Article Text

Abstract
Objectives To compare the analgesic effects of intrathecal neostigmine with bupivacaine, morphine with bupivacaine and bupivacaine alone among patients undergoing surgical procedures below the umbilicus.
Design and setting A multicentre prospective cohort study was conducted from 29 May to 29 August 2023 at Wolaita Sodo University Comprehensive Specialized Hospital, Nigest Mohammed Eleni Memorial Comprehensive Specialized Hospital and Werabe Comprehensive Specialized Hospital. A systematic random sampling technique was used to select the participants from the sample of 180.
Participants The study included American Society of Anesthesiologists classes I and II patients aged 18–85 years scheduled for elective surgeries under spinal anaesthesia with bupivacaine with neostigmine (50 µg), bupivacaine with morphine (100 µg) and bupivacaine alone at a dose of 17.5 mg.
The primary outcome measures The duration of pain relief, the severity of pain and the time of first analgesic requirement.
The secondary outcome measures Postoperative complications such as respiratory depression, pruritus, nausea and vomiting
Results Administration of intrathecal bupivacaine with neostigmine group (NG) and morphine group (MG), respectively, produces a long duration of postoperative analgesia with a first analgesia request mean time of 9.4±3.18 and 9.65±4.9, while using bupivacaine group (BG) alone produces a shorter duration of postoperative analgesia with a mean first analgesia request time of 3.58±0.98 hours. The mean visual analog scale scores in 28 hours were 0.99, 0.79 and 2.05 for the NG, MG and BG, respectively. The overall postoperative pain severity was highest in the BG. The mean total analgesic consumption was 77.5, 73.8 and 189.2 mg for diclofenac, whereas 54.2, 63.9 and 151.7 mg for tramadol in the NG, MG and BG, respectively. Incidence of nausea (31.3%) and vomiting (30%) was highest in the NG, while pruritus (15%) and respiratory depression (15%) were more in the MG.
Conclusion Compared with BG, MG and NG had longer-lasting postoperative analgesic effects, less severe pain and required fewer analgesics overall. Patients in the NG had more incidences of nausea and vomiting. The incidences of pruritus and respiratory depression were highest in the MG. Effective analgesia appeared to work better in the MG and NG. We recommend morphine and neostigmine as adjuvants to local anaesthetics for effective postoperative analgesia. We also recommend researchers compare different doses of neostigmine and morphine as adjuvants to bupivacaine in further studies.
- Pain management
- Trauma
- ACCIDENT & EMERGENCY MEDICINE
- Anaesthesia in obstetrics
- Ethiopia
- Medicine
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THE STUDY
Different surgeons, including consultants and residents, participated in this study; this does not allow for uniformity in terms of surgical skills that can have a direct relationship to the discomfort experienced by the patients.
The presence of confounding factors that may affect our findings.
We did not evaluate the dose-response of individual drugs, which may clearly indicate the role of these drugs in postoperative pain management.
Introduction
Pain is a distressing sensory and emotional experience related to an actual or potential tissue injury after surgery.1 In case it is not treated enough, it can cause shallow breathing, atelectasis, retention of secretions and an increase in the chance of profound venous thrombosis (DVT) and afterwards increase the frequency of postoperative morbidity, leading to postponed recovery and hospital release.2 3 Most of the patients experience more pain after surgery than during surgery and before they are discharged.4 Therefore, postoperative pain management plays a crucial role in determining the overall success of any surgery.5–7 Acute postoperative pain management has received careful attention, and the field has advanced significantly at the same time.8 Despite this progression, postoperative pain continues to be challenging, and if not adequately treated, it can cause persistent uneasiness, stress and dissatisfaction.9
The widely used anaesthetic method for lower abdominal surgical procedures, like those below the umbilicus, is spinal anaesthesia.10 Spinal anaesthesia employing a local anaesthetic (LA) agent separately or in combination with additives is one of the strategies used to control or treat this intense pain.11–13 Administration of bupivacaine, a commonly used local anaesthetic drug, is effective in managing postsurgical patients; however, when bupivacaine is used alone without adjuvants, it has a short duration of action to cover the postoperative pain.5
Opioid adjuvants such as morphine play a great role in enhancing local anaesthetic-induced analgesia, and in addition to bupivacaine, they give intraoperative pain relief and also provide a prolonged analgesic effect.14 However, morphine has the potential for unfavourable impacts such as pruritus, nausea and vomiting, and delayed respiratory depression.7 15 Non-opioid anaesthetics like neostigmine have been used in an effort to create non-opioid pain relief with fewer side effects.12 Efforts at finding the perfect additive drug to local anaesthetic agents to satisfactorily manage acute intraoperative and postoperative pain pose a challenge to anaesthetists.
