Article Text

Abstract
Objective To determine wealth-based inequality and the dropout rate in the completion of the maternal continuum of care (CoC) in Ethiopia.
Setting Ethiopian Demographic and Health Survey-2019.
Participants Reproductive-age women (15–49 years) in Ethiopia.
Primary outcome Completion of the maternal CoC services is the primary outcome. Maternal CoC is defined as a situation where women have at least four antenatal care (ANC) visits, deliver their babies at a health facility and receive at least one postnatal care service for both mother and newborn baby.
Methods We analysed the 2019 Mini demographic and health survey data using STATA V.17. Multilevel logistic regression analysis was employed for the factors associated with the maternal CoC. The concentration index was used to measure equity.
Result Overall, 24% (95% CI: 21.6 to 26.5) of women completed the maternal CoC. There was wealth-based inequality in the completion of maternal CoC in Ethiopia (concentration index: 0.25 (95% CI: 0.18 to 0.31, p≤0.001)), rural residents (concentration index: 0.15 (95% CI: 0.09 to 0.21, p≤0.001)) and urban residents (concentration index: 0.15 (95% CI: 0.05 to 0.26, p≤0.01)). Being an urban resident (adjusted OR (AOR)=1.59, 95% CI: 1.09 to 2.33), attaining secondary (AOR=1.67, 95% CI: 1.19 to 2.33) or higher education (AOR=1.93, 95% CI: 1.30 to 2.87) and early initiation of ANC (AOR=1.97, 95% CI: 1.61 to 2.41) were positively associated with the completion of maternal CoC. However, belonging to a pastoral region (Afar or Somali) (AOR=0.46, 95% CI: 0.28 to 0.77), belonging to the poorest (AOR=0.58, 95% CI: 0.37 to 0.92) or middle (AOR=0.62, 95% CI: 0.40 to 0.96) wealth quintile, not being informed about obstetric danger signs (AOR=0.54, 95% CI: 0.43 to 0.66) and blood pressure not being measured (AOR=0.53, 95% CI: 0.32 to 0.85) were negatively associated with maternal CoC.
Conclusion We concluded that completion of the maternal CoC was low in Ethiopia. There was significant inequality in the completion of maternal CoC across wealth status, place of residence and educational status. Strategies and interventions that target the disadvantaged group of women are needed to improve the utilisation of maternal healthcare services. Tailored and multisectoral intervention considering women with poor or middle wealth, women in pastoralist regions and women with no information on obstetric danger signs improves the CoC practice in the country.
- Maternal medicine
- Ethiopia
- Reproductive medicine
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. All data relevant to the study are included in the article or uploaded as supplementary information. All relevant data are within the manuscript and its supporting information file.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
Using a relatively large sample size, high response rate and high-quality data increase the strength of evidences.
Using a substantial sample size of individuals from various regions across the country makes it representative of the entire population.
The study also used simple and complex inequality analysis methods which help to clearly understand the level of inequalities in the completion of maternal CoC.
Multilevel modelling accounts for the hierarchical nature of the data, ensuring robust statistical analysis.
The study relies on self-reported data, which may introduce the potential for recall and socially desirable biases as limitations of the study.
