Article Text

Abstract
Objective This study was conducted to evaluate the causal analysis of undernutrition among adolescents in the context of the agrarian community of North-West Ethiopia.
Design A community-based case-control study was conducted among 149 cases and 297 control adolescents.
Setting Agrarian communities of North-West Ethiopia.
Participants Adolescents aged 10–19 years, who reside in a randomly selected study setting.
Outcome measures The stunting and thinness nutritional status of adolescents was determined using the WHO AnthroPlus 2010 software. A general structural equation modelling approach was used to determine a multicausal analysis of undernutrition. The Food Frequency Questionnaire was tested for internal reliability among 30 adolescents. The reliability test for the actual dietary tool was done using Cronbach’s alpha coefficient (α), which was 0.79. The model adequacy was tested using the Akaike information criterion and Bayesian information criterion. The significant direct and indirect determinants were identified with a value of p<0.05.
Result Adolescents with lower traditional and mixed dietary pattern consumption habits were determinant factors for stunting with adjusted β=0.65, 95% CL (0.143 to 1.159) with a value of p=0.012, adjusted β=2.697, 95% CL (0.563 to 4.831) with a value of p=0.013, respectively. Breakfast eating frequency had a negative indirect determinant factor on the reduction of stunting via lower traditional habits, with adjusted β=−0.207 (−0.299 to–0.116) with a value of p=0.001, and higher consumption habits of animal sources with traditional alcoholic drinking habits with adjusted β=−0.163, 95% CL (−0.260 to –0.065) with a value of p=0.001. Whereas breakfast eating frequency had a direct influence on thinness with adjusted β=−0.332, 95% CL (−0.588 to –0.076) with a value of p=0.011, and an indirect influence via dietary patterns for both stunting and thinness (p<0.05).
Conclusion Dietary patterns and breakfast-eating frequency were direct and indirect determinant factors for adolescents’ stunting and thinness. Public health interventions should be implemented to reduce stunting and thinness by improving the dietary feeding and breakfast consumption habits of adolescents and strengthening the national deworming programmes in study areas and similar settings.
- Adolescents
- NUTRITION & DIETETICS
- Public health
- Body Mass Index
Data availability statement
Data are available upon reasonable request. Data are included within the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
Using a robust statistical model to identify direct and indirect determinants of undernutrition.
A validated Food Frequency Questionnaire was used to ensure data quality.
As a limitation of this study is the inability to identify all food items like spices.
The identified dietary patterns did not triangulate with biomarker levels of nutrients.
Introduction
Adolescence is a transitional period characterised by physical, cognitive, emotional and social changes that lay the foundation for later life, health and well-being.1 2 Adolescence is the most appropriate time to develop positive health behaviours that can continue throughout life. At the same time, it is the most vulnerable period in terms of the development of diseases that can be seen in adulthood.3 Adolescents encounter different problems that threaten their health during their growth and development stages. The main nutritional problems of adolescents living in developing countries are malnutrition, obesity and other chronic diseases, and inadequate, unhealthy eating habits and lifestyle.4 5
Undernutrition among adolescents is a serious public health issue in developing nations in Asia and Africa.6 7 Undernutrition affects 36.00% of adolescents in South Asia. In Ethiopia, from 12.60%–58.30% of adolescents were thin, and 12.50%–33.10% of adolescents were stunted.8–11 This figure indicates that undernutrition among adolescents is one of the most important public health problems in Ethiopia.12 13
Adolescent undernutrition is affected by multifaceted and complex inter-related factors that range from basic, underlying and immediate causes.14 15 Studies conducted in different settings identified various factors for undernutrition among adolescents. Some of the commonly reported determinants of undernutrition are being a rural resident, early age of adolescents, household food access and availability, household wealth status, inadequate meal frequency, lack of safe water for drinking, low diet diversity and suboptimal access to nutrition and health information.9 10 16
Adolescent undernutrition has been identified as one of the priority areas that require an immediate response. However, there is a lack of a comprehensive study on multicausal determinants of undernutrition in the study setting through a causal pathways approach.14 17 Identifying the direct and indirect individual, household and community-level determinants of adolescent undernutrition would allow policymakers to design integrated public health interventions.14 18 Therefore, this study was conducted to identify causal determinants of undernutrition in the study area to generate evidence for public health action.
