Article Text

Abstract
Objective To assess patient satisfaction (PS) with services and its associated factors across selected primary care facilities in Kono district, Sierra Leone.
Design Facility-based cross-sectional study.
Setting Five primary healthcare facilities (Wellbody, Sewafe, Kombayendeh, Gandorhun and Kayima) located in Kono district, Sierra Leone. All five are Community Health Centres (CHCs), with two CHCs benefiting from a comprehensive package of support (5S model) from the non-governmental organisation, Partners In Health (PIH). This support, dubbed as 5S health systems strengthening (HSS) model, will be elaborated in this article. The other three CHCs were not beneficiaries of the 5S model.
Participants The study population comprised all patients and caregivers who attended outpatient services at the selected health facilities. We included adult outpatients over 18 years old and adult caregivers accompanying their children while waiting in the various outpatient departments. This study considered a sample size of 290 and the data were collected from 3rd March to 31st March 2021.
Outcomes PS was measured using an 11-item Likert scale questionnaire. The outcome was categorised as good or poor satisfaction level using the median value. Descriptive statistics were applied to assess satisfaction level and multivariable binary logistic regression analysis was applied to identify factors associated with the outcome variable.
Results Out of the 290 respondents included for analysis, the overall PS level was 63.8% (95% CI 58.1% to 69.0%). Around 69.2% (95% CI 62.1% to 75.4%) of respondents from PIH intervention sites and 53.9% (95% CI 44.1% to 63.4%) from the non-PIH intervention sites had a good satisfaction level. The multivariable binary logistic regression analysis indicated that PIH intervention site status (adjusted OR (AOR)=2.47, 95% CI 1.28 to 4.78), educational status of respondents (AOR=0.53, 95% CI 0.28 to 0.98), distance to health facility (AOR=0.40, 95% CI 0.18 to 0.87) and waiting time to receive care (AOR=0.41, 95% CI 0.22 to 0.76) were the significant factors associated with PS.
Conclusion The overall PS was relatively high andPIH-supported health facilities show better PS than non-PIH health facilities. In addition, patients’ educational status, distance to health facility and waiting time were negatively associated with PS level. The findings suggest that PIH’s model of health systems strengthening with targeted investment on the 5S model can be scaled up and the Ministry of Health could consider implementing this approach for improving the quality of services provided at the primary healthcare facilities.
- Patient-Centered Care
- Patient Satisfaction
- Primary Care
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
Since this was a facility-based cross-sectional study conducted at a point in time, we cannot establish cause–effect relationship and the findings might not be generalisable to the national Sierra Leone context.
The finding of this study might also be subjected to social desirability bias because the respondents were interviewed within the health facilities compounds.
Since the data are self-reported by the patients or caregivers, there might be recall bias from the patients, especially if they had previously different experiences from another health facility.
Perceptions and experiences of patients were not captured qualitatively.
Facilities included in this study are from all the cardinal points of the district, and therefore, respondents are from all the cardinal points (east, west, north, south and central) of the district, providing a wide respondent representation of the district.
Introduction
Patient satisfaction (PS) describes how happy a patient is with the healthcare they receive from their healthcare providers. Within the public health literature, there is a growing emphasis on including patients in their care processes and an increasing call for clinicians and healthcare systems to shift their focus away from diseases and back to the patient needs. To optimise this, the interaction between clinicians and patients should be a collaborative and mutual agreement where the patients’ care decisions are shared decisions among clinicians, patients and/or their family members.1 2 Understanding a patient’s experience of illness and addressing their needs within an increasingly complex and fragmented healthcare delivery system can influence patient health-related behaviours, including adherence to treatment and recommendations of healthcare plans.3
In Sierra Leone, peripheral healthcare units (PHUs) serve as the foundation of the healthcare system, and the majority of patient consultations include the management of long-term chronic conditions and the delivery of preventive services. As a result, PHUs often act as gatekeepers to the other parts of the healthcare delivery system. The UN defined provision of quality healthcare that is safe, affordable and accessible as one of the sustainable development goals of agenda 2030.4 While many countries and healthcare institutions are making strides towards achieving this goal, there are discrepancies in the perception of patients’ expectations and satisfaction between healthcare professions and the patients they serve.
