Article Text

Abstract
Objectives To assess the demands for support measures of healthcare workers (HCWs) in China’s high-workload provinces during the COVID-19 pandemic and identify specific needs to make evidence-based recommendations.
Design Prospective cross-sectional study.
Setting Conducted in three Chinese provinces characterised by their significant healthcare demands during the pandemic.
Participants The study comprised 683 HCWs, including doctors, nurses, resident physicians and hospital administrators. The sample was predominantly female (68.1%), with the majority aged between 25 and 34 years. Participants were recruited through convenience and snowball sampling methods, with a focus on individuals working in high-intensity clinical environments.
Results Hierarchical analysis was performed to assess the layered impact of support measures across different roles and genders. Substantial gender disparity was observed, with female staff reporting significantly reduced access to material support (p<0.001), family counselling (p<0.001) and health management (p<0.05), alongside a generally higher demand for various support types. In contrast, HCWs assigned to COVID-19 units did not exhibit heightened needs for COVID-specific training (p<0.001), material support (p<0.001), stress management (p<0.001), family counselling (p<0.001) or rational shift patterns (p<0.001) compared with those in non-COVID-19-focused roles.
Conclusion The study identifies significant support deficiencies, particularly among female HCWs, and emphasises the necessity for targeted interventions to strengthen healthcare system resilience. Recommendations include prioritising adequate rest, equitable resource allocation and the implementation of gender-oriented policies to ensure workforce sustainability and maintain care quality. Further research should focus on longitudinal support dynamics.
- COVID-19
- Burnout
- HEALTH SERVICES ADMINISTRATION & MANAGEMENT
- Percieved Social Support
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The study addresses a critical gap by examining healthcare worker (HCW) support needs during a pandemic in high-workload settings, providing contextually relevant insights.
A diverse sample of clinical roles and genders was included, enhancing the understanding of role-specific and gender-specific challenges.
The focus on a high-intensity healthcare environment adds value to understanding systemic responses under significant operational stress. The use of convenience and snowball sampling methods may limit the representativeness of the findings across broader HCW populations.
The cross-sectional design provides a snapshot of HCWs’ support needs but does not capture longitudinal trends and evolving support needs over time.
Introduction
In late 2022, a resurgence of respiratory infections worldwide placed Chinese healthcare workers (HCWs) back in an immensely stressful and demanding work environment,1 once again, jeopardising their physical and mental well-being.
The WHO has emphasised the significance of safeguarding the health and safety of HCWs as an integral part of the health sector’s core operations.2 The American Medical Association advocates for Employee Assistance Programmes (EAPs)/Physician Assistance Programmes to ensure doctors and senior practitioners receive essential psychological support and access existing resources.3 Measures such as flexible scheduling, adequate breaks, robust managerial support, open channels of communication, involvement in decision-making and provisions for mental health resources and well-being to address work-related stress, including assistance with childcare or eldercare, are recommended to alleviate staffing shortages.4
In 2021, China issued guidelines for establishing a long-term mechanism for the protection, care and concern of medical personnel.5 These guidelines outlined the creation of a protective system covering six key areas: guaranteeing working conditions, maintaining physical and mental health, implementing professional title policies, enhancing humanistic care, creating a safe practising environment and promoting professional ethics to effectively guarantee the realisation of the rights and interests of HCWs.
Support measures6 refer to an array of policies, procedures and practices implemented within organisations to assist employees in managing work-related stress, enhancing job efficiency and satisfaction, fostering personal and professional growth and preserving their physical and mental well-being. National health departments and hospitals employ a wide range of strategies to support HCWs since the beginning of the COVID-19 pandemic,7 including comprehensive infection control training, adequate provision of protective gear, psychological counselling services, health management and optimised work and rest schedules. The necessity for such interventions has been validated by the elevated risks encountered during pandemics; however, it also potentially contributed to increased professional stress, burnout and compromised patient care quality.8 9
While these measures are critical for staff welfare, operational risk reduction and improved healthcare institution performance,10 reports from hospital assessments in 2020 and 2021 indicate minimal improvements in employee satisfaction, highlighting challenges in implementing support measures.11 12 These initiatives might face constraints due to logistical, financial and structural limitations. The diversity among medical staff roles necessitates a tailored approach to address the unique needs and stresses inherent to each role.