Materials and methods
Study settings and target population
A community-based case-control study was conducted among adolescents from agrarian communities in randomly selected kebeles of Dembecha district, North-West Ethiopia. The data were collected from 10 January to 30 February 2022. The study area consists of three agro-ecological zones (lowlands, midlands and highlands) which are conducive to diversified agricultural production.
Adolescents aged 10–19 years who were residing in Dembecha district were the source population for this study. The study population comprised adolescents who were residing in randomly selected study sites or kebeles (the lowest administrative level in the case of Ethiopia) from the study district. This age group has often been overlooked for nutrition interventions in developing countries, including Ethiopia, as well as in the current setting. Therefore, this study was conducted to generate evidence for designing nutrition interventions for public health action. Adolescents with spinal curvature who could not stand properly and who used a wheel chair were excluded from the study.
Sample size determination and procedures
The required sample size was determined by a double population proportion formula using Epi Info V.7 by assuming a 95% confidence level and a 59.7% proportion of control exposed in the low wealth index category for stunting,16 A case-to-control ratio of 1:2, and adding a 10% non-response rate. The final sample size was 149 cases and 297 controls, with a total sample of 446.
The study area was purposively selected due to its three unique agro-ecologies (lowlands, midlands and highlands), which are representative of the entire north-west region of the country. Next, two research settings, or kebeles (the lowest administrative unit in the case of Ethiopia), were randomly selected from each agro-ecological zone for data collection.
In each study setting, eligible households that had at least one adolescent were surveyed and registered, and a sampling frame was prepared. Before conducting a case-control study, a first cross-sectional survey was conducted to determine nutritional status to identify cases and controls among adolescents. Then, one case of stunting and two consecutive controls were selected from each study setting for further interviews.
Data collection tools and measurement
A pretested, structured, interviewer-administered questionnaire was used for data collection. The tool was adapted and customised to the local context from peer-reviewed articles and also from the UNICEF conceptual framework. This questionnaire was organised to collect basic, underlying and immediate factors for adolescent undernutrition.19
Data on the dietary patterns of adolescents were collected using a validated Food Frequency Questionnaire (FFQ) contextualised to the setting over one week. The FFQ is a validated and less expensive tool to measure habitual diets (dietary patterns) with serum biomarkers and other dietary assessment methods of a population.20 21 For the current study, the FFQ assessment tool was developed as follows. First, a list of local food items that were consumed by adolescents at different times of meals and snacks was collected by conducting a pilot study on 30 adolescents for two non-consecutive weekdays and 1 weekend day.2 22 The FFQ was organised in a semiquantitative manner and administered using 24-hour dietary recall methods. Adolescents’ anthropometric data of weight and height were measured using a standard weight and height scale with precisions of ±0.1 kg and ±0.1 cm, respectively, based on WHO protocol.23 During measurement, adolescents wore lightweight clothing without shoes to minimise error. Trained human nutrition graduates collected data through interviews and anthropometric measurements.
Data quality control
To ensure data quality, the data collection tool was translated from English to the Amharic version (local language). A 1 day training was given for data collectors and supervisors on the objective, procedures and data collection technique by the principal investigator. A pretest was done on 5% of study participants outside of the study area; an amendment to the questionnaire was performed based on the findings of the pretest. In addition, before conducting the actual dietary data collection from each sample, the FFQ was tested for internal reliability among 30 adolescents. The reliability test for the actual dietary tool was done using Cronbach’s alpha coefficient (α), which was 0.79. This α indicated that the FFQ is internally reliable to measure the dietary patterns of adolescents. During the measurement of anthropometric data (weight and height), frequent calibration of instruments was done at the end of each measurement. In addition, local food-coloured pictures were used to minimise recall bias.
