Article Text

Abstract
Objective To investigate whether prophylactic nebulised antibiotic inhalation reduces the incidence of ventilator-associated pneumonia (VAP) in critically ill adults undergoing mechanical ventilation.
Study design Systematic review and meta-analysis of randomised controlled trials.
Data sources PubMed, Embase and the Cochrane Central Register of Controlled Trials were searched from inception to 1 January 2024 without language restrictions.
Eligibility criteria for selecting studies We included randomised controlled trials comparing prophylactic nebulised antibiotics with placebo or no treatment in mechanically ventilated adult intensive care unit (ICU) patients. Two independent reviewers conducted data extraction and assessed risk of bias. A meta-analysis was performed using random-effects models to calculate relative risks (RRs) for VAP and secondary outcomes.
Results Of the 2663 studies screened, four were deemed suitable for analysis, involving a total of 1160 patients (574 receiving prophylactic antibiotics via nebulised inhalation). Nebulised antibiotics reduced the incidence of VAP compared with control (RR 0.70, 95% CI 0.52 to 0.93, I²=38%, low-certainty). There were no statistically significant differences in ICU mortality (RR 0.89, 95% CI 0.73 to 1.09, I²=0%, low-certainty, moderate-certainty) or hospital mortality (RR 0.93, 95% CI 0.78 to 1.11, I²=0%, moderate-certainty). Risk of bias varied across studies, with one trial assessed as high risk, one with some concerns and two with low risk.
Conclusions Nebulised prophylactic antibiotics may reduce the incidence of VAP in critically ill patients receiving mechanical ventilation, though secondary outcomes did not differ between the intervention and control groups. The findings should be interpreted with caution due to the small number of included trials and low certainty of evidence.
PROSPERO registration number CRD42024496276.
- Infection control
- Adult intensive & critical care
- Meta-Analysis
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. All data are in the manuscript and supporting information files.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This systematic review and meta-analysis included only randomised controlled trials.
A rigorous systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, ensuring methodological transparency and reproducibility.
Variations in antibiotic types, dosages and nebuliser devices across trials may have introduced heterogeneity that limits generalisability.
The certainty and generalisability of the findings are limited by the dominance of a single large randomised controlled trial in the pooled analysis.
Introduction
Ventilator-associated pneumonia (VAP) is the most common type of hospital-acquired infection affecting the lower respiratory tract and is recognised as the leading nosocomial infection globally. This condition primarily affects patients receiving invasive mechanical ventilation in intensive care units (ICUs).1 Studies indicated that VAP affects approximately 5% to 40% of critically ill patients2 3 and carries a substantial economic burden.4–6 Consequently, the prevention of VAP is of utmost importance.
Preventive application of antibiotics to the tracheobronchial tree is a preventive approach to decrease VAP.7 Nebulised antibiotic inhalation is an innovative treatment modality that enables the delivery of concentrated antibiotics to the tracheobronchial tree, lung tissue and tracheal tube biofilm.8 However, the use of preventive antibiotics may contribute to the emergence of multidrug-resistant organisms and may cause adverse events, such as nephrotoxicity and bronchospasm.
A meta-analysis9 conducted in 2018 revealed that the use of preventive antibiotics administered through the respiratory tract can reduce the incidence of VAP. However, the majority of patients (73% (845/1158)) included in these pooled analyses received treatment before 2000, using antibiotics via intratracheal instillation, a modality that has been abandoned in recent randomised controlled trials and clinic settings.10–12 Hence, it may have reflected earlier experiences with VAP prevention. Additionally, the study was limited by its inclusion of non-randomised controlled trials10 and small sample sizes. A new trial with the largest number of participants on this topic has recently been available. In light of this, we conducted a systematic review and meta-analysis to evaluate the effect of nebulised inhalation of antibiotics as a current modality of administration in preventing VAP in critically ill patients undergoing mechanical ventilation in the ICU.
Methods
Protocol and guidance
The present study adhered to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines,13 which are widely recognised as a framework for reporting systematic reviews and meta-analyses. Before starting the study, we prospectively registered the research protocol with the International Prospective Register of Systematic Reviews (PROSPERO) under the registration number CRD42024496276; URL: https://www.crd.york.ac.uk/prospero/.
