Article Text

Abstract
Importance Women are under-represented in senior roles within academic medicine, including as authors in high-impact journals.
Objective To examine trends and predictors of female authorship in the Canadian Medical Association Journal (CMAJ) as the only high-impact Canadian journal over a 10-year period to understand gender balances in Canadian academic publishing.
Design This cross-sectional study analysed trends and predictors of female authorship in articles published in CMAJ from 1 January 2013 to 31 December 2023.
Setting Data were extracted from PubMed for CMAJ, the only high-impact Canadian medical journal (impact factor ≥10). Data extraction used the RISmed package in R Studio.
Participants The study included articles published in CMAJ within the specified period. Author gender was predicted using the validated Genderize.io software. Articles where the gender of the authors could not be predicted were excluded from analysis.
Main outcomes and measures The co-primary outcomes were proportions of female first and last authors. Statistical analyses included χ2 tests comparing proportions, Jonckheere and linear regression models to evaluate trends. Among multiauthor articles, multivariable logistic regression models assessed predictors of female first and last authorship.
Results From 5805 included articles, women comprised 47% of first authors and 43% of last authors (p<0.001), both significantly lower than men (p<0.001). Female first authorship increased by 17.7% and female last authorship by 10.5% over the study period (both p<0.05 for trend), reaching a majority (58%) and near parity (48%) in 2023, respectively. Female editor-in-chief and higher proportion of female coauthors were associated with higher odds of female first and last authors; female last authors were additionally associated with higher odds of female first authors.
Interpretation Women were under-represented in authorship overall, though female first and last authorship increased over time, with first authorship exceeding parity in recent years and last authorship nearing equal representation. Female editors-in-chief and a higher proportion of female coauthors were associated with greater female first and last authorship, while female last authorship was additionally associated with higher odds of female first authorship. These findings provide insight into authorship trends in a high-impact Canadian medical journal and may inform future efforts to support gender equity in academic publishing.
- Sexual and Gender Minorities
- Health Equity
- Physicians
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
Analysed a decade of publications in the only high-impact Canadian medical journal.
Used validated software for gender prediction to systematically classify authorship.
Although validated software was used for gender prediction, this may have lower accuracy for gender-neutral names or across different cultures.
Predicted gender may not reflect an individual’s self-identified gender or account for non-binary identities.
This study did not examine the intersection of gender and race or ethnicity.
Introduction
Women remain under-represented in science and academic medicine, comprising a minority of positions across the career spectrum, especially in senior roles.1 Despite an increasing number of women entering the field, significant gender disparities persist, including in the realm of academic authorship—a key measure of academic success and leadership. Women are less likely to achieve senior authorship positions, receive lower research funding and are under-represented as editors, peer reviewers, grant panellists or conference speakers.2–7 These disparities not only hinder individual career progression but also limit the diversity of perspectives essential for innovative research. Although Canadian data is scarce, evidence of this inequity was highlighted in a 2018 review by the Canadian Medical Association (CMA).8
Previous research has documented these gender disparities in publications across various scientific disciplines and regions.9–18 Female-authored papers are less likely to be published in high-impact journals, take longer to get published and receive fewer citations compared with their male counterparts.9 11 15 16 19–22 Factors contributing to these disparities include unequal mentorship opportunities, biases in the peer review process and the added burden of balancing professional and domestic responsibilities.23 A review of selected publications in high-impact US and British journals from 1994 to 2014 reported an increase in female first authorship from 27% to 37%, which had plateaued and even declined in some journals, highlighting ongoing inequities.15 A 2019 publication in JAMA described differential increases in female first and last authors across specialties in high-impact US and British journals from 2008 to 2018, with women experiencing slower transitions from first to last author.9 These temporal trends underscore efforts to improve equity while highlighting areas for further targeted improvement.
Although gender disparities in academic publishing are well-documented, local evaluations are essential, as inequities vary by jurisdiction due to sociocultural, historical and systemic factors. In Canada, women comprise 54% of physicians under 40 and are projected to reach overall parity by 2030, yet barriers persist for career advancement.8 A 2019 Lancet Global Health review found that women represented only 22–42% of Canadian authors, highlighting ongoing inequities.24 As Canada’s leading and only high-impact medical journal, the CMA Journal (CMAJ) plays a key role in supporting local researchers, publishing regionally relevant findings and informing national health policy.25 26 A recent bibliometric review of leading medical journals observed that journals are more likely to publish studies from the country in which the journal is based, and authors are more likely to cite work from their own country.27 Local journals can therefore shape academic opportunities within their countries, making CMAJ an important lens to assess gender equity in Canadian medical publishing.28 29 To date, no study has examined female authorship trends within the Canadian publishing context. Notably, CMAJ employs a single-blinded peer review process, where reviewers know the authors’ identities, thereby introducing potential for gender bias.30 This study aims to investigate trends and predictors of female authorship in CMAJ over a 10-year period.
