Article Text

Abstract
Objectives To develop and validate a risk prediction model for adverse outcomes in patients with angina with non-obstructive coronary arteries (ANOCA) confirmed by invasive coronary angiography.
Design Retrospective cohort study.
Setting A tertiary cardiovascular care centre in China.
Participants From 17 816 consecutive patients undergoing coronary angiography for suspected coronary artery disease, 5934 met ANOCA criteria after rigorous exclusion: (1) significant stenosis (≥50% luminal narrowing), (2) established coronary artery disease history, (3) incomplete baseline/follow-up data, (4) non-cardiovascular life-limiting conditions.
Primary and secondary outcome measures The primary outcome was a composite of all-cause death, non-fatal myocardial infarction (MI), stroke and repeat percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG). The secondary outcome was major adverse cardiovascular events, defined as cardiac-related death, non-fatal MI, non-fatal stroke, repeat PCI and CABG.
Results The derivation cohort (n=4452) and validation cohort (n=1482) demonstrated comparable baseline characteristics. The nomogram incorporated eight prognosticators: age, haemoglobin, serum urea, serum sodium, alanine aminotransferase/aspartate aminotransferase ratio, N-terminal pro-B-type natriuretic peptide (NT-proBNP), left atrial diameter and left ventricular ejection fraction. The prediction model showed robust discrimination for primary endpoint, achieving area under the curve (AUC) values of 0.82 (1 year), 0.90 (2 years) and 0.89 (3 years) in the derivation cohort, with corresponding validation cohort AUCs of 0.75, 0.77 and 0.78. Calibration plots revealed close alignment between predicted and actual event-free survival probabilities in both cohorts. Risk stratification identified two distinct prognostic groups with significant survival differences (log-rank p<0.0001).
Conclusions This predictive model integrates routinely available clinical parameters to accurately stratify mortality and cardiovascular risk in ANOCA patients, providing a potential valuable decision-support tool for personalised therapeutic strategies.
- Angina Pectoris
- Coronary heart disease
- Prognosis
Data availability statement
Data are available upon reasonable request. The original data supporting the findings of this study can be obtained from the corresponding author upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study used a large sample size (n=5934) with rigorous internal validation through training and testing cohorts.
Leveraged Lasso-penalised Cox regression with 10-fold cross-validation to optimise model generalisability.
The nomogram integrates routinely available clinical variables, enhancing clinical applicability.
Limitations include the retrospective design, which may introduce selection bias.
Data were derived from a single centre, potentially limiting generalisability.
Backgrounds
Chest pain is a common symptom among patients seeking medical services, often raising concerns about potentially life-threatening conditions such as coronary artery disease (CAD).1 2 Timely and accurate diagnostic assessments, including electrocardiography, coronary CT angiography (CCTA) and coronary angiography (CAG), are frequently recommended for individuals presenting with chest pain to rule out severe conditions such as myocardial infarction (MI).3 4 However, in the cohort of patients undergoing diagnostic workup, approximately half exhibit non-obstructive coronary arteries (stenosis less than 50%),5 6 a condition known as angina with non-obstructive coronary arteries (ANOCA).7
ANOCA patients often seek medical care due to symptoms and undergo repetitive invasive examinations, leading to significant healthcare resource utilisation and imposing individual burdens and additional risks.8–10 In a randomised controlled trial involving over 10 000 patients suspected of CAD with intermediate pretest likelihood, only approximately 12% of them yielded a positive result in the final coronary artery functional tests.11 Patients with a low pretest probability exhibit an exceedingly low positivity rate in diagnostic workup and experience fewer adverse outcomes.12 Therefore, clinical guidelines recommend delaying diagnostic testing for patients at low risk for CAD.13 14 However, patients without obstructive coronary arteries confirmed by CAG or CCTA have been observed to experience more adverse outcomes compared with the general population.15–17 Identifying high-risk individuals in ANOCA patients remains a challenge.