The 2014 Ebola outbreak in Sierra Leone had severely disrupted primary healthcare programmes and the country lost many of the gains from previous health system strengthening efforts. Subsequently, at the end of the Ebola outbreak, the utilisation of the primary healthcare facilities reduced drastically.5 Although we saw an increase in service utilisation at PHUs years after Ebola due to health systems strengthening efforts by non-governmental organisations (NGOs), especially Partners In Health (PIH), little to nothing is known about the overall PS with the services.
Patient dissatisfaction, as indicated by a study conducted in Ethiopia, is associated with the unavailability of drugs and service providers not being polite.6 Another study in Ethiopia indicated that PS at hospital outpatient departments (OPDs) was high with no statistically significant differences between PS at the private wing and regular adult OPDs’ of public hospitals.7
In North India, a study indicated that the majority of patients using outpatient and inpatient services were satisfied with the care received with a notable recommendation to reduce waiting time at registration and laboratory service departments. However, it was also noted that attention should be given to new medicines prescribed for a patient, and that the possible side effects and purpose of giving the medicine should be explained to them.8 With these findings, patients’ experiences and satisfaction with their treatment are becoming increasingly important in the context of quality assurance, and patient experiences healthcare and reporting this information helps patients to have choices in their healthcare seeking.9
While PS is considered one of the desired outcomes of healthcare and is directly related to the utilisation of health services, there is scant information on PS with services provided in public health facilities in Sierra Leone. In this study, we will assess patients’ satisfaction with the level of services offered at both PIH-supported and non-PIH-supported Community Health Centres (CHCs) and its associated factors in Kono district, Sierra Leone.
Methods
Study setting
This study was conducted in 2021 in Kono District in the eastern region with an estimated population of about 600 000, of which 75% of individuals reside in rural areas.10 Five Ministry of Health (MoH) health facilities categorised in the Sierra Leone health system as CHCs in Kono District, Sierra Leone were included. The five CHCs are Wellbody Clinic, Sewafe, Kombayendeh, Gandorhun and Kayima. These health facilities offer general outpatient services, maternal and child health services, non-communicable diseases, HIV and tuberculosis services, as well as additional services, including pharmacy and laboratory as a part of the primary healthcare service package. These facilities are distributed across the district, in the west: Sewafe CHC, east: Kombayendeh CHC, south: Gandorhun, north: Kayima and central: Wellbody Clinic CHC.
We categorised these facilities into ‘intervention’ (Wellbody Clinic and Sewafe CHC) and ‘non-intervention’ facilities (Kombayendeh, Gandorhun and Kayima). The ‘intervention facility’ refers to a facility where PIH provides additional support through their ‘5S Model’.
The 5S model was developed through the iterative work of the US-based NGO PIH to assure that the poorest and most vulnerable patients have access to high-quality healthcare and achieve equitable health outcomes with richer patients. The model recognises the supply side limitations of health facilities in impoverished areas—including lack of staff and commodities, dilapidated facilities and a lack of ability to provide follow-up care. Finally, the model recognises that social supports are needed to overcome the barriers to care for the poor. Thus, the 5S includes improvements in staff (upgraded staffing in number and quality through capacity building and mentorship), space (upgraded infrastructure to provide enough space for adequate service provision, but also clean and dignified space with electricity, clean water, etc., conducive for high quality of care), stuff (ensuring availability of essential drugs and medical commodities, and functional equipment), system (ensuring cohesive mechanism, tools and standardised protocols and procedures are being followed for the provision of care) and social support (for a holistic and patient-centred approach considering the socioeconomic needs of each beneficiary) (figure 1) on the top of the existing MoH structure. In the non-intervention facilities, these facilities received the regular MoH support.

PIH 5S model. PIH, partners in health.
Study design
We conducted a health facility-based cross-sectional study among outpatients and caregivers (guardians of patients under 5 years of age) attending five selected health facilities.
