Article Text

Abstract
Objective To estimate the associations between refraction and ocular biometry of preschool children (3–6 years old) in Shunyi District, Beijing.
Design Cross-sectional study.
Setting This study was conducted in 11 kindergartens in Shunyi District, Beijing.
Participants A total of 1186 Chinese children aged 3–6 years old without any history of Down’s syndrome, epilepsy, history of ophthalmologic surgery and other psychiatric disorders were selected. Exclusions: Children who were unable to cooperate with the examination. 1141 preschoolers completed the examination. 555 subjects (48.6%) were boys and 586 subjects (51.4%) were girls. Cycloplegic refraction, axial length (AL), anterior chamber depth (ACD) and corneal radius (CR) were measured for all children. AL-to-CR ratio, lens power (LP) and spherical equivalent (SE) were calculated. Those children were divided according to SE into three groups: hyperopia group, premyopia group and myopia group.
Interventions None.
Primary and secondary outcome measures Refraction and ocular biometric parameters.
Results The prevalence of myopia, premyopia and hyperopia was 2.7% (95% CI 1.8% to 3.7%), 27.3% (95% CI 24.7% to 29.8%) and 70.0% (95% CI 67.4% to 72.7%), respectively. The mean SE was (1.15±0.76) D, and the refraction in the premyopia group was about 1 D lower than in the hyperopic one. The mean AL, ACD, CR, AL/CR and LP were 22.28±0.67 mm, 3.33±0.67 mm, 7.74±0.25 mm, 2.88±0.06 and 25.62±1.46 D, respectively. Differences in AL, ACD, AL/CR and LP among different age groups were statistically significant. Premyopic children had longer eyes, greater ACDs and higher AL/CR ratio than hyperopic children. SE was negatively correlated with AL, ACD, AL/CR and LP.
Conclusions The most common refractive status of children aged 3–6 years in Shunyi District, Beijing, was hyperopia. The prevalence of premyopia was by no means low. Understanding the refractive status of preschoolers and associations between ocular biometric parameters and refraction might be helpful in providing more effective prevention before the onset of myopia.
- Myopia
- Paediatric ophthalmology
- Child
Data availability statement
All data relevant to the study are included in the article.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study used a random sample of preschool children in a suburb of Beijing, China.
The study participants were children aged 3–6 years, generally considered to be the period before the onset of myopia.
The study participants included students exclusively from kindergartens and may not be representative of children not enrolled in these educational settings.
The cross-sectional design limits the ability to establish causality.
Introduction
Individual refractive development is dynamic throughout life. Children are born with a peak of approximately +2.00 D hyperopia, and the peak moves towards emmetropia over the first 2 years after birth.1 However, studies of children’s refractive development in large populations suggest that emmetropia is not the natural endpoint of this process.2 The ocular components such as corneal and LP, anterior chamber depth (ACD) and axial length (AL) are crucial in the refractive development. It is the balance between these ocular components that determines the refractive status.3 After 3 years of age, AL and ACD increased with limited changes in corneal power but significant decreases in LP.4 Studies have shown that one of the main determinants of refractive status is AL.5 Myopia may develop when rapid increases in AL exceed the compensatory capacity of the lens.
Refractive error in children has been one of the global public health problems nowadays, and myopia accounts for a large proportion of refractive error.6 In recent decades, the onset of myopia among children has displayed a trend of younger age. 10.7% of preschoolers aged 5–6 years suffered from myopia in Taiwan,7 and the overall prevalence of premyopia was high among preschoolers.8 Children with an adequate physiological hyperopic refraction, defined as ‘hyperopic reserve,’ are unlikely to become myopic.9 In 2019, the International Myopia Institute (IMI) defined ‘premyopia’ as ‘refraction ≤0.75 D and >−0.50 D’ in children.10 Prior to the onset of myopia, rapid changes in refraction and ocular components may provide predictive information.11 One longitudinal study reported that LP loss suddenly slowed down 1 year before the onset of myopia combined with relatively high rates of axial elongation.12
For these reasons, there is an urgent need to identify children at high risk of early myopia. The optimal time for myopia prevention should be earlier than elementary school age. However, there are fewer large-scale refractive data available on children aged 3–6 years, not to mention data about premyopia in preschoolers. Therefore, this study was conducted to evaluate the refraction and ocular components of preschool children. Understanding the premyopic refractive status and identifying the associated factors can provide guidance for early prevention. Further objectives include investigating the relationships between refraction and the ocular biometric parameters involved in refractive development.