There is limited research on predicting adverse outcomes in ANOCA patients confirmed through CAG or CCTA. Some studies have validated the utility of specific pretest indicators, such as age, sex and traditional cardiovascular disease risk factors (eg, hypertension), to identify low-risk ANOCA patients.18 However, several investigations have shown that specific blood biomarkers, including high-sensitivity troponin and lower high-density lipoprotein cholesterol (HDL-C) levels, operate as independent predictive factors for poor prognosis in ANOCA patients, adding prognostic value.19 To date, comprehensive studies that screen non-invasive indicators and develop a prognostic model are lacking, and most previous studies are reliant on data derived from the Women’s Ischemia Syndrome Evaluation (WISE) study,19–21 which exclusively includes female participants. One study also used WISE data to validate the effectiveness of some risk scores originally designed for other populations, such as the Atherosclerotic Cardiovascular Disease score, in predicting adverse outcomes in ANOCA patients, but the results showed suboptimal performance.22 Therefore, it is necessary to develop a predictive model based on non-invasive indicators to forecast adverse outcomes in ANOCA patients of both sexes. This study aims to bridge this gap to optimise clinical decision-making and patient management.
Method
Study population
This is a retrospective cohort study that consecutively enrolled patients who presented with suspected symptoms of CAD and underwent CAG at the department of cardiology or emergency department of the Second Hospital of Tianjin Medical University between January 2019 and June 2023. The Second Hospital of Tianjin Medical University is a cardiac centre serving the northern Chinese city of Tianjin and its surrounding regions. This study adheres to the principles outlined in the Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD) statement.23
ANOCA patients were defined as angina with non-obstructive epicardial coronary arteries (stenosis <50%), adhering to current expert consensus.7 Patients meeting the following criteria were excluded from the study: (1) patients with acute coronary syndrome or obstructive coronary arteries (defined as a luminal stenosis of ≥50% in a major epicardial coronary artery7 24); (2) patients with a prior diagnosis of CAD, history of percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG); (3) individuals with severe liver or kidney dysfunction, malignancies or other non-cardiovascular conditions significantly affecting life expectancy; (4) those with substantial missing baseline data and (5) patients lost to follow-up.
Clinical data collection
Patient data were retrospectively obtained from electronic medical records, including demographic information, medical history, vital sign data, laboratory parameters, echocardiographic data, CAG findings and other relevant details.
Follow-up and endpoints
A dedicated follow-up team conducted systematic postdischarge surveillance through a standardised protocol, with scheduled assessments at 30 days, 3 months, 6 months and annually thereafter. Data collection employed a multimodal approach: (1) comprehensive electronic health record review, (2) cross-referencing with regional death registries and (3) telephone or email interviews. The observational window for this analysis was finalised on 1 August 2023. Two board-certified cardiologists (LZ and Z-KX, each with >5 years clinical experience) independently evaluated all events using standardised diagnostic criteria.25 26 For discrepancies in event classification, an adjudication committee comprising two senior interventional cardiologists (TL and K-YC, both with >20 years catheterisation laboratory experience) conducted final arbitration through consensus review.
The primary endpoint was a composite of all-cause death, non-fatal MI, stroke and repeat PCI or CABG during follow-up. The secondary endpoint was major adverse cardiovascular events (MACE), defined as cardiac-related death, non-fatal MI, non-fatal stroke, repeat PCI and CABG during follow-up. The composite endpoint was selected based on its established utility in prognostic studies of ANOCA.19 20 22 27
Statistical analysis
For the small amount of missing data in smoking and alcohol consumption history, multiple imputation was performed using the MICE package (Multiple Imputation by Chained Equations package). To establish a reliable model, the entire study cohort was randomly stratified into two subsets, a training set and a validation set, with a ratio of 0.75 to 0.25, respectively. The training set was used to generate the predictive model, while the validation set was used for model internal validation.
Categorical variables were described as frequencies and percentages, with group differences assessed using the χ2 test or Fisher’s exact test as applicable. Continuous variables were expressed as either the mean±SD or median (IQR), and group comparisons were conducted using the t-test or Kruskal-Wallis test as appropriate. Variables with variance inflation factor ≥5 were excluded prior to Lasso regression to mitigate multicollinearity. The variables selected through Lasso regression were incorporated into the Cox proportional hazards regression model, and a nomogram was generated based on the Cox regression analysis model. The discriminative ability of the predictive model was evaluated using area under the curve (AUC). The model’s calibration was assessed through the calibration curve. Additionally, decision curve analysis was employed to evaluate the clinical utility of the nomogram.
