Article Text

Abstract
Introduction Evidence links night shift work to circadian rhythm disruption, causing hormonal and metabolic alterations, as well as increased risk for cardiovascular disease (CVD). This study investigates whether night shift work affects blood glucose variability and dysregulation, potentially driven by circadian misalignment. It also examines whether such disruptions elevate inflammatory markers involved in atherosclerosis and contribute to the exacerbation of CVD risk markers.
Methods and analysis The study includes 60 participants: rotating night shift workers (day, evening, and night shifts) and day workers (controls) at a pharmaceutical plant. We will assess the effects of night shift work on metabolic and cardiovascular health over three phases: an initial 6-week observational period (phase I), baseline registration of CVD risk factors (phase II), and follow-up assessment of CVD risk factors at 2 years (phase III). Phase I registrations include working hours derived from payroll data, sleep metrics by OURA ring (actigraphy, plethysmography and temperature), continuous assessments of blood glucose using continuous glucose monitor, self-reported food diary and measurements of circadian rhythm markers (monocyte mRNA expression). In phases II and III, blood CVD risk factors such as markers of inflammation, lipids, glycosylated haemoglobin, D-dimer, clinical examination of blood pressure, resting heart rate, arterial stiffness by the means of carotid to femoral pulse wave velocity, carotid intima–media thickness and maximal oxygen uptake (V̇O2max) are measured. To this end, a comprehensive set of methods will be used in a prospective manner to provide new knowledge on shift work-induced glucose regulation and CVD risk factors.
Ethics and dissemination All participants provided written informed consent prior to participating in the study, which will adhere to the principles outlined in the Declaration of Helsinki. Ethical approval has been granted by the Norwegian Regional Committee for Medical Research Ethics South-East B (reference # 745702). Dissemination plans include academic and public publications, as well as collaborations with national and regional policy-makers.
- Cardiovascular Disease
- DIABETES & ENDOCRINOLOGY
- SLEEP MEDICINE
- NUTRITION & DIETETICS
- OCCUPATIONAL & INDUSTRIAL MEDICINE
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Cardiovascular Disease
- DIABETES & ENDOCRINOLOGY
- SLEEP MEDICINE
- NUTRITION & DIETETICS
- OCCUPATIONAL & INDUSTRIAL MEDICINE
Strengths and limitations of this study
Study will provide new insights into the relationship between night shifts and cardiovascular disease (CVD) risk factors.
Extensive data collection associated with real-life night shift work, including continuous blood glucose, self-reported food intake and sleep behaviours associated with night shifts.
Baseline and 2 years follow-up on a wide spectrum of CVD risk factors.
The sample size is a potential limitation to interaction and subgroup analyses.
Introduction
Production efficiency, logistical demands and economic globalisation all have an impact on the labour market and workplace organisation; thus, various forms of shift work are, therefore, widespread.1 In Norway, this affects up to 4 out of 10 workers in the industry sector. Around 11% of workers in Norway, about 290 000 individuals, report night-time work in the last 3 months2; the corresponding figures in Europe are 19%.3 Different definitions exist on shift work and night work. The European Working Conditions Survey defines night shifts as those occurring at least once per month, with each shift including at least two working hours between 22:00 and 05:00 hours.3
The impact of night shift work on cardiometabolic health, or the overall health of the cardiovascular and metabolic systems, is a major source of concern. This includes factors involving blood pressure, adiposity, lipids and blood sugar levels. Recent systematic reviews and meta-analyses encompassing several hundred thousand individuals have demonstrated an increased risk of cardiovascular disease (CVD) in night shift workers compared with those working daytime only.4–6 Research conducted at our institute has shown that shift work is associated with atherosclerosis and low-grade inflammation,7 in addition to increased arterial stiffness or arteriosclerosis.8 9 Studies have also suggested an association between shift work and type 2 diabetes (T2D), in particular among night shift workers.10–12
Night shift work may predispose individuals to unhealthy lifestyle habits, such as irregular eating patterns, smoking and reduced physical activity. However, it may also have direct physiological effects.13 Night work might reduce melatonin release, alter cortisol levels, and elevate inflammatory markers, and disrupt insulin and other endocrine hormones. Circadian misalignment and disruptions in circadian rhythm/sleep duration have also been considered a risk factor for T2D. Both excessively long and short sleep durations have been linked to T2D. The explanation for the association with reduced sleep may be disturbances in endocrine function such as decreased glucose tolerance and insulin disturbances, higher cortisol levels in the evening, increased sympathetic activation and decreased secretion of leptin, which is a hormone in adipose tissue. Further, elevated plasma glucose levels, or hyperglycaemia, are a significant risk factor for atherosclerosis.14