Methods
Study design and subjects
This was the first-year results of the 2-year longitudinal study with evaluation of subjects aged 3–6 years from Shunyi District, Beijing. Based on a previously published myopia prevalence rate in preschool children aged 3–6 years,13 a sample size of 1107 preschoolers was needed to achieve precision of 0.01 and 95% CIs, taking into account a cluster design effect of 1.5 and assumed dropout rate of 10%. Stratified cluster sampling was employed. Shunyi District is situated in the suburban northeast region of Beijing. Under the support of the preschool section of the Shunyi District Education Commission, a total of 1186 children were randomly selected from 11 kindergartens in Shunyi District. Data for all the participants were collected from October 2020 to June 2021. Children who have any history of Down’s syndrome, epilepsy, history of ophthalmologic surgery and other psychiatric disorders were excluded. 1141 children aged 3–6 years who finished all the examinations were carefully analysed one by one in this study.
Examination
Prior to the examination, all the relevant information such as the patient’s age and gender was recorded. Visual acuity at a 5 m distance was measured using an international standard E chart (Guangdong Yuehua Medical Instrument Factory) in a well-illuminated room. Anterior segments were examined with a slit lamp. Auto refraction and corneal radius (CR) were checked using a desktop autorefractor (model number: KR-8800; Topcon Corporation, Tokyo, Japan). Biometric examination was performed with the Lenstar LS 900 (Haag-Streit, Switzerland) prior to cycloplegia. Ocular biometric parameters including AL and ACD were checked three times, with an automatic calculation of the average in each eye. A concentration of 1% cyclopentolate (Alcon, USA) was used to carry out the examination of cycloplegia. After 30 min, if the pupil diameter was ≥6 mm and there was no light reflex, three successive measurements of refraction were taken. Fundus photography was applied, and no abnormality was found in the fundus examination. All examinations were carried out by ophthalmologists and optometrists who had undergone uniform training.
Definition
Both spherical power and cylindrical power were measured following cycloplegia. The average of three measurements was taken to calculate the spherical equivalent (SE) refraction. SE is equal to half the cylindrical power plus the spherical power. The Bennett-Rabbetts formula14 was used to figure out the LP. Since the high correlation between the right and left eyes, data from the right eyes were chosen in the present study. The mean of the longest and shortest CR of curvature was used to figure out the CR. The definition of the AL/CR ratio was the AL divided by the mean CR. Based on the IMI definition,10 myopia was defined as SE≤−0.50 D, premyopia as −0.50 D<SE≤0.75 D and hyperopia as +0.75 D<SE.
Patient and public involvement
None.
Statistical analysis
The chi-square test was performed to compare the prevalence of refractive error among different age groups. The mean values of SE refraction, AL, ACD, CR, AL/CR and LP were compared between boys and girls using an independent samples t-test. To find out the differences in ocular biometric components across different age groups and refractive error groups, analysis of variance was employed. Trend analysis was conducted to detect age differences. The multiple linear regression model was used to figure out the correlations between SE refraction and ocular biometric components. Statistical significance was defined as p values <0.05. SPSS V.26.0 (IBM SPSS, USA) was used to carry out statistical analyses.
Results
Among the 1186 sampled children who planned to undergo examinations, 1141 completed the cycloplegic refraction and ocular biometric examination after exclusions. The mean age of these subjects was 4.52±0.87 years. 555 subjects (48.6%) were boys, and 586 subjects (51.4%) were girls. It can be summarised from the data in table 1 that the prevalence of myopia, premyopia and hyperopia was 2.7% (95% CI 1.8% to 3.7%), 27.3% (95% CI 24.7% to 29.8%) and 70.0% (95% CI 67.4% to 72.7%), respectively.
Prevalence of refractive errors in children aged 3–6 years
Table 2 displays the mean, SD of the SE refraction, AL, ACD, CR, AL/CR and LP of all participants. The mean SE refraction was 1.15±0.76 D, and it remained stable during this age range. No significant gender differences were found among different age groups.
Distribution of the ocular biometric parameters in different age groups
AL, ACD and AL/CR increased while LP decreased with age. The mean AL was 22.28±0.67 mm, which increased from 22.07 to 22.49 mm. The mean ACD was 3.31±0.25 mm, which ranged from 3.21 to 3.36 mm. Both AL and ACD increased with age. When the data were split by gender, we found the same trend. The mean value of CR was 7.74±0.25 mm. CR did not change with age, but it was higher in boys at 4–6 years (p<0.001). AL/CR increased with age, and the mean value was 2.88±0.06, which increased from 2.85 to 2.91. The AL/CR in boys was higher than in girls at age 3–5 years (p<0.01). The mean LP was 25.62±1.46 D, which decreased from 26.50 to 24.96 D. It was also lower in boys in all age groups (p<0.001). Compared with girls, boys had 0.51 mm longer AL, 0.13 mm greater ACD, and 1.02 D lower LP.