The total score for each patient was calculated based on the nomogram, and the study population was stratified into high-risk and low-risk groups according to the score corresponding to the 3-year 95% event-free survival probability. Event-free survival for the high-risk and low-risk groups in the training and validation sets was estimated by Kaplan-Meier method and compared with the log-rank test. All statistical analyses were performed with R software V.4.3.1 (R Foundation for Statistical Computing). All statistical tests were two-tailed, with a significance level set at p<0.05.
Patient and public involvement
None.
Result
Study population and patient characteristics
Out of a consecutive cohort of 17 816 patients who underwent CAG for suspected CAD, 9883 individuals with significant coronary artery stenosis and 1816 patients with a documented history of coronary heart disease were excluded. An additional 131 individuals were excluded due to missing baseline or follow-up data, and 52 patients with severe conditions such as malignant tumours were also excluded. Final analysis included 5934 patients with negative CAG results (figure 1).

Flowchart of study participation. CAD, coronary artery disease.
The mean age of the overall cohort was 43.6±10.8 years, with 58.3% being female, and the median follow-up time was 631 (270, 972) days. Detailed baseline data are provided in online supplemental table 1. During the follow-up period, 145 (2.44%) patients had primary endpoint events, 82 (1.38%) had MACE, 106 (1.79%) had all-cause death, 33 (0.56%) had MI and 11 (0.19%) had a stroke. The Kaplan-Meier method was employed to estimate the survival without various adverse events for the total study population (online supplemental figure 1).
Supplemental material
Nomogram built based on Lasso-Cox regression
The entire cohort was randomly divided into a training cohort consisting of 4452 patients and a validation cohort comprising 1482 patients. There were no statistically significant differences in the collected variables between these two groups (online supplemental table 1). Lasso regression was employed to select variables with the strongest correlation to the primary endpoint. As the regularisation parameter (λ) increased, certain coefficients were reduced to zero, effectively eliminating those variables from the model (figure 2A). We used a tenfold cross-validation approach to identify the optimal model. Due to the relatively limited number of cases undergoing primary endpoint events in the validation cohort (145), we employed the 1-SE rule, resulting in eight selected variables (figure 2B). These variables were incorporated into a Cox proportional hazards regression model, with results presented in table 1. All models satisfied proportional hazard assumptions (global test, p=0.057). A nomogram was developed based on the Cox regression model, with the regression coefficients of these factors amalgamated into a scoring system, ranging from 0 to 100 (figure 3). For example, an 81-year-old male patient with a haemoglobin level of 92 g/L, serum urea of 14.1 mmol/L, serum sodium of 145.6 mmol/L, an alanine aminotransferase (ALT)/aspartate aminotransferase (AST) ratio of 1.68, NT-proBNP at 272 ng/L, left atrial diameter of 38.83 millimetres and an LVEF of 62% received a total score of 115. The 1-year, 2-year and 3-year event-free survival rates were 99.5%, 96.2% and 89.0%, respectively.
Prediction of event-free survival probability using the Cox proportional hazards regression model based on Lasso regression

Variable selection based on Lasso regression. (A) Variation characteristics of variable coefficients; (B) selection process of optimal λ value in Lasso regression model using cross-validation.

Nomogram for predicting the probability of 1-year, 2-year and 3‐year event-free survival of ANOCA patients as assessed by coronary angiography. ALT, alanine transaminase; ANOCA, angina with non-obstructive coronary arteries; AST, aspartate transaminase; LVEF, left ventricular ejection fraction.