Neostigmine, an anti-cholinesterase drug that is used to antagonise non-depolarising muscle relaxants, has been tried for postoperative analgesia as an off-label use, and it has been shown that small dosages of neostigmine (50 µg) can improve sensory anaesthesia with few side effects when combined with low-dose bupivacaine spinal anaesthesia.16 It is demonstrated that the addition of neostigmine to bupivacaine reduces postoperative pain, the visual analog scale (VAS) scores and analgesic requirements as compared with bupivacaine alone.11 17 18
Nevertheless, neostigmine intrathecal injection did not significantly raise blood pressure in human clinical trials.12 After receiving neostigmine intrathecally, patients experienced pruritus, nausea and vomiting, and even a small dosage of neostigmine can result in severe, protracted vomiting that is resistant to antiemetic and prokinetic medications.5 19
Despite years of advances in pain management, the mainstay of postoperative pain therapy in many settings is still systemic opioids, which, in the face of their effectiveness, have been associated with respiratory depression, hypoxia and respiratory arrest, which limit their use in pain management.7 15
In Ethiopia, limited studies were available on the analgesic effects of intrathecal bupivacaine with neostigmine or morphine among elective surgical patients. Thus, this study aimed to assess the analgesic effect of intrathecal bupivacaine with neostigmine and with morphine among elective surgical patients in selected comprehensive specialised hospitals in southern Ethiopia.
Methods
Study design, period and settings
A multicentre prospective cohort study was carried out from 29 May to 29 August 2023 at Wolaita Sodo University Comprehensive Specialized Hospital (WSUCSH), Nigest Mohammed Eleni Memorial Comprehensive Specialized Hospital (NMEMCSH) and Werabe Comprehensive Specialized Hospital (WCSH). All the hospitals were included. WSUCSH, which is located in Sodo town, 330 km southwest capital of Ethiopia, Addis Ababa. NMEMCSH is located 232 km southwest of Addis Ababa and WCSH is 170 km, southwest of the capital city, which is Addis Ababa. The study was approved by the Institutional Review Board and registered at the research Registry https://www.researchregistry.com/browse-the-registry%23home/ with the unique identifying number of researchregistry11129.
Study design and period
Source populations
All adult patients who had undergone elective surgery below the umbilicus under spinal anaesthesia with neostigmine, morphine and bupivacaine during the study period at comprehensive specialised hospitals were served as a source population.
The patients were randomly allocated into three groups, each group consisting of 60 patients:
Neostigmine group (NG): atients received 50 µg of neostigmine with 17.5 mg of 0.5% bupivacaine intrathecally.
Morphine group (MG): atients received 100 µg of morphine with 0.5% of 17.5 mg bupivacaine intrathecally.
Bupivacaine group (BG): patients received 17.5 mg of 0.5% bupivacaine alone intrathecally.
Inclusion and exclusion criteria
Inclusion criteria
All adult patients who were in the age group of 18–85 years, classified by the American Society of Anesthesiologists (ASA) as classes I and II and scheduled for elective surgeries under spinal anaesthesia with neostigmine, morphine and bupivacaine at a dose of 17.5 mg during the study period were included.
Exclusion criteria
Patients allergic to the study drugs, refusing to participate in the study, failing spinal anaesthesia, having bleeding disorders, alcoholics, drug addicts, pregnant mothers, psychotics, unconscious or mentally retarded were excluded from the study. In addition, patients on medication like cimetidine, Coartem, clonidine, captopril and Antiretroviral therapy (ART) were also excluded from participating in this study.
Variables
Dependent variables
Time to first analgesia request, pain severity among the groups and total analgesic consumption in 28 hours.
Independent variables
Sociodemographic factors: age, gender, height and weight.
Perioperative factors: ASA physical status, duration of surgery, comorbid illness, and the type of surgical procedure.