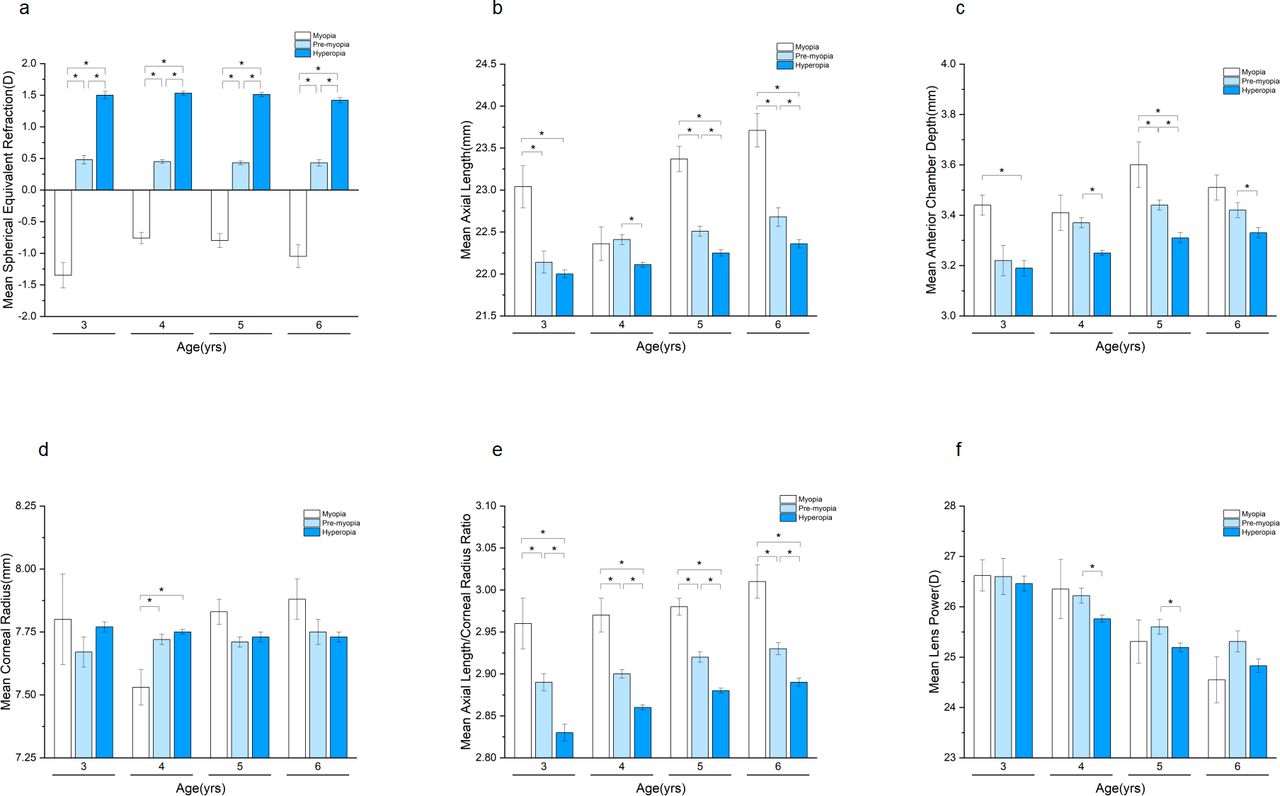
As shown in figure 1, similar trends with age were detected in the premyopia and hyperopia groups. SE and CR remained stable from 3 to 6 years in both groups. AL, ACD and AL/CR increased with age while LP decreased with age. The difference in mean SE refraction between the two groups was about 1.06 D. Premyopic children were approximately 0.28 mm longer in AL, 0.12 mm greater in ACD, and 0.41 D higher in LP compared with their hyperopic peers (p<0.05). The difference in AL/CR ratio between the two groups was about 0.04 unit, which was higher in the premyopia group. The AL in the myopia group at age 4 was shorter along with steeper CR than in the premyopia group. However, when the data were calculated with AL divided by CR, a different result was obtained. Myopic children had a higher ratio of AL/CR than children from premyopic and hyperopic groups. No statistical differences were observed in CR for different refractive groups.

Mean values of SE refraction and ocular biometric parameters among different age and refractive error groups. The error bars represent SEM, *statistically significant. (a) Mean values of SE refraction among different age groups. (b) Mean values of AL among different age groups. (c) Mean values of ACD among different age groups. (d) Mean values of CR among different age groups. (e) Mean values of AL/CR among different age groups. (f) Mean values of LP among different age groups. ACD, anterior chamber depth; AL, axial length; CR, corneal radius; LP, lens power; SE, spherical equivalent.