Discrimination and calibration of the nomogram
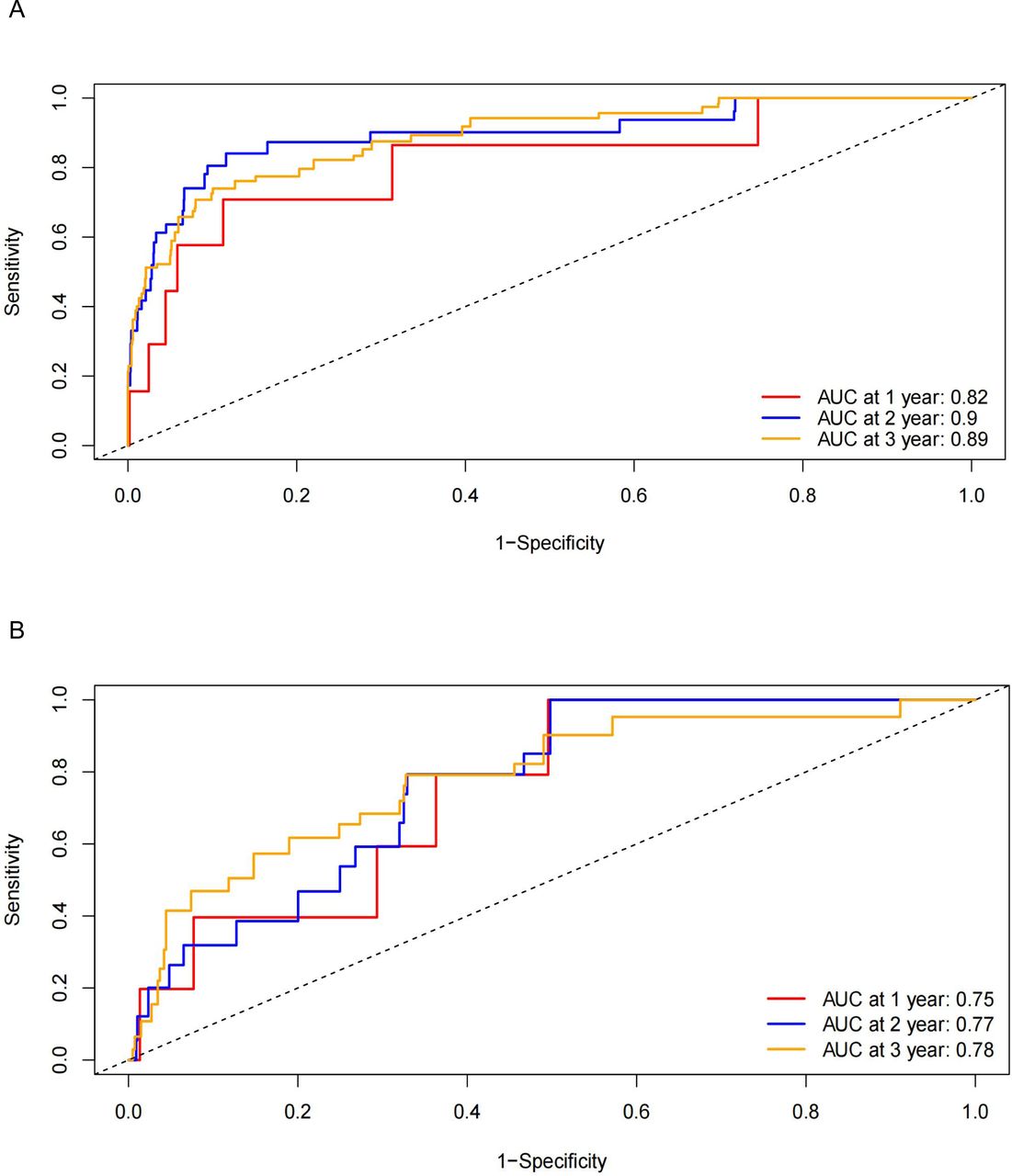
The discriminative ability of the model was assessed by plotting receiver operating characteristic curves. In the training set, the AUC for 1-year, 2-year and 3-year predictions was 0.82, 0.90 and 0.89, respectively. In the validation set, the corresponding AUC for 1-year, 2-year and 3-year predictions was 0.75, 0.77 and 0.78, respectively (figure 4).

Receiver operating characteristic curve for the 1-year, 2-year and 3‐year primary endpoints of the nomogram in the training set (A) and validation set (B). AUC, area under the curve.
Figure 5 illustrates calibration plots for the models predicting 1-year, 2-year and 3-year survival in both the training and validation datasets. In well-calibrated models, the points closely align with the ideal 45° line, indicating that predicted survival closely matches observed survival and demonstrating good model calibration.

Calibration plot of predicted 1-year, 2-year and 3-year event-free survival based on the nomogram in the training set and validation set. (A–C) Training set; (D–F) Validation set.
