and caregiver perceptions of participant CC, including social issues they care about, activities they engage in to advance those issues, family members or other people who helped develop their interest and the emotional impact of their involvement. For participants who do not endorse an interest in social issues, interviews will explore other interests and activities they enjoy, as well as reasons for their lack of interest or engagement with social issues. Interviews will be conducted using a qualitative interview guide, which was developed by the investigator (see online supplemental material).
Data collection
This study is funded from 1 August 2021 to 1 August 2026, with a possible extension to 1 August 2027. Recruitment began in November 2022 and ended in March 2023. Data collection is currently ongoing.
Staff training
All staff members are required to complete training in the ethical treatment of human subjects, child safety policies, the history of structural racism in Baltimore and historical abuses of research power by Baltimore research institutions that have created mistrust of research among many Black and Latinx Baltimore residents. Research assistants are trained to be clear, respectful and sensitive in their interactions with youth and families and alert for signs of participant discomfort. All parents and youth will be informed that they are free to decline research participation, stop participation at any time, restart participation at any time (ie, miss one survey data point, but wish to complete others) and skip questions they do not wish to answer. Our team includes Spanish-speaking staff who will reach out to Spanish-speaking families; consents, questionnaires and interviews can be administered in Spanish if preferred.
We will also train several young people from the YAB to serve as qualitative interviewers for this study. This training will include education about the nature of, and rationale for, qualitative research, discussion of effective interview techniques and role plays with feedback. We will pair interviewers with adolescent participants based on shared gender and race/ethnicity whenever possible. Study investigators will review the first few audiotaped interviews each young person conducts and will provide supervision and coaching as needed. The young people will be paid for their time in training and conducting interviews.
Quantitative data collection
Participants will complete the survey on REDCap using a Smartphone or computer; dates and completion of follow-up surveys will also be tracked using REDCap. Participants lacking appropriate technology or digital access can opt to have a team member administer the survey to them over the phone or can complete a paper copy mailed to them. Participants will receive a text and email with a personalised survey link every 6 months. The study staff will also contact participants to remind them to take the survey and will follow up with those who do not complete it via email, text, phone calls and private, direct social media messages (if social media contact information was provided by the participant at enrollment). For participants under the age of 18 at enrollment, parents will be contacted to remind them that their child needs to complete the survey if needed.
Each follow-up survey will have a 5 week window for completion. Participants will be contacted 2 weeks prior to their follow-up date and will have until 2 weeks after the date to complete the survey. For example, if a participant has a follow-up survey scheduled for Tuesday in the second week of March, they will be contacted on Monday in the fourth week of February to start the questionnaire and will have until Friday of the fourth week of March to complete it.
Qualitative data collection
We will identify a subsample of Black, Latinx and White participants with whom to conduct in-depth interviews. We will select 12 participants who are Black: six with high baseline scores on CC and six with low baseline scores (with a particular focus on their scores on the sociopolitical participation subscale). We will attempt to interview an equal number of boys and girls at each level of CC to explore possible gender differences in the development of CC. We will follow the same approach for identifying subsamples of Latinx and White youth for interviews for a total of 36 youth who participate in qualitative interviews.
We will conduct 30 min audio-recorded phone or Zoom interviews with this subset of adolescents once per year and (separately) with one of their parents or caregivers (n=36) once per year. YAB members who are trained as interviewers will conduct the interviews with adolescent participants. The study staff will conduct interviews with parents/caregivers. We will follow the same subset of adolescents and caregivers over the 4 years of data collection to gather longitudinal qualitative data. If interviewees no longer wish to participate or are unreachable, we will identify participants with similar characteristics to interview in their stead.
Protocol for addressing youth mental health needs
Our surveys will not assess suicidal ideation or behaviour but will include measures of psychological distress (see table 1). The REDCap system will score the measure of depressive symptoms in real time. Participants will be notified at the end of the questionnaire if they scored above a clinical cut-off on depressive symptoms that their answers indicated they may be experiencing some distress; they will be linked with a list of local mental and behavioural health services and will be encouraged to reach out to Dr Mendelson if they have questions. If they are under 18, their parents/caregivers will receive a similar communication. Dr Mendelson, a licensed clinical psychologist, will be available to address questions from adolescents and their parents over the study and provide additional information about local mental health services if desired. We will also provide a list of local mental and behavioural health services to all participants at the end of each questionnaire regardless of their questionnaire scores.
