Article Text

Abstract
Introduction Current clinical practice in bariatric surgery follow-up care is highly heterogeneous, and patients have reported needing more and extended personalised support. Especially, they want more support on how to self-manage and cope with the changes and challenges of living with the chronic aspects of obesity and a changing body following surgery. The overall aim of this study protocol is to develop and validate a digital self-management support checklist in bariatric surgery aftercare.
Methods We propose a protocol for a modified, electronic Delphi study design using qualitative and quantitative methods to develop and validate the content of the checklist. The study is divided into two phases: (1) generation of candidate checklist attributes and (2) validation of candidate checklist attributes. In Phase 1, two qualitative studies involving individual interviews with patients and focus groups with healthcare professionals will be conducted to derive context-specific knowledge. This knowledge will be combined with best-practice evidence and stakeholder input to generate candidate checklist attributes, that is, principles, items and features. In Phase 2, a two-round electronic Delphi survey with an expert panel will be conducted to assess the relevance, comprehensibility and comprehensiveness of candidate checklist attributes and to determine the final checklist attributes based on content validity results from the Delphi process. Reflexive thematic analysis will be used on qualitative data and descriptive statistics on quantitative data.
Ethics and dissemination The study has been approved by the Regional Committee for Medical and Health Research Ethics, Region West (2023/676367). The Data Protection Officer at Førde Hospital Trust and collaborating hospital trusts have approved the project (4386–4386). The results will be presented at scientific conferences, published and open-accessed in international peer-reviewed journals.
- Self-Management
- Bariatric Surgery
- Obesity
- Delphi Technique
- Chronic Disease
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study will combine best practice-evidence, context-specific knowledge and expert opinions to develop a digital self-management support checklist, seeking to contribute to a more systematic and sustainable approach for assessing and guiding individual self-management support in the long term following bariatric surgery.
Key stakeholders are involved in the development of the checklist, which may improve feasibility and utility.
Potential limitations in the literature review may impact the comprehensiveness of the candidate checklist.
Participant bias in the Delphi process may influence the selection of final checklist principles, items and features.
Introduction
In the last 50 years, the prevalence of obesity has nearly tripled in Europe, making obesity the leading risk factor for disability and the fourth leading cause of death in the region.1 Obesity is a chronic, complex disease defined by excessive adiposity that can lead to both physical and psychological health problems.2 It further increases the risk of a range of other chronic diseases such as diabetes type 2, cardiovascular diseases and certain types of cancer.3 Norway has the highest prevalence of obesity among the Nordic countries, with approximately 23% of the adult population being obese.1 This makes obesity one of the major health challenges in Norway today and one of the most expensive chronic diseases, attributing to approximately 98 billion NOK per year in social costs related to healthcare, production loss and disease burden.4
It is acknowledged that obesity should be managed as other chronic diseases when it comes to prevention, diagnosis, treatment and life-long follow-up.5–7 In a recent health delivery framework for obesity management published by the World Health Organization,5 self-management support is presented as the first level of care and an essential component of complementing and strengthening medical and surgical treatment options. Supporting self-management involves a patient-centred, collaborative approach that systematically provides patients with the education and support needed to enhance their knowledge, skills and confidence in managing their long-term condition.8 This involves supporting behavioural change techniques to facilitate necessary lifestyle changes and health-promoting behaviours.8 Additionally, healthcare professionals must aid patients’ development of skills needed to manage their chronic disease’s medical, role and emotional impact, including decision-making, problem-solving, goal setting and taking action based on established goals.8 9
For patients with obesity presenting with weight-related diseases and impaired functional abilities, surgical and endoscopic options (ie, bariatric surgery) are recommended to obtain sustained weight loss and improve obesity-related comorbidities and quality of life.10 However, weight-loss maintenance following bariatric surgery (BS) is, for many, a lifetime task with continuing struggles,11 12 where internal and external factors contribute to the challenges of integrating self-management strategies in daily life routines.13 14 Although patients often experience improvements in several aspects of life following surgery, particularly in terms of their physical health, they may struggle with coping and adapting to the psychosocial and emotional challenges of living with obesity and a changing body, leading to a sense of ambivalence.11 14 Many patients report increased difficulty and a ‘lack of control’ in managing their eating, leading to actual or fear of weight regain and less confidence in managing other areas related to their chronic condition.14 Consequently, lifelong multidisciplinary self-management support tailored to individual needs is recommended following BS, focusing on both psychosocial factors, eating behaviours and remission of weight-related comorbidities, nutrition and physical activity.15 16 Despite these recommendations, patients report the need for more and extended support to self-manage their condition and take responsibility for seeking support when required, especially regarding behavioural and psychosocial issues.17