Glucose variability refers to fluctuations in blood glucose levels that happen throughout the day, in conjunction with food intake. High glucose variability has been linked to inflammation markers like C reactive protein (CRP).15 It is also a cause of concern considering ‘the metabolic memory theory’, which states that early intensive control of hyperglycaemia reduces the risk of diabetic micro/macro vascular complications later in the course of the disease independent of glycosylated haemoglobin (HbA1c) levels.16 17 Periods of high glucose can affect the blood vessels and, in the long term, cause complications. Dysregulation of blood sugar in shift workers is one possible factor linking shift work to CVD.17
Circadian misalignment is often described as sleeping or being active at an inappropriate circadian time characterised by a mismatch between sleep-wake behaviours (eg, sleep, activity and food intake) and circadian physiology, including rhythms of body temperature, melatonin production and cortisol secretion.18 Thus, the degree of circadian misalignment associated with (shift) work can be determined based on chronotype and deviations of midpoint of sleep. Another force that is influencing circadian misalignment is entrainment of the internal time to shift work behaviours and altered light exposure. Normal pancreatic function and insulin production fluctuate during the day and depend on circadian oscillations of gene expression in the insulin-producing β-cells.19 Circadian misalignment associated with travel and jet lag impairs glucose homeostasis.20 If high levels of glucose appear at night, activation of epigenetic mechanisms may increase the levels of inflammatory markers and thus cause arterial affection.21
While glucose regulation may play a key role in cardiovascular health among night shift workers, previous studies have primarily relied on simulated shift work or standardised metabolic challenges in controlled laboratory settings.22–28 A gap remains in our understanding of how glucose regulation functions under real-world shift work conditions, and whether it contributes to CVD risk factors, particularly in the context of disrupted sleep, irregular food intake and circadian misalignment.
We hypothesise that acute dysregulation of blood sugar while working night shifts, and in the immediate days after, is associated with long-term worsening of CVD risk factors among night shift workers (figure 1). Repeated bouts of circadian misalignment may be one underlying mechanism.
A theoretical model showing circadian misalignment and glucose variability as mediators of the relationship between night work and health risks and outcomes. Circadian disruption and glucose variability are the potential mechanisms explaining how night work impacts cardiometabolic health and risk of developing cardiovascular disease.
Research aims and objectives
The first aim is to observe whether night shift work is associated with blood glucose variability and dysregulation:
1.1 Continuously monitor blood glucose levels during consecutive night shifts and the subsequent recovery days, assessing variability and regulation compare with daytime work and non-shift working controls.
1.2 Describe sleep behaviours, the timing of food intake and the macronutrient composition of meals (including lipids, amino acids and carbohydrates) associated with night shift work and examine how these factors interact with blood glucose regulation—compare with non-shift working controls.
The second aim is to explore circadian rhythm shifts and glucose regulation as potential mechanisms connecting consecutive night shifts to changes in cardiometabolic health markers:
2.1 Determine the acute effect of consecutive night shifts on cardiometabolic markers compared with day shifts, and these markers in non-shift working controls.
2.2 Measure peripheral circadian markers in conjunction with consecutive night shifts to reveal potential rhythm shifts related to work exposure and the associated sleep behaviours.
2.3 Measure molecular cardiometabolic risk markers after consecutive night shifts and day shifts and relate these to circadian markers and glucose variability.
The third aim is to determine the long-term impact of night shift work on CVD risk factors29:
3.1 In night shift workers and non-shift workers, measure and compare cardiometabolic health markers and CVD symptoms at baseline and at a 2-year follow-up (FU).
3.2 Investigate the relationship between baseline glucose variability and long-term development of CVD risk factors including insulin resistance and the metabolic syndrome.