Before the pandemic, healthcare professionals primarily emphasised support needs concerning career development, workplace improvement and achieving work-life balance.13 14 However, COVID-19 dramatically altered the working conditions and pressures, intensifying the demand for support measures. The pandemic led to a surge in the need for personal protective equipment (PPE), such as masks, protective suits and goggles,15 to ensure safety while interacting with patients. Additionally, it amplified psychological strain, emphasising the urgency for mental health support.16–18 A systematic review on the mental health of HCWs in the COVID-19 pandemic found that the prevalence of stress among HCWs ranged from 29.8% to 62.99%,19 indicating HCWs faced aggravated psychological pressure and even mental illness during the pandemic. Moreover, the prolonged and demanding work hours, high-risk environments and uncertainties surrounding patient conditions contributed to significant psychological stress and trauma among HCWs.20 21 A substantial number of studies have demonstrated a correlation between the well-being of HCWs, including burnout, and the quality, safety and patient outcomes in a multitude of countries and care settings.22 23 Consequently, the attention of the administrations shifted towards protecting and supporting HCWs. While there is a general awareness and acknowledgement of the changing support needs during the pandemic,24 25 systematic research in this area is still insufficient. Given the persistent threat of COVID-19 and other emerging infectious diseases, it is crucial to identify and address potential gaps in the current support systems, warranting further research on the topic.
Various countries have implemented different support measures to mitigate these challenges. For example, a hospital in the UK introduced psychological support services including support groups on the wards, training workshops as well as one-to-one support to staff in line with the British Psychological Society (BPS) guidelines.26 And interventions like psychoeducational resources, phone support line and clinical treatment programme were provided at Montefiore Medical Center in the USA,27 which proved to be both validating and practically useful. In Italy, a multidisciplinary non-governmental initiative called Italian Response to COVID-19 was implemented to ensure HCWs’ safety and well-being.28 Nevertheless, the efficacy of these measures in high-workload settings remains poorly documented. As indicated in the China Health Statistical Yearbook 2022, medical personnel in Shaanxi, Jiangsu and Anhui exhibited elevated levels of burden workloads and average daily burdens.29 Therefore, we initiated a survey in the three Chinese provinces—characterised by high and comparable daily averages of outpatient visits and inpatient beds.30 This survey aimed to assess the implementation and demand for support measures among HCWs during the COVID-19 pandemic, discerning the specific needs of different medical personnel. According to the analysed results, we aim to provide guidance for healthcare institutions, policymakers and social service providers to better support HCWs, ensuring that they receive adequate protection and assistance during the pandemic and in potential future crises.
Methods
Data collection
This study was a prospective, cross-sectional study designed to assess the specific demands and support needs among healthcare professionals during the COVID-19 pandemic across three high-workload provinces of China. A combination of convenience and snowball sampling techniques was employed via an online survey platform (https://www.wjx.cn/vm/PQNSgoo.aspx) over a 45-day period from 3 January to 16 February 2023. Of the initial 691 participants, 683 responses passed quality control measures (see below) and were deemed suitable for analysis, resulting in a valid response rate of 98.84%.
Ethical considerations
This study was reviewed and approved by the Medical Ethics Committee of Xiamen University (XDYX202308K50). Participants were informed about the study’s purpose, content and their rights before completing the online questionnaire, ensuring that informed consent was obtained prior to participation. Participation was entirely voluntary, with the right to withdraw at any time without consequences.
To ensure participant protection, the study did not involve any interventions that could pose physical or psychological risks. Regarding data confidentiality, all collected data were fully anonymised, with no personally identifiable information recorded. Data were securely stored on a password-protected server and accessible only to authorised members of the research team. To further safeguard confidentiality, the dataset will be used solely for research purposes and will not be shared with third parties.
Patient and public involvement
HCWs were represented by their unions and professional bodies, which were involved in the development of the research instrument and the dissemination of the online survey. These representatives helped ensure that the survey addressed the relevant concerns of HCWs regarding the adequacy of protective measures, although the HCWs themselves were not directly involved in the study design.
Questionnaire
The self-designed questionnaire (online supplemental material 1) encompasses four key sections: (1) basic demographic information; (2) survey on medical staff’s needs for support measures: derived from previous surveys and national policies,31–33 eight prioritised support measures were selected for evaluation, including training related to COVID-19; material support: essential resources including PPE, medical supplies, nutrition and financial support which were needed to ensure HCWs’ safety, well-being and effective performance; psychological counselling; stress management; health management; sleep-assisted instruction; psychological counselling for family and rational shift patterns: a scheduling approach that ensures adequate rest and manageable work hours, aimed at preventing burnout and supporting HCW well-being. Demand level of these measures was categorised into five distinct tiers, ranging from unnecessary to necessary on a scale of 1 to 5. (3) Survey on the implementation of support measures for COVID-19 dedicated HCWs: assessed five support measures including material support, psychological counselling, stress management, health management and psychological counselling for family. (4) Open-ended question: ‘What are your current needs?’. The consistency test results of the questionnaire indicate that Cronbach’s alpha coefficient is 0.836, indicating high reliability of the questionnaire.