Identifying and implementing efficient self-management support in obesity management and BS care can be challenging due to the large diversity in interventions and poor sustainability.18–20 In Norway, large geographical diversities in treatment and follow-up exist,21 including variations in the number of outpatient consultations, consultations with general practitioners and percentage of patients receiving lifestyle treatment in rehabilitation institutions. Furthermore, challenges related to capacity and competence in primary care lead to highly variable and often insufficient services to support rehabilitation and lifelong follow-up of these patients.22
Recently, the European Union Horizon project COMPAR-EU, which collated evidence and made recommendations for effective self-management interventions in chronic diseases, presented their results for adults living with obesity.23 Although the certainty of the evidence was low, they recommended monitoring, action-based and emotional-based behavioural techniques and social support rather than usual care for improving weight management and patient-reported outcomes such as self-efficacy, quality of life and coping with disease. They further emphasise the need for patient-centred care that involves a collaborative decision-making process, taking individuals’ preferences, values and needs, availability of resources and other contextual factors into consideration.23 This is supported by a recent systematic review on self-management interventions following BS,24 which presents the need for a patient-centred care approach to enhance treatment adherence and patient satisfaction. This review further highlights technology and eHealth strategies to improve care continuity and patient satisfaction with the BS follow-up care processes.
One model that can contribute to a more personalised approach for BS follow-up care is the stepped care model for self-management support.25 A fundamental principle of this model is that resources are allocated based on patient needs. The stepped care approach has shown benefits in the follow-up of other chronic diseases26 and was recently recommended by the British Obesity and Metabolic Surgery Society for managing psychological aspects in BS.27 Here, the first two steps focus on assessing and triaging patients’ needs, monitoring and promoting health literacy and patient activation through access to online resources. Indeed, research indicates that digital health interventions through online platforms and resources can positively impact behaviour changes and improve psychological and disease outcomes for chronic conditions.28 29 However, current literature on the effectiveness of digital health interventions following BS is limited and inconclusive.30
Given the patients’ reported need for more self-management support following BS and the lack of a common practice for self-management support, it is crucial to determine the specific aspects that need to be assessed to provide appropriate and effective long-term support. In chronic diseases, frameworks in the form of taxonomies and checklists for self-management strategies and support have been developed to guide the design of self-management interventions, assess the comprehensiveness of support given in current practice and better understand and identify patients’ needs and challenges over time.31–33 However, the development of these frameworks is mainly based on patients with cardiovascular diseases, diabetes, cancer and neurological diseases. Although there are similarities in self-management processes across chronic conditions, in-depth knowledge about disease-specific processes is needed to provide suitable self-management support for different patient populations.34 Moreover, the frameworks are developed mainly by and for researchers and healthcare providers, potentially leading to the exclusion of essential aspects and terminology that might be challenging for some patients to understand31 and inappropriate for patients living with obesity.35 In addition, context-specific knowledge is needed to adapt and augment generic frameworks to fit contextual features such as specific needs, priorities, resources and existing delivery models in the proposed context of use.
Despite the recognised need for long-term self-management support after BS, significant knowledge gaps remain. First, there is limited knowledge of how patients use their own intrapersonal resources, as well as support from community, social networks and healthcare services, to develop and maintain self-management capabilities in the long term following BS. Additionally, little is known about healthcare professionals’ perspectives on their role in supporting long-term self-management and how they navigate shared responsibility in follow-up care. Furthermore, while frameworks and checklists for self-management support exist in other chronic diseases, there is insufficient knowledge on how such tools should be specifically structured and tailored for individuals undergoing BS, including which aspects are most relevant to this patient group in sustaining long-term health outcomes. Addressing these gaps is essential for developing more effective, patient-centred approaches to self-management support after BS and ensuring that follow-up care aligns with individuals' long-term needs and challenges.