Introduction
In 2020, 287 000 maternal deaths occurred globally, of which 70% were from sub-Saharan Africa according to the report of WHO.1 In 2020, Ethiopia’s maternal mortality was 267 maternal deaths per 100 000 live births.2 Nearly 80% of maternal mortality and many causes of neonatal death are preventable and curable.3 In low and middle-income countries and disadvantaged populations, the burden of death is elevated.4
Ethiopia experiences significant inequalities in maternal health service utilisation, ranking among the highest globally.5 This gap is a major contributor to the country’s high maternal mortality rates.6 While the Ethiopian government is dedicated to implementing equitable health service standards for all demographics, access to vital maternal services continues to be restricted.7 These services encompass antenatal care (ANC), characterised by at least four visits during pregnancy, skilled attendance during childbirth and postnatal care.8 In various developing countries, including Ethiopia, marginalised groups particularly struggle to access these essential, life-saving services, primarily due to their low socioeconomic status.8–11 This barrier presents a substantial challenge to the initiatives aimed at lowering maternal mortality.12
One of the sustainable development goals that Ethiopia signed was equity in maternal healthcare.13 Inequality in healthcare access and services is avoidable.14 15 Narrowing disparities in access to maternal health services reduces maternal morbidity and mortality.16 To improve maternal and neonatal health, the WHO designed a continuum of care (CoC), and the care is provided during pregnancy, birth and the postnatal period.17–19 CoC is the right intervention at the right time20 that reduces maternal and neonatal deaths and disabilities.19 Previously conducted studies in Bangladesh,21 22 sub-Saharan Africa,23 Kenya24 and Ethiopia25 showed that there is an existing inequality in the completion of maternal CoC. Women with higher education, living in urban areas, with access to the mass media and who are wealthier tend to complete maternal CoC more than their counterparts.21 22
To minimise maternal health service inequalities, Ethiopia designed multiple initiatives, including following fee-exemption policies, strengthening community-based health services,26 scaling up community-based health insurance (CBHI)27 and expanding primary healthcare.28 Despite these efforts, studies suggested the persistence of inequities in maternal service utilisation,10 29 even with an increasing trend between 2000 and 2016.8
Studying the continuum of maternal healthcare emphasises the interconnected nature of care throughout pregnancy, childbirth and the postpartum period.30 31 By concentrating on the entire continuum instead of viewing each aspect in isolation, we can prevent complications and enhance overall health outcomes. This holistic approach acknowledges that any disruptions or gaps at any stage can adversely affect both the mother and the child.32 33
Previous studies have focused on the magnitude and factors affecting maternal health services utilisation for specific services.34–36 But studies conducted based on the Ethiopian Demographic Health Survey (EDHS) data on CoC completion and dropout37–39 never considered inequality. In addition, some studies assessing inequality did not assess the complete CoC.8 29 40 Some studies have examined inequalities in the continuum of maternal healthcare25 yet lack detailed information about inequalities in maternal CoC. In Ethiopia, the maternal CoC is essential for the reduction of maternal and newborn mortality and the enhancement of health outcomes.41 42 By providing timely and effective access to these critical services, the CoC aims to prevent complications during pregnancy, labour, delivery and the postpartum phase, thereby significantly improving the health and well-being of mothers and their infants.43 44 The demographic and health survey (DHS) report does not assess the enabling and inhibiting factors of wealth-based inequality on CoC. Therefore, to fill these gaps, this study aims to determine wealth-based inequalities and factors associated with the completion of maternal CoC using the most recent population-based 2019 mini-EDHS. The findings of this study will help policymakers and programme planners in developing specific policies, strategies and programmes to benefit the disadvantaged subgroups of women. In addition, identifying the inequality enables the monitoring of the progress of sustainable development goals. Therefore, this research is also an input for international programme designing for a disadvantaged group of the population.
Methods and materials
Study design and setting
The 2019 mini-EDHS used the population-based cross-sectional study design.29 Ethiopia, one of the countries in sub-Saharan Africa, was the study setting.
Study population
All reproductive-age women (aged 15–49 years) in the selected enumerated areas who gave birth within 5 years before the 2019 mini-EDHS and who had at least one ANC visit for their last child were the study population.
Sample size determination and sampling procedure
Out of 8885 reproductive-age women interviewed, 3979 had given birth within 5 years before the survey, with 1061 of them not receiving ANC during their last pregnancy.45 Consequently, the final analysis included 2918 women, with weighted samples comprising 2913 participants. The mini-EDHS employed a stratified two-stage cluster sampling technique, using a population census as the sampling frame to select enumeration areas based on household estimates and residential types in both urban and rural regions of Ethiopia.45 A detailed illustration of the sampling procedure is presented in the online supplemental figure 1.
Supplemental material
Measurements
Dependent variable: the completion of the maternal CoC is defined as a situation where women have at least four ANC visits, deliver their babies at a health facility and receive at least one postnatal care (PNC) service within 6 weeks after giving birth, either before or after being discharged from the health institution. Conversely, an incomplete CoC is indicated when women who initiated ANC services do not receive any of the three essential services: four or more ANC visits (ANC 4+), institutional delivery and PNC.37 To explain the exposure and the outcome variable, we included directed acyclic graphs to illustrate how the exposure and various covariates influence the outcome in online supplemental figure 2.
Supplemental material
Wealth quantile
The combined wealth index produced in this study has a mean of zero and a SD of one. After calculating this index, national-level wealth quintiles are established by assigning the household score to each de jure household member. Individuals are then ranked according to their scores, and this ranking is divided into five equal parts, creating quintiles. Quintile one represents the lowest wealth group (the poorest), while quintile five represents the highest wealth group (the wealthiest). In this study, the wealth quintiles are derived from the wealth scores obtained through the DHS.