Methods and analysis
Setting and study population
In this longitudinal controlled cohort study at a Norwegian pharmaceutical plant department, we aimed to recruit a night shift working population (n=30) of both sexes aged 18–64 years old. The night shift workers follow a 6-week rotating shift schedule including night work (figure 2). A separate group of day workers (n=30) has been recruited as a control group. This control group is from the same pharmaceutical plant as the night shift workers. Our previous experience suggests a participation rate of approximately 80% among the night shift workers.7 We have assessed baseline measurements and will carry out FU measurements after a period of 2 years. Data collection at baseline and FU includes an in-house questionnaire, the Munich Chronotype Questionnaire for Shift workers (MCTQshift), registration of actual working hours from payroll data (to detect deviations from scheduled work) and the following medical examinations: cardiorespiratory fitness testing, blood pressure, arterial stiffness, carotid intima–media thickness (cIMT), body weight, body height, waist circumference, body composition and venous blood collection under fasting (>8 hours) and non-fasting conditions. At baseline, we measured blood glucose over a 14-day period using a wearable continuous glucose monitor (CGM; Freestyle Libre Pro iQ-system, Abbott). During this time, participants simultaneously logged their food intake through a smartphone app questionnaire created with ‘nettskjema.no’, a survey solution developed and hosted by the University of Oslo (nettskjema@usit.uio.no). Additionally, sleep and physical activity was monitored during a 6-week period using an activity ring (OURA, Oura Health Oy, Oulu, Finland).

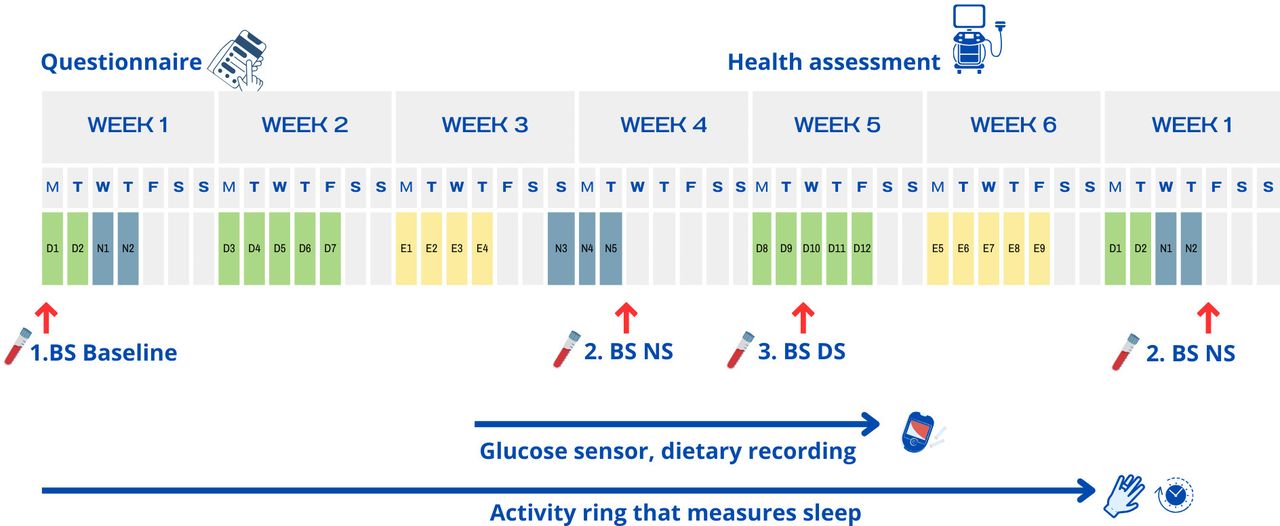
The study’s data collection scheme of the 6-week rotating shift schedule. Blood samples will be collected on day 2 of week 1 (before day shift; fasting), day 2 of week 4 (after night shift; non-fasting), or day 5 of week 1 of new rotating shift (after night shift; non-fasting) and day 3 of week 5 (before day shift; non-fasting). Food intake will be recorded with a smartphone app questionnaire, and blood glucose will be estimated using a continuous glucose monitor (CGM), as indicated, for 14 days from week 3 (E3) until week 5 (D10). Health monitoring will be conducted during the 6-week time-period. Sleep, heart rate and movement will be tracked by an Oura ring from week 1 (D2) to week 6 (E7). Blood samples are indicated by bold ‘BS’, followed by shift indication: ‘NS’, for after night shift; ‘DS’, before day shift; ‘D’, for day shift; ‘N’, for night shift and ‘E’, for evening shift.