Aims and objectives
The overall aim of this study is to develop and validate a digital self-management support checklist in BS aftercare.
The checklist will provide a structured, context-specific framework that captures essential aspects of self-management processes and support following BS. By supporting a shared decision-making process, the checklist will empower patients to take an active role in their care. It will complement and enhance existing BS follow-up practices, providing a basis for personalised care and supporting the evidence-based implementation of the initial steps in a stepped-aftercare model for self-management support. In specific, this involves providing a structure to (a) systematically assess individuals’ self-management capabilities and needs, (b) guide the level of care needed to support self-management throughout the care process, (c) monitor and evaluate the impact of self-management strategies and support given, and (d) provide online resources to support individual self-management.
To achieve this, the objectives of the study are
To identify and review best-practice evidence related to self-management processes and support in BS, obesity management and chronic diseases in general.
To explore the experiences and perspectives of BS patients and healthcare professionals to derive context-specific knowledge on self-management processes and support.
To generate candidate checklist attributes, including key principles, items and features, based on best-practice evidence, context-specific knowledge and stakeholder input.
To assess the relevance, comprehensibility and comprehensiveness of candidate checklist attributes among an expert panel through a Delphi process.
To determine final checklist attributes based on content validity results from the Delphi process.
Methods and analysis
The study protocol is informed by (1) the standards for reporting qualitative research (SRQR),36 (2) the ACcurate COnsensus Reporting Document (ACCORD)37 and (3) the COSMIN checklist for evaluating the quality of the development of instruments used in healthcare services.38
Study design
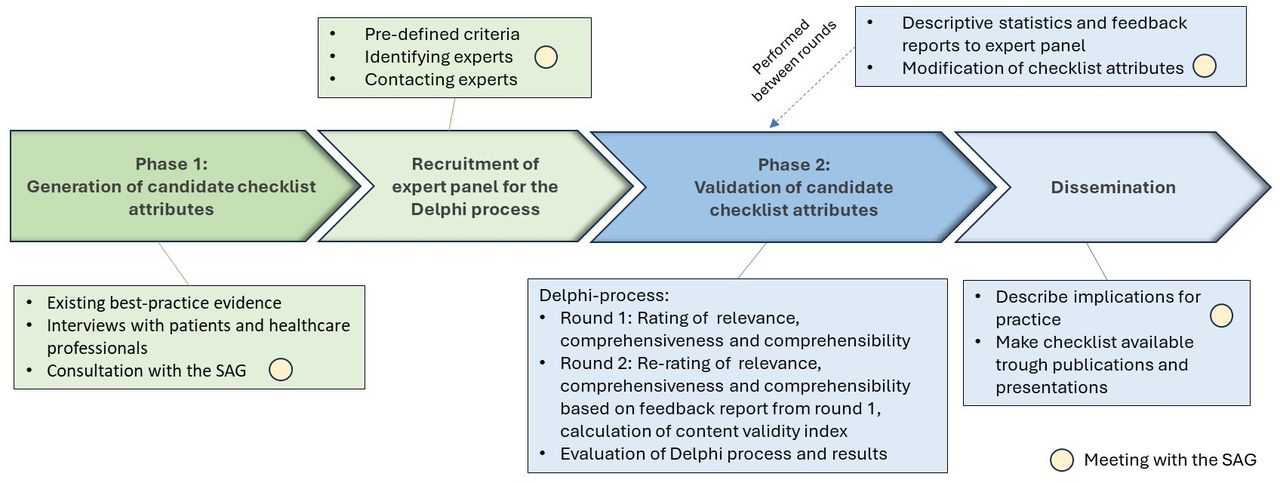
We propose a protocol for a modified, electronic Delphi study design to develop and validate the checklist (figure 1). We chose this design to build a comprehensive understanding of the contextual factors involved in self-management processes and support following BS, as well as to obtain multiple perspectives and validation of these results among essential stakeholders to address the variations in Norwegian BS follow-up care services. The study will be conducted from January 2025 to September 2029 and will be divided into two phases: (1) generation of candidate checklist attributes, including principles (ie, how the digital checklist should be used), items (ie, what the digital checklist should include) and features (ie, what functionality the digital checklist should have) and (2) validation of candidate checklist attributes.