Data processing and analysis
Data from the 2019 mini-EDHS dataset were downloaded, extracted, cleaned, recoded and analysed. All descriptive and inequality analyses were weighted to account for the unequal probability of selection among the strata, using a weighted variable. The complex nature of the data was addressed by incorporating clusters into the multilevel model.
The concentration curve illustrates inequality by plotting the cumulative proportion of maternal care on the y-axis against the cumulative proportion of the population on the x-axis, considering various socioeconomic factors. The concentration index is defined as twice the area between the concentration curve and the line of equality (the 45 degree line). This index ranges from −1 to +1. In the absence of inequality in the completion of maternal care, the index equals 0, and the concentration curve aligns with the line of equality. A negative value indicates that the curve lies above the line of equality, signifying a disproportionate concentration of the health variable among disadvantaged groups. Conversely, a positive value indicates that the curve lies below the line of equality.46
The concentration index (C) can be computed as follows:

where, h=healthcare outcome of interest (ie, completion of maternal CoC), μ is the mean of h and r and r is the rank of an individual living standards variable.
We focused on the concentration curve for four regions (Tigray, Amhara, Oromia and Southern Nations, Nationalities and Peoples’ Region (SNNPR)) with adequate sample sizes, excluding Addis Ababa due to its skewed income distribution towards wealthier subgroups. Given the hierarchical nature of DHS data, women within the same cluster may show greater similarity than those in different clusters, potentially violating the assumption of independence. We assessed this using the intraclass correlation coefficient, which indicated that 25.9% of the variance in maternal CoC was due to clustering.
To account for the clustering effect, we used a multilevel logistic regression model, which included the fitting of four distinct models: a null model without predictors, a model incorporating community-level factors, a model featuring individual-level factors and a model that combined both community and individual-level factors. The fourth model demonstrated the best fit, as evidenced by its lowest Akaike Information Criterion (AIC=2912.0) and the highest log-likelihood (LL=−1429.0). In comparison to the other models, model 4 outperformed the random intercept-only model (null model, AIC=3189.9), the model with only community-level factors (AIC=2988.6) and the model with only individual-level factors (AIC=3097.6). Notably, model 4 is the most appropriate model for data with the lowest AIC among the alternatives. Therefore, our interpretations and reports are based on the findings from model 4 (online supplemental table 1). Before further progress, we checked the assumption of multilevel logistic regression analysis, such as multicollinearity. The Pearson correlation was used to check for multicollinearity. The correlation coefficient ranges between −1 and 1. A value close to 0 indicates no linear association between independent variables. The minimum and maximum variance inflation factor (VIF) values were 1.25 and 3.75, respectively. A VIF value greater than 1 indicates the presence of some correlation among the predictor variables. A VIF value of exactly 1 signifies no correlation. Typically, VIF values ranging from 1 to 5 indicate mild, >5 indicate moderate multicollinearity and values exceeding 10 indicate a serious level of multicollinearity.47
Supplemental material
Both bivariable and multivariable analyses were conducted, with variables showing a p value ≤0.25 in the bivariable analysis considered for the multivariable model. Important variables, such as marital status and CBHI, were included in the final multivariable multilevel logistic regression model. We used adjusted ORs (AORs) with a 95% CI and a p value <0.05 to determine statistical significance in the final model.
Operational definition
Disadvantaged women: a disadvantaged group of women refers to those who experience greater risks of poverty, social exclusion, limited access to healthcare and violence compared with the general population.
Dropout from the maternity CoC: It is considered if a woman drops out of ANC, skilled birth attendant and/or PNC visits.
ANC initiation is defined as early <16 weeks of gestation and late ≥16 weeks of gestation.
Patient or public involvement
Patients or the public were not involved in the design, conduct, reporting or dissemination plans of our research.
Results
Background characteristics of study participants
Over one-third of the respondents, specifically 37%, hailed from the Oromia region, with a significant 70.3% identifying as rural residents. The average age of participants was 27.5 years, with an SD of ±0.15. Notably, 53.0% of respondents fell within the age category of 25–34 years. A substantial majority, 94.3%, were married, while 41.8% identified as followers of the Orthodox Christian faith. Furthermore, 44.0% reported having never attended formal education. Additionally, 87% of households were headed by men, with 33.8% classified in the lowest wealth quintile and 30% enrolled in CBHI (see table 1). The minimum age of the study participants was 18 years and the maximum age was 48 years.