Methods
Search strategy and study selection
We abstracted all articles published from 1 January 2013 to 31 December 2023 in the CMAJ, which represented the only Canadian medical journal with an impact factor of 10 or higher. The search was conducted on Pubmed on 18 June 2024 with the term ‘CMAJ’ for the period of interest using the RISmed package in R Studio (V.2023.09.1+494). Articles were excluded if they were retracted or published in erratum. There were no other restrictions on article type to capture the broad range of articles published in CMAJ. This study did not require Research Ethics Board approval as it analysed public data.
Outcomes
The co-primary outcomes were proportion of female (1) first and (2) last authors. The last author was reported as this typically denotes the most senior author by convention. These outcomes were reported overall, temporally and in relation to journal characteristics. Secondary outcomes were female composition of authorship teams and predictors of female first and last authorship. In the case of single-authored publications, the author was considered as both first and last author. Gender was considered as a sociological binary construct (ie, female or male); biological sex and non-binary gender could not be evaluated in this study design. First names of first and last authors were used to predict gender at a threshold of 50% using validated software (Genderize.io (https://genderize.io)), and publications where author gender could not be predicted were excluded from analysis.31
Data extraction
Author names, article type, publication dates and PubMed identifiers (PMID) were extracted from articles. Journal editor-in-chief name, impact factor and details of the journal’s review process were obtained from a web search including the journal website.32 33 Gender of journal editor-in-chief was similarly predicted using Genderize.io (https://genderize.io).31
Data analysis
All statistical analyses were performed using RStudio (V.2023.09.1+494).
The Wilcoxon rank sum test was used to compare number of articles published per year and across eras. Descriptive statistics included binomial proportion of female authors overall, per year and during each journal editor’s tenure. χ2 test was used to compare proportions of female authors overall and by author type (first vs last), year, gender of journal editor and within article types. Paired t-test was used to compare annual proportions of first versus last female authors within each year. Jonckheere-Terpstra test was used to evaluate temporal trends in the number of articles and annual proportion of female authors over the 10-year period. Univariable linear regression models were used to evaluate associations between annual proportion of female first and last authors with year of publication and journal impact factor. Among a subcohort of publications with more than one author, multivariable logistic regression models examined potential predictors of female first or last authorship including female editor-in-chief, female composition of the authorship team, publication year and journal impact factor; the model for female first authorship also included female last author as a predictor. All covariates were included as fixed effects. P values <0.05 were considered statistically significant.
Patient and public involvement
None. This study did not involve medical patients.
Results
The literature search identified 6024 articles, and 5805 articles were ultimately included after gender prediction was applied to author names. There was no difference in the total number of articles published annually or before versus after 2019 at the onset of the global COVID-19 pandemic. However, there was a trend to fewer annual publications in 2022–2023 compared with prior years (p=0.07) (online supplemental file 1).
Supplemental material
Women comprised 2728/5805 (47%) of first authors and, slightly less commonly, 2491/5805 (42.9%) of last authors (p<0.001) over the 10-year period, and these were significantly lower than male author counterparts (p<0.001) (figure 1). Women comprised about half of authorship teams (mean 0.46, SD 0.41).

Proportion of female first and last authors in Canadian Medical Association Journal from 2013 to 2023.
Temporal trends of female authorship
The annual proportion of female first and last authors for each year is shown in figure 2. The proportion of female first authors increased by 17.7% and female last authors increased by 10.5% from 2013 to 2023. Women comprised a slight majority of first authors in 2022 (53%) and 2023 (58%) and roughly half of last authors in 2023 (48%). There appeared to be a very small but significant increase in the annual proportion of female first (Jonckheere test p=0.009; linear regression estimate 0.01 (95% CI 0.004, 0.02), p=0.007) and last (Jonckheere test p=0.02; linear regression estimate 0.007 (95% CI 0.0005, 0.01), p=0.04) authors that followed similar trajectories over time (figure 2C). Women were less likely to be last versus first authors in each year assessed (p<0.001). Additionally, there was no difference in the annual proportion of female first or last authors before versus after 2019 at the onset of the global COVID-19 pandemic (data not shown).