Shift work schedule
As illustrated in figure 2, the regular night shift work schedule consists of a rotating ‘6-shift plan’. The 6-week shift plan has a total of 5 night shifts, lasting from 20:30 or 23:30 to 07:00, with a recovery period of 3–5 days. The night shifts occur in two bouts separated by approximately 3 weeks: 2-day shifts (from 06:30 to 14:00) precede two consecutive night shifts, followed by 3 days off; then three consecutive night shifts followed by 5 days off. The 6-week shift schedule also consists of 10 additional day shifts and 9 evening shifts (from 14:00 to 23:00). Each shift worker is part of a team of five individuals that oversee the production using computers, manages and maintains machinery, and participates in product quality control, all inside a clean environment free of potentially hazardous dust or aerosols. The day workers are exposed to the same environment as the shift workers; however, they do not move around in the production area.
Criteria for excluding further participation
We have excluded potential study participants diagnosed with severe heart or lung disease, cancer or showing very high blood pressure levels (>180/110) at the baseline medical examination. In addition, we excluded individuals with metabolic syndrome at baseline29 and those aged ≥64 years. Controls that were not ethnically comparable to the night shift workers were excluded.30 In cases where previously unknown medical conditions were identified during examinations, the affected worker was referred to their general practitioner or an appropriate specialist for further evaluation and/or treatment.
Data collection period
The data collection started in late autumn of 2024 and is scheduled to end 2 years later, in 2026. The shift workers are distributed in six teams working the same shift schedule (figure 2) but in a staggered fashion. Therefore, we conducted baseline data collection and tracked each team accordingly for 6 weeks (phase I). Health assessments and fasting blood samples were taken at baseline (phase II) and will be collected at the 2-year FU (phase III).
Data collection procedure at baseline: phase I
Measurement of glucose levels
The FreeStyle Libre Pro iQ CGM (Abbott) was applied with a separate sensor applicator to the back of the upper arm where it measured blood glucose indirectly in the interstitial fluid every 15 min (figure 2) for 14 days. During use, the data were stored locally in the sensor, and at the end, downloaded wirelessly by a project worker.
Self-reported food diary
Food intake registration was carried out for 14 days overlapping with CGM blood glucose measurements. For this, participants used the mobile app ‘Nettskjema’, which is an online survey tool developed by the University of Oslo (figure 3). Participants took time-stamped photos and commented on all food intakes including leftovers. Images and text will be manually translated into quantitative micronutrient intake using a calculation tool. To minimise variability and misclassification, the same scorer is used throughout the study.

{kind=link}
{kind=link}
{kind=link}
Mobile app ‘Nettskjema’, an online survey tool developed by the University of Oslo.
Registration of sleep and physical activity
Throughout the shift cycle of 6 weeks, the participant continuously wore an OURA Gen 3 health tracker ring (OURA, Oura Health Oy) that uses a three-dimensional accelerometer to measure movement, a negative temperature coefficient thermistor to measure body temperature, and infrared photoplethysmography to measure body signals such as heart rate, heart rate variability, peripheral oxygen saturation and respiration. Sensor data enable the extraction of metrics such as sleep duration, sleep onset, sleep latency, sleep period end and sleep stages using the OURA Sleep Staging Algorithm 2.0, which has been validated against polysomnography.31 Mid-sleep, that is, midpoint between sleep onset and wake-up time, on free days, will be used as a proxy for assessing chronotype.
Registration of time at work
To map actual working hours, the employer will provide us with actual working hours from payroll data including extra shifts, holidays and sick leaves.