Supplemental material
Quality control
The minimum sample size required first has to be determined before the statistical model is established. The sample size calculation is shown below:
where n is the sample size,  value is 1.96 typically,
p
is the overall staff job satisfaction rate and
value is 1.96 typically,
p
is the overall staff job satisfaction rate and  is the desired level of precision. And then, we assumed 95% confidence and 5% precision. Based on previous surveys,34–36 the lowest satisfaction rate of HCWs was 25.62%. Therefore, the minimum sample size was 293. The questionnaire was developed through collaborative discussions among experts in evidence-based medicine, hospital infection control and public administration. Multiple rounds of feedback from frontline medical staff were incorporated. The online questionnaire can be accessed via the following link: https://www.wjx.cn/vm/PQNSgoo.aspx, and the responses of the participants were centrally summarised on the WJX.cn platform. All questions were mandatory, and any vacancy was considered as a waiver to withdraw from this survey. Two researchers independently reviewed the collected data to ensure accuracy and identify any logical inconsistencies. Exclusions were made for responses completed in less than 25 s or showing eight consecutive identical answers, resulting in 683 valid questionnaires eligible for further analysis.
is the desired level of precision. And then, we assumed 95% confidence and 5% precision. Based on previous surveys,34–36 the lowest satisfaction rate of HCWs was 25.62%. Therefore, the minimum sample size was 293. The questionnaire was developed through collaborative discussions among experts in evidence-based medicine, hospital infection control and public administration. Multiple rounds of feedback from frontline medical staff were incorporated. The online questionnaire can be accessed via the following link: https://www.wjx.cn/vm/PQNSgoo.aspx, and the responses of the participants were centrally summarised on the WJX.cn platform. All questions were mandatory, and any vacancy was considered as a waiver to withdraw from this survey. Two researchers independently reviewed the collected data to ensure accuracy and identify any logical inconsistencies. Exclusions were made for responses completed in less than 25 s or showing eight consecutive identical answers, resulting in 683 valid questionnaires eligible for further analysis.
Statistical analysis
The data were entered and subjected to statistical analysis using SPSS (V.24.0; SPSS Institute). Descriptive statistics were presented as frequency distributions and percentages, and χ2 tests were employed for inferential statistics. The Bonferroni correction was applied for pairwise comparisons. The Mann-Whitney U test was employed for comparing ordinal data between two groups, while the Kruskal-Wallis H test was used for comparing ordinal data across multiple groups. p<0.05 is considered to be statistically significant. A visual depiction of the responses to open-ended questions was conducted on R (V.4.2.0; R Institute) Package (wordcloud2).
Results
Demographic overview
The study comprised 683 participants (table 1), with a notable predominance of female participants, accounting for 68.1% (n=465), while male participants constituted 31.9% (n=218). Most of the participants were in the age group of 25–34 (43.9%, n=300), followed by those aged 35–44 (33.8%, n=231). In the departmental breakdown of HCWs, the preclinical sector comprised the plurality with 36.6% (n=250) of the participants, followed by nursing staff at 23.1% (n=158). The respondents were nearly equally divided between those working in environments focused on COVID-19 (48.0%, n=328) and those in non-COVID-19 settings (52.0%, n=355). Further statistical analysis highlights a striking gender disparity within the nursing category, with only four male nurses compared with 154 female nurses, reflecting the predominantly female composition of this group (table 2).