(A) Proportion of female first authors each year from 2013 to 2023. (B) Proportion of female last authors each year from 2013 to 2023. (C) Proportions of female first and last authors each year from 2013 to 2023.
Journal characteristics and female authorship
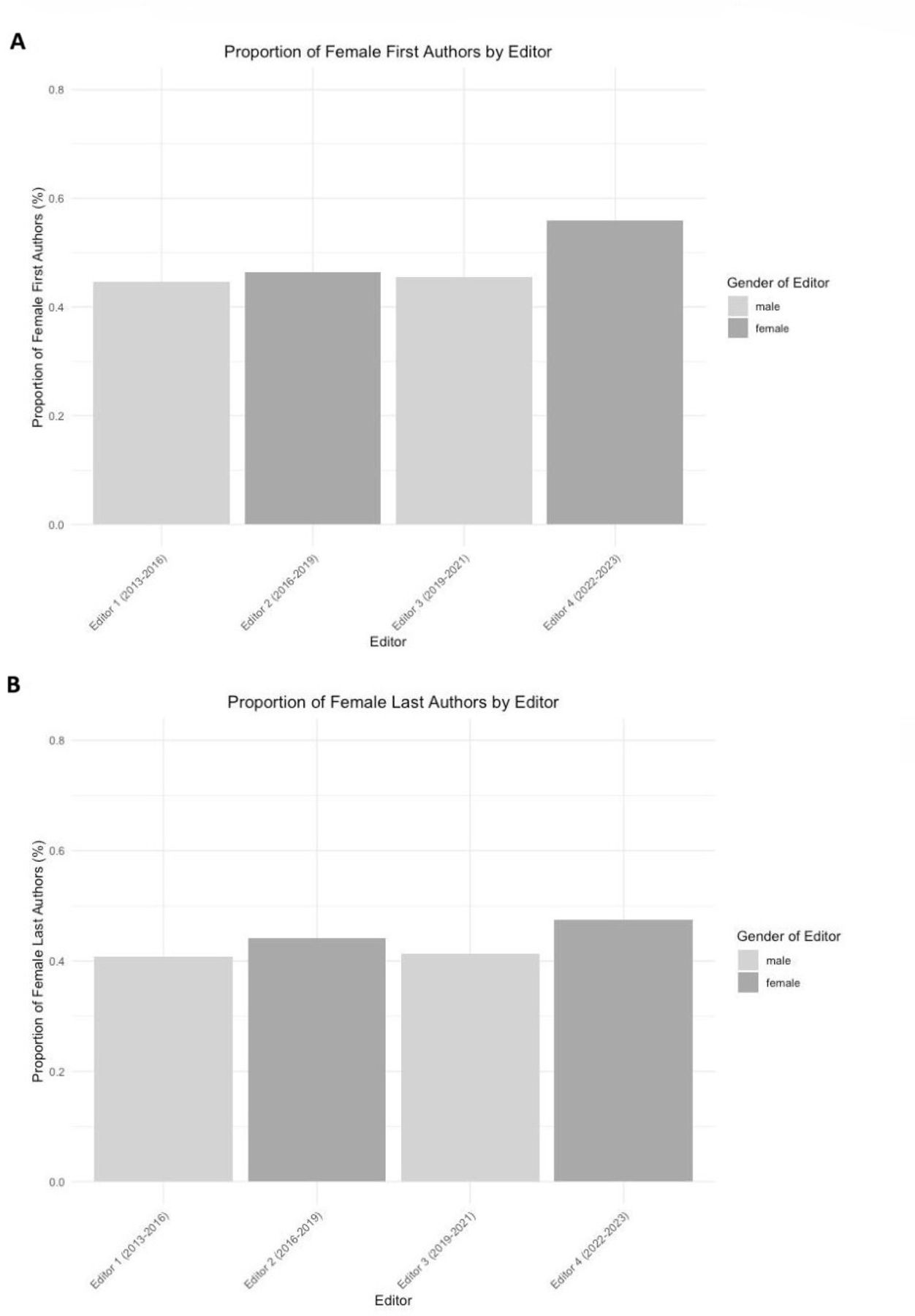
There were four journal editors during the period of interest, two of whom were women. The proportion of female first (p=0.002) and last (p=0.002) authors was higher during the tenure periods of female editors (figure 3).

{kind=link}
{kind=link}
{kind=link}
(A) Proportion of female first authors by journal editor and gender. (B) Proportion of female last authors by journal editor and gender.