Outcome measurement
Adolescents stunting (case)
Adolescents stunting was determined using height for age (HAZ) and computed using WHO Anthro Plus software.24 To classify nutritional status, HAZ-scores <−2 SD were categorised as stunted and <−3 SD were categorised as severe stunting.24
Adolescents’ thinness
Adolescents’ thinness was determined based on body mass index (BMI) for age Z-scores. BMI for age Z-scores <−2 SD was categorised as thinness, and >+1 SD was categorised as overweight/obese using the WHO cut-off points.23
Dietary patterns
Exploratory factor analysis was conducted to determine key dietary patterns from consumption data based on its factor load. Based on the score, different dietary patterns were developed.25 26 Then each dietary pattern was classified into quartiles (Q) based on their contribution to each pattern and assuming an increasing order from Q1 to Q4.27 Finally, Q1 and Q2 were combined to represent low consumption habits while Q3 and Q4 represented high consumption dietary habits.2
Dietary diversity
Dietary diversity was assessed based on Food and Agriculture Organization tools that measure women’s dietary diversity. Food, consumed by adolescents, was assessed using a 24-hour recall method, and then food items were categorised into 10 food groups. A Dietary Diversity Score was created as a summary measure of dietary intake.28
Traditional dietary pattern
In this study, traditional dietary patterns described the traditional home-made and legume-based diets, which include local diets such as injera, injera with wot as sauces with added salt, spices, and oils in the local area.29
Mixed dietary pattern
A mixed dietary pattern includes the habit of consumption of a mixed diet that includes whole grains, high-carbohydrate food items, fruits and vegetables.29
Animal source and alcoholic drinking dietary pattern
This includes the consumption habit of a diet from animal sources (meat, eggs, milk) and traditional homemade alcoholic beverages such as tella (a traditional fermented alcoholic drink), areki or katikala (traditional distilled alcoholic beverages).29
Data analysis
Data were entered and cleaned using SPSS V.25 software and exported to STATA V.17 for further analysis. Descriptive statistics was conducted to describe the study population with relevant variables. Exploratory data analysis was conducted to check the potential outliers and normality of distribution for continuous variables. For wealth index of households was measured using principal component analysis. The modal assumption was checked and finally classified into thirds for categorisation.30
Adolescents’ stunting and thinness were determined based on HA and BMI for age Z-scores, respectively, computed using WHO Anthro Plus software.23 24 Exploratory factor analysis was conducted to derive major dietary patterns based on the consumption data after checking for basic assumptions.
The General Structural Equation Modelling (GSEM) overcome this limitation of structural equation models that require normally distributed data for analysis.31 In GSEM, it is possible to have a model with both continuous and discrete variables grouped together. As such, GSEM combines the power and flexibility of both SEM and Generalised Linear Model (GLM) in a unified modelling framework. The advantages of GSEM are (1) To evaluate potential causal relationships with the structural model; (2) To consider both direct and indirect multiple interacting factors simultaneously; and (3) The possibility of using appropriate probability density functions other than the normal one for manifest indicators and latent constructs.31–33
The GSEM was used to determine factors associated with each domain of determinant factors that influence stunting and thinness. The factors that affect undernutrition were classified as count, continuous, ranked, and categorical, with Poisson, Gaussian, ordinal, and binomial distributions for each domain of variables (online supplemental material).