Measurement of internal circadian time
Peripheral CD14+monocytes were isolated from EDTA-stabilised blood at the second and third blood sampling during phase I, as described in a former paper.32 Briefly, we will analyse isolated RNA with Nano String Counter technology to quantify expression levels with a panel of 48 marker RNAs designed to reflect circadian time, as described earlier.33 The panel used in our study will include six additional core circadian clock elements and reference transcripts (BMAL1, CLOCK, B2M, RPL37A, SDHA, TBP). Differences in monocyte expression profiles at two different phases of the shift cycles, in the morning after consecutive night shifts and before day shift, will be used to estimate changes in circadian internal time associated with night shifts. We will perform FU measurements of global expression with proteomics analysis on monocyte lysates with an Orbitrap Exploris 480 mass spectrometer equipped with a FAIMS unit.
CVD-risk factor registration at baseline and 2-year FU: phase II and phase III
This part of the project aims to see if there is an association between occupational exposure to shift work including work at night and cardiovascular outcomes such as vascular stiffness, carotid artery changes, inflammation and diabetes risk.
Blood collection and analyses
Whole blood samples (both fasting and non-fasting) will be collected at identical chronological time points for all participants, with measurements taken at baseline and FU assessments. Refer to online supplemental table 1 for an overview of the inflammation, adhesion, thrombosis and metabolic markers investigated in this study, along with their respective sample source and detection method. We will collect HbA1c, haemoglobin (Hb) and leucocytes in EDTA tubes and analyse them with a Tosoh G7 HPLC analyser (Tosoh Bioscience, San Francisco, California, USA). We will collect serum using gel tubes for the investigation of lipids; cholesterol, low-density lipoprotein, high-density lipoprotein and triglycerides, as well as CRP, and then subsequently centrifuge at 2100× g for 10 min within 60 min of the blood collection. The lipids are analysed using an enzymatic colourimetric method (Cobas pro, c503 Modular Analyzer Roche Diagnostics). Citrate plasma for D-dimer will be collected in citrate tubes and analysed within a period of 9 hours. CRP in serum and D-dimer in citrate plasma will be assessed by the particle enhanced immune turbidimetric method on Cobas pro, c503. Whole blood, collected in non-fasting EDTA plasma tubes, will be inverted five times prior to undergoing centrifugation at 2100× g for a duration of 10 min. Plasma will be collected and aliquoted into approximately 500 µL volumes in 1.5 mL cryo tubes, subsequently stored at −80°C for future analysis. Cytokines and adipokines will be determined using magnetic bead-based Luminex screening assays with an IS 200 or Intelliflex instrument (Luminex).
Supplemental material
Questionnaire
The participants will complete an electronic questionnaire during the examination developed by the institute, at both baseline and at FU. The questionnaire is delivered by email and assesses the participants’ educational level, work experience, employment history, physical workload, pain symptoms, medication usage, medical history, lifestyle factors, sleep patterns, drinking, smoking and smokeless tobacco ‘snus’ habits. Additionally, the questionnaire addresses blood pressure and cholesterol lowering medication, and exercise habits (the frequency and duration of light/moderate to intense activity). MCTQshift will be used to collect chronotype information,34 supplemented with OURA sleep metrics.
Anthropometric measurements
Body weight is measured with participants lightly dressed using a Precision Health Scale UC-321 balance (A&D Co., Saitama, Japan) and TANITA T8148 MC-780MA S WHITE (TANITA, Tokyo, Japan; EUROPE B.V.). Height measurements, in centimetres, are taken using a Seca device attached to the wall (Seca, Hamburg, Germany). Further, waist circumference is calculated according to the recommendations put forward by WHO (Waist circumference and waist-hip ratio. Report of a WHO expert consultation, WHO 2008).
Blood pressure and resting heart rate
Blood pressure and resting heart rate are measured after a 5-min seated rest from the subject’s left arm using BpTRU (Bp TRU medical devices, Coquitlam, Canada), using a regular adult cuff with a bladder size of 12×23 cm. None of the participants included in the study had either extremely small or extremely large arm circumferences. Systolic and diastolic blood pressure are measured three times at 1-min intervals, and the mean of the two last readings is used in data presentations.
Arterial stiffness measurements
Central blood pressure, augmented pressure and its index are measured in a non-invasive manner using a SphygmoCor XCEL (Atcor Medical, New South Wales, Australia). Furthermore, carotid to femoral pulse wave velocity (cfPWV) is measured according to the manufacturer’s guidelines (Medical A. Actor Medical 2019, available from www.actormedical.com) using the adult cuff (23–33 cm) or, for the most overweight participants, the large adult cuff (31–40 cm). For the thigh measurement, the only cuff provided by the manufacturer is used (code: 1-00897), with an approximate size of 80 cm.