Background characteristics of the study participants
Maternal obstetrics and service-related factors
Almost half of the respondents, specifically 47%, were multiparous. Additionally, 40% of them had their first childbirth before reaching the age of 18 years. A significant 62.7% began their ANC late, while 60% were aware of the warning signs associated with pregnancy. Furthermore, 88.1% indicated that their blood pressure was measured during their visits. In terms of laboratory tests, 78.8% reported that their blood samples were taken, and 73.8% confirmed that their urine samples were collected for analysis during their ANC appointments (refer to table 2).
Completion of maternal continuum of care by maternal obstetric factors and service provided for reproductive-age women in Ethiopia, 2019 (n=2913)
Dropout rate of components of maternal CoC
Out of a total of 2913 women who participated in at least one ANC visit, 1225 women (42.0%) dropped out during the ANC follow-up, having attended fewer than four visits. Among the 1688 women who completed ANC 4+, 445 (26.4%) gave birth at home, resulting in their dropout from the programme. Of the remaining 1243 women who delivered at a healthcare facility, 545 (56.2%) did not receive a PNC check-up. Overall, from the initial group of 2913 women who registered for ANC, 2215 (76.03%) missed at least one service, whether it be ANC, delivery or PNC (see figure 1).

Show dropout of components of the continuum of maternal health services. ANC, antenatal care; PNC, postnatal care.
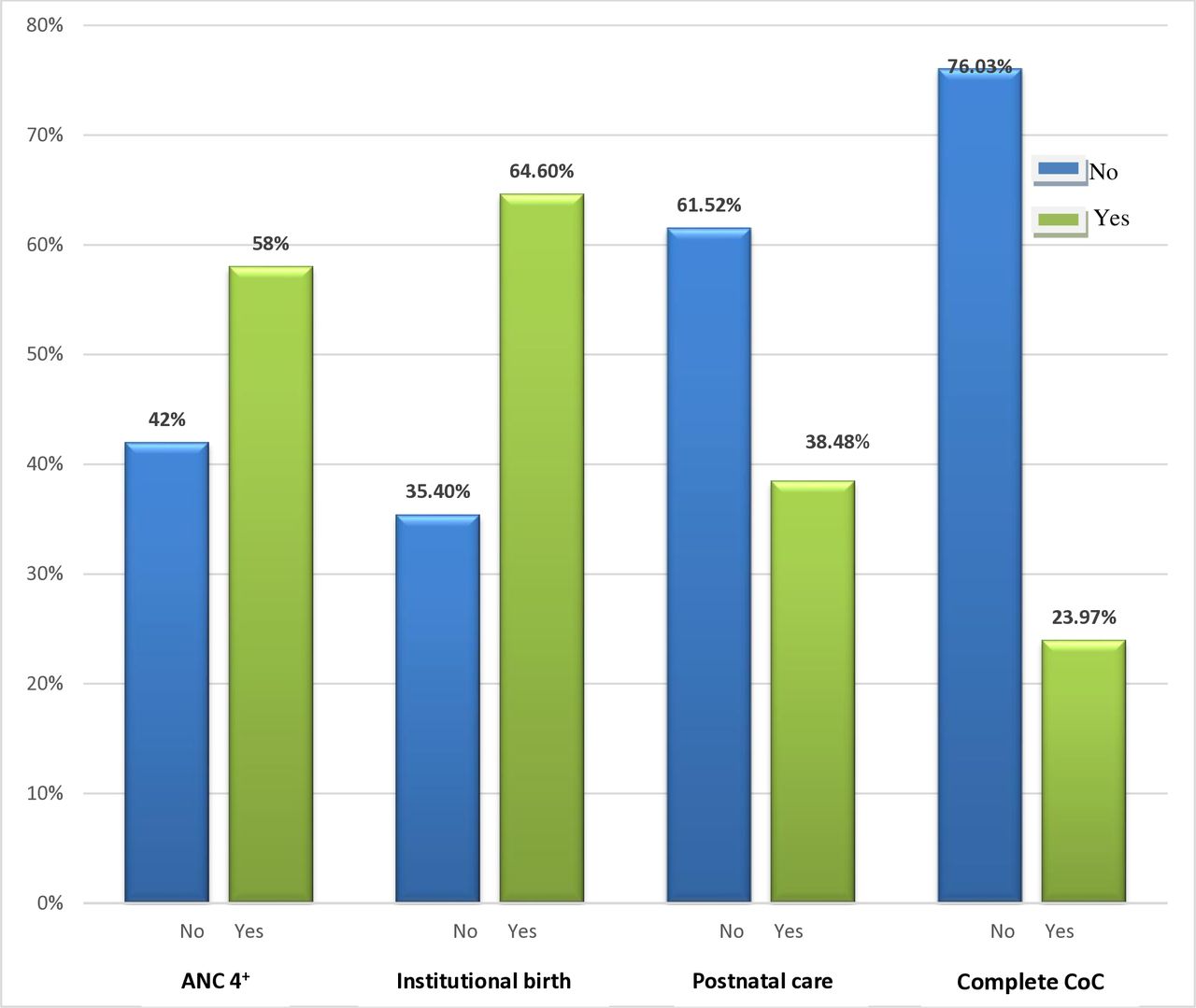
Utilisation of components of the continuum of maternal healthcare
Out of all respondents, 24% of women completed the continuum of maternal healthcare in Ethiopia, with a 95% CI of 21.6% to 26.5%. Specifically, 58% of women attended ANC4+, 64.6% gave birth in a health facility and 38.5% received at least one PNC visit (see figure 2).