Supplemental material
Finally, using appropriate link functions corresponding to each variable and outcome type. Therefore, GSEM is an appropriate approach used to identify direct and indirect determinant factors through causal analysis. The GSEM model was fitted in a stepwise process to identify the direct, indirect and total influence that affects undernutrition. The first hypothesised model was constructed as shown in figure 1, and the final fitted model was also shown in figures 2 and 3. To select fitted GSEM model adequacy, it was tested using Akaike information criterion (AIC) and Bayesian information criterion (BIC), based on scores of AIC=2128.88 and BIC=2283.83 for the hypothesised model and AIC=2843.60 and BIC=2953.70 in the fitted model. The scores of AIC and BIC in the hypothesised model and the fitted model were reduced, which indicates the model fitted for analysis. Finally, the fitted GSEM model was run to measure the direct and indirect determinants on stunting and thinness in the final specified model based on their level of significance. Significant determinant factors were identified based on a value of p<0.05.

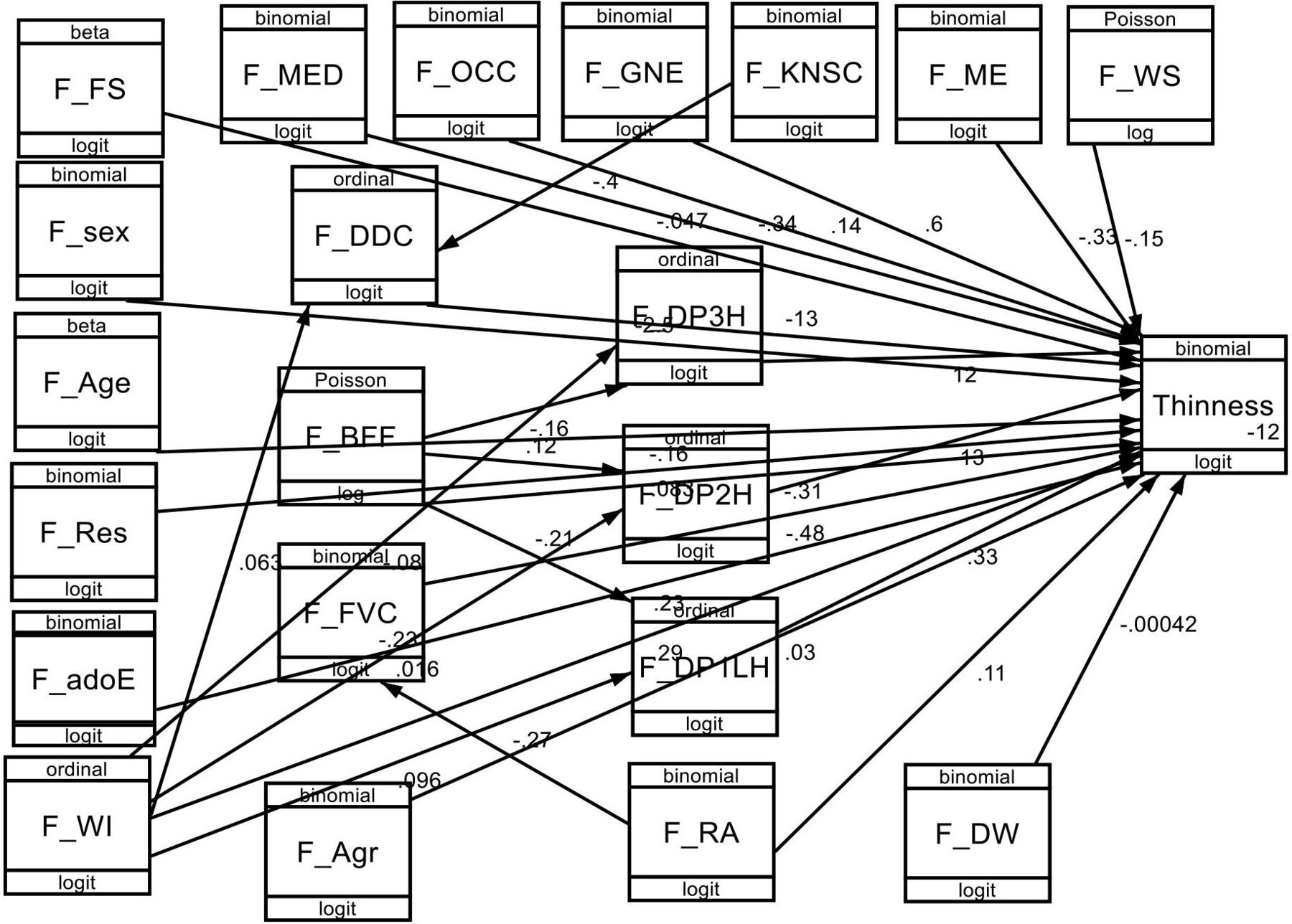
Hypothesised model on causal analysis of determinants of undernutrition among adolescents in the context of the agrarian community of North-West Ethiopia, 2021. F-Letter represents factor; F_adoE, adolescent educational status; F_age, age of the adolescent; F_Agr, agro-ecology; F_BFF, breakfast eating frequency; F_DDC, dietary diversity; F_DP1LH, traditional dietary pattern; F_DP2H, mixed dietary pattern; F_DP3H, animal sources with traditional alcoholic drinking dietary pattern; F_DW, deworming; F_FS, family size; F_FVC, fruit and vegetable consumption; F_GNE, getting nutrition education; F_KNSC, knowledge of nutrition; F_ME, having media exposure; F_MED, adolescent mother educational status; F_OCC, adolescent family occupation; F_RA, irrigation land access; F-Res, residence; F_sex, sex of adolescent; F_WI, ealth ndex; F_WS, wearing shoes.