Decision curve
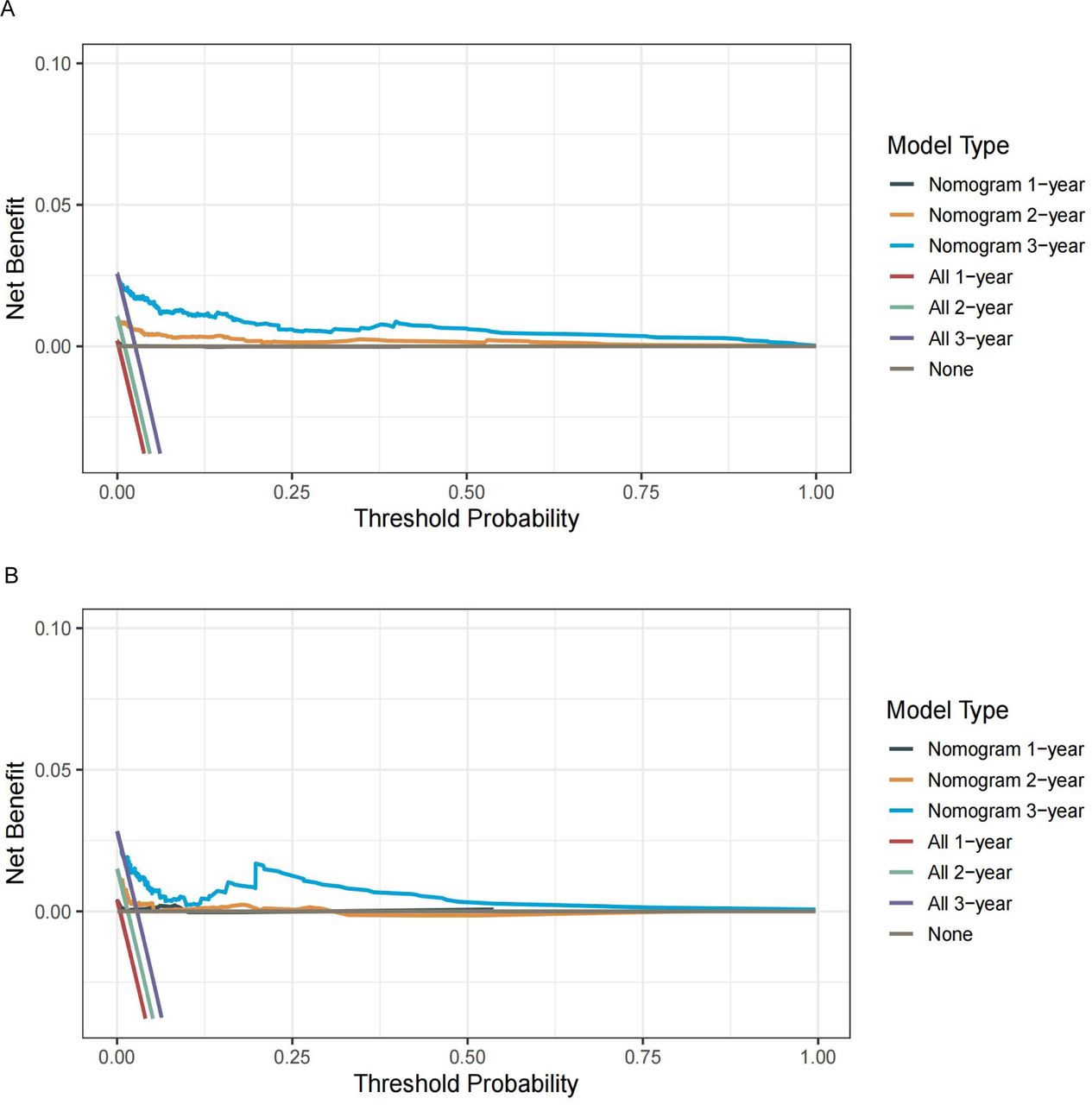
Decision curve analysis was employed to evaluate the potential improvement in clinical outcomes through nomogram-assisted decision-making for patients. As illustrated in figure 6, the results reveal that across a broad spectrum of threshold probabilities in both the training and testing cohorts, utilising the nomogram for predicting the 2-year or 3-year event-free survival probability offers a more significant net benefit when compared with strategies of ‘treat all’ or ‘treat none’. These findings underscore the clinical utility of the nomogram.

Decision curve analysis of the nomogram in the training cohort (A) and validation cohort (B). The x-axis represents the threshold probability, and the y-axis measures the net benefit. The left-slanting straight line shows the net benefit of treating all patients. The bottom horizontal grey line represents the net benefit of not treating any patients. The curve in the middle represents the nomogram.