The journal impact factor more than doubled from 8.3 in 2020 to 16.9 in 2021 and peaked most recently at 17.4 in 2022 (online supplemental table 1). There was a non-significant trend to slightly higher annual proportion of female first authors (estimate 0.005 (95% CI −0.0002, 0.001), p=0.06), and no association with female last authors (p=0.37), when the journal impact factor was higher.
Supplemental material
Article type and female authorship
There were 2185 articles with an indexed article type. Compared with male authors, female authors were significantly less likely to be first authors of practice guidelines (31%), observational studies (30%), case reports (36%) and comments (32%), and there was a trend to fewer randomised controlled trials (RCTs) (36%, p=0.06). Female last authors were also less common in practice guidelines (28%), multicentre studies (33%), comparative studies (29%), case reports (29%) and comments (30%). Female authors were also less likely to be last authors compared with first authors for meta-analyses, comparative studies and case reports (p<0.001) (table 1).
First and last author gender by article type
Predictors of female first and last authorship
There were 3133 articles with multiple authors and females constitute 1330 (42.5%) of first authors and 1093 (34.9%) of last authors (p<0.001). Odds of female first author were higher when there was also a female last author (OR 1.49; 95% CI 1.15, 1.93), higher proportion of female authors in the team (OR 1.59; 95% CI 1.15, 2.20) and a female editor-in-chief (OR 1.18; 95% CI 1.00, 1.39). The odds of female last author were also higher with a higher proportion of female authors in the team (OR 2.38; 95% CI 1.94, 2.93) and female editor-in-chief (OR 1.25; 95% CI 0.05, 1.48) (table 2). These findings were robust to data-driven adjustments of era effects before and after 2019 (COVID-19 pandemic onset) and 2022 (lower number of publications annually) (data not shown).
Multivariable logistic regression models for female (1) first and (2) last authors.
Discussion
This study investigated trends and predictors of female authorship in a high-impact Canadian medical journal over a 10-year period. Women were less likely to be last versus first authors. The annual proportion of female authors increased by 18% for first authors and 11% for last authors over the study period, and women constituted a slight majority of first authors in recent years. Higher proportions of female first and last authors were observed during the tenure of female editors-in-chief. Odds of female first and last authors were higher with female editors-in-chief and higher proportion of female authors on the team. Moreover, having a female last author was associated with higher odds of having a female first author, highlighting potential benefits of mentorship or support networks.
We identified a lower proportion of female first and last authors overall, but crucially, temporal analyses showed increasing representation over time. The proportion of female first authors increased by 18% and female last authors by 11% over the study period, with females making up a slight majority of first authors and nearly half of last authors since 2022. This trend aligns with broader efforts to improve gender equity in academia and mirrors increases reported in high-impact US and British journals, though the magnitude of change in CMAJ appears greater than in prior studies of general medical journals.9 15 However, improved gender parity was observed in more recent years in this contemporary CMAJ cohort; updated analyses of other medical journals would therefore be needed to examine whether these positive changes in gender balances were isolated or more widespread. Importantly, we found no significant decline in female authorship from the onset of the COVID-19 pandemic, despite early studies showing lower submission and authorship rates for female scientists during the pandemic.34–37 However, female last authorship remained lower than first authorship, suggesting persistent barriers to senior authorship, which has been reported in other studies. Additionally, female authors were under-represented in more impactful publications, such as practice guidelines, RCTs and comparative studies, which are more likely to be highly cited and influence clinical practice and policy.38 These imbalances may reflect ongoing gender disparities at senior levels of the workforce and could reinforce barriers to academic promotion by skewing citation metrics. At the same time, a 2018 US study found that publication-related productivity helped mitigate gendered differences in achieving full professor rank but not senior leadership positions.1 Multifaceted approaches are clearly needed to target these intertwined domains.
The increased odds of female first authorship when the last author was female highlight the role of mentorship and sponsorship in fostering gender equity in academic publishing. Our study also found that a higher proportion of female coauthors was associated with greater odds of both female first and last authorship, suggesting that diverse authorship teams may create more supportive environments for female researchers. Prior research shows that gender-diverse teams produce more novel, high-impact work, reinforcing the broader benefits of diversity in academia.39 A 2019 systematic review reported that mentorship programmes for women led to high satisfaction, increased publications, promotions and retention in medicine.40 Strong female networks and diverse external connections are also associated with higher leadership success for women.41 However, the gender imbalance among senior academics in Canada limits access to female mentors, particularly in fields where women remain under-represented.42 43 Establishing an independent research programme often overlaps with childbearing years, and limited grant funding for female researchers further restricts their ability to mentor junior trainees.2 3 23 44 Female trainees may also struggle to develop effective mentor-mentee relationships due to fears of male mentors in the #MeToo era.45 A Canadian training programme with a gender-balanced award selection committee and structured mentorship has shown benefits in promoting gender diversity and equity for early researchers.44 Having observed real-world improved gender parity for female authors in CMAJ, these findings support the need for future studies examining the identified factors associated with increased female authorship. Implementation studies should also explore potential roles of formal mentorship structures and diverse research teams to promote equitable opportunities for women in academic medicine.