Sample size determination
The sample size was determined by using G*Power V.3.1.9.4 software, and the mean difference between the two independent groups is taken from a previous study done in India on the topic of intrathecal bupivacaine with neostigmine or MgSo4, for postoperative analgesia after major gynaecologic surgery.12 Using G*Power V.3.1.9.4 software, the calculated effect size is 0.5189421, α=0.05 and power (1–β) = 80%. The computed sample size was 180.
Sampling technique
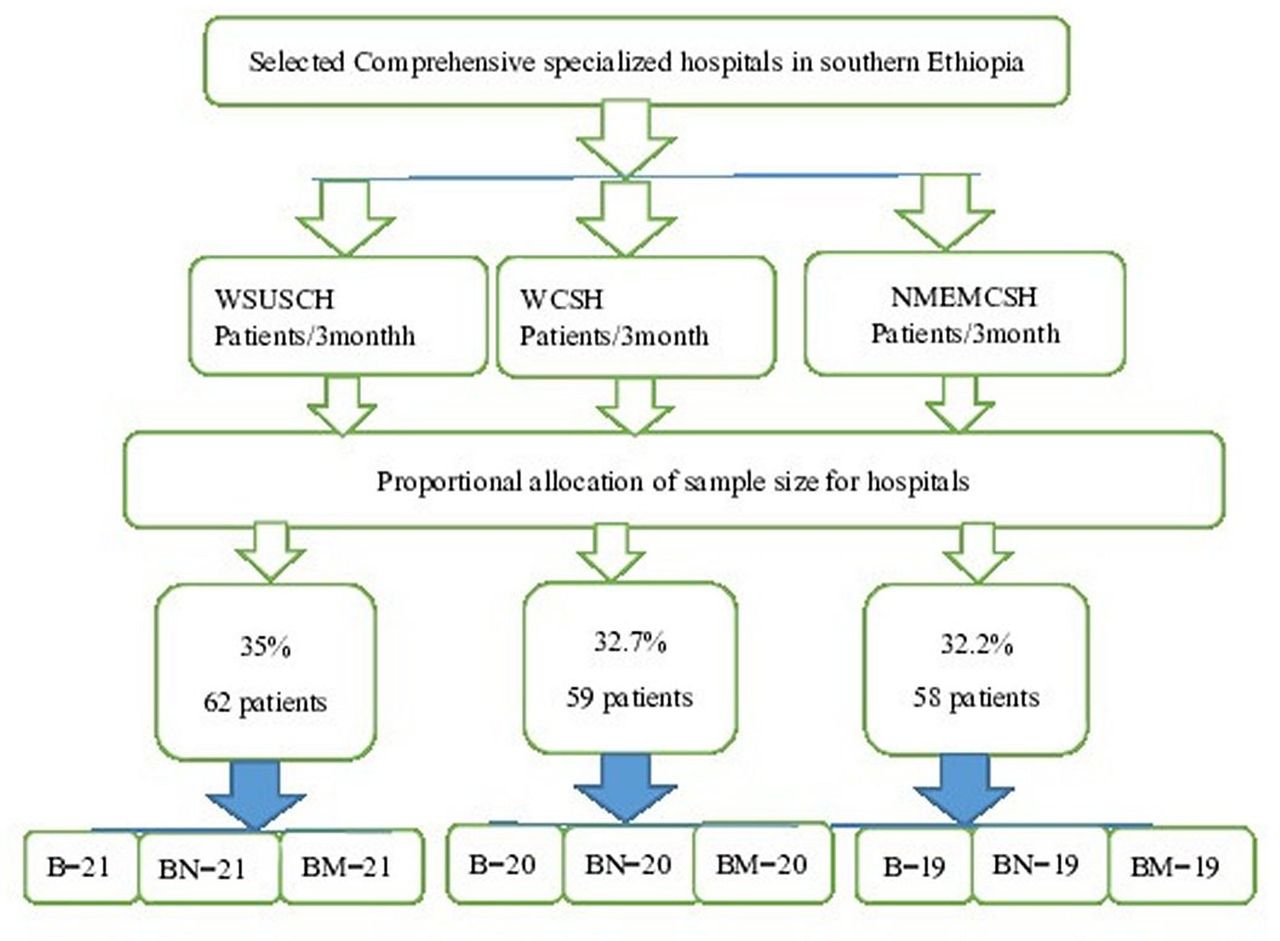
All three hospitals, namely WSUCSH, NMEMCSH and WCSH, were included in this study. From the situational analyses of the postoperative patient logbook of these hospitals, 430 patients were operated on under spinal anaesthesia within 3 months (29 May to 29 August 2023). Then, patients who underwent operations under SA were proportionally allocated for each comprehensive hospital from the logbook record in the 3-month situational analysis (ie, WSUCSH=150, NMEMCSH=140 and WCSH=140).