Risk stratification
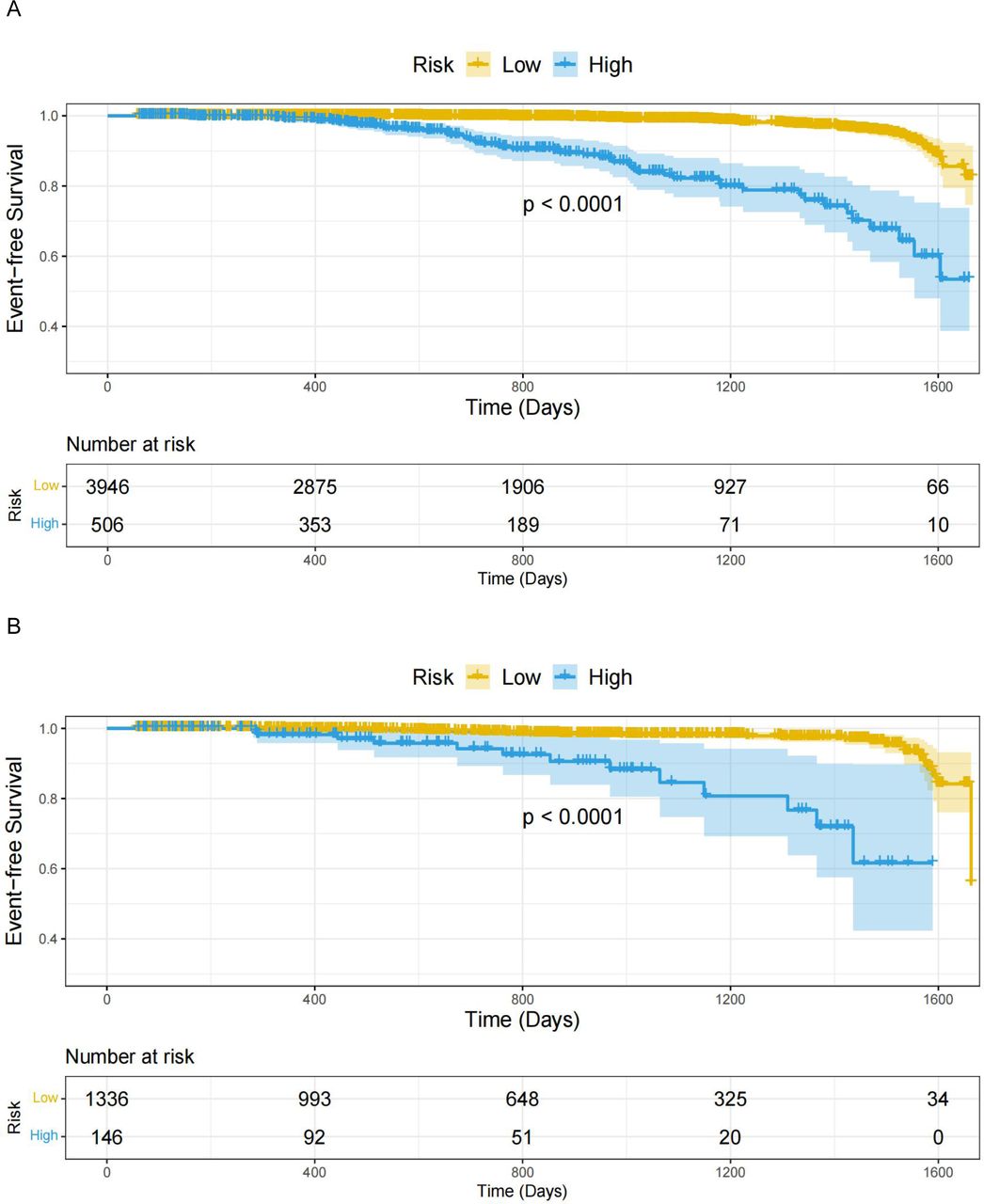
Considering that the study population consists of low-risk patients with non-obstructive coronary artery stenosis, the threshold for further risk stratification was set at a higher event-free survival probability, specifically a score of 104 points corresponding to the 95% 3-year event-free survival probability as determined by the nomogram. Individuals scoring below this threshold were categorised as low risk, while those scoring equal to or above it were classified as high risk. Kaplan-Meier curves depicting event-free survival were created for the two risk groups in the training and validation sets (figure 7). Furthermore, MACE event-free survival of these groups is shown in online supplemental figure 2. These results consistently demonstrated the model’s efficacy in patient risk stratification.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier curves for primary endpoint event-free survival in the low-risk and high-risk groups in the training set (A) and validation set (B).