Measurement of cIMT
cIMT is defined as the distance between the lumen-intima interface and the media-adventitia interface and plaque as a focal structure that protrudes into the arterial lumen of at least 0.5 mm or 50% of the surrounding cIMT value, or that demonstrates a thickness of more than 1.5 mm measured from the media–adventitia interface as reported in the Mannheim consensus document.35 cIMT is determined using automated software (EchoPAC; GE Medical Ultrasound, Horten, Norway). The mean of at least three measurements in the last 10–15 mm of the common left and right carotid arteries is assessed. In addition, the bifurcation and internal and external carotid arteries are assessed for the presence of plaques, and maximal IMT is measured.
Aerobic fitness
The gold standard for determining aerobic fitness is measuring the maximal oxygen uptake (V̇O2max) by the means of gases.36 A standardised graded test using a cycle ergometer (Monark 874 E, Monark Exercise AB, Vansbro, Sweden) is used to examine all participants. Simultaneously, we measure oxygen uptake with a Cosmed K5 metabolism analyser (Cosmed Srl, Rome, Italy). The participants start with a load of 70 Watts and a cadence of 70±2 revolutions per minute (RPM). Loads are thereafter increased by 28 Watts or 0.4 kg every minute. We consider the participant exhausted when he/she fails to keep up with a minimum cadence of 60 RPM despite encouragement. We use the 30 s averaged interval with the highest measurements to calculate participants’ V̇O2max.
Data management
Storage of data
Collected data will be temporarily cloud-stored by the University of Oslo, Walr Group, Abbott and Oura Health Oy and then downloaded and stored at STAMI in an encrypted database which is protected by a two-step verification code and firewall. All physical documentation will be stored in an enclosed locker, with a physical lock. Only personnel in the project will have access to these files or facilities.
Statistical analyses
For research objectives 1.1 and 1.2, the primary dependent variables are plasma glucose level (CGM data). For research objectives 2.1–2.3, the primary dependent variables are circadian rhythm markers in monocytes, as well as functional and molecular risk markers for CVD listed in online supplemental table 1. For research objectives 3.1 and 3.2, the dependent variables are functional risk markers for CVD and markers of insulin sensitivity and metabolic syndrome. Linear and logistic mixed models will be used to determine if dependent variables vary with type of working time arrangement (night shift work or day time work only), shift types (consecutive night shifts or day shifts), number of consecutive night shifts, sleep metrics, food intake (timing, frequency, energy intake, nutritional constituents) and levels of circadian misalignment and disruption as measured in peripheral cells. As for the continuous outcomes, we will apply a linear mixed model and a random intercept for worker, adjusting for age, sex and smoking history (pack years). Two-way and three-way interactions among variables will also be analysed to explore their combined effects. The primary group comparison will focus on shift vs day workers during the 6-week shift period in phases I and II. The secondary within-group comparisons will be between phase II baseline and phase III 2-year FU. In these cases, the exposure variable will be dichotomous with categories shift worker and day worker (control group). In all analyses, participants will be included as a random effect. Statistical analyses will be performed in Stata 19 (StatCorp) or R (www.r-project.org) or similar software.
Loss to FU, compliance and missing data
Our previous experiences suggest a participation rate of approximately 80% of the total workforce among night shift workers and a higher one for the control subjects. During the 2-year period, we expect a 10%–20% loss to FU due to participants leaving employment or being on sick leave. Mixed models are well suited for handling unbalanced data and can yield unbiased estimates, even in the presence of missing data, assuming the data are missing at random. However, if we identify patterns indicating that this assumption may not hold, we will consider applying imputation techniques. To ensure the robustness of our findings, we will compare the outcomes of analyses using both imputed and non-imputed datasets.