Then, participants were selected by systematic sampling technique by the assumption that the populations in these hospitals are homogenous to the variable to be studied. The K interval was calculated by K=N/n, where N is the number of patients undergoing surgical procedures below the umbilicus (gynaecological, orthopaedic and surgical operations) under spinal anaesthesia within 3 months reported in selected hospitals and n is the sample size.
K=430/180 ≈ 2. Then, a random number between 1 and 2 is selected by the lottery method. After that, every second patient selected for the study from each operating theatre underwent surgery below the umbilicus until we got 180 patients. The detail can be seen from the following figure 1.

Schematic representation of the selection of samples. NMEMCSH, Nigest Mohammed Eleni Memorial Comprehensive Specialized Hospital; WCSH, Werabe Comprehensive Specialized Hospital; WSUCSH, Wolaita Sodo University Comprehensive Specialized Hospital.
Patient and public involvement
This research was discussed with a patient and public group who helped emphasise the importance of reducing delay times and options for treatment that avoid hospital admission. This group co-agreed on the data fields included in this analysis and helped in writing a professional summary about the project.
Data collection procedure
The questionnaire was adopted after reviewing different pieces of literature.19 20 The principal investigator gave orientation on data collection instruments, the objectives of the study and how to facilitate data collection for data collectors. Data were collected by three trained BSc degree holder anaesthetists. Three trained MSc degree holder anaesthetists were assigned to supervise the data collection process. After receiving patients into the preoperative waiting area, they were assessed on their patient-related characteristics immediately after obtaining informed consent from each study participant. Once the patient entered the operation theatre, all patients were kept on fasting for 8 hour for solid food. On arrival in the operating room, standard monitoring was established. An intravenous line was started with an 18-gauge canula, followed by preloading with 10 mL/kg lactated ringer’s solution and maintenance infusion of 6–10 mL/kg/h. Spinal anaesthesia was carried out in the supine position in the middle of lumbar 3 and 4. Bupivacaine 17.5 mg of 0.5% was combined with morphine (100 µg) and neostigmine (50 µg) and administered intrathecally after clear free flow of cerebrospinal fluid (CSF) using a 23-gauge disposable spinal needle after the implementation of the standard hospital monitoring protocol. The patient and the observer collecting the data about study parameters were blinded to the treatment groups. The time of intrathecal injection was recorded, and the patient turned to the supine position. Then, data collectors observed and filled out questionnaires for intraoperative variables. The remaining postoperative data, such as the first-rescue analgesia request (duration of effective analgesia), was noted as the time from intrathecal injection to first-rescue analgesia. The postoperative VAS score (pain severity) was assessed every 4 hours apart until 28 hours, and total analgesic consumption was taken from the patient chart at the end of the follow-up period. On the morning of the surgery, the data collector instructs the patient on how to self-report pain using VAS scores 0 and 10 on the line, 0 for no pain and 10 for severe pain, which was displayed by figure 2 below. The patients were followed for 28 hours. The questions and response categories for each survey are shown in online supplemental table 1.
Supplemental material

Visual analog scales (VAS).
Outcome variables
The primary outcomes were the duration of pain relief, the severity of pain and the time of first analgesic requirement. The secondary outcomes were measurement of postoperative complications (respiratory depression, pruritus, nausea and vomiting).
Data processing and analysis
The data collected were marked, entered, cleaned and exported using EpiData V.4.6 to SPSS V.26 for further analysis. The data were tested for normality using the histogram, kurtosis, skewness and Shapiro-Wilk normality tests and homogeneity of variance by Levene’s test. Data were presented as mean±SD for normally distributed continuous data, and categorical data were presented as numbers, frequencies and percentages. Normally distributed data were analysed using one-way analysis of variance (ANOVA) with post hoc analysis for multiple tests, and the comparisons of categorical variables were analysed using the χ2 and Fisher exact tests as appropriate. A post hoc test (Tukey honest significance analysis) was applied to correct all significant P values among groups. A P value of <0.05 is considered statistically significant.