Quantitative data analyses
Overall analytic approach
Both the study conceptual framework and data-responsive model building will inform our approach to allow for flexibility in modelling individual differences. We will use growth mixture modelling41 to identify the race-related stress exposure and CC trajectories and explore the heterogeneity of these trajectories.41–44 Using these techniques allows for accounting of missing data through full information maximum likelihood methodology, if the data are missing at random.41–45 These person-centred analyses will also explicate the role of race and ethnicity in the trajectories and their associated outcomes. While we will be appropriately powered to explore differences across Black, White and Latinx groups,46 we will be underpowered for analyses focused on multi-racial groups. For these, and other low prevalence races, we will focus on more descriptive analyses. Additionally, sensitivity analyses will explore whether the magnitude of associations differ when the Project POWER participants are or are not included in analyses. Further, in all analyses, we will include gender, age, ethnic identity and prior trauma as predictors of class membership and may test if these variables moderate the relationship between stress exposures and EBH outcomes.36 47 48
Aim 1a: identify trajectories of adolescent stress exposure and test how they differ for Black, Latinx and White youth
We will first determine the number of trajectories present in the overall sample using growth mixture modelling.43 After identifying trajectories, we will use measurement invariance testing to account for trajectory differences associated with race/ethnicity following the multiple-indicator multiple-causes49 and item response theory50 frameworks. If measurement invariance testing suggests differential item functioning (DIF) with regard to race/ethnicity, we will perform iterative models testing for uniform and non-uniform DIF across all items.
Aim 1b: assess how trajectories of race-related stress are associated with EBH outcomes and test how these associations may differ for Black, Latinx and White youth
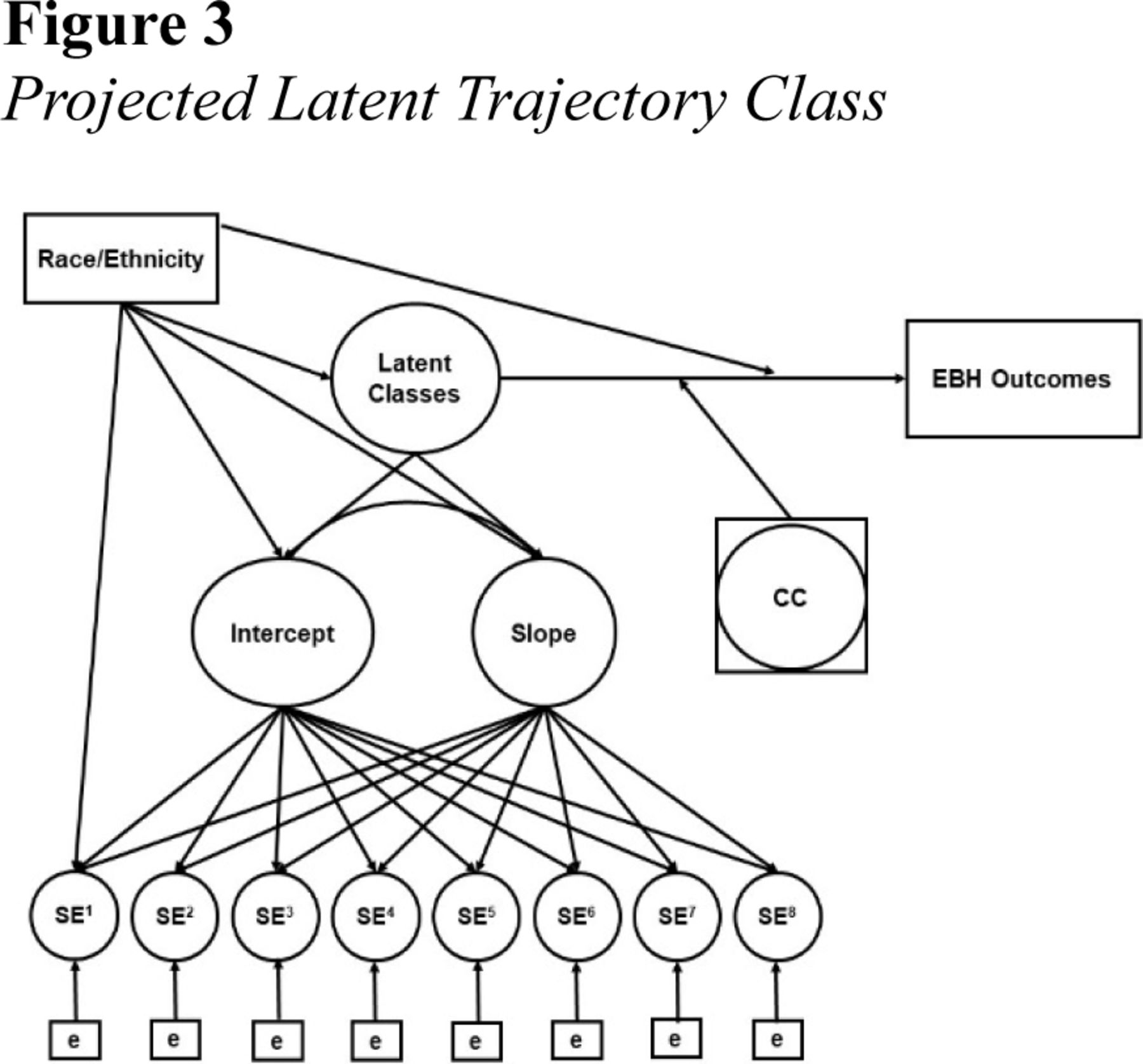
For this aim, latent trajectory classes and posterior class probabilities estimated in Aim 1a will be used to extend the model to include a distal outcome (EBH; see figure 3). After the main effect model is estimated, we will add an interaction between the latent trajectory classes and race/ethnicity to determine51 if race/ethnicity moderates the relationship between stress exposure trajectories and EBH outcomes.

{kind=link}
{kind=link}
{kind=link}
Projected latent trajectory class. CC, critical consciousness; EBH, emotional and behavioural health.
Aim 2a: identify trajectories of CC and test how they may differ for Black, Latinx and White youth