Study population
The study population comprised all patients and caregivers attending outpatient services at Wellbody, Sewafe, Kombayendeh, Gandorhun and Kayima health facilities in Kono District, Sierra Leone between 3rd March and 31st March 2021. We included adult outpatients over 18 years old and adult caregivers accompanying their children while waiting in the various OPDs. Patients or caregivers experiencing mental distress or critical medical conditions were excluded from the study. We used subjective judgement by the data collectors or the patient or caregivers self-report on current or previous mental health conditions.
Patient and public involvement
Neither the patient nor the public was involved in the design, conduct, reporting or dissemination plans of this study.
Sample size and data collection
This study considered a sample size of 290 individuals and the data were collected from 3rd March to 31st March 2021. The sample size comprises the entire population of patients that visited the facilities in study during the study period. A structured questionnaire was developed for the purpose of data collection after reviewing relevant literature.9 11 12
The research team gathered information on non-identifiable demographic characteristics, including age, sex, ethnicity, education, facility location and role at the facility. These data were electronically collected using a CommCare app, with the CommCare content programmed by the research team.
Before the start of data collection, the data collectors received training in research ethics, covering respect for study participants, consent procedures and secure storage and maintenance of data. They also underwent survey-specific training and pretested the survey questionnaire; patient-exit surveys (online supplemental material 1). The quality of the collected data was maintained through daily supervisions, spot checking and reviewing the completed questionnaire by trained staff. The principal investigator and supervisors cross- checked the questionnaire for completeness, accuracy and consistency.
Supplemental material
Study variables
Dependent variable
The outcome variable is PS, defined as patients’ perceived needs and expectations in relation to factors, such as the healthcare provider and amenities. Satisfaction level was assessed using an 11-item Likert scale questionnaire. PS was then categorised as good and poor satisfaction using the median value, given that the data distribution was skewed.
Independent variable
The independent variables included sociodemographic factors, such as age, sex, education, marital status, reason for choosing the health facility, distance to health facility, waiting time and wealth index score. Wealth index was measured as a composite variable comprising of 11-item questionnaire using principal component analysis.
Data analysis
The collected data were exported into Stata V.15 for data cleaning and analysis. Both descriptive and analytical statistical procedures were employed. The statistical analysis included descriptive statistics, with data summarised using frequencies, percentages and graphs. To assess the presence of significant difference in the level of PS across health facilities, we applied χ2 tests.
A binary logistic regression model was used to identify factors significantly associated with PS. Initially, the association between each independent variable and the outcome variable was assessed using bivariate logistic regression analysis. Subsequently, those variables with p value less than or equal to 0.2 were included in a multivariable logistic regression model to control for possible confounding variables. Finally, multivariable logistic regression analysis findings were presented using an adjusted OR (AOR) with their corresponding 95% CIs.
The research team then employed Hosmer and Lemeshow tests in order to assess the final model’s fit. Further, a multicollinearity test was performed using variance inflation factor (VIF) to test the presence of correlation among the independent variables included in the final model.
Results
Characteristics of respondents
Overall, 290 patients were included in the analysis. Table 1 reports the baseline characteristics. In total, 123 (42.4%) were in the age range of 21–30 years and about 85% of respondents were females. Pertaining to educational status, half (50%) had secondary education and above, while 42.4% had no formal education. 202 (69.7%) of the respondents were married. Three-quarters (76.2%) of the respondents reported that they travelled for less than an hour to access the health facilities. 128 (44.1%) of the participants reported that the waiting time to receive care is more than 2 hours (table 1).
Sociodemographic characteristics of respondents (N=290)
Patient satisfaction
The study showed that the overall PS was 63.8% (95% CI 58.1% to 69%). Around 69.2% (95% CI 62.1% to 75.4%) of the respondents from PIH intervention sites and 53.9% (95% CI 44.1% to 63.4%) from the non-PIH intervention sites had a good satisfaction level (figure 2). The findings also revealed that PS was high (76.7%) at Wellbody followed by Gandorhun (58.5%) health facility. Contrastingly, respondents who visited Kayima health facility reported low levels of satisfaction (44.1%). The difference in level of satisfaction among the health facilities was statistically significant (p value: 0.002) (table 2).