{kind=link}
Modified, electronic Delphi study design for the development of a digital self-management support checklist. SAG, stakeholder advisory group.
The Delphi method is an iterative process for systematic solicitation and collation of individual expert opinions, which aims to explore group agreement and/or achieve consensus on a certain research topic.39 In healthcare, it is a widely used method serving various purposes such as ranking issues by importance, defining a concept and identifying best practices.40 41 By conducting a Delphi survey, we can leverage multiple experiences and perspectives to ensure a comprehensive and consensus-based checklist covering all essential aspects of long-term self-management support for BS patients. Many clinical guidelines and recommendations for treatment and follow-up care after BS are based on collating expert opinions through consensus-based processes.15 27 42
The Delphi method will be modified as initial checklist attributes will be generated based on empirical data from qualitative studies and not an unstructured open first round to collect suggestions from experts.43 The electronic approach eliminates the need for physical meetings, avoids travel costs and reduces geographical constraints.44 A key feature of the Delphi process is participant anonymity, which ensures that individuals’ identities and responses remain confidential from one another.45 This confidentiality reduces conformity pressures from dominant viewpoints and promotes a more genuine exchange of opinions.45
A targeted literature search will be performed to identify and review best-practice evidence related to patient-centred self-management support and follow-up care following BS and in obesity management in general. This involves the search for (a) clinical guidelines and recommendations for self-management support and follow-up care in BS and obesity management in general; (b) systematic reviews on self-management support interventions following BS and in obesity management in general, including eHealth interventions; and (c) generic frameworks for self-management strategies and support in obesity management and chronic diseases in general. This approach ensures that relevant and up-to-date evidence is considered when developing the checklist.
Setting
The study will be conducted in the Norwegian BS follow-up care setting. In Norway, approximately 13 000 patients are scheduled for follow-up care (1, 2, 5 or 10 year follow-up visits) after BS at any given time.46
Our research team includes key Norwegian researchers in obesity, an international researcher and a policy advisor on health management. The team holds expert knowledge on obesity management, health communication, qualitative methodology, service user participation in research and implementation of research and technology into clinical practice.
Patient and public involvement
A stakeholder advisory group (SAG) consolidated by a representative from the national board of the Norwegian Association for Overweight Individuals, an experienced healthcare provider of follow-up care following BS and a prominent researcher on obesity management with a particular focus on life stories, lifestyle changes, primary healthcare measures and coordination between service levels. The SAG has been consulted in the study design process and will be actively involved in developing, modifying and disseminating the checklist. In addition, two engaged service users with extensive experience in self-managing their condition following BS have been recruited as user representatives. These have been asked for advice on the written informed consent, interview guides and recruitment process for the individual interviews with patients. They will be consulted throughout the study when it comes to ethical considerations, interpreting data and conveying results.
Phase 1: generation of candidate checklist attributes
Individual interviews with patients and focus-group interviews with healthcare professionals will be conducted to obtain context-specific knowledge about self-management processes and support in the Norwegian BS care follow-up setting. This insight allows for the adaptation of the checklist to align with the cultural, psychosocial and organisational factors that may influence patients’ self-management processes and support practices in Norwegian BS follow-up care. It may further enhance the relevance and usability of the checklist by incorporating local practice, language and terminology that patients are familiar with, ensuring the checklist aligns with the existing care pathway. Moreover, the data may highlight areas where patients may require support in this specific setting, enabling us to design a checklist that addresses patients’ specific needs and preferences in this context. In addition, a deeper insight into how patients develop and maintain self-management capability in this context allows us to consider factors such as technology accessibility and patient preferences for digital self-management interventions to support these processes.
Recruitment
A maximal variation sampling approach will be used to capture various perspectives and insights. This approach will be combined with a pragmatic selection process, allowing respondents to suggest further interviewees (ie, snowball sampling).47 The estimated sample sizes are guided by the principle of information power48 and available methodological49 and empirical guidance on sample sizes50 for individual interviews and focus groups.