This aim will follow the same general modelling procedure as Aim 1a: an iterative process to develop a measurement model that accounts for potential DIF for race/ethnicity. The class enumeration process will use standard fit statistics to determine the best fitting model, followed by the measurement invariance testing process laid out in Aim 1a.
Aim 2b: assess how trajectories of CC are associated with EBH outcomes and test how these associations may differ for Black, Latinx and White youth
Analyses for this aim parallel the methods described for Aim 1b. Using the model determined in Aim 2a, a nominal latent class variable, along with the posterior class probabilities, will be used to build a latent trajectory regression model (see figure 3). The main effect model will include a regression between latent trajectory class and EBH outcomes and then the interaction between latent trajectory class and race/ethnicity regressed on EBH outcomes.
Aim 3: evaluate CC as a protective factor that reduces harmful links between race-related stress and EBH and test how these associations may differ for Black, Latinx and White youth
Informed by the measurement invariance testing in Aims 1 and 2, we will first build a structural equation model to appropriately model stress exposure and CC over time. The specific model will depend on the measurement models determined in Aims 1 and 2. For example, if CC remains stable across time, we may consider including a CC score averaged across timepoints as a moderator of the relation between stress exposure trajectories and EBH outcomes (see figure 3).52 53
Alternative analytic approach
Our goal is to recruit approximately even numbers of Black, Latinx and White youth; however, given that Baltimore is a majority Black/African American population, it is possible that our sample sizes will be uneven. If this occurs, we would consider analysing the proposed aims separately for Black, Latinx and White youth rather than using race/ethnicity as a moderator.
Power
The focus of this study is to investigate the heterogeneity of trajectories of key constructs over time and estimate the influence of predictors on these patterns. Given the complexity surrounding the determination of power to identify the accurate number of classes in a given growth mixture model, we rely on prior simulation studies suggesting that we have adequate power (approximately 80%) to extract the correct number of classes with eight items and between 300 and 600 participants. Further, assuming the presence of EBH constructs approximately match the prevalence rates from Project POWER (rates of elevated anxiety, depression and trauma range from 20%–45%) with a two-tailed alpha level of 0.05, we will have approximately 80%–95% power to detect a statistically significant relationship between EBH outcomes and stress exposure trajectory class membership. Thus, we feel confident in power levels for detecting small-moderate effect sizes for full sample analyses and moderate to large effects for within race/ethnicity analyses.