Discussion
This study focused on patients initially suspected of having CAD but who were found to have non-obstructive coronary arteries following CAG. A wide range of variables, including demographic information, vital signs, laboratory parameters and echocardiographic measurements, were meticulously examined. Ultimately, 8 key variables, namely age, haemoglobin levels, serum urea, serum sodium levels, ALT/AST ratio, NT-proBNP levels, left atrial diameter and LVEF, were identified. The study successfully developed a nomogram to predict the probability of event-free survival for these patients, demonstrating excellent discriminatory and calibration abilities in both the training and validation sets. The utilisation of this predictive model in clinical practice empowers healthcare providers to conduct more precise risk stratification, particularly for individuals initially classified as low risk, thereby improving diagnostic, management and treatment strategies and ultimately enhancing patient outcomes.
In clinical practice, a substantial number of patients with potential cardiac issues, such as chest pain, actively seek medical attention in both outpatient and emergency department settings. In the United Kingdom, for instance, approximately 1%–2% of adults consult primary care facilities when experiencing chest pain for the first time.15 Similarly, millions of individuals in the USA undergo stress tests in outpatient clinics each year for undiagnosed heart conditions.11 However, research has consistently shown that following diagnostic assessments like CAG, approximately 50% of patients do not exhibit obstructive coronary artery stenosis.5 16 24 28 Traditionally, such patients were often considered to have a favourable prognosis and no significant cardiac conditions, potentially resulting in the omission of further diagnostic measures and therapeutic interventions.29–31 However, recent research has indicated that these patients face a significantly elevated risk of adverse outcomes compared with the general population. The WISE study revealed that over a 10-year follow-up, patients without obstructive coronary stenosis on CAG had rates of cardiovascular death and MI of 6.7% and 12.8%, respectively, underscoring the heightened risk among female ANOCA patients.21 32 33 Other studies have also demonstrated that ANOCA patients, regardless of their gender, face an increased risk of experiencing CAD-related outcomes compared with the general population.16 28 34
Our findings from this study indicate that ANOCA patients tend to be younger, with an average age of 43.6 years, and a higher proportion of them are female (58.3%).7 During a median follow-up period of 2 years, the rates of all-cause death, MI and stroke were 1.79%, 0.56% and 0.19%, respectively. These findings align with a previous study reporting 1-year MI rates ranging from 0.11% to 0.59% and 1-year mortality rates ranging from 1.38% to 2.3%.28 Our research further supports the characterisation of ANOCA patients and provides additional evidence of their elevated risk for adverse outcomes across diverse populations.
While clinical guidelines suggest risk stratification of chest pain patients and deferring testing for those with a low likelihood of CAD, this strategy may inadvertently exclude high-risk ANOCA patients who require further assessment and appropriate therapeutic interventions.13 14 As highlighted in a recent review, a significant proportion of ANOCA patients (ranging from 75% to 90%) exhibit various underlying causes, such as coronary microvascular dysfunction, microvascular spasm, endothelial dysfunction, epicardial coronary spasm and/or myocardial bridging,7 35 emphasising the critical importance of identifying high-risk ANOCA patients to optimise their further management.