Level of satisfaction among the respondents (n=290). PIH, Partners In Health.
Level of PS by health facilities (n=290)
Motivations for visiting health facilities
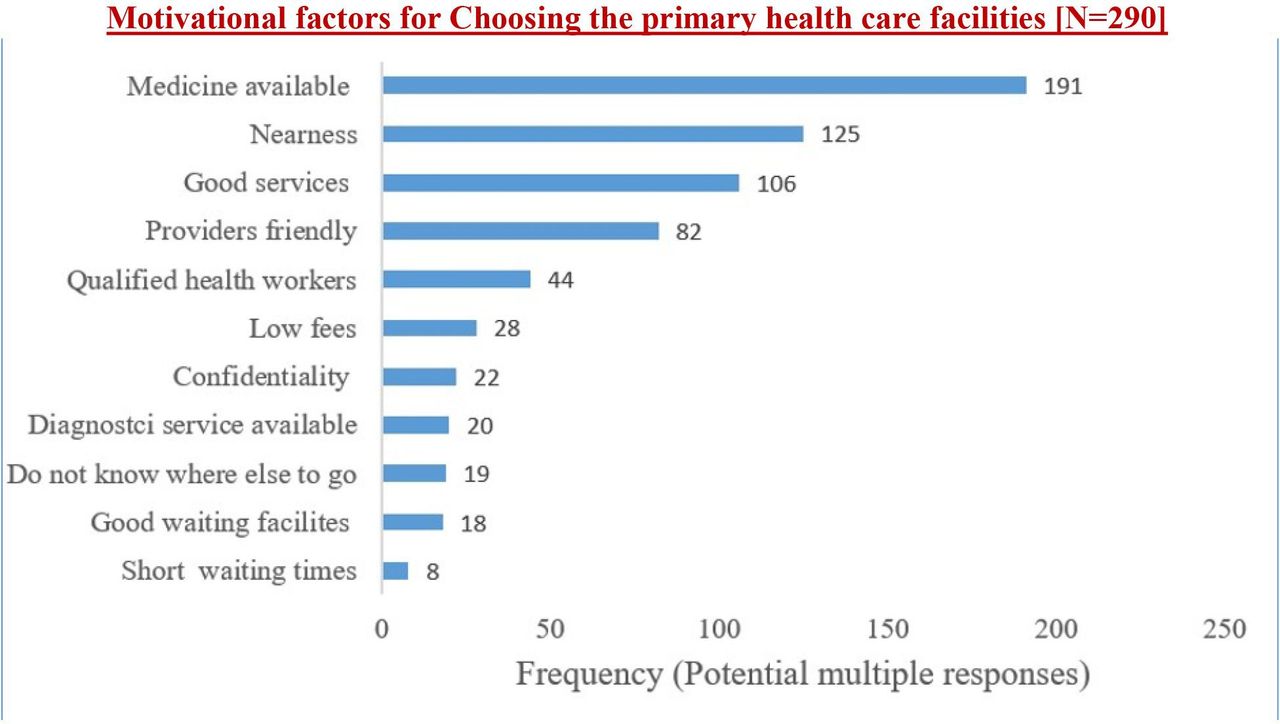
The motivations for visiting health facilities were mentioned by the study’s 290 respondents with an option to select multiple responses. The major motivations for visiting the health facilities were availability of medicines (n=191), accessibility (n=125) and good service provision (n=106). Further, the availability of friendly and qualified health workers were reported as a reason to visit these health facilities (figure 3).

{kind=link}
{kind=link}
{kind=link}
Motivational factors for choosing the primary healthcare facilities (n=290).
Factors associated with PS
Bivariable and multivariable binary logistic regression analysis model were fitted to identify the factors associated with PS. In the bivariable regression model, the variables age of respondent, marital status, occupation, gender, educational status, wealth index, distance to health facility, waiting time to receive care and being a PIH intervention site were included. With this, marital status, gender, occupation and educational status of respondents, were statistically insignificant at the bivariable regression analysis at a p value of 0.2. However, educational status was frequently reported as a predictor for PS in previous literature and considered for the multivariable analysis of this study accordingly. Hence, the variables age of respondent, educational status, wealth index, distance to health facility, waiting time to receive care and PIH intervention site status, were included for the multivariable binary logistic regression analysis.