Qualitative and mixed methods analyses
As noted above, we will use an explanatory sequential design,30 54–56 in which the qualitative subsample consists of Black, Latinx and White youth, who are selected for in-depth interviews based on their baseline survey scores on CC (high/low), as well as a caretakers of youth who are interviewed will also be invited to participate in a separate interview. Interviews will be audiotaped, transcribed and uploaded into a qualitative data management programme (Atlas.ti).57 Emergent themes will be summarised, as outlined by Miles and Huberman.58 Interview data will be coded independently by a primary coder and two secondary coders, by tagging and then regrouping responses by observed themes. A few transcripts will be read by each coder to develop an initial coding scheme. After reading all transcripts, coders will meet to refine the scheme until no new codes emerge. Once data are coded, matrices of the key codes will be developed to look for patterns, particularly themes regarding how aspects of CC may influence stress responses and EBH. Causal network diagrams may also be developed to illustrate relations emerging from the data.58 For instance, a causal network diagram can be created to ‘map’ how linkages among stressors, CC and mental health influence one another.
Interview data will be used to contextualise, interpret and expand on quantitative survey findings. For instance, questionnaires will gather information about participants’ level of CC, and interviews will explore how adolescents become engaged in activities related to critical action, what these activities mean to them and how these activities affect their mood. To aid in merging quantitative and qualitative data, we may create joint displays of quantitative and qualitative findings that enable cross-comparisons.59 We anticipate that these mixed-methods analyses will provide insights into how, for whom and under which conditions CC may serve a protective function, with implications for future intervention development.46 60
Discussion
This mixed-methods longitudinal study will gather data on race-related stress exposures, mental health and CC over a 4 year period in a sample of Black, Latinx, White and multi-racial adolescents residing in an urban context. RISE Baltimore’s focus on current crises and their impact on adolescents is both novel and timely. The global COVID-19 pandemic, structural racism and associated economic and social upheavals are impacting adolescents in ways that may shape their lives for years to come, particularly Black and Latinx adolescents in under-resourced communities who are exposed to cumulative traumatic stressors stemming from structural racism. In particular, the COVID-19 pandemic and related financial downturn are likely to usher in a prolonged period of economic hardship, exacerbating existing disparities in wealth and in adolescent race-related stress, trauma and associated mental health problems.
Thus, it is critical that we understand the influences of these race-related stressors on adolescent EBH, as well as potential protective factors such as CC, to develop programmes and policies that support adolescent thriving now and into adulthood. CC is theorised to be a “developmental competency that may promote thriving for children and adolescents, particularly those experiencing marginalizing systems” (p.547).21 However, no studies to our knowledge have explicitly tested CC as a protective factor that can reduce the harmful impact of race-based stress. Although we hypothesise that for most youth, CC will be protective, there is the possibility that for some youth higher levels of CC, particularly CC knowledge, may lead to more mental distress, as youth may feel overwhelmed by a perceived burden of responsibility to change ‘the system’. The proposed study will be unique in its 4 year longitudinal assessments of race-related stress, CC and EBH for Black, Latinx and White youth and its rigorous assessment of protective effects of CC, as well as examining moderators that may reveal for which youth CC is protective vs distressing.
If found to be protective against these stressors, CC holds exciting potential for benefiting adolescent health. Interventions and policies that enhance youth CC may prove instrumental in empowering Black and Latinx adolescents, promoting adolescent health equity, and, ultimately, helping to dismantle oppressive social systems. The proposed research will advance theory and research regarding race-related stress, CC and adolescent development, as well as inform public health practice and policy related to an important and growing segment of the US population. Findings from this study will help shape long-term, sustainable public health practices and policies to support adolescent mental health equity.