Study power
Study power has been estimated based on CGM glucose data.20 With an effect size of 4% change in mean glucose over a 72-hour night shift period, sample size calculations estimated that 24 participants are sufficient in each of the two groups (power 80%, α=0.05). In the present study, we invited n=60 workers at the plant, which should yield between 48 and 54 participants and sufficient power. Further, our power calculation assumes a dropout of 20% after 2 years and is based on a former study by our group exploring the change in cfPWV during a 5-month study period,37 but also on calculations performed in a similar project.32 A formal power calculation for interactions was not conducted. We aimed for the largest feasible sample size but recognise that this may limit the ability to detect smaller interaction effects, and we will interpret such findings with caution.
Patient and public involvement
Workers’ and managements’ representatives from the plant were first involved after the first draft of the protocol in the spring of 2024. Based on meetings and feedback on our presentations, the research question(s) were developed and informed by their priorities, experience and preferences. Their involvement impacted the design and conduct of the study to harmonise with work tasks and routines. Involvement also influenced the choice to include the VO2max.
Discussion
In the present study, we will investigate the relationships between shift work with night work, glucose levels and early manifestations of CVD.38–40 The main aims are to determine if night shift work is associated with dysregulation of blood glucose, elucidate the impact of circadian disturbances (phase I) and investigate the association with and long-term effect on CVD risk (phases II and III). We will employ a prospective approach, using multiple methods to identify and highlight potential cardiovascular risk factors. Our main independent variable is blood glucose assessed by CGM for 14 days. Further, sleep and physical activity monitoring along with food intake registrations will provide additional knowledge on important aspects of the investigated association between shift work and cardiovascular health. Individual differences in chronotype and shift work-related entrainment of internal clocks will be taken into account by MCTQshift, OURA actigraphy and measuring circadian rhythm mRNA markers in isolated monocytes, respectively. In addition, our plan to apply proteomic analyses in FU the monocyte samples will allow us to further disentangle the health effects due to changes in internal clocks or exposure to circadian misalignment through pathway analyses. To this end, we will be able to disentangle the biological strain associated with the night work exposure at the individual level and make better predictions of CVD risk after years of shift work.
Obesity, insulin resistance and diabetes, along with hypertension and hypercholesterolaemia, are important when it comes to the development of atherosclerosis.14 Night shift workers are subjected to circadian disturbances which, combined with eating at night, might affect glucose metabolism, increasing the risk of obesity, diabetes, and eventually CVD. In addition to the above mentioned risk factors, systemic inflammation may contribute to the development of various manifestations of CVD.14 The development and progression of atherosclerotic CVD is very complex, in which several inflammatory agents are also involved.41 Affection of several markers of inflammation has been linked to increased risk of developing CVD.14 41–43 These markers, along with adipokines in the fat tissues, will provide information on CVD risk and progression of risk during the FU among the participants.
As to affection of the arterial wall, we will investigate both signs of arteriosclerosis and atherosclerosis, use non-invasive methods by the means of cfPWV and cIMT. Pulse wave velocity (PWV), irrespective of blood pressure, has a better predictability of cardiovascular outcomes and all-cause mortality than standard brachial measured blood pressure,44–46 and is also a predictor of various other organ disorders and mortality.47 An increased risk has been found to be associated with shift work.8 9 As to cIMT, the literature has revealed an increased values in night shift workers,40 but also non-positive studies have been published.8 9 48
A major strength of the current study is that it not only provides CVD-related assessments in both night shift and day-working populations at baseline and at 2 years FU—potentially reproducing findings in our earlier studies17 37—but also incorporates several distinguishing and novel features. This study applies a comprehensive set of health measures, including continuous monitoring of glucose levels, detailed tracking of food intake and sleep patterns, molecular measures of internal circadian time, and the assessment of plasma markers related to inflammation, thrombosis, metabolism and endocrine function. The unique value of this study lies in the combination of these comprehensive health measures, providing a multidimensional understanding of cardiometabolic health that would be unattainable through isolated assessments. The primary advantage of CGM lies in its capacity to capture interstitial glucose levels at frequent intervals over extended periods while the study subjects work their actual shifts, and with ad lib food intakes, providing a detailed view of daily glucose homeostasis in a real-life setting. This contrasts with earlier studies, which often rely on simulated shift work in a laboratory setting,22–26 or postprandial responses to simulated meals or glucose tolerance testing.22–28 At this point, our study not only bridges existing knowledge gaps but also increases our understanding of previous studies. The CGM approach has been used to examine the effects of circadian misalignment during air travel20 and shorter periods in shift workers49 but has not been applied to night shift work in combination with the parallel collection of detailed sleep metrics, food intake and peripheral molecular clock data, as in our study. Our approach will enable the detection of glucose fluctuation patterns associated with night shift work; a period characterised by circadian misalignment. As previously noted, glucose patterns may provide insights into glucose regulation in relation to the timing and nutritional composition of food intake as the night shift progresses, as well as during the recovery period in the days following bouts of night work. Additionally, the complex set of biomarkers in isolated monocytes—validated in earlier studies33—will offer gene expression profiles related to internal time at specific points in the work schedule and give mechanistic insight to a potential link between working time and physiology. Another advantage of this study is the controlled environment of the pharmaceutical plant, allowing us to assume that the working conditions are free from hazardous dust or aerosols that could potentially harm the cardiovascular system. In addition, the plant provides a detailed description of not only planned working hours according to shift schedule for every participant, but also the actual working hours based on payroll data.