Information sources and search strategy
A systematic search was conducted across major electronic databases, including the Cochrane Central Register of Controlled Trials, PubMed and Embase. The search aimed to retrieve relevant studies for this meta-analysis and included articles published from the inception of these databases until 1 January 2024. By including studies from a wide range of databases and considering articles published up until the specified date, we aimed to ensure a comprehensive and up-to-date review of the available literature. No language restrictions were imposed during the search process to minimise bias based on language. The comprehensive search terms employed in each database are outlined in online supplemental table S1 of the Data Supplement.
Supplemental material
Selection criteria
Studies were included if they (1) enrolled critically ill patients requiring mechanical ventilation for more than 48 hours in the ICU,2 compared nebulised inhalation of antibiotics with no treatment or placebo,3 provided clear details about the antibiotics used,4 reported outcomes of interest, including the incidence of VAP, mortality and others,5 and were randomised controlled trials (including individually randomised trials, cluster randomised trials, quasi-randomised trials). Studies were excluded if they were cross-over randomised trials.
Outcomes
The primary outcome was the first episode of ventilator-associated pneumonia, as adjudicated from the time of randomisation. Secondary outcome measures included ICU and hospital mortality, adverse events, the incidence of ventilator-associated pneumonia associated to multidrug-resistant pathogen, duration of mechanical ventilation (in days), length of stay in the ICU (in days) and length of stay in the hospital (in days).
Study selection
Two independent reviewers, XY and SZ, screened the titles and abstracts identified through the systematic search. Following this initial screening, the selected articles underwent a full-text review conducted by the same two reviewers. Any disagreements that arose during this process were resolved through discussions between the two reviewers to reach a consensus, minimising bias. If a consensus could not be reached, a third reviewer, YZ, was appointed as an adjudicator to make the final decision.
Data extraction
Two independent reviewers, XY and SZ, extracted relevant data from the selected trials. The data extraction process focused on important characteristics, such as study population, study design, sample size, average age and specific interventions used. In addition, a third expert reviewer, YZ, meticulously cross-validated the extracted data to ensure accuracy and identify any potential errors or discrepancies. This rigorous validation process was conducted to improve the accuracy and reliability of the collected data. In the event of any disagreements among the reviewers, a comprehensive discussion was conducted to reach a consensus.
Assessment of risk of bias
Two independent reviewers, XY and SZ, adhered to the guidelines outlined in the Cochrane Risk of Bias tool.14 This tool assesses bias in seven domains, allowing for a comprehensive evaluation. In each trial, each domain was assigned a study-level score indicating the level of bias risk, categorised as low, high or unclear. This systematic approach ensures a thorough assessment of potential sources of bias in the trials included. In cases where disagreements arose between the two independent reviewers, a thorough discussion was held to resolve them. If a consensus could not be reached, a third reviewer, YZ, was appointed as an adjudicator to make the final decision.
Confidence of evidence
Two independent reviewers, XY and SZ, conducted a systematic assessment using the Grading of Recommendation, Assessment, Development, and Evaluation (GRADE) methodology.15 The GRADE methodology evaluates various aspects of included trials, such as study design, risk of bias, inconsistency, imprecision and indirectness. Subsequently, the evidence was classified into four levels: high, moderate, low or very low, based on these criteria. Disagreements between reviewers were resolved by discussion. If a consensus could not be reached, a third reviewer, YZ, was appointed as an adjudicator to make the final decision.