{kind=link}
{kind=link}
Utilisation of components of the continuum of maternal healthcare services in Ethiopia. ANC, antenatal care; CoC, continuum of care.
Inequalities in the completion of the CoC
A survey conducted among 865 urban and 2048 rural residents revealed that 36.2% of urban participants and 18.8% of rural participants completed the maternal CoC. Relative inequality was calculated as the ratio of completion rates between urban and rural residents. The residence-based relative inequality in the completion of maternal CoC was found to be 1.9. In the Tigray region, 40.7% of women completed the maternal CoC, whereas in Oromia, this figure was significantly lower at 18.5%. The absolute inequality in completion rates between these regions amounted to 22.3%. In Tigray, 50.7% of women from wealthier backgrounds completed the maternal CoC compared with 28.4% from poorer backgrounds. Similarly, in Oromia, 25.4% of women from the rich subgroup completed the maternal CoC, while only 10.4% of those from the poor subgroup did so. When examining urban and rural residence within Tigray, 62.1% of urban women completed the maternal CoC, in contrast to 30.6% of rural women. In Oromia, 25.0% of urban women and 31.6% of rural women completed the maternal CoC. In the SNNPR, the completion rates were 14.3% for rural women and 16.7% for urban women. The residence-based relative inequality in maternal CoC completion was 2.2 in SNNPR, 2.0 in Tigray and 1.5 in Oromia. Wealth-based relative inequality in the completion of the maternal CoC was 2.4 in Oromia, 2.38 in Amhara and 1.8 in Tigray (online supplemental figure 3).
Supplemental material
Furthermore, a wealth-based inequality was observed in the completion of maternal CoC across Ethiopia, indicated by a concentration index of 0.25 (95% CI: 0.18, 0.31). The positive concentration index for ANC 4+, institutional births and overall completion of CoC suggests a correlation with wealth distribution. However, the concentration index for PNC among urban residents was insignificant, indicating no notable differences in PNC service utilisation among urban women of varying socioeconomic statuses. Conversely, the negative concentration index for fewer than four ANC visits and home births indicates that poorer women disproportionately received inadequate ANC and were more likely to give birth at home. Overall, except for home births and ANC 4+, a greater degree of inequality was observed among rural residents compared with urban counterparts, with wealthier urban and rural women completing maternal CoC at higher rates than their poorer counterparts (online supplemental figure 4).
Supplemental material
Education-related absolute inequality in the completion of maternal CoC was also evident, with 44.7% of women who had attained higher education completing the CoC, compared with only 15.8% of those with no formal education, resulting in a difference of 28.9% (online supplemental figure 5). The concentration curve for all selected regions fell below the line of equity, confirming that the completion of the CoC was disproportionately concentrated among women from wealthier households (online supplemental figure 6).
Supplemental material
Supplemental material
Enabling factors associated with the completion of the continuum of maternal healthcare
In this study, urban-dwelling women were 1.6 times more likely (AOR=1.6, 95% CI: 1.09, 2.33) to complete the CoC. Educational status also played a crucial role; women with secondary education or higher had 1.7 times (AOR=1.7, 95% CI: 1.19, 2.33) and 2.0 times (AOR=1.9, 95% CI: 1.30, 2.87) higher odds of completing the continuum compared with those without any formal education. Early initiation of ANC was associated with a 2.0 times increase (AOR=1.97, 95% CI: 1.61, 2.41) in the odds of completing the continuum. The median OR (MOR) of 2.77 in the null model indicates a variation in the completion of the CoC between clusters. This suggests that women from clusters with a higher proportion of continuum completion were 2.77 times more likely to complete care compared with those from clusters with lower proportions. Furthermore, the proportional change in variance of 70.4% in the fourth model indicates that individual-level and community-level factors together explained 70.4% of the variability in the completion of the CoC (table 3).