Fitted model for causal analysis on determinants of stunting among adolescents in the context of the agrarian community of North-West Ethiopia, 2021. F-Letter represents factor; F_age, age of adolescent; F_BFF, breakfast eating frequency; F_DDC, dietary diversity; F_DP1LH, traditional dietary pattern; F_DP2H, mixed dietary pattern; F_DP3H, animal sources with traditional alcoholic drinking dietary pattern; F_DW, deworming; F_FVC, fruit and vegetable cultivation; F_KNSC, knowledge of nutrition; F_ME, having media exposure; F_RA, irrigation and access; F_Sex, sex of adolescent; F_WI, Wealth Index; F_WS, wearing shoes.

{kind=link}
{kind=link}
{kind=link}
Fitted model for causal analysis of thinness among adolescents in the context of agrarian community of North-West Ethiopia, 2021. F-Letter represents factor; F_adoE, adolescent educational status; F_Age, age of adolescent; F_Agr, agro ecology; F_BFF, breakfast eating frequency; F_DDC, dietary diversity; F_DP1LH, traditional dietary pattern; F_DP2H, mixed dietary pattern; F_DP3H, animal sources with traditional alcoholic drinking dietary pattern; F_DW, deworming; F_FS, family size; F_FVC, fruit and vegetable cultivation; F_GNE, getting nutrition education; F_KNSC, knowledge of nutrition; F_ME, having media exposure; F_MED, adolescent mother educational status; F_OCC, adolescent family occupation; F_RA, irrigation land access; F-Res, residence; F_Sex, sex of adolescent; F_WI, Wealth Index; F_WS, wearing shoes.
Patient and public involvement
The study participants were not involved in the development of the research question, outcome measures, design, recruitment or conduct of the study.
Results
Sociodemographic characteristics of the study participants
The mean (±SD) age of the participants was 14.36±1.76 years. Almost a fifth (18.30%) of the adolescents were at the early adolescent stage (10–13 years), 69.50% of them were between 14 years and 17 years, and the remaining 12.20% were in the late adolescent stage (18–19 years). There was no significant difference in the proportion of stunted adolescents across the different sociodemographic characteristics except adolescents sex and age (p<0.05) (table 1).