Data analysis
The statistical analysis of the data adhered to established meta-analysis standards and was conducted using Review Manager (version 5.3, The Cochrane Collaboration) and Stata. For dichotomous outcomes, we calculated the relative risk (RR) along with a 95% CI. For continuous outcomes, we used the mean difference (MD) to summarise the results. Statistical significance was defined as a p value of less than 0.05. This analytical approach followed recognised guidelines to ensure the accuracy and validity of the findings. To assess heterogeneity among the included studies, we employed the I² estimate,16 which quantifies the percentage of total variation attributed to heterogeneity. Heterogeneity is considered acceptable when I² is less than 50%, small when I² is less than 25%, moderate when I² is between 25% and 50%, high when I² is between 50% and 75% and extremely high when I² exceeds 75%. Additionally, random-effects models were used to enhance the reliability and robustness of the results, as this approach accounts for potential variations across studies and provides a more conservative estimate. Potential publication bias was assessed using both visual inspection of funnel plots and statistical tests, including Egger’s17 and Harbord’s18 tests for detecting small study effects. By adhering to these rigorous statistical methods and principles, we aimed to deliver a comprehensive and robust analysis of the available data.
Sensitivity analysis
To assess the robustness of our findings, we conducted sensitivity analyses using: (1) a fixed-effect model, (2) exclusion of high-risk and (3) leave-one-out analysis to evaluate the influence of individual studies.
Subgroup analysis
To achieve a more comprehensive understanding of the potential heterogeneity in the effect of nebulised inhalation of antibiotics on preventing VAP in critically ill patients, we conducted subgroup analysis on the primary outcome based on the following criteria: (1) mean age, (2) antibiotic variety, (3) nebuliser type and (4) length of antibiotic usage.
Trial sequential analysis
We conducted a trial sequential analysis19 (TSA 0.9Beta) in order to mitigate the possibility of type I error and uphold the credibility of our results. This approach encompassed combining the calculation of information size with a modified threshold for statistical significance. In order to uphold a 5% overall risk of type I error and attain 80% power, we carried out a two-sided trial sequential analysis. Our objective was to detect a 20% decrease in RR for our primary outcome.
Patient and public involvement
Patients and members of the public were not involved in the design, conduct, analysis or reporting of this research.