The significant influence of female journal editors on female authorship underscores the importance of leadership in fostering gender equity. Our findings align with prior research showing that female peer reviewers and editors are associated with increased female authorship. However, editorial leadership remains predominantly male across academia. Despite some progress, women still comprise less than one-third of journal editors, with even smaller proportions serving as editors-in-chief, particularly in male-dominated fields like surgery.17 46–50 This lack of representation in editorial leadership may contribute to the slower progression of female authors to senior authorship roles. CMAJ’s single-blind peer review process, where reviewers know the authors’ identities, creates the opportunity to potentially introduce gender bias, as replicated by our study’s gender prediction software. A 2022 systematic review found mixed results on the impact of double-blind versus single-blind peer review on publication decisions by perceived author gender.51 Studies on gender balance would benefit from transparent reporting by journals of author gender at all stages from submission to publication; ideally, studies such as this would not be needed. A recent Canadian review called for collecting and reporting gendered data, promoting voluntary gender disclosure during manuscript submission and advocating for funding bodies to disclose funding success rates by gender.52 Strengthening gender diversity in editorial leadership, alongside transparent peer review and authorship reporting practices, could help advance gender equity in academic publishing.
This study has several strengths. It provides a unique examination of gender disparities in academic authorship within the Canadian context, covering a decade-long period. The use of validated software for gender prediction enhances the reliability of our findings, enabling a robust analysis of trends and predictors of female authorship. However, there are also notable limitations. While the gender prediction software is validated, it is inherently limited and may not accurately identify gender, particularly for gender-neutral names or across different cultures. Additionally, it may not reflect an individual’s self-identified gender or account for non-binary identities. This study also did not examine the intersection of gender and race or ethnicity. Our analysis was restricted to published articles, and we could not assess gendered differences at the submission stage. Article types were classified based on PubMed indexing, which was not uniformly available and may not comprehensively capture all nuances, though we highlighted significant gender differences in first and last authorship as per available data. This study did not analyse manuscript content, which may be an important factor influencing publication patterns. Women are more likely to conduct research on female-focused health issues, which have historically received less recognition and funding. If such research is perceived as lower priority by journals or reviewers, it could partially explain disparities in authorship representation and impact. Future research should explore whether topic selection plays a role in gendered differences in academic publishing. Statistical models are susceptible to residual unmeasured confounding; however, the nature of the dataset precluded broad adjustment for potential confounders. The structure of the data precluded the use of individual fixed effects, which may limit the ability to account for unmeasured author characteristics such as writing style, field of expertise or reputation, that could contribute to observed gender differences in authorship. Finally, we assumed a traditional first versus last author distinction of seniority, which may not always apply, potentially overlooking other collaborative dynamics within author teams.
In conclusion, women were under-represented as first and last authors overall, but we observed increasing female authorship in CMAJ over the past decade, with female first authors surpassing parity in recent years and female last authors achieving near-equal representation. Female journal editors were associated with greater female last authorship, underscoring the role of leadership in shaping authorship patterns. Additionally, a higher proportion of female coauthors was linked to increased odds of both female first and last authorship, while female last authors were associated with higher odds of female first authors, reinforcing the importance of diverse research teams and mentorship in supporting female career progression. These findings suggest that editorial leadership, team composition and mentorship networks play a crucial role in advancing gender equity in academic publishing. Strengthening policies that promote gender-inclusive editorial boards, transparent authorship tracking and structured mentorship programmes may help sustain progress towards equitable representation in medical research.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but was not approved by an Ethics Committee(s) or Institutional Board(s). This study did not require Research Ethics Board approval as it analysed public data. This study did not involve medical patients.
References
Footnotes
Contributors CR: study conception and design, data extraction, statistical analysis, results interpretation and manuscript preparation. CR is the guarantor.
Funding CR is supported by a Kidney Research Scientist Core Education and National Training Program (KRESCENT) salary award co-funded by the Kidney Foundation of Canada, the Canadian Society of Nephrology and the Canadian Institutes of Health Research (CIHR). The funders had no role in defining the content of this article.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.