Current research on factors related to adverse outcomes in the ANOCA population is limited. One study attempted to develop a risk tool for chest pain patients with normal coronary arteries to predict favourable outcomes. This tool comprised 10 variables, including age, gender and the presence of conditions like hypertension, diabetes or dyslipidaemia. However, it is important to note that this study solely relied on pretest clinical data and accessed coronary arteries through CCTA.18 In contrast, our predictive model incorporated pretest indicators, including demographic variables and medical history, with age being one of the key factors. Age is a variable included in many traditional CAD prediction models because it is easily obtainable and reflects the ageing of the entire cardiovascular system, including increased arterial stiffness and decreased vascular endothelial function.22 36
Previous studies have also indicated that several blood biomarkers are associated with unfavourable outcomes in ANOCA patients, including lower levels of HDL-C, elevated levels of soluble urokinase-type plasminogen activator receptor and high-sensitivity troponin.19 20 However, none of these studies conducted comprehensive screening of clinical variables or developed a predictive model. After a thorough screening of blood biomarkers, our predictive model incorporated haemoglobin, serum urea, serum sodium and NT-proBNP, which are rarely reported to be associated with adverse outcomes in ANOCA patients. Anaemia, for example, is a common pathological condition involved in the occurrence and development of CAD and heart failure through various mechanisms.37 It significantly increases the risk of developing CAD and heart failure and is associated with adverse outcomes in these patients.38 39 Serum urea reflects renal function, which is a crucial factor influencing the cardiovascular system.40 Previous research has shown that an elevated serum urea levels increase the risk of CAD and serve as predictive factors for adverse outcomes in CAD and heart failure patients.41 42 The role of serum sodium in cardiovascular disease is still not fully understood, but several studies have indicated that even mild reductions in serum sodium, even within the normal range, are associated with higher all-cause mortality and cardiovascular mortality in elderly individuals or the general population.43–46 The underlying mechanisms behind this association require further research. NT-proBNP is a widely recognised marker for heart failure and exhibits strong predictive capabilities for the prognosis of heart failure patients.47 Previous studies have also demonstrated its ability to predict cardiovascular events and mortality even in community-dwelling or elderly populations without heart failure.48–51
Our predictive model also considered echocardiographic parameters. Echocardiography is a non-invasive, easily performed and cost-effective imaging technique that provides comprehensive insights into cardiac structure and function. In our model, left atrial diameter and LVEF were included. Left atrial enlargement is closely associated with conditions like atrial fibrillation and heart failure, and factors such as hypertension and mitral valve diseases can also lead to left atrial enlargement. It is commonly regarded as a biomarker for adverse cardiovascular outcomes.52–55 The LVEF serves as one of the diagnostic and classificatory criteria for heart failure, with the latter often signifying the advanced stage of diverse cardiac ailments and indicates an unfavourable prognosis.56 57
Limitations
This study has several limitations. First, the retrospective design precludes control of treatment strategies and introduces potential selection bias. Second, the study population consisted entirely of individuals from northern China, so caution should be exercised when generalising the findings of this study to other populations. Third, the inability to subclassify ANOCA patients into those with versus without atherosclerosis represents an important limitation, as pathophysiological differences between these cohorts may contribute to population heterogeneity. However, this aligns with current guideline definitions, and future studies incorporating intracoronary imaging could refine risk stratification. Finally, while the predictive model developed from single-centre data has not yet undergone external validation, internal validation confirmed its robust discrimination and calibration, indicating strong performance within the original cohort.
Conclusion
In summary, we conducted a comprehensive evaluation of clinically accessible variables and successfully developed a predictive model for assessing adverse outcomes in angina patients with suspected CAD who do not exhibit obstructive coronary artery stenosis. This nomogram equips clinicians with a valuable tool for risk stratification in ANOCA patients, allowing for optimised management and treatment strategies aimed at improving patient outcomes.
Data availability statement
Data are available upon reasonable request. The original data supporting the findings of this study can be obtained from the corresponding author upon request.
Ethics statements
Patient consent for publication
Ethics approval
This study received approval from the Ethics Committee of the Second Hospital of Tianjin Medical University, with a waiver for written informed consent granted for the retrospective use of fully anonymised clinical data (Number KY2025K008). Participants gave informed consent to participate in the study before taking part.
References
Footnotes
Contributors LZ: conceptualisation, investigation, methodology, data curation, software, formal analysis, visualisation, writing—original draft. Z-KX: investigation, data curation, formal analysis, writing—review and editing. XW: methodology, writing—review and editing. JKZ: methodology, writing—review and editing. S-TH: data curation, writing—review and editing. Y-KZ: data curation, writing—review and editing. TSG: data curation, writing—review and editing. TL: supervision, validation, writing—review and editing. S-WR: supervision, validation, funding acquisition, writing—review and editing. K-YC: conceptualisation, funding acquisition, project administration, resources, supervision, writing—review and editing. All authors approved the final manuscript. K-YC is responsible for the overall content as guarantor.
Funding This study was supported by the Key Project of Tianjin Natural Science Foundation (Grant Number: 21JCZDJC01080), Academic Backbone of 'Clinical Talent Training and Climbing Plan' of Tianjin Medical University.
Competing interests This study received infrastructure support from Tianjin Medical University. The funding organisation played no role in study design, data collection, analysis, interpretation, manuscript preparation or publication decisions. All authors declare no additional competing interests.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer-reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.