Results
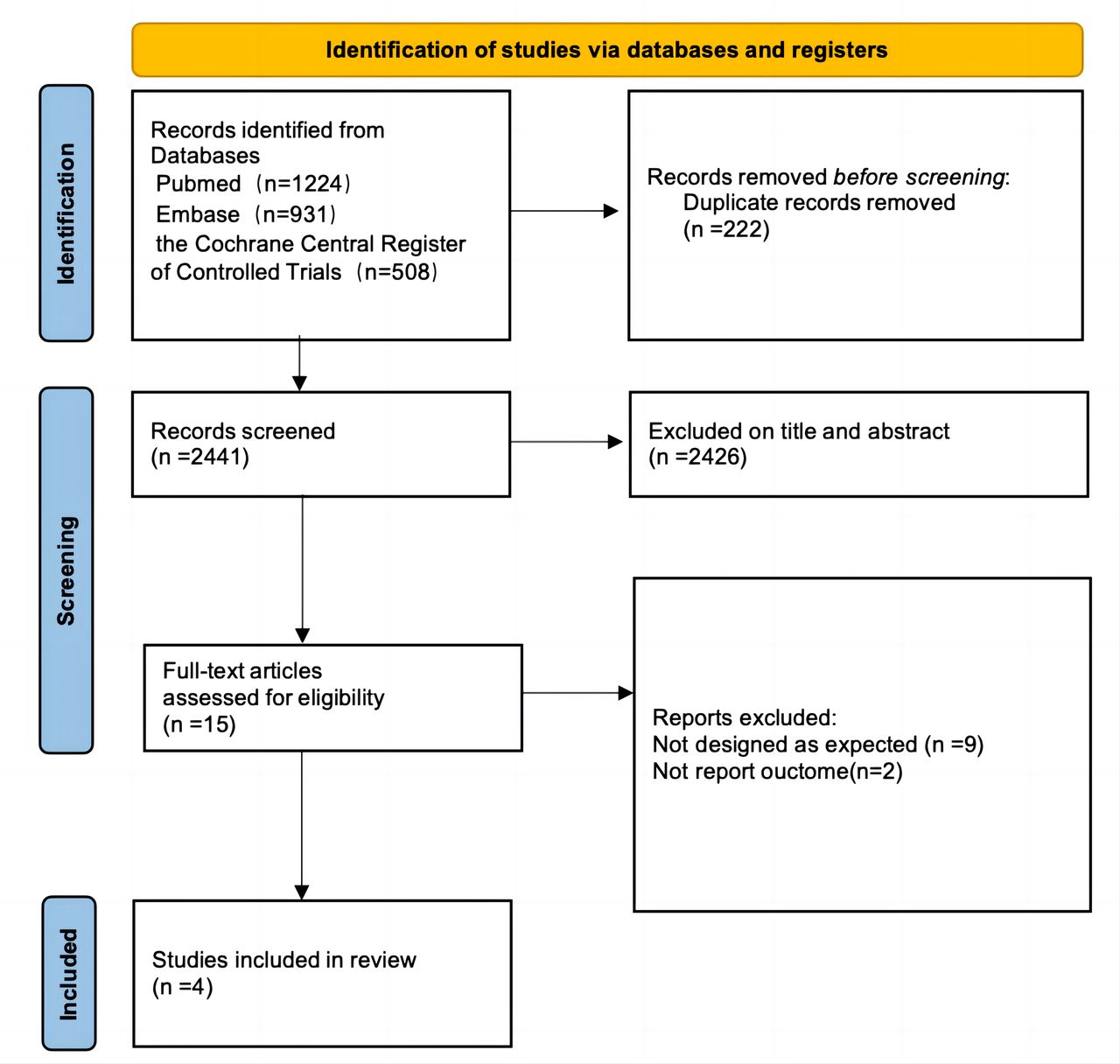
Our initial literature search yielded a total of 2663 articles. After removing duplicates, we screened 2441 unique articles. Following a thorough evaluation of titles, abstracts and full texts, we identified four trials20–23 that met the inclusion criteria for this systematic review (figure 1).

Search strategy and final included and excluded studies.
Table 1 summarises the characteristics of each trial included in this analysis. Ceftazidime was the most frequently used nebulised antibiotic, employed in two studies, while colistin and amikacin were used in the other two. These trials were published between 2002 and 2023, with sample sizes ranging from 40 to 847 patients. Online supplemental table S4 provides the definition of VAP in these studies.
Characteristics of studies included in the meta-analysis
Among the 574 patients who received nebulised antibiotics, 108 (18.8%) experienced the first incidence of VAP, compared with 159 (27.1%) of the 586 patients in the placebo group. This suggests that the use of nebulised antibiotics may reduce the risk of VAP in patients on mechanical ventilation (RR 0.70, 95% CI 0.52 to 0.93, I²=38%, low-certainty) (figure 2). No significant differences were observed between the nebulised antibiotics group and the placebo or no treatment group in terms of ICU mortality (RR 0.89, 95% CI 0.73 to 1.01, I²=0%, moderate-certainty), hospital mortality (RR 0.93, 95% CI 0.78 to 1.11, I²=0%, moderate-certainty), adverse events (RR 1.71, 95% CI 0.47 to 6.23, I²=61%, low-certainty), the incidence of ventilator-associated pneumonia associated to multidrug-resistant pathogen (RR 0.86, 95% CI 0.48 to 1.52, I²=60%, low-certainty), the total duration of mechanical ventilation (MD 0.33, 95% CI −0.51 to 1.16, I²=0%, moderate-certainty), length of hospital stay (MD 0.07, 95% CI −0.93 to 1.08, I²=0%, moderate-certainty) and length of ICU stay (MD 0.25, 95% CI −1.81 to 2.31, I²=0%, moderate-certainty) (figure 3).

Forest plots of the effect of nebulised inhalation prophylactic antibiotics, compared with placebo, on the incidence of ventilator-associated pneumonia.

Forest plots of the effect of nebulised inhalation prophylactic antibiotics, compared with placebo, of secondary outcomes.
The subgroup analysis revealed that none of the following factors significantly contributed to the observed heterogeneity: mean age (≤60 years vs. >60 years, P for interaction=0.97), antibiotic variety (ceftazidime vs colistin vs amikacin, P for interaction=0.83), nebuliser type (jet nebuliser vs vibrating mesh nebuliser, P for interaction=0.97) and length of antibiotic usage (≤7 days vs. >7 days, P for interaction=0.45) (figure 4).