The modest sample size of 60 participants is a potential limitation, particularly for interaction and subgroup analyses. Although power analyses and previous experience from similar industry-based studies suggest that this sample size is sufficient to detect significant effects—even when accounting for potential dropouts—it may still limit the ability to detect smaller, nuanced differences. A lack of a formal power calculation for interactions is a limitation. As for the blood pressure and measurements for arterial stiffness, we only used one cuff size for all participants. This could be a limitation. However, we did not register any participants with extremely large or small arms in the study population. While the study’s longitudinal design is strengthened by a robust 2-year FU period, it may still be insufficient to fully capture long-term cardiovascular outcomes, especially given that CVD typically develops in the long term. Participant dropouts are also possible due to factors such as job changes, health issues or declining motivation to participate. Loss of motivation could impact on the quality and completeness of the data. To mitigate this, regular meetings will be held between participants and the project team throughout the FU period. This approach is expected to improve compliance and limit loss to FU. Maintaining participant motivation is also critical during periods involving CGM, sleep tracking and food intake registration. Some data, such as food intake, will rely on self-reported measures, which are prone to recall bias and underreporting. Additionally, participants’ increased awareness of their behaviours during monitoring may introduce further bias, in particular food intake and sleep behaviours. There is also a potential for selection bias, as individuals who choose to participate may differ systematically from those who do not. Healthier workers or those more concerned about their health may be more likely to participate. However, achieving adequate response rates will help mitigate this concern. Furthermore, the study may be influenced by the healthy worker effect, particularly among shift workers who may represent a self-selected group that tolerates shift work better than average. There is also a possibility that the day-working controls may have previously engaged in shift work, meaning they are not entirely shift-free and could have opted out of shift work due to low tolerance for it.
This project will provide new knowledge on the mechanisms connecting night shift work, disturbances of the circadian rhythm, glucose regulation and CVD risk factors. This knowledge might affect how shift work in industry is organised and potentially prevent or reduce detrimental health effects in this part of working life. Additionally, the study findings may also be applicable to other parts of the shift-working population.
Ethics statements
Patient consent for publication
Acknowledgments
This study will be carried out in collaboration with a pharmaceutical company in Southern Norway, and we would like to thank them for their willingness to participate. We would like to thank the Department Managers at the site for their assistance to coordinate measurements and testing procedures with work schedules and tasks. We also thank Associate Professor Monica Carlsen, University of Oslo, for food diary design.
References
Footnotes
Contributors MS and FH came up with the initial study idea. All authors have contributed to form the study design. SA had overall responsibility for the paper drafting. SA and FH will be responsible for blood analysis. MS will be responsible for cardiovascular measurements. All authors reviewed, edited and approved the final version of the manuscript. FH serves as the guarantor and chief investigator of the study, overseeing study registrations, attaining approvals, communicating important protocol modifications and maintaining overall responsibility for its execution. In some instances, Chat GTP was used to polish and revise writing.
Funding Funding in part is provided from Circle K Norge AS Fond for Arbeidsmedisinsk Forskning; and Borregaard Forskningsfond; Title: "Kan døgnrytmeforstyrrelse ved nattarbeid påvirke stabiliteten av blodsukkeret, og er dette forbundet med endringer i hjerte- og karsystemet" (2024).
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.