Multilevel mixed-effect logistic regression analysis for enabling factors associated with the completion of the continuum of care
Inhibiting factors associated with the completion of the continuum of maternal healthcare
The findings revealed that women from pastoralist communities had 54% lower odds (AOR = 0.46, 95% CI: 0.28, 0.77) of completing the continuum of maternal healthcare compared with their agrarian counterparts. Furthermore, women in the poorest wealth quintile were 42% less likely (AOR=0.8, 95% CI: 0.37, 0.92) to complete the continuum, while those in the middle wealth quintile had 38% lower odds (AOR=0.62, 95% CI: 0.40, 0.96) compared with women in the richest wealth quintile. Additionally, women who were not informed about pregnancy danger signs had 46% lower odds (AOR=0.54, 95% CI: 0.43, 0.66) of completing the continuum, and those whose blood pressure was not measured had 47% lower odds (AOR=0.53, 95% CI: 0.32, 0.85) (online supplemental table 2).
Supplemental material
Discussion
This is the inaugural national study from Ethiopia’s survey, focusing on wealth-based inequality in the maternal CoC. It aims to achieve two main objectives: first, to investigate wealth-based inequality in maternal care and, second, to identify factors influencing the completion of the maternal CoC. Despite fulfilling these objectives, the study has some limitations. Being a cross-sectional survey, it does not allow for the establishment of causal relationships between the completion of care and its predictors. Furthermore, reliance on self-reported data could introduce recall and social desirability biases. The analysis also focused only on two group-level variables: region and residence. Moreover, due to limited sample sizes in specific regions, simple inequality analysis and concentration curves were computed for only four regions.
The overall completion rate of the continuum of maternal healthcare was 24%. This finding is consistent with a study conducted in sub-Saharan Africa,48 which is higher than the results from a study in Bangladesh.21 On the contrary, it is lower than the findings from a study in South and Southeast Asia, specifically in Nepal.49 This situation may contribute to the persistently high rates of maternal and neonatal mortality and morbidity in the country.19 Our results indicate that many dropouts occur between institutional births and PNC services. This trend aligns with studies conducted in Ethiopia.39 One possible explanation for this could be that PNC is often the most neglected and weakest aspect of reproductive and child health programmes.50 In addition, there is a strong community health extension programme implementation that contributes to maternal CoC.51 The advancement of telemedicine enhances the completion of the maternal CoC in the country and the region.52 This suggests that a considerable number of women are failing to complete the maternal CoC, and healthcare facilities are not effectively retaining women who have registered for ANC services within the maternal CoC pathway.
Among women who gave birth in health institutions, a significant 36.6% did not receive PNC before being discharged. A study conducted across sub-Saharan African countries indicated that 71.7% of women received PNC before discharge, with rates varying from as low as 27% in Eswatini to as high as 94% in Burkina Faso.53 Despite existing guidelines recommending PNC,54 it was found that women who were more educated, wealthier and residing in urban areas were more likely to receive predischarge postnatal checkups compared with their less-educated, poorer and rural counterparts.53 Additionally, an analysis of data from the Ugandan DHS revealed that 35% of women did not receive immediate PNC after giving birth in health facilities.55 The likelihood of receiving immediate PNC was notably higher among women who delivered in private health facilities.56 In contrast, a study from Ethiopia found that giving birth in a health facility was negatively correlated with the utilisation of immediate postnatal care.57 This may be due to women opting for early discharge to avoid incurring additional fees58 or due to factors such as poor quality of care, lack of support, verbal or physical abuse and neglect by healthcare professionals during childbirth.59 Other contributing factors may include the low implementation of immediate PNC guidelines by healthcare providers and a shortage of healthcare professionals, which can lead to increased workloads and job dissatisfaction.
We observed significant disparities in the completion of maternal CoC, with urban residents demonstrating a higher likelihood of completion compared with their rural counterparts. This observation corroborates findings from previous studies conducted in Ethiopia,37 48 Bangladesh22 and Ghana.60 Our analysis reveals a regional inequality in maternal CoC completion, with an absolute disparity of 22.28%. This aligns with research conducted in Ethiopia,61 62 Bangladesh22 and Pakistan63 which also highlighted similar trends. The observed differences may be attributed to the better access to healthcare services, infrastructure and socioeconomic factors experienced by urban women.64 These factors include higher levels of education and greater media exposure compared with women living in rural areas. Consequently, this suggests that targeted interventions, taking into account the residential location of women, could be effective in enhancing the implementation of CoC programmes. The observed urban-rural disparities align with regional inequities in health infrastructure and service quality. Targeted investment in rural facilities and transportation could mitigate this gap.