Baseline information
Gender and clinical role distribution among healthcare workers (HCWs)
Word cloud
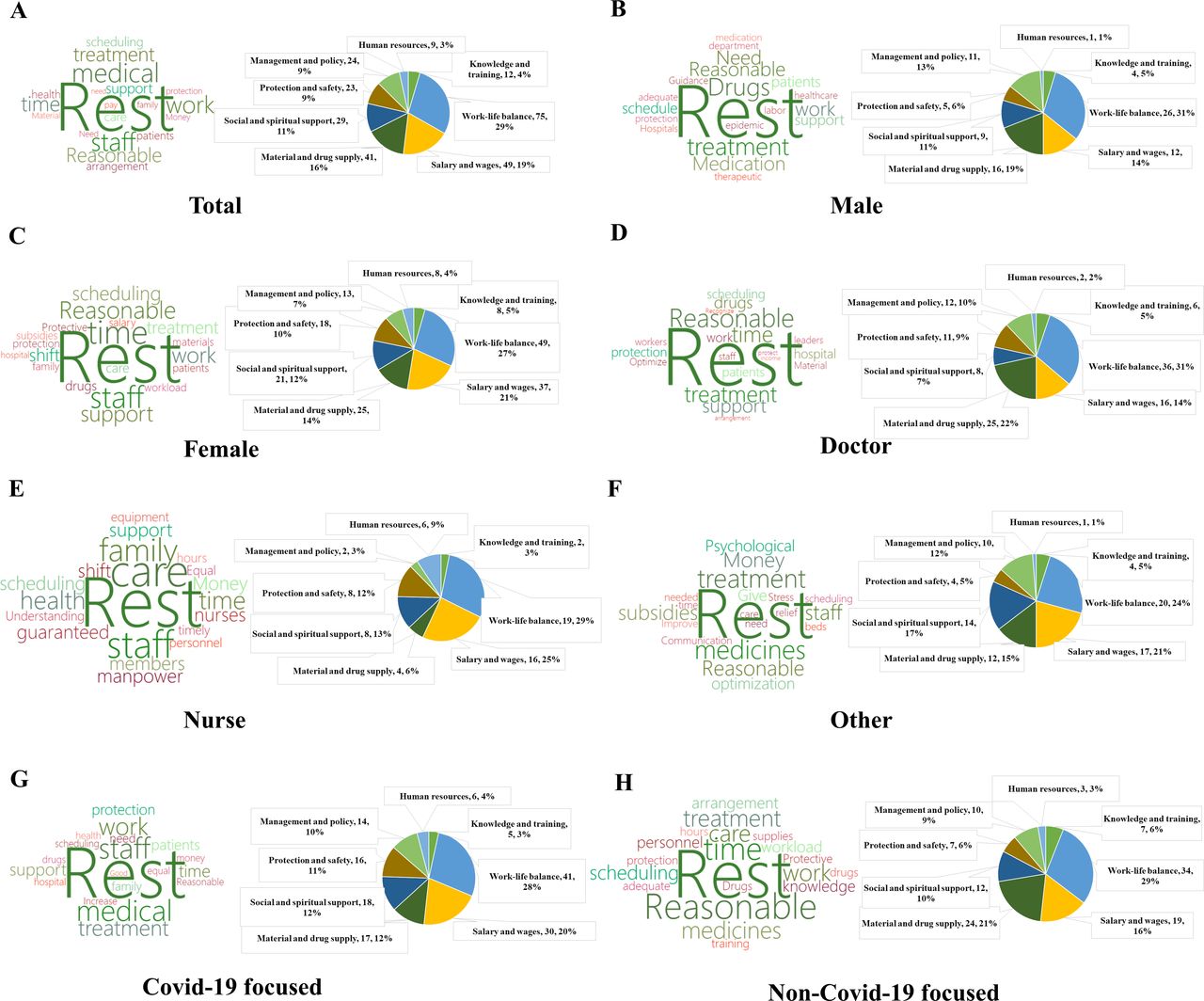
Out of the 683 survey respondents, 265 HCWs provided answers to the open-ended question regarding their current needs. The qualitative data were categorised, and a word cloud (figure 1) was generated, revealing prominent themes among respondents.

Word cloud and pie chart illustrating medical staff needs. The word cloud represents articulated needs extracted from responses provided by medical personnel categorised into different groups. Each word’s size within the cloud corresponds to the frequency of its occurrence, offering a visual representation of the predominant needs. The colour scheme used is for differentiation purposes only and does not carry interpretative significance. The accompanying pie chart illustrates the relative proportions of various identified needs among medical staff.
According to the word cloud, ‘rest’ is a pervasive need among all HCWs. Additionally, recurring terms such as ‘medication’, ‘reasonable’, ‘care’, ‘employees’ and ‘money’ indicate critical areas of concern. Further classification of these needs highlights widespread challenges in balancing work and rest, coupled with dissatisfaction regarding wages, subsidies and the availability of pharmaceuticals. Notably, female HCWs, nurses, personnel in various staff positions and those primarily engaged in COVID-19-related work expressed a considerable demand for salary increases, constituting over 20% of the feedback in these categories.