Operational definitions
Postoperative pain the presence of pain in the postoperative period was defined as a patient having pain and any pain score other than zero starting from recovery within 28 hours.12
First analgesia request time
A time in an hour from the intrathecal administration to first-time analgesia was given.12
Total postoperative analgesia consumption total dose and type of analgesic medication given in mg within the first 28 hours starting from admission to the recovery room.12
Visual analog scale (VAS)
A visual analog scale (figure 2) is an instrument used to assess the severity of pain based on subjective answers in response to postop pain; the subject can mark the severity of their pain on a 10 cm line with the starting end labelled as no pain (0) and the endpoint labelled as very severe pain (10 cm).21
Additives
Adjuvants are drugs used along with local anaesthetics in neuraxial blockade to prolong postoperative analgesia and improve the quality of intraoperative and postoperative analgesia.7
Respiratory depression
Respiratory rate <10 breaths/min.12
Results
Comparison of patient-related characteristics of the study participants
A total of 180 patients participated in the study, which means there was no loss to follow-up due to postponed surgery, and supplemented any other anaesthesia that can alter our study results. Each group includes 60 patients. The age distribution of the participants in the study groups was a mean of 49.7±15.55, 43.93±17.27 and 48.93±17.95 years in NG, MG and BG, respectively, with statistically no significant difference among the groups (P value <0.07). There are no significant differences among the groups regarding the distribution of gender, height and weight (table 1).
Comparison of patient-related characteristics who underwent surgery below the umbilicus during the study period at comprehensive hospitals in southern nation nationalities of Ethiopia
Comparison of the type of procedures among the group
The types of procedures in figure 3 (Delmolo, Types of procedures 2024, 12) of the study group were gynaecology, orthopaedics and surgical patients. 57.5% of surgical, 38% of orthopaedic and 29% of gynaecological operations, respectively, were done among MG, NG and BG patients. The distribution of the type of procedure among the groups did not show statistically significant differences.

{kind=link}
{kind=link}
{kind=link}
Type of procedures.
Comparison of perioperative variables
The distribution of ASA physical status I among the group was 65% (39/60), 65% (39/60) and 50% (30/60), whereas ASA physical status II among the group was 35% (21/60), 35% (21/60) and 50% (30/60) in the NG, MG and BG, respectively, with a χ2 value of 0.174, which has statistically no significant difference among the group (table 2). Comorbid illness, onset of motor block and duration of the surgery have no significant differences among the groups.
Comparison of perioperative variables who underwent surgery below the umbilicus during the study period at comprehensive hospitals in southern nation nationalities of Ethiopia
Comparison of postoperative variables
The mean duration of analgesia among the groups was 9.4±3.18 hours, 9.65±4.93 hours and 3.58±0.98 hours in NG, MG and BG, respectively (P value<0.001) (table 3). The MG and NG have a longer duration of analgesia than the BG. MG and NG had a statistically similar duration of analgesia. The overall mean VAS scores in the 28 hours among the groups were 0.99±0.39, 0.79±0.31 and 2.05±0.91 for NG, MG and BG (P value<0.001), respectively. The overall postoperative pain severity on the mean VAS was higher in the BG. MG and NG have no statistically significant differences in mean VAS. The mean total analgesic consumption (ie, mean diclofenac consumption) was 77.5±19.37 mg, 73.77±46.42 mg and 189.16±55.68 mg, whereas the mean tramadol consumption was 54.167±23.09 mg, 63.93±42.95 mg and 151.667±37.92 mg among NG, MG and BG, respectively (P-value<0.001). BG had more total analgesic consumption than MG and NG.