Subgroup analyses of the association between nebulised inhalation of antibiotics and ventilator-associated pneumonia.
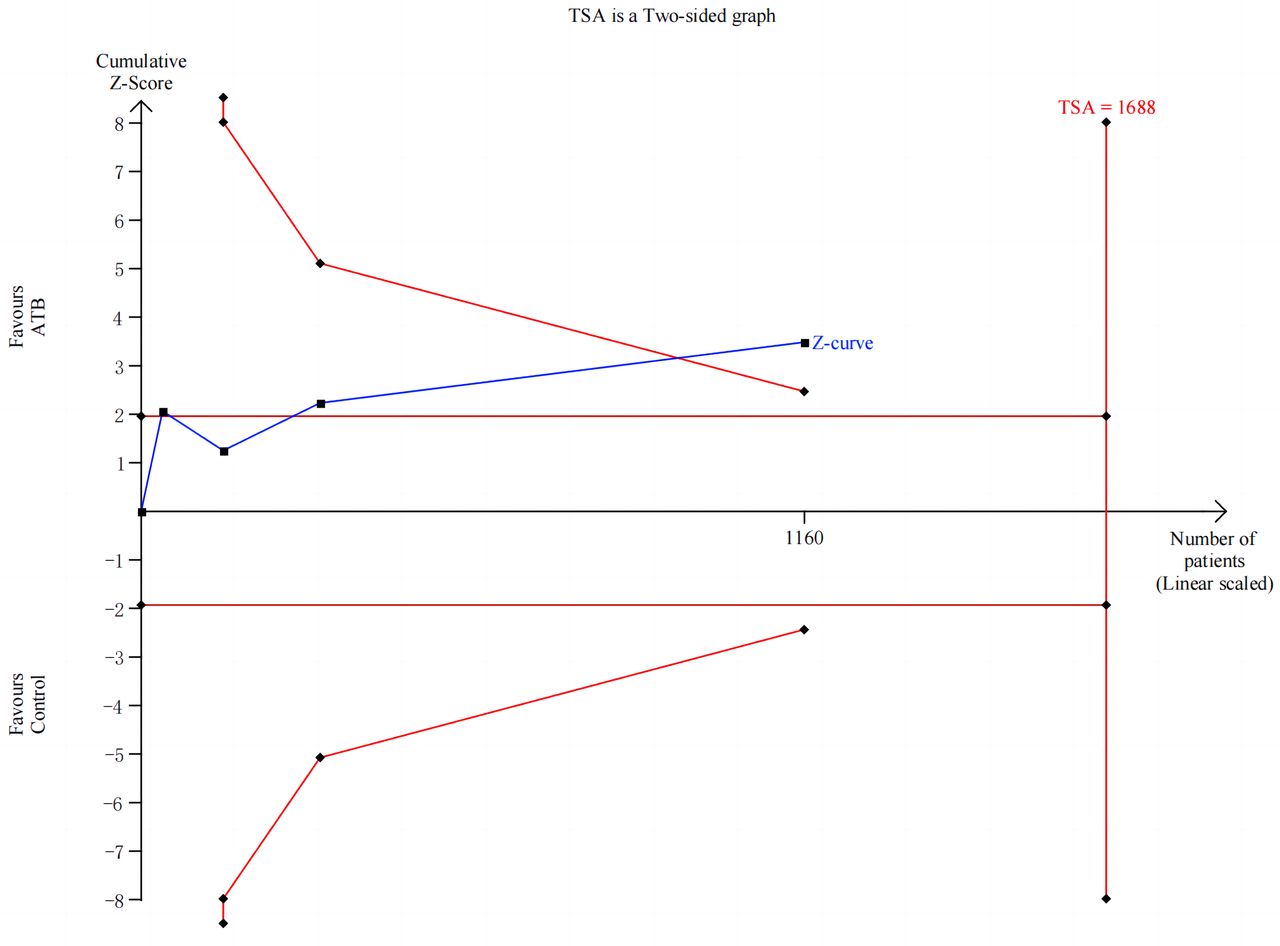
Egger’s test (p=0.51) and Harbord’s test (p=0.53) did not indicate any significant small study effects, and visual assessment of the funnel plot similarly demonstrated no marked asymmetry (online supplemental figure S2). Furthermore, the trial sequential analysis of the primary outcome revealed that, despite the actual sample size not reaching the anticipated level, the cumulative Z-value surpassed the targeted threshold for sequential analysis, indicating that the minimum information size criterion was satisfied (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Trial sequential analysis of the incidence of ventilator-associated pneumonia.