Differences in support measures for COVID-19 dedicated healthcare workers
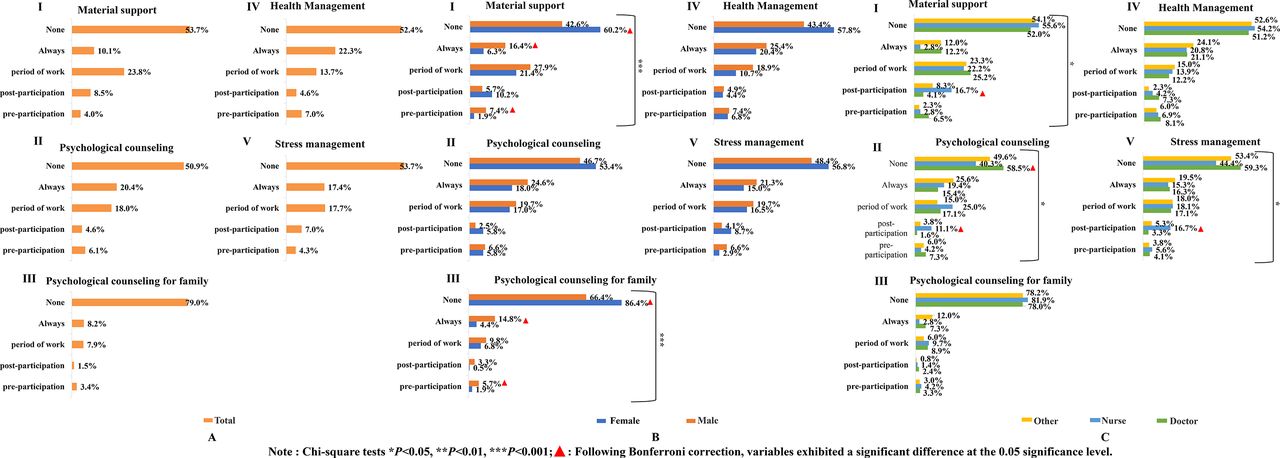
The analysis highlighted disparities in the provision of support measures for COVID-19-focused medical staff. As shown in figure 2, more than half of the medical staff reported a lack of access to these five support measures (figure 2A).

Disparities in implementation of support measures among COVID-19-focused health professionals. The choices of COVID-19-focused health professionals, categorised into various subgroups indicated by different colours, were first subjected to a descriptive frequency analysis. This was succeeded by a χ2 test to assess the disparities in frequency occurrences, with statistical significance denoted by asterisks to indicate the magnitude of p values and red triangles highlighting significant differences as determined by the Bonferroni test at the 0.05 level of significance. Chi-square tests *P<0.05, **P<0.01, ***P<0.001;  : Following Bonferroni correction, variables exhibited a significant difference at the 0.05 significance level
: Following Bonferroni correction, variables exhibited a significant difference at the 0.05 significance level
Female staff reported lower access to material support compared with their male colleagues (χ²=21.010, p<0.001), with more than 60% of females claiming not to receive this support (figure 2B-I). What is more, there are also disparities in material support across clinical roles (χ²=16.875, p<0.05), with a higher proportion of nurses receiving this support after participation (figure 2C-I).
Additionally, psychological counselling support varied among clinical roles (χ²=18.961, p<0.05), with a notable proportion of doctors not receiving any psychological counselling (figure 2C-II). Psychological counselling for HCWs’ family members showed a gender-based discrepancy (χ²=22.033, p<0.001), a higher percentage of females lacking this support compared with males (figure 2B-III). Surprisingly, this support was infrequently accessible across clinical roles (figure 2C-III).
Health management support showed no gender-related differences (χ²=7.584, p>0.05), yet females reported lower levels of health management support (figure 2B-IV). Similarly, no significant differences were seen across clinical roles (χ²=4.805, p>0.05) (figure 2C-IV).
Gender showed no significant impact (χ²=7.917, p>0.05) on stress management support (figure 2B-V). However, considerable differences were observed across clinical roles (χ²=15.560, p<0.05), notably with a higher percentage of doctors not receiving this type of support (figure 2C-V).
Medical staff perceptions of COVID-19-related support measures
Health workers regarding different genders, medical roles and whether their focus was on COVID-19 had different attitudes towards the provision of relevant support measures during COVID-19 (figure 3). Significant differences were observed based on gender (χ²=12.412, p<0.05) and whether COVID-19-focused (χ²=55.334, p<0.001), with females and non-COVID-19-focused staff emphasising the need for COVID-19-related training (figure 3B-I,C-I).

{kind=link}
{kind=link}
{kind=link}
Discrepancies in demand for support measures among health professionals. The choices of health professionals, categorised into various subgroups indicated by different colours, were first subjected to a descriptive frequency analysis. This was succeeded by a χ² test to assess the disparities in frequency occurrences, with statistical significance denoted by asterisks to indicate the magnitude of p values and red triangles highlighting significant differences as determined by the Bonferroni test at the 0.05 level of significance. Chi-square tests *P<0.05, **P<0.01, ***P<0.001;  : Following Bonferroni correction, variables exhibited a significant difference at the 0.05 significance level.
: Following Bonferroni correction, variables exhibited a significant difference at the 0.05 significance level.
Material support had no significant difference between genders (χ²=5.307, p>0.05) (figure 3B-II), but a difference was noted between those in COVID-19-focused (χ²=44.034, p<0.001), with a majority of respondents in COVID-19 considering the material support to be necessary or extremely necessary (figure 3C-II).