As can be seen from figure 2, SE was negatively correlated with AL, ACD and LP. There was a significant negative correlation between SE and AL/CR (r=−0.56, p<0.001). A strong positive correlation was found between AL and CR. There was a significant positive correlation between AL and ACD and a negative correlation between AL and LP.

{kind=link}
{kind=link}
Correlation between SE refraction and ocular biometric parameters. Correlation values shown in lower triangular. *p≤0.05; **p≤0.01; p≤0.001. ACD, anterior chamber depth; AL, axial length; CR, corneal radius; LP, lens power; SE, spherical equivalent.
Multiple linear regression models were established to indicate the associations between SE and ocular biometric parameters (table 3). After being adjusted for age and gender, SE decreased linearly with increasing AL, with a −0.455 D change in SE for a 1 mm increase in AL. SE decreased linearly with increasing AL/CR, with a 0.1 unit increase in AL/CR associated with −0.72 D change in SE. Model 1 explained 13.3% of the variance of SE, while Model 2 accounted for 31.3% of the variance of SE, which was better than Model 1. The results suggested that SE was associated negatively with AL and AL/CR.
Linear regression models for SE refraction and ocular biometric parameters (adjusted for age and gender, boys as reference)
Discussion
The increase in myopia is widely believed to be driven by environmental factors such as fewer outdoor activities and more near-work activities. Genetic susceptibility also plays a role in myopia.15 Premyopia is a non-myopic refractive status that may progress to myopia. By realising the relevant risk factors and taking appropriate intervention measures, we can achieve the goal of preventing or at least delaying the onset of myopia. In this study, the overall prevalence of premyopia was 27.3%, which was slightly higher than in Shanghai (21.9%).16 An analysis of the data from children aged 4–6 years who were screened between 2005 and 2021 showed a significant increase in the prevalence of premyopia (19.0% vs 26.5%).17
In the present study, the mean SE refraction was 1.15 D, which was slightly lower than that of Guangzhou (1.42±0.79 D)18 and Shenzhen (1.37±0.63 D),19 but which was similar to that of Shanghai (1.20±1.05 D).20 The results suggest that the refractive development of children aged 3–6 years remained mildly hyperopic in Shunyi District, Beijing. The refraction in the premyopic group was 0.44±0.32 D, which was about 1 D lower than that in the hyperopic group. The study on the prevalence of premyopia in preschoolers in Taiwan suggested that the mean SE in the premyopia group was 0.35±0.33 D.8 The Taiwan study did not use 1% cyclopentolate for cycloplegic auto-refraction, which may have contributed to the difference in SE refraction. Early educational pressure, such as assignments for preschoolers and extensive tutorial classes after school hours,21 leads to early depletion of hyperopia reserve. Therefore, investigation of hyperopia reserve as well as regular monitoring of refraction are significant for myopia prevention.
During the rapid development of infant eyes in the first few years, lower mean levels of hyperopia and early refractive error changes, axial elongation and deepening of the anterior chamber are synchronised with corneal flattening and LP reduction.22 Previous studies have suggested that the cornea flattens with age to compensate for the growth of AL.23 In order to find out the relationship between corneal curvature and refraction, researchers recorded different results. Zhang et al20 found that the mean CR increased with age in boys but not in girls among preschoolers. No significant difference was found in CR between different ages in this study. This finding is consistent with that of Ma et al24 who observed that the 1-year change in CR was 0.00±0.04 mm in children aged 3–5 years, indicating very little change in this period. Zadnik et al25 reported that CR remained stable in different age groups and was higher in boys than in girls. In age groups 4–6, the mean CR was 0.13 mm higher in boys than in girls.
Since corneal power was reported to cause small changes after year 2,26 AL and LP were the determinant factors of SE The AL in newborns is approximately 16.5 mm,27 which rapidly develops to 20 mm at 9 months and reaches 21.42 mm at 3 years of age.28 The mean AL of children in this study was 22.28±0.67 mm. AL increases with age in children aged 3–6 years, and it is 0.51 mm longer in boys than in girls. A similar finding was reported by He et al.29 There was a negative correlation between AL and SE. AL increased while refraction decreased. The AL in the premyopia group was significantly longer than that of hyperopia. In accordance with previous findings,30 a strong positive correlation was found between AL and CR.