Comparison of postoperative variables who underwent surgery below the umbilicus during the study period at comprehensive hospitals in southern nation nationalities of Ethiopia
Post hoc test result
The mean difference in first analgesia request time between NG and MG was 0.25, which has no statistically significant difference (p value<0.92) (table 4). The mean difference in first analgesia request time between MG and BG was 6.06, which was a longer duration of analgesia in the MG (p value<0.001). The mean differences in VAS scores between MG and NG at 8 hours, 12 hours, 16 hours, 20 hours, 24 hours and 28 hours were 0.08, 0.85, 0.03, 0.40, 0.13 and 0.22, respectively, which were statistically similar in pain severity. The mean differences in VAS scores between NG and BG at 20, 24 and 28 hours were 0.57, 0.50 and 0.57, respectively, which have no significant difference in pain severity. MG and BG have no significant difference in VAS scores at 24 hours (p value<0.05). The mean difference in total analgesic consumption between the MG and NG was 3.73 mg diclofenac (p value<0.9) and 9.77 mg tramadol (p value<0.3), which were statistically similar. The mean difference in total analgesic consumption between BG and MG was 115.3 mg of diclofenac (p value<0.001) and 87.73 mg of tramadol (p value<0.001), which was more total analgesic consumption in the bupivacaine group.
Post hoc multiple comparisons among the groups who underwent surgery below the umbilicus during the study period at comprehensive hospitals in southern nation nationalities of Ethiopia
Incidence of perioperative complications among the groups
The incidence of nausea was 31.3% (19/60), 6.7% (4/60) and 0% (0/60) for NG, MG and BG, respectively. It was also observed that the incidence of vomiting was 30% (18/60), 3% (5/60) and 0% (0/60) for NG, MG and BG, respectively (p value<0.001). The incidences of pruritus were 1.7% (1/60), 15% (9/60) and 1.7% (1/60) (p value<0.03), and respiratory depression was 1.7% (1/60), 15% (9/60) and 0% (0/60) (p value<0.001), respectively, in the NG, MG and BG, with more incidence in the MG than in the NG and BG (table 5).
Comparison of incidence of perioperative complications among the group who underwent surgery below the umbilicus during the study period at comprehensive hospitals in southern nation nationalities of Ethiopia
Discussions
In the current study, the mean duration of the first analgesia request was longer in MG and NG compared with BG. Similarly, MG and NG had less severe pain and required fewer analgesics overall. Patients in the NG had more incidences of nausea and vomiting. The incidences of pruritus and respiratory depression were highest in the MG. Effective analgesia appeared to work better in the MG and NG.
According to the present study, the duration of effective analgesia, which is the first analgesia request time, was higher in the NG (9.4±3.18 hours) and MG (9.65±4.93 hours) than in the BG (3.58±0.98 hours), which was similar to the findings of the study done in China,22 which reported that both the NG and MG provided a longer duration of analgesia than the BG. A recent meta-analysis also reported results in line with the results of our study but with different adjuvant drugs.14 Another study done in India12 reports that the mean duration of analgesia was significantly longer in the NG (25 µg) (308.76±127.40 min) than the BG (229.52±59.16 min), but the analgesic duration of the NG in this study is lower than in our study. This difference might be due to a lower dose of the adjuvant drug used.
Neostigmine increases the CSF levels of acetylcholine, which in turn inhibits spinal cord motor neuron outflow and may also potentiate bupivacaine-induced axonal conduction block, but no prolongation was observed in studies by Lauretti23 and Almedia, which used lower doses of neostigmine.
A study done in China,24 which was in line with the result of our study, reported that intrathecal tetracaine with neostigmine 100 µg and intrathecal tetracaine with neostigmine 50 µg showed a prolonged duration of analgesia (6–9 hours) compared with the tetracaine alone group. Our study is also in line with studies done in India and Iran,25 26 which showed that the neostigmine group had a much longer duration of analgesia than the control group. Another study conducted in Turkey in 201427 showed that the times until the first analgesia requested in the MG took significantly longer than the other two groups (p<0.01), and NG took significantly longer than the control group, but in our study, MG and NG have statistically similar durations of analgesia. The possible reasons for this discrepancy might be due to the choice of analgesic drug and route of administration.
In conflict with our study, studies conducted in the USA28 and India18 found that the duration of analgesia was similar in the NG, MG and BG, with a p value of >0.05. This difference might be due to the study design, the population included in the study, and the variation in the dose of local anaesthetic agents and adjuvants they used.