Sensitivity analyses demonstrated significant instability in pooled estimates when excluding individual studies (online supplemental figure S2). Although the primary analysis indicated a statistically significant reduction in VAP incidence (RR 0.70, 95% CI 0.52 to 0.93, I²=38%), this finding proved fragile to the removal of specific trials. These inconsistencies led to a GRADE downgrade from moderate to low-certainty evidence due to critical susceptibility to study selection.
Online supplemental figure S1 in the Data Supplement presents the risk-of-bias assessments. Two trials20 21 had low-risk of bias. One trial had some concerns,23 primarily due to the lack of description of the blinding method. Another trial22 had high-risk, primarily due to its use of an open-label design. The quality of evidence for the primary outcome, as assessed by GRADE, was deemed low (online supplemental table S3).
Discussion
This meta-analysis, which included a total of 1160 participants from four trials, indicated that nebulised inhalation of antibiotics was associated with a favourable outcome in reducing the incidence of VAP in mechanically ventilated patients. Conversely, no disparities were observed in ICU and hospital mortality, adverse events, duration of mechanical ventilation, length of stay in the ICU and length of stay in the hospital.
Previous meta-analysis9 similar to our study, it similarly concluded that prophylactic antibiotics administered through the respiratory tract reduce the occurrence of VAP. However, our methodologies differ. First, the previous meta-analysis9 included intratracheal instillation as an inhalation approach for antibiotics, a modality that has since been abandoned in recent randomised controlled trials and clinical settings. In contrast, our analysis focuses exclusively on the nebulised inhalation of antibiotics. Second, unlike the previous meta-analysis,9 which included non-randomised controlled trial (Rouby et al10), we specifically included randomised controlled trials to enhance the reliability and credibility of our findings. Third, our study incorporated a significant trial that accounted for 73% (847/1160) of the sample patient population. These additional data strengthened our conclusions, improved the precision of our findings regarding the treatment effects of nebulised antibiotic inhalation and satisfied the minimum information size criterion in the trial sequential analysis.
The efficacy of nebulised inhalation antibiotics in preventing VAP can be attributed to several factors. First, nebulised antibiotics deliver medication directly to the lungs, increasing local concentrations and enhancing efficacy in preventing respiratory infections.8 Second, this mode of administration has the potential to decrease the development of antibiotic resistance and enhance synergy with local immune responses, highlighting its advantages.24–26 Third, the protective effect of antibiotics administered via the respiratory tract can also be ascribed to their ability to treat pneumonia in its early stages, as experimental models have shown that nebulising antibiotics during the initial stages of infection effectively reduces lung bacterial load and alleviates the severity of inflammatory lesions.27–29
Pharmacokinetic factors may have influenced the efficacy of nebulised antibiotics across included trials. In particular, the use of jet nebulisers, lower dosages or shorter durations of administration may have limited pulmonary drug deposition. Jet nebulisers are less efficient than vibrating mesh nebulisers, which produce finer particles and achieve better lung deposition. For instance, a study demonstrated that pulmonary aerosol deposition was six times higher with a vibrating-mesh nebuliser compared with a jet nebuliser (34.1% vs 5.2%, p<0.001).30 Furthermore, the presence of antibiotic-degrading enzymes in bronchial secretions could reduce local efficacy unless higher doses or more efficient delivery systems—such as vibrating mesh nebulisers—are employed. These factors warrant consideration in future clinical trial designs and clinical application.