The current investigation found that the development of children’s eyes was characterised by a reduction in LP and the growth of AL and ACD. There was a significant difference in ACD in different refractive error groups. Anterior chambers deepen gradually and sequentially among preschoolers from the hyperopia group to the myopia group. The deepening of ACD may also have something to do with lens thinning. The reduction in LP can largely counteract the myopic shift caused by the lengthening of the eye.3 There was no significant difference in SE between different age groups, which indicated that LP reduction associated with AL and ACD growth can counteract the myopic drift. LP was negatively associated with AL, and the change in LP is one of the main factors affecting the early progression of refractive status. Compared with girls, boys had longer AL, greater ACD and lower LP. These findings are in line with those of previous studies.19 25 31
Some children with relatively short eyes might be myopic, such as the myopic children from the 4-year-old group in this study. However, the sound conclusion can be reached after the AL/CR was obtained. This finding confirmed that compared with AL, AL/CR can more accurately reflect the real refractive status.29 AL/CR≥3 suggests that myopia has occurred.32 He et al29 examined 3922 children aged 6–12 years in Shanghai, analysed their data by receiver operating characteristic curves and found AL/CR greater than 2.99 was diagnostic of myopia. This study suggested that the mean AL/CR ratio was 2.88±0.06. In the myopia group, the mean AL/CR was 2.98±0.06, and it was higher in boys than in girls (3.00±0.06 vs 2.95±0.05). AL/CR increased gradually with age, and elongation of AL also occurred among preschoolers in the premyopia and hyperopia group. In the myopia group, AL/CR increased from 2.95 to as much as 3. Among myopic children, who are younger than 6, the values of AL/CR were less than the reported threshold of 2.99. In the premyopia group, AL/CR increased from 2.89 to 2.93. In the hyperopia group, AL/CR was the lowest, and its ratio was less than 2.90. Therefore, the setting up of the age-specific thresholds of AL/CR will improve the accuracy of myopia screening, particularly for preschoolers. Apart from changes with age, significant gender differences were detected in AL/CR. Boys aged 3–5 years had an average 0.02 unit higher AL/CR ratios than girls. One recent study reported the age and gender-specific percentile growth curves for AL and AL/CR in Chinese children. AL and AL/CR were narrowly distributed in the population at 4 years of age.33 An Irish study assessing risk factors associated with premyopia showed that participants with >2 hours/day of screen time (2.92 (0.09)) had significantly higher AL/CR ratios than those with ≤2 hours/day (2.88 (0.08)).34 Clinicians and parents should pay more attention to children with relatively high AL/CR ratio and provide more timely, useful lifestyle guidance in the prevention of the onset of myopia.
Admittedly, there were several limitations in our study. First, the LP was figured out by means of the Bennett-Rabbetts formula, but the lens thickness was not measured, which could affect the accuracy of LP measurements. This limitation may lead to complications in interpreting the role of the lens in refractive error. Second, the differences we observed across age groups cannot be explained by age alone, but by multiple factors such as environmental and behavioural factors, socio-economic factors and other unmeasured confounders. Third, our investigation was a cross-sectional one; it was not possible to assess changes in ocular biometrics before the onset of myopia. Therefore, two follow-up visits were conducted every 6 months to evaluate the changes in refraction and ocular biometric parameters over time. The first-year data of the 2-year longitudinal study is of great importance because it can well illustrate the baseline distribution of ocular biometrics and lays a firm foundation for more scientific research in the future.
In conclusion, the overall refraction was hyperopic, but the ocular biometric parameters including AL, ACD and LP changed significantly from 3 to 6 years old, and associations between ocular biometry and refraction were observed. The refraction in the premyopic group was about 1 D lower than in the hyperopic group. Compared with hyperopic children, premyopic children had longer eyes, greater ACDs, higher AL/CR ratio but similar CR. Whether specific ocular biometric parameters actively attribute to myopia development or merely correlate with refractive status needs longitudinal studies to clarify.
Data availability statement
All data relevant to the study are included in the article.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Ethics Committee of Beijing Shunyi Hospital, No. 2020125. The research was conducted in conformity with the Declaration of Helsinki. Before the examination, the parents were all well informed of the study’s objectives, the examination procedure and the possible consequences, and of course, we received written informed consent from each and every parent.
Acknowledgments
The authors would like to acknowledge the participation of the children and their guardians in the Beijing Shunyi Children Eye Study.
References
Footnotes
Contributors AJ: study design, study supervision and manuscript revision. LZ: data analysis and manuscript writing. QX: study design and data collection. JY, ZL and RW: data collection. AJ is responsible for the overall content as a guarantor.
Funding This work was supported by a grant from Capital’s Funds for Health Improvement and Research, Grant Number 2020-3-7102.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.