For the individual in-depth interviews, between 12 and 17 patients will be recruited from bariatric outpatient clinics in collaborating hospitals in the western Norway healthcare region. Participants will be purposively sampled for maximum variation across age and gender, time since surgery, education level, marital status, household and employment status. Designated gatekeepers will coordinate recruitment at each collaborating hospital. The criterion for inclusion will be an age above 24 and below 67 years, a minimum 2 year follow-up since BS, having the capability to give informed consent or dissent and communicating in Norwegian in the interviews.
Healthcare professionals will be recruited for four focus-group interviews, with four to eight persons in each focus group. The participants will be purposively sampled for maximum variation across clinical roles and length of work experience within the field. Online focus groups will be conducted if necessary to address any geographical or practical restrictions compromising representativeness.
Data collection
Individual interviews and focus groups will be recorded using a high-quality audio recorder to ensure the most accurate representation of both verbal communication and non-verbal vocal cues, such as the tone and intensity of the voice and pauses and hesitations in speech.51
The interview guides (see online supplemental material) are based on established conceptual frameworks for self-management processes and support.9 52 They have been developed by the research team and further refined through review and feedback from the SAG. The interview guides will provide a structured foundation for each interview and focus group while allowing flexibility to explore participants’ unique perspectives in greater depth. As data analysis progresses, the guides will be continuously refined to ensure a structured yet adaptable approach to exploring participants’ perspectives and experiences.
Supplemental material
Data analysis
Our analysis will be grounded in the constructivist/interpretivist research paradigm.53 The recorded interviews will be transcribed verbatim. Reflexive thematic analysis (RTA), as described by Braun and Clarke,54 will be used to capture the complexity and nuances of patients’ and healthcare professionals’ experiences and perspectives on self-management processes and support following BS.
We will adopt Braun and Clarke’s six-phase approach to thematic analysis to systematically explore our data.55 56 The process will begin with familiarisation with the data through repeated reading of transcripts.56 In the next phase, initial codes will be generated in a fluid and iterative manner.56 Following initial coding, we will use an inductive, data-driven approach to identify patterns across the dataset,55 clustering related codes into preliminary themes. This will be done collaboratively within our research team to enhance reflexivity, challenge assumptions and ensure a richer interpretative depth. The preliminary themes will undergo an iterative process of refinement and will be structured into a thematic map representing key narratives within the data. Finally, themes will be situated and discussed with relevant theoretical frameworks.55
The research team will operationalise findings from the qualitative studies as a list of candidate checklist principles, items and features. Best-practice evidence identified in the literature review will be used to add or modify potential checklist attributes. The SAG will draw on their expertise and experience as clinicians and service users to add any additional attributes and refine the wording and description of each of them to improve clarity. Each attribute will include a description and rationale including sources for generating the attribute (eg, qualitative studies, best-practice evidence and/or expert opinion from the SAG).
Phase 2: validation of candidate checklist attributes
A two-round electronic Delphi survey will be conducted to evaluate candidate checklist attributes’ content validity. Content validity refers to the extent to which the content of an instrument accurately represents the construct it is intended to measure.38 Measuring content validity is a fundamental part of the validation assessment process and essential for determining the quality of new health instruments.57 It ensures that all attributes are relevant, covers all necessary aspects of the construct (ie, comprehensive) and is easy to understand for the intended users (ie, comprehensible). Performing an expert judgement through a Delphi survey is an acknowledged method for systematically assessing and quantifying content validity.40 58 59
Recruitment of expert panel
Establishing an expert panel is a fundamental part of the Delphi method. The panel must include a diverse and comprehensive set of skills, experiences and social abilities relevant to the phenomena of interest.60 Participants in the expert panel will include (1) healthcare professionals in BS follow-up care and (2) service users who have undergone BS (above 24 years old and at least 2 years post-bariatric surgery). We aim to establish a geographically diverse expert panel representing all health regions in Norway, with 15 participants in each expert class. According to the literature, 8 to 23 participants in each expert class will provide sufficient diversity of perspectives.41 The participants will give informed consent upon completion of survey rounds. No extrinsic motivation for participation will be given except from pre-access to survey results.
We will ask leaders of the regional centres/units for obesity management to identify four experts/healthcare professionals in their region who (a) are involved in BS follow-up care, (b) have recognised experience in the field and (c) are interested in participating. We will seek a balance of practitioners working in a university or non-university hospital and variance in age, years of working experience within the field and occupation. Recruitment of service users will be conducted in collaboration with the designated gatekeepers at the BS units in the participating hospitals. In addition, participants recruited in Phase 1 of the study will be invited to participate in the expert panel.