Stress management analysis revealed significant disparities between genders (χ²=39.207, p<0.001) and COVID-19 focus (χ²=151.048, p<0.001), with a larger proportion of females and COVID-19 focus staff rating stress management to be extremely necessary (figure 3B-II,C-II).
Psychological counselling showed gender differences (χ²=18.337, p<0.01), with a greater percentage of females considering it necessary or extremely necessary (figure 3B-IV). Clinical roles also showed significant differences (χ²=16.803, p<0.05) regarding the perceived necessity of psychological counselling (figure 3D-IV).
The need for psychological counselling for family members did not exhibit significant gender differences (χ²=6.862, p>0.05) (figure 3B-V) but did show differences between COVID-19-focused and non-focused staff (χ²=19.018, p<0.01), with non-COVID-19-focused staff considering it more necessary (figure 3C-V).
Significant gender differences were noted in health management (χ²=25.976, p<0.001), with females rating it as more necessary (figure 3C-VI). Rational shift patterns did not differ by gender (χ²=7.972, p>0.05) or clinical role (χ²=5.646, p>0.05) but showed differences based on COVID-19 focus (χ²=15.947, p<0.01), with non-COVID-19-focused staff considering it more necessary (figure 3C-VII).
Significant gender-based differences were observed (χ²=16.832, p<0.001) with females considering it more necessary (figure 3B-VIII).
The demands for different support measures of healthcare workers
In examining the perceived necessity of various COVID-19 support measures among medical staff, our analysis revealed several significant findings (table 3).
Support measures necessity by gender, COVID-19 focus and clinical role
Females demonstrated higher needs compared with males in COVID-19-related training (Z=−3.343, p<0.001), stress management (Z=−5.379, p<0.001), psychological counselling (Z=−3.522, p<0.001), health management (Z=−4.431, p<0.001), rational shift patterns (Z=−2.124, p=0.034<0.05) and sleep-assisted instruction (Z=−3.786, p<0.001).
COVID-19-focused HCWs exhibited higher needs compared with non-COVID-19-focused health workers in COVID-19-related training (Z=−7.044, p<0.001), material support (Z=−6.546, p<0.001), stress management (Z=−12.097, p<0.001), psychological counselling for family (Z=−3.544, p<0.001) and rational shift patterns (Z=−3.706, p<0.001).
Various clinical roles displayed a consistent level of need for all support measures, except for differences in the level of need for psychological counselling (H=−8.222, p=0.016<0.05).
Discussion
The enduring impact of the COVID-19 pandemic has imposed unprecedented challenges on healthcare professionals, placing them at the forefront of the battle against the virus, not only in their professional capacities but also in their personal lives. Initial data indicate that various Chinese national ministries and commissions swiftly issued 14 policies aimed at supporting frontline medical workers within a month of the epidemic in 2020.31–33 The majority of these policies, comprising 11 logistical support initiatives and four protective measures, primarily emphasise immediate concerns. However, an analysis of these policies reveals a discernible gap between the articulated needs of frontline medical staff and the actual provisions made.37 While these policies commendably underscore the importance of remuneration and recognition for frontline workers, they are misaligned with the needs identified in surveys. Notably, the emphasis on protective measures overshadows critical aspects such as psychological and family support,38 but there is still a lack of specialised and systematic intervention strategies.38 39 There is a notable absence of attention towards aspects such as professional insurance, skill training, psychological impact factors, mental health changes, family health protection and public education. Moreover, proactive intervention strategies targeting the mental well-being of HCWs are largely lacking.
While these policies were introduced in a timely manner, they predominantly offer short-term solutions without adequately considering sustainable mechanisms. The absence of long-term strategies, such as establishing a safe practice environment and fostering personal career development, remains a critical lacuna in these policies.
This study aims to evaluate the efficacy of support initiatives extended to medical personnel during the pandemic, focusing on their implementation and aligning them with healthcare staff’s actual needs. By discerning precise demands and their breadth among healthcare professionals, our findings have informed the following recommendations.
Ensuring adequate rest for healthcare workers
In our survey, we identified adequate rest as a fundamental need for all HCWs. Prepandemic studies40–42 have consistently highlighted the elevated risk of sleep disorders among healthcare professionals compared with the general population due to demanding shift work, high job intensity and challenging working conditions. These factors contribute to chronic sleep deprivation, leading to a spectrum of physical and mental health issues,43 44 including chronic pain, headaches and fatigue. The pandemic has exacerbated the incidence of sleep disorders and poor sleep quality among HCWs, intensifying the urgency to prioritise rest. Notably, our survey findings reveal a heightened risk of sleep disorders among female healthcare professionals, nurses and individuals holding lower professional titles. Research45 46 corroborates this, indicating that unconventional shift patterns, particularly night shifts, substantially escalate the risk of both reproductive health issues and sleep disorders among these specific groups.