Limitations and strengths
Like most observational studies, our study will not use a random sample of youth, and the results will not be weighted to represent Baltimore or national adolescent populations. However, our relatively large sample size and attempts to recruit young people across a range of city settings and networks will enhance the study’s capacity to illustrate developmental trends and themes. We acknowledge that while our study is focused on Black, Latinx and White youth, there are many other racial/ethnic groups that experience racism that are not part of this study (eg, Asian and Native youth). In addition, the subset of participants recruited from our prior Project POWER sample may differ significantly from new participants, further expanding the range of youth included in our sample. Our inclusion criteria for RISE Baltimore are largely the same as those for Project POWER so that combining these groups is simple and justified. Further, we plan to conduct sensitivity analyses to assess potential differences between the samples and will control for Project POWER participation. Of note, approximately half of Project POWER participants were randomised to a trauma-informed intervention during the fall of their eighth grade year, which may influence their EBH over time above and beyond other factors assessed in the present study. To address possible intervention effects, we will control for intervention arm assignment in analyses.
The study also has several important strengths. First, both quantitative and qualitative data will be gathered over a 4 year period when participants are becoming young adults, providing insights into an important developmental transition with implications for adult EBH. Second, our collection of survey data at eight assessment points across the study will enable examination of trajectories of Black, Latinx and White youth. Third, the study’s rigor and potential to advance the field are enhanced by the recruitment of a racially and ethnically diverse adolescent sample, mixed methods with sequential explanatory analyses and the assessment of three domains of emotional and behavioural functioning, including emotional well-being. Finally, partnership with youth-serving community agencies and guidance and implementation support from a study YAB comprised of young people increases our capacity to engage the adolescent population and represent their perspectives authentically.
In summary, this study will lay a foundation for future development of actionable policy and intervention strategies that not only improve mental health and well-being for marginalised adolescents but also address the structural barriers that create disproportionate stress and trauma for them in the first place. Our mixed-methods approach will enable an in-depth look at which stressors associated with racism most negatively impact Black and Latinx youth. These data can inform policies and practices that dismantle those aspects of oppression (eg, harmful police interactions). Our data will also provide insights into how adolescents engage in CC and social justice activism and how this engagement may benefit them. If study findings suggest CC is a protective factor, an intervention that promotes CC can be developed or adapted and rigorously evaluated, considering what we have learnt about for whom CC is protective and under what conditions. Findings may suggest ways to optimise and evaluate existing approaches being implemented by grassroot organisations that train young people to be community leaders and advocates. While it is not the responsibility of young people to solve social problems they did not create, young leaders can play an important role in dismantling structural oppression and improving conditions for other young people. We see strong potential to translate the longitudinal data collected in this study into practice-based solutions for promoting youth mental health equity.
Ethics and dissemination
Study procedures were approved by the Johns Hopkins Bloomberg School of Public Health Institutional Review Board (#00017850). Findings will be disseminated through publications in peer-reviewed journals and presentations at academic conferences. We will also communicate with study participants to share research findings and will explore ways to disseminate findings to the Baltimore community, such as developing a brief to be shared by the Baltimore City Health Department and/or hosting a town hall meeting for Baltimore families.
Ethics statements
Patient consent for publication
Acknowledgments
We thank Steven Sheridan who provided extensive data management and questionnaire design support. We also thank Krishna Johnson and Melinda Scott for their assistance in formatting and editing the final version of the manuscript.
References
Footnotes
X @renee_m_johnson
LKC and TM contributed equally.
Contributors LKC is the guarantor for this manuscript. LKC and TM developed the study design, manuscript draft and procured funding. RW conducted foundational research on critical consciousness and helped shape our thinking about the construct and its measurement. MGV and JH, our community partners, helped inform our approach to including youth voices through a Youth Advisory Board. LKC, TM, RW, MGV, DJ, JH, LW, RM, RMJ, DS and MJ contributed to the study design, protocol development and selection and refinement of measures. All authors approved the final manuscript.
Funding Research reported is supported by Eunice Kennedy Shriver National Institute of Child Health and Human Development of the National Institutes of Health under award number R01HD106654 (MPI: LKC/TM). The content is solely the responsibility of the authors and does not represent the official views of the National Institutes of Health or the National Center for Health Statistics.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, conduct, reporting or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; peer reviewed for ethical and funding approval prior to submission.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.