Cross-tabulation of sociodemographic characteristics of adolescents and their families, with adolescents’ nutritional status, North-West Ethiopia, 2021
Causal analysis of determinants of adolescents’ stunting
The first GSEM model was fitted based on the hypothesised model to identify determinants of stunting. Then, based on the model assumptions, a test of a fitted model for causal analysis of thinness was constructed in steps, and the final best-fitted model was run to measure the direct and indirect determinants of the variables separately (figure 2).
In the direct-fitting GSEM model, adolescents who had lower traditional and mixed dietary consumption habits had a direct positive influence on stunting with adjusted β=0.65, 95% CL (0.143 to 1.159) with a value of p=0.012, adjusted β=2.697, 95% CL (0.563 to 4.831) with a value of p=0.013, respectively.
Breakfast eating frequency had a negative indirect influence on the reduction of stunting via lower traditional and higher consumption habits of animal source food items with traditional alcoholic drinking habits, with an adjusted β of −0.207 (−0.299 to –0.116) with a value of p=0.001, and β=−0.163, 95% CL (−0.260 to –0.065) with a value of p=0.001, respectively.
In addition, breakfast eating frequency had a positive direct influence on stunting via lower consumption of mixed dietary habits with adjusted β=2.697, 95% CL (0.563 to 4.831) with a value of p=0.013. From the adolescent’s inherent variables, adolescents who were female had a negative influence on stunting with adjusted β=−1.039, 95% CL (−1.488 to –0.592) with a value of p=0.001. In addition, from health service-related factors, adolescents who were dewormed had a direct negative influence on stunting with an adjusted β=−0.579, 95% CL (−1.015 to –0.143) with a value of p=0.009 (table 2).
Direct and indirect determinant factors affecting stunting among adolescents in the context of the agrarian community, North-West Ethiopia, 2021
Causal analysis of determinants of adolescents’ thinness
The first GSEM model was fitted based on the hypothesised model to identify determinants of thinness. Then, based on the model assumptions, a test of a fitted model for causal analysis of thinness was constructed in steps, and the final best-fitted model was run to measure the direct and indirect determinant factors (figure 3).
Adolescents' lower breakfast eating frequency had a direct negative influence on the reduction of thinness with adjusted β=−0.332, 95% CL (−0.588 to –0.076) with a value of p=0.011. In addition, adolescents' breakfast consumption frequency had a negative indirect influence on thinness via lower consumption habits of the traditional dietary pattern, with adjusted β=−0.207, 95% CL (−0.298 to –0.116) with a value of p=0.001, and with higher animal source food with a traditional alcoholic drinking pattern with adjusted β=−0.163, 95% CL (−0.261 to –0.064) with a value of p=0.001. However, it had a positive indirect influence on thinness via a lower mixed dietary pattern with an adjusted β=0.124, 95% CL (0.022 to 0.225) with a value of p=0.017. Adolescents who were female had a direct protective influence on thinness with adjusted β=−2.628 95% CL (−3.90 to –1.356) with a value of p=0.001 (table 3).