Given the pivotal roles these individuals play in critical healthcare functions such as nursing, clinical and laboratory work in the fight against the pandemic, implementing targeted support measures becomes imperative. Strategies centred around sleep guidance and stress management are crucial to improving sleep quality and ensuring adequate rest, especially among female HCWs.
Ensuring the equitable implementation of support measures across different genders
During the COVID-19 pandemic, disparities in the allocation of support measures for HCWs were pronounced.47 48 Our survey revealed significant discrepancies in material support among different clinical roles, suggesting a fragmented approach to resource distribution. Physicians, nurses and other healthcare professionals reported varying levels of support, reflecting the hierarchical nature of the medical system and differing perceptions of needs across roles. These disparities underscore the urgency for a more coordinated and equitable resource allocation strategy to ensure that all clinical staff have access to essential materials required for safe and effective job performance.
Of great concern is the notable absence of psychological counselling for a significant portion of the workforce amid the high-pressure environment during the pandemic. It is imperative that psychological health support becomes universally accessible to all healthcare personnel, irrespective of their specific clinical role. The survey revealed that female staff reported lower levels of material support compared with their male counterparts, coupled with inadequate stress management, health support and a lack of psychological counselling services for their family members. These gender-based discrepancies might emanate from systemic biases or disparities in job roles and functions.49
The under-representation of women in higher-status positions within healthcare institutions exacerbates this inequality, emphasising the need to address such disparities to foster an equitable and supportive work environment for all staff. Establishing a robust legal framework to combat discriminatory practices in healthcare and empowering women to assume leadership roles within health organisations are crucial steps toward enhancing female visibility, acknowledging and rewarding women in leadership and nursing roles and nurturing women’s confidence, resilience and independence.50 51
Initiatives such as gender-specific leadership training, peer mentoring programmes and flexible work policies can significantly bolster women’s agency and decision-making power within healthcare settings.52–54
Optimising support measures for healthcare workers considering event characteristics
The global COVID-19 pandemic has been characterised by its extensive spread, large affected population, prolonged duration and frequent viral mutations.55 These characteristics offer insights for potential future public health emergencies, emphasising the significance of optimising support measures for HCWs to enhance medical services. This study’s comparative analysis of the needs between those actively involved in epidemic control and those not engaged in such activities revealed a higher demand for various support measures among the latter. This indicates that HCWs exhibit increased requirements for support measures before entering high-pressure work environments, highlighting the necessity of implementing support and incentive policies proactively before the onset of epidemic duties. Extending support measures throughout the middle and later stages of an epidemic, with initial support acting as supplementary, can effectively sustain HCWs’ motivation.56
Interestingly, our survey indicated a disproportionately low demand for stress management among the group not involved in epidemic control, possibly signalling an overestimation of their psychological resilience and stress-coping abilities. Research57 58 related to the EAP during the pandemic highlighted the importance of implementing stress management initiatives before the onset of a crisis. Acknowledging the harsh realities of the work environment and preparing for the consequent psychological and physical stress could better mitigate adverse mental health outcomes.
However, many HCWs in this survey reported participating in multiple online and offline mental health surveys. They complained that these surveys often include numerous psychological scales, which are time-consuming and provide no actual benefit to their mental health, even raising concerns about being referred for psychological counselling.55 59 Moreover, in our study, both groups of HCWs, involved and not involved in epidemic control, demonstrated a lower demand for psychological counselling services compared with other forms of support. Similarly, research by Chen et al 60 suggested that during an epidemic, HCWs prioritise assurances related to food and rest over psychological support, signalling a preference for logistical and material support.
In light of these insights, decision-makers should prioritise enhancing logistical and material support for HCWs engaged in high-pressure environments, instead of solely focusing on psychological health guidance. This nuanced approach aligns support measures with the distinct needs and preferences of HCWs during challenging work scenarios.
Improving comprehensive support measures for healthcare workers considering regional characteristics
While our survey focused on regions with relatively advanced medical resources, it is crucial to recognise the challenges faced by healthcare facilities in less economically developed areas. These regions often grapple with shortages in materials, manpower and financial resources, posing significant hurdles in providing adequate support measures.61 Institutions in these areas may contend with lower management levels due to limited funding, lacking standardised procedures, clear delineation of responsibilities and assessment mechanisms. These limitations curtail their ability to safeguard the rights of HCWs and impede the provision of necessary support measures.62 63
Moreover, the relative imperfections in the healthcare system exacerbate the challenges for HCWs, subjecting them to substantial work pressure and risks without effective safeguards or support. Furthermore, the lack of awareness among the local public regarding the invaluable contributions of HCWs, coupled with insufficient respect and understanding,64–66 compounds the obstacles in providing adequate care measures to healthcare staff. This discrepancy in the distribution of medical resources across regions and institutions results in some facilities being unable to deliver quality medical services and essential support measures.