In the present study, the overall mean VAS scores in 28 hours among the groups were 0.99±0.39, 0.79±0.31 and 2.05±0.91 for NG, MG and BG, respectively. The VAS pain scores were significantly higher in the BG compared with the NG and MG. Consistent with these findings, studies from China22 and Brazil29 reported a statistically significant lower VAS score in the doses ranging from 25 to 75 µg in the neostigmine group compared with the bupivacaine group. Another study done in the USA30 showed that patients treated by intrathecal morphine had significantly lower mean VAS scores (1.5±1.6 vs 2.5±1.9, p value<0.001), which is consistent with the result of our study. A study conducted in Turkey27 reported that the VAS scores in the bupivacaine group were significantly higher than the MG and NG. No significant differences were found between the morphine and neostigmine groups, which is similar to our study findings. It would appear that there was some residual analgesic effect in the morphine and neostigmine groups over that period. However, our result was in conflict with a study conducted in China22 which detected no significant difference in VAS scores after 8 hours among BG, NG and MG. The reasons for this conflict of results might be due to study design variation, variation in type of surgical procedure, study population variation and difference in dosage of local anaesthetics they used.
In our study, the total analgesic requirements within the 28-hour follow-up period of the three groups were compared, and it was found that the total analgesia used in the 28 hours postoperatively was significantly higher in the BG than the others. The total analgesic consumption between the NG and MG was statistically similar. A comparable result to this finding was reported by a study done in India,12 which showed that the analgesic requirements were significantly higher in the BG than in the MG and NG. Other studies conducted in Brazil31 and Turkey27 also reported findings that were congruent with our study results. However, an incongruent finding was reported by a study conducted in Iran.26 The possible justification for this finding lies in the fact that the analgesic effect of neostigmine follows a pattern that is dependent on the dosage administered, the difference in duration of follow-up, the pain assessment tool they used, and the time they administered the analgesic drugs.
Moreover, in our study, more incidences of nausea and vomiting were observed among those patients in the NG than in the MG and BG. This was in line with the study conducted in Egypt.13
This study is subject to some limitations. The presence of confounding factors (observer bias and the different types of surgeries the patients underwent) may affect our study findings. Different surgeons, including consultants and residents, participated in this study, which does not allow for uniformity in terms of surgical skills, which may have a direct relationship to the discomfort experienced by the patients. We did not evaluate the dose-response, which may clearly indicate the role of these drugs in postoperative pain management. In the face of these, it was conducted at multiple centres and has a follow-up period of 28 hours, which were the strengths of this study.
Conclusions
In summary, the addition of a low dose of morphine (100 µg) and neostigmine (50 µg) to 0.5% isobaric bupivacaine (17.5 mg) for lower abdominal surgery significantly prolonged the duration of postoperative analgesia, thereby reducing the need for early postoperative analgesic use, decreasing postoperative pain severity, and minimising total analgesic consumption compared with bupivacaine alone in a 28-hour period, and it also enhanced the quality of analgesia. But the neostigmine group has a higher incidence of nausea and vomiting than the morphine and bupivacaine groups.
Recommendations
We recommend anaesthetists use MG and NG as adjuvants to local anaesthetics for effective postoperative analgesia rather than bupivacaine alone, and we recommend doing further research using randomised controlled trial. We also recommend comparing different doses of NG and MG as adjuvants to bupivacaine by further studies.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Ethical approval was obtained from the Institutional Review Board of Wolaita Sodo University with reference number of CHSM/ERC/03/15 and submitted to each hospital. A permission letter was obtained to conduct the research from those hospitals. Written informed consent was obtained from each participant, and all participants’ privacy and information were kept confidential. Additionally, all methods were carried out in accordance with relevant institutional guidelines and regulations. The Helsinki Declaration was followed in the conduct of this investigation.
Acknowledgments
We would like to acknowledge the data collectors and anaesthesia staff of the WSUCSH, NMEMSCH and WCSSH for their support during data collection. Finally, our heartfelt thanks go to NMEMSCH as well as Wachamo and Wolaita Sodo University for their outgoing contributions.
References
Footnotes
Contributors NSD, TS, AS and SR: conceptualisation, investigation, methodology, data curation, formal analysis, writing-original draft, writing-review and editing and visualisation. AK, MK, MT, SS, RE, NCW and MJ: conceptualisation, writing-review and editing. GD: conceptualisation, supervision, writing-review and editing. NCW is a guarantor who accepts full responsibility for the finished work and the conduct of the study as well as having access to the data and controlling the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, conduct, reporting or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer-reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.