In theory, the administration of antibiotic prophylaxis should result in a reduction in mortality due to its effectiveness in decreasing the incidence of VAP. However, our study indicated that nebulised antibiotics did not significantly reduce mortality rate. This discrepancy can be attributed to several key factors. First, VAP is a significant contributor to the overall mortality in ICU, but it is not the sole determinant. Other factors, such as sepsis, organ failure and the underlying conditions of patients, play crucial roles. Second, the limited sample sizes and/or the modest reduction in VAP incidence may have resulted in an insignificant impact on mortality. Third, most of the studies included in our analysis primarily focused on the incidence of early-onset VAP, which is typically caused by less virulent microorganisms and contributes less significantly to mortality. Fourth, it is worth considering that the studies included in our analysis may not have fully captured the long-term effects of nebulised antibiotic prophylaxis. While short-term reductions in VAP incidence might not translate into significant mortality reductions, longer-term follow-up could reveal more substantial benefits, particularly if the intervention successfully prevents VAP episodes or reduces the overall burden of infectious complications in critically ill patients.
The emergence of multidrug-resistant pathogens poses a significant challenge in the realm of antibiotic prophylaxis. However, our findings indicate that nebulised antibiotic administration does not appear to be associated with an increased incidence of VAP caused by multidrug-resistant pathogens. This may be attributed to the direct administration of antibiotics to the respiratory tract via nebulisation, which bypasses the gastrointestinal tract and reduces systemic exposure. This approach potentially minimises the selective pressure for antibiotic resistance, in contrast to intravenous administration, such as the strategy of administering intravenous cefuroxime to prevent VAP in trauma patients, which may lead to higher systemic concentrations and increased selective pressure.
Several significant limitations must be considered. First, only four studies were included in our analysis. The limited number of studies diminishes the statistical power to detect significant effects, thereby increasing the likelihood of type II errors. This constraint also results in wider confidence intervals, potentially undermining the robustness and validity of the findings. Second, our analysis is primarily shaped by the randomised controlled trials conducted by Ehrmann et al,21 given the large patient cohorts they possessed. Although TSA indicated that the required information size was achieved, the conclusion is largely driven by this single large-scale trial. This reliance may compromise the generalisability of the findings and highlights the need for additional high-quality RCTs to replicate and validate these results across different ICU populations and clinical contexts. Third, the included studies exhibited heterogeneity in terms of the antibiotic regimens used, which may have contributed to variations in the observed treatment effects across the studies. Moreover, the various underlying diseases of patients recruited in included studies may be another confounding factor. Fourth, the included studies present varying definitions of VAP, it complicates the comparison of results. Fifth, the primary outcome did not achieve the anticipated grade of evidentiary quality. Excluding trial assessed as having a high-risk altered the direction of the combined effect, consequently lowering the evidentiary quality of the primary outcome in our GRADE assessment. Sixth, our meta-analysis does not provide sufficient evidence to demonstrate a statistically significant difference in mortality between the trial group receiving nebulised antibiotics and the control group. As a result, the overall evidence base remains limited.
Conclusion
Nebulised prophylactic antibiotics may reduce the incidence of ventilator-associated pneumonia in critically ill patients receiving mechanical ventilation, though secondary outcomes did not differ between the intervention and control groups.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. All data are in the manuscript and supporting information files.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Footnotes
XY, YF and JW contributed equally.
Contributors YZ was responsible for the overall content as a guarantor; study concept: YZ; design: all authors; acquisition, analysis or interpretation of data: XY, SZ, YF, JW, QB, YS, YD, YS, XJ, QL and XC; statistical analysis: XY and SZ; drafting of the manuscript: XY, YF, SZ and JW; critical revision of the manuscript for important intellectual content: all authors.
Funding This work is supported by National Natural Science Foundation of China(82271364), the innovation team project of Affiliated Hospital of Clinical Medicine College of Chengdu University (CDFYCX202203), and the project of Sichuan Science and Technology Bureau (22ZDYF0798), the 1·3·5 project for disciplines of excellence-Clinical Research Incubation Project, West China Hospital, Sichuan University (21HXFH046), the project of health commission of Sichuan province (2019HR50), Experimental Teaching Research and Reform Project of Chengdu University(cdsyjg2022022), and Science and Technology Research Program of Chongging Municipal Education Commission(KJQN202200452).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.