Comparative analysis of global support strategies for healthcare workers: lessons and recommendations
Support measures for HCWs vary significantly across regions and countries, reflecting tailored responses to local healthcare challenges and resource availability. In order to assist HCWs in coping with stress, China established hotlines and peer support groups,67 as well as providing hotels for HCWs and their families to minimise risk.68 Financial incentives, including bonuses and hazard pay, were provided to frontline workers in Italy.69 Additionally, supported well-being centres have been set up in UK hospital trusts in an effort to mitigate the psychological impact of COVID-19 on HCWs, and the UK government mandated that the education sector organises free childcare for essential workers, which has proved instrumental in addressing work-life balance concerns.70 71
Nevertheless, there were still significant deficiencies in the implementation level for the support measures. Our survey revealed critical gaps between the support HCWs received and their perceived needs, highlighting a fragmented resource distribution influenced by the hierarchical structure of the medical system, further exacerbated by untimely and non-transparent communication of feedback. These challenges are not unique to China but resonate globally. A narrative review revealed that the majority of psychological support programmes lacked long-term sustainability plans, which are essential for effective long-term mental health support.72 And another systematic review noted that many countries implemented interventions to ensure adequate PPE supply and training, but the effectiveness of these measures varied significantly based on local management and communication practices.73 This underscores the potential of a data-driven approach to enhance responsiveness to evolving demands and bolster overall safety for HCWs. Effective communication was also linked to increased security and teamwork among HCWs, which highlights the significance of establishing robust communication platforms such as regular town hall meetings or anonymous surveys that can ensure that staff concerns are addressed promptly.74
Conclusion
The diverse needs of HCWs underscore the importance of addressing critical issues in support measures. Particularly, ensuring equitable and high-quality support for female medical staff remains paramount. Optimising the implementation timeline and sequence of these measures, considering regional disparities and the challenges faced by less economically developed areas, is essential. Overcoming the hurdles in the comprehensive rollout of support initiatives is crucial for bolstering the well-being and resilience of healthcare professionals in varying healthcare settings.
Applicability and limitations
Applicability
The findings from this study hold practical implications for healthcare institutions and policymakers, particularly in managing the well-being of healthcare professionals amidst public health crises. Pinpointing specific support needs can serve as a blueprint for tailored interventions aimed at alleviating challenges encountered by medical staff. Leveraging this insight, institutions can revamp workplace protocols, optimise resource distribution and augment support services to align with the healthcare workforce’s needs. Addressing highlighted gaps, such as the need for adequate rest, material support, psychological counselling and optimised work schedules, can fortify the resilience and effectiveness of healthcare professionals. Furthermore, these insights can lay the groundwork for strategising and preparing for future pandemics, ensuring a resilient and adaptable healthcare workforce.
Limitations
This study’s limitations are chiefly associated with its sampling methods and scope. The utilisation of convenience and snowball sampling might curtail the generalisability of findings across all healthcare professionals in China or other regions, potentially limiting representation. Focusing solely on three Chinese provinces may overlook regional variations in support measures and needs. Additionally, the study’s cross-sectional design offers a singular snapshot in time, not capturing the dynamic changes in support needs over the pandemic’s course. Subjectivity in survey responses introduces the likelihood of response bias, affecting the accuracy of reported experiences and needs. Future research could mitigate these limitations by employing diversified and stratified sampling approaches, engaging longitudinal studies to track evolving needs and broadening the geographical scope to encompass a more diverse range of healthcare settings.
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. The investigation was reviewed by the Medical Ethics Committee of Xiamen University (XDYX202308K50). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors extend their sincere gratitude to the medical staff from the following institutions for their substantial support: the affiliated hospital of Nanjing Medical University, the affiliated hospital of Xi'an Jiao Tong University and the affiliated hospital of Xiamen University, among others.
References
Footnotes
LW, JZ and NH contributed equally.
Contributors LW: conceptualisation, data curation, formal analysis, investigation, methodology, software, validation, visualisation and writing – original draft. JZ and NH: project administration, resources and writing – original draft. WX and YF: conceptualisation, formal analysis, investigation, validation and writing – review and editing. SM, HX, YL and DG: investigation and writing – review and editing. LZ: funding acquisition, project administration, resources, supervision and writing – review and editing. LZ is the guarantor of this study and accepts full responsibility for the work, had access to the data and controlled the decision to publish.
Funding This work was partly supported by the Research Project on Teaching Civics in the Curriculum of Xiamen University (JG20240824).
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.