The multivariable regression analysis indicated that being a PIH intervention site has a positive statistically significant association with PS after controlling for other variables. Respondents from PIH intervention sites had 2.5 times higher odds of satisfaction (AOR=2.47, 95% CI 1.28 to 4.78) as compared with those respondents from the non-PIH sites (table 3).
Bivariable and multivariable binary logistic regression analysis of factors associated with PS (n=290)
This study reported that those with a lower educational status have a higher PS. After controlling for other confounding factors, respondents who have secondary education and above had 47% lower odds of satisfaction (AOR=0.53, 95% CI 0.28 to 0.98) as compared with those who have no formal education.
After controlling for other variables, long distance to health facility was negatively associated with PS. Accordingly, those respondents who travelled for more than 2 hours to access the health facility had 60% lower odds of satisfaction (AOR=0.40, 95% CI 0.18 to 0.87) as compared with the reference category (table 3). Looking at waiting time to receive care, respondents who waited for more than 2 hours at the health facility had 59% lower odds of satisfaction (AOR=0.41, 95% CI 0.22 to 0.76) as compared with those who waited for less than 1 hour. The multivariable regression analysis also showed that the age of respondents and wealth index have no statistically significant association with PS (table 3).
Multicollinearity
Multicollinearity checks were performed among the independent variables included in the multivariable regression model. The test showed that the mean VIF was 1.92 and all included variables have VIF values of less than 10 with the maximum VIF value of 4.1 showing that there is no multicollinearity among the predictor variables.
Model fitness test
The Hosmer and Lemeshow goodness-of-fit test was statistically insignificant (p value=0.53) showing that the final model fits the data.
Discussion
This study revealed that around two-thirds 63.8% (95% CI 58.1% to 69%) of respondents have an impression of good satisfaction in the services provided in the health facilities, and a greater level of satisfaction was felt in the PIH-supported health facilities where the PS was 69%. Respondents’ educational level, distance to health facility and waiting time were predictors of PS.
This finding corroborates with a finding in Ethiopia and Nigeria, which revealed that about 65% and 59.3% of the respondents, respectively, were satisfied with the health services provided.6 13
The high level of satisfaction seen in this study could be attributed to the deliberate effort made to strengthen healthcare systems and quality of care after the Ebola pandemic in Sierra Leone.
The study also showed that respondents from PIH-supported health facilities have reported a higher PS level. This relatively higher level of PS is enumerated in the survey and relates to PIH’s 5S model of healthcare delivery under which the staff are augmented, mentored and supported—providing friendly, dignified care and improved supply chain—resulting in the availability of medications and diagnostics at all times, and social support, in the form of expanded accessible healthcare.
In line with this, in another study, it was also reported that patients seek quick and convenient health services.14 15
The overall PS level is, however, clearly lower than the findings of studies conducted in the following low- and medium-income countries (LMICs): Ethiopia (77%),16 Nigeria (94%),17 Nigeria (78%),18 Tanzania (72.8%)19 and India (80%).8 The difference might be because those studies were conducted in different contexts, including referral hospitals, which are equipped very well and have enough diversity of health professionals of different levels that are expected to demonstrate the standard way of patient examination, resulting in higher level satisfaction. Further, the Nigerian study also included private health facilities that might affect the PS positively, given that these health facilities are profit making.17
Timeliness of healthcare services at the primary healthcare level impacts positively on the perception of quality of services rendered to patients. The findings from this study showed that PS decreased with an increase in perceived length of waiting time. This is in agreement with findings from previous studies.14 16 18 20 21 However, increased wait time could be associated with the high patient load that is suggestive of good services, including adequate staffing and staff capacity building to provide quality healthcare.9 The long waiting time could also be attributed to the free service provision at Wellbody Clinic with indirect consequence on the PS.15