Survey pre-test
A survey pre-test will be conducted on a small group of fellow researchers and representatives of the expert panel to ensure that the survey questionnaire is clear and understandable and that the survey length is less than 30 min to minimise survey fatigue and reduce attrition rate.61
Delphi survey: round one
In the first round, we will collect the expert panel’s initial ratings and narrative comments on candidate checklist attributes’ relevance, comprehensibility and comprehensiveness.
The survey questionnaire will be distributed electronically to each panellist. A concise description of the study’s overall purpose and research objective and an explanation of concepts used in the survey will be provided to establish a thematic understanding and a shared knowledge base among the panellists. Participants will be informed that individual responses will be de-identified and anonymous for other participants, but known for the first author. In addition, necessary instructions for answering the survey will be provided. Participants will be asked to rate the relevance of each candidate checklist attribute using a four-point Likert scale (1, not relevant; 2, somewhat relevant; 3, quite relevant; 4, highly relevant)62 and be encouraged to provide a rationale for their answer by giving a narrative comment. Participants will subsequently be asked to judge the comprehensibility of the checklist’s attributes using a four-point Likert scale from ‘very easy to understand’ to ‘not easy to understand’ and be encouraged to suggest modifications to make the attribute more applicable and/or clear to them. Regarding comprehensiveness, participants will be encouraged to suggest any additional principles, items and/or features they consider essential to completely capture the underlying construct of self-management support following BS. At the end of the survey, participants can provide general comments and feedback on the checklist.
Participants will be given 2 weeks to complete the survey, with a reminder sent after 1 week to those who have not answered. The first author will contact non-responders to inquire whether they are willing and if they have the opportunity to respond within 3 days.
Data analysis and preparation of individual feedback reports for each panellist will be conducted within a maximum of 4 weeks. The individual feedback report will include aggregated group responses in histograms, the panellist’s own individual responses, a synthesis of findings from the narrative comments and an overview of revisions made. The first author will not be blinded to participants’ individual responses to allow for elaboration on unclear responses or comments. Descriptive statistics will be used to analyse the profile information and the ordinal Likert scale data, calculate the frequency and percentage of respondents on each option and calculate the median Likert score for each attribute. RTA will be used to systematically and objectively analyse the open-ended comments.54 The research team will combine and interpret the quantitative results with the findings from the narrative comments to make well-informed decisions about modifying or adding principles, items and/or features to the checklist. This collaborative process will involve working closely with the SAG.
Delphi survey: round two
In the second round, panellists will be asked to re-rate the checklist’s principles, items and features, accompanied by a reminder of which rating option they chose in the first round and the median Likert score for the specific attribute. It will be emphasised that they do not have to change their answer from their original response if they do not wish to do so. If they change their answers, participants will be encouraged to provide a narrative comment explaining the rationale for this change. In the last section, panellists will be encouraged to give a final comment or feedback on the checklist. The analysis and feedback process after the first round will be repeated.
Content validity and finalisation of the checklist
After the re-rating in round two, the relevance of each attribute will be evaluated by calculating the content validity index (I-CVI). The I-CVI will be calculated by dividing the number of panellists rating an attribute as ‘relevant’ or ‘very relevant’ by the total number of participants rating the attribute. Attributes with an I-CVI of >0.78 are relevant59 and will be included in the final checklist. Attributes with an I-CVI between 0.78 and 0.70 need revision59 and will be discussed with the research team and the SAG before being excluded or included in the checklist. Attributes with an I-CVI <0.70 will be eliminated59 from the checklist. To evaluate the total content validity of checklist principles, items and features, the average CVI (S-CVI/Ave) will be calculated by dividing the sum of I-CVIs in each section by the total number of attributes in each section. A S-CVI/Ave of a minimum of 0.80 will be deemed acceptable, while an S-CVI/Ave of 0.90 or above will be considered to reflect excellent content validity.62
Final checklist principles will be used to describe how the digital self-management support checklist can be used to support a stepped aftercare pathway following BS. Items included in the final checklist will be used to assess and monitor individuals’ self-management capabilities and needs and guide the level of support needed. Mapping and collating evidence-based online resources for each final checklist item will be initiated on completion of the Delphi survey. These resources may be publicly available through national health authorities and public health portals or available within healthcare institutions across the country. Engaging key stakeholders, such as healthcare professionals, patient organisations and the regional centres for obesity management, will be crucial in identifying and facilitating access to effective resources. Features included in the final checklist will be forwarded and prioritised in parallel work with the digitalisation of the checklist, adapting already available technology to fit any specific features.