The positive concentration index for ANC 4+, institutional births and the completion of maternal CoC indicates a wealth distribution in the access to these services. In contrast, the negative concentration index for ANC with fewer than four visits and home births suggests that inadequate ANC utilisation and home births are disproportionately common among poorer women. Although rural women have higher absolute home birth rates, the relative inequality in urban areas such as wealthier urban women accessing institutional births at much higher rates creates sharper intraurban disparities. This aligns with a study using Ghana’s DHS data, which indicated that women in the poorest wealth quintile living in urban areas have higher odds of opting for home births.65 Interestingly, regardless of their wealth status, affluent women in rural areas also choose home births, which may obscure socioeconomic disparities among rural populations. This observation is further supported by a case-control study conducted in rural Ethiopia, where wealth status was not found to be a significant determinant of home birth,66 and a study conducted in Bangladesh.21 The decision to give birth at home among rural women is influenced by various factors, including the desire for psychological support from family members, access to culturally acceptable food, the ability to adopt preferred birthing positions and culturally accepted methods for placenta disposal.67–69
The regression analysis indicated that women from the poorest or middle wealth quintiles have lower odds of completing maternal CoC compared with those from the richest quintile. This finding aligns with studies conducted in India,70 Ethiopia,71 Cambodia72 and Sierra Leone.73 It suggests that economically disadvantaged women encounter various barriers such as direct,74 indirect75 or opportunistic76 costs associated with maternal healthcare services. These results underscore the fact that current maternal health services disproportionately benefit wealthier women, highlighting the urgent need to address socioeconomic disparities. Empowering women economically and granting them control over their income could significantly improve the completion rates of maternal CoC among disadvantaged women. This suggests that enhancing women’s economic status and enabling them to manage their own finances may lead to increased completion rates of maternal CoC, ultimately ensuring equitable access to essential healthcare services.
The socioeconomic disparities in the utilisation of PNC among urban residents were found to be statistically insignificant. This suggests that women’s knowledge about PNC services may play a crucial role in predicting service utilisation in urban areas.77 In contrast, when examining rural residents, there is a notable inequity in the components of the continuum of maternal services, except home births and receiving ANC 4+.
There is a notable disparity in the completion of maternal CoC between women with formal education and those without, as well as among women with varying levels of educational attainment. This observation aligns with findings from studies conducted in India,70 Bangladesh21 and sub-Saharan Africa.48 78 One possible explanation for this inequality is that education enhances women’s cognitive skills, economic resources and autonomy.79 Being educated empowers women to make informed decisions regarding their reproductive health rights.80 Additionally, it improves health literacy, enabling them to effectively evaluate health information81 and engage in proactive health-seeking behaviours.82 Conversely, women without formal education often have limited access to health information and face geographical barriers, requiring them to travel long distances to reach the nearest health facilities.83 84
Living in pastoral regions has a detrimental impact on the completion of the maternal CoC. Several factors contribute to this challenge, including physical inaccessibility, lack of awareness about maternal healthcare services, economic constraints, insufficient infrastructure, sociocultural norms and limited autonomy for women.85 These findings suggest that policies must address sociocultural beliefs and enhance both the accessibility and quality of maternal healthcare services in pastoral areas to ensure that women remain engaged in the CoC. Key strategies may include increasing the number of female healthcare providers,86 collaborating with community elders and religious leaders, improving infrastructure and empowering women within these communities.85
The completion of the maternal CoC was positively associated with urban residency. This finding aligns with studies conducted in Cambodia72 and sub-Saharan Africa.48 60 A possible explanation for this trend is that health facilities in Ethiopia are predominantly located in urban areas.87 Research conducted across five regions, Amhara, Oromia, Tigray, SNNP and Harari, along with two administrative cities, Addis Ababa and Dire Dawa, indicated that the average time to reach the nearest health facility is approximately 18 min (±11 min).88 In contrast, studies in rural areas have shown that women often have to walk distances of 60–70 km89 and spend over 2 hours travelling to access services.90 Additionally, some districts lack transportation options altogether.75 89 90 Urban health facilities are three times more likely to have ambulances available on-site compared with their rural counterparts.91 These findings suggest that addressing the barriers to accessing maternal health services in rural and marginalised areas could significantly enhance the completion rate of the maternal CoC.