Direct and indirect determinant factors affecting thinness among adolescents in the context of the agrarian community, North-West Ethiopia, 2021
Discussion
Adolescent dietary habits and breakfast eating frequency were the key directed and mediated determinant factors for stunting and thinness in the study setting. Adolescents who had lower traditional and mixed dietary consumption habits had the most substantial causal determinants on stunting with a path coefficient of adjusted β=0.65 and β=2.697 (p<0.05), respectively. This finding is in agreement with other previous studies, as frequent consumption of diversified food items and breakfast skipping habit were related to nutritional status,34 which reveals that the lower consumption habits of daily dietary habits did not satisfy the required daily requirement of nutrients for adolescents’ physical growth and development. This inadequate intake of macronutrients and micronutrients, poor quantity and quality diet directly causes adolescents to be stunted and thin.35 This finding was supported by other related studies that indicate adolescents fail to meet dietary recommendations for overall nutritional status and for specific nutrient intake.36
Adolescents who had frequent breakfast eating frequency had a direct influence on the reduction of thinness with adjusted β=−0.332. In addition, adolescents' breakfast consumption frequency had a negative indirect influence on thinness via lower consumption habits of traditional dietary pattern, with adjusted β=−0.207, and with higher animal source food with traditional alcoholic drinking pattern with adjusted β=−0.163. Different evidence supported that higher breakfast and meal frequency eating habits per day had decreased odds of stunting than those reporting a lower consumption habit per day.37 38 As adolescents consumed a frequent breakfast-eating habit, it enhanced daily intake of macronutrients and micronutrients and reduced adolescents' risk of stunting and thinness.34 39
Animal source food consumption dietary habit had an indirect influence on thinness via breakfast eating frequency. In this study setting, the community had a traditional dietary habit of consuming animal-source food items with an alcoholic drinking habit. Animal-source foods are an important source of essential nutrients such as protein, iron and zinc, which prevent undernutrition.40 41
Adolescents who were dewormed by intestinal parasites had a direct reduction in stunting with adjusted β=−0.579 (p<0.05). This finding confirmed that adolescents who had access to health and nutrition services such as deworming had a positive impact on minimising intestinal parasite infection, which causes undernutrition. If the adolescent is not dewormed, the parasite directly sucks nutrients from the gut and causes malnutrition and poor growth.42 43 Parasitic infections affect linear growth and nutritional status through several mechanisms such as by declining food intake.44
Being female adolescents had a negative influence on stunting and thinness with adjusted β=−1.039 and β=−2.628, respectively, as compared with being male adolescents (p<0.05). The reason why female adolescents are less likely to be stunted and thin as compared with male adolescents might be related to biological, hormonal, behavioural and sociocultural influences, and similar findings were observed in different parts of Ethiopia and Nigeria.37 45–47
Even though this study was conducted with a validated FFQ, measurement tools and a robust statistical model to identify direct and indirect determinants for undernutrition, it may have methodological limitations due to the inability to identify all food items that are used to prepare the local traditional diet, as adolescents were not involved in food cooking at home, which might have led to under-reporting of food items like spices. In addition, the identified dietary patterns did not triangulate with biomarkers’ level of nutrients.
Conclusion
Dietary patterns and breakfast eating frequency are key determinant factors for adolescent stunting and thinness. Health service-related factors like deworming had a direct influence on stunting. Public health interventions should be implemented to reduce stunting and thinness by improving dietary and breakfast consumption habits. At the healthcare level, strengthening the national deworming programmes in study areas and similar settings can contribute significantly to the reduction of adolescents’ undernutrition. Further study will be conducted using biomarker nutritional assessment methods to determine the level of micronutrients and their relation with identified dietary patterns.
Data availability statement
Data are available upon reasonable request. Data are included within the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. Ethical approval was obtained from the College of Natural and Computational Sciences institutional review board (IRB) with IRB number CNCSDO/188/14/2021, Addis Ababa University. Besides, a permission letter was secured from Dembecha Woreda health office. The aim, potential risk, benefits and confidentiality were made known to respondents in the informed consent form. Additionally, participation was voluntary and we gave them full right to refuse or accept to participate. Anonymity and confidentiality of the respondents’ data were assured. Informed oral assent for participants under 18 years of age was taken from their parents or legal guardians. Direct informed consent was taken from adolescents who were above 18 years and adult study participants. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors thank the study participants for their substantial contributions to participate in this study. The authors also thank their data collectors and field facilitators for their support in collecting the data. The authors also thank their data collectors, study participants and Keble’s administrators for their holistic support.
Footnotes
Contributors EA conceptualised the research design, formulated the research questions, takes full responsibility for the work, designed and implemented the research methodology, and conducted extensive reviews of the manuscript. ZA and AA contributed to refining the research objectives and conceptualisation of the study, designing the methodology and editing the manuscript, and interpreted the results. EA acts as the guarantor.
Funding This research was funded by Addis Ababa University (grant number CNCSDO/188/14/2021).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.