Evaluation of the process and results
The panellists will receive the individual reports from the second round of the Delphi survey, the content validity results and an overview of attributes included in the final checklist. Participants will be asked to answer questions evaluating the Delphi process and the perceived utility of the results. This involves the overall quality and clarity of the presentation of the questions, the degree to which the feedback received between rounds improved their confidence in the answers given, their satisfaction with participation in the study and the usefulness of the results achieved. Results from this evaluation will be included in disseminating the results to allow readers to evaluate the degree of credibility more easily and the perceived usefulness of the resulting self-management support checklist.63
Ethics and dissemination
Written informed consent will be obtained from all participants in the study. Participants can withdraw from the study at any time before publication. The study has been approved by the Regional Committee for Medical and Health Research Ethics, Region West (2023/676367). The Data Protection Officer at Førde Hospital Trust and collaborating hospital trusts have approved the project (4386–4386). The SAG meetings will evaluate ethical considerations regarding any potential adverse consequences of the conduction or results of the project.
Results will be available for clinicians and researchers through open-access international articles in peer-reviewed scientific journals and professional journals. The results will also be presented at national and international conferences within the field of BS and relevant service users forums.
A staged approach for reporting the results will be used. Results from two qualitative studies will be published separately, and the resulting checklist will be presented in a third article, where the building approach from the qualitative data to the candidate checklist attributes will be described together with the results from the Delphi process. The research results will also be published as part of a doctoral work at the Western Norway University of Applied Sciences.
Implications
This project seeks to contribute to a more sustainable and frugal approach to follow-up care after BS, promoting self-management and patient empowerment. User involvement is key to ensure the validity and relevance of the self-management support checklist, aligning it with users’ experiences and needs and the intended context of use.
The checklist can provide a standardised framework for assessing self-management needs, supporting healthcare professionals to efficiently develop personalised self-management support plans and determine the appropriate level of care, both before surgery and in long-term follow-up care. By facilitating tailored access to online evidence-based resources, it can promote autonomy, health literacy and continuity of care. This patient-driven approach can optimise resource allocation and enhance service quality by enabling more targeted interventions and encouraging active user participation in the care process.
Designed to evolve with clinical advancements and emerging evidence, the checklist will be regularly updated to maintain its relevance and accuracy. This ensures an ongoing development of high-quality, evidence-based self-management support while adapting to the changing clinical landscape. By systematically identifying and integrating existing resources, the checklist can drive knowledge translation among healthcare professionals and institutions, reducing duplication and promoting more efficient, coordinated care. Additionally, it can highlight gaps in available resources, guiding the development of new resources to address unmet needs, ultimately improving the quality of aftercare for BS patients.
Ethics statements
Patient consent for publication
Acknowledgments
We thank our collaborating partner, Prof. Jane Ogden, at the University of Surrey, for the valuable discussion on study design and helpful comments on the manuscript. We thank Prof. and research group leader Christian Moltu and the research group for personalised health services (PERSONFORSK) at Førde Hospital Trust for contributing with expert knowledge on practice-oriented research, co-creation with stakeholders and implementing research and technology into clinical practice. We also thank the members of the stakeholder advisory group and the user representatives for their valuable input in the development of this study protocol, particularly in relation to the study design, interview guides, and recruitment strategy.
References
Footnotes
Contributors J-MTØ: corresponding author; conceptualisation; writing – original draft, writing – review and editing. J-MTØ is responsible for the overall content as guarantor. EN: conceptualisation; supervision; writing –review and editing. JRA: conceptualisation; co-supervision, writing –review and editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests As academic researchers, all authors are governed by management plans that transparently deal with potential conflicts of interest.
Patient and public involvement Patients and/or the public were involved in the design, conduct, reporting or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.