The timely initiation of ANC has been shown to enhance the completion of the maternal CoC. This finding aligns with research conducted in sub-Saharan Africa.48 73 78 When women book their ANC appointments early, they tend to have longer interactions with healthcare providers. This extended engagement allows for thorough discussions about the importance of maternal and child healthcare services. As a result, women become better informed about potential danger signs during pregnancy, can create a well-defined birth plan and enhance their birth preparedness. This includes understanding delivery dates, recognising signs of labour and being aware of postpartum care.92 Our study also found that women who were not educated about obstetric danger signs had lower odds of receiving comprehensive care. This observation is consistent with findings from other studies conducted in the country.37 62 The lack of knowledge regarding pregnancy danger signs is likely linked to inadequate birth preparedness and readiness for complications.93 Furthermore, factors such as birth preparedness, readiness for complications and planned pregnancies are crucial determinants of the CoC.94 95 These findings underscore the importance of encouraging pregnant women to initiate ANC early and ensuring that they receive quality services, along with proper counselling during each visit. Such measures would significantly promote the timely utilisation of comprehensive maternal and child health services.
The completion of the maternal CoC was adversely affected by the absence of blood pressure measurements. This finding aligns with studies conducted in Egypt96 and Ethiopia.62 The lack of blood pressure monitoring during pregnancy is a significant component of the proxy measures for the quality of ANC services.97 98 High-quality ANC services enhance client satisfaction,99 and satisfaction with these services encourages pregnant women to seek and continue using them.100 Therefore, ensuring the provision of appropriate and high-quality ANC services during pregnancy is crucial for retaining women in the ongoing maternal CoC.
Clinical and public health implications
This study has important clinical and public health implications for decreasing maternal and neonatal morbidity and mortality linked to various preventable causes. Moreover, the findings will aid in ensuring equitable access to maternal health services for disadvantaged groups within the population by implementing the targeted interventions on the identified barriers. This initiative aligns with the pursuit of Sustainable Development Goal 3, particularly targets 3.1, 3.2 and 3.8. Additionally, this research will provide valuable insights for the country’s Health Sector Transformation Plan-II as input for national maternal CoC and monitoring the programme progress of sustainable development goals. In clinical settings, this research will also serve as a crucial tool for evaluating progress in reducing maternal mortality.
Conclusion
The completion rates for maternal care in Ethiopia remain alarmingly low, highlighting significant disparities influenced by factors such as wealth status, geographic location and educational attainment. Research has identified several key factors statistically associated with the successful completion of maternal healthcare, including region, residential area, educational background, wealth index, timing of ANC initiation, awareness of danger signs and blood pressure monitoring.
To address these inequalities, we recommend that policymakers and programme planners prioritise the development of effective and inclusive policies, strategies and programmes specifically targeting women in rural areas, those with lower educational levels and economically disadvantaged groups. Healthcare professionals should focus on counselling pregnant women about potential danger signs during pregnancy and ensure the provision of high-quality ANC services, which include regular blood pressure assessments. The observed urban-rural disparities align with regional inequities in health infrastructure and service quality. Targeted investments in rural facilities and transportation could help bridge this gap.
Equity-oriented healthcare reform in Ethiopia is essential for identifying disparities in access to quality healthcare services and understanding the factors contributing to these disparities. This information can guide the design of tailored interventions, resource allocation and policy implementation to meet the needs of underserved populations effectively.
Additionally, programmes and policymakers must create targeted interventions for marginalised groups. Mobile ANC clinics, increased deployment of female community health workers and conditional cash transfers could significantly enhance access to care in pastoral and rural areas. Tailored approaches that consider the unique needs of impoverished, rural, uneducated and pastoralist women are strongly recommended to help bridge the existing gaps in maternal healthcare, including ANC, PNC and institutional deliveries.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. All data relevant to the study are included in the article or uploaded as supplementary information. All relevant data are within the manuscript and its supporting information file.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Footnotes
Contributors MSA comprehended and designed the conception of the study. All authors (MSA, SG and DA) contributed to the data extraction, analysis, interpretation of the result and drafting of the article. All authors participated fully in revising the article, have agreed on the journal to which the article will be sent for publication, gave final approval of the version to be published and agreed to take responsibility for all aspects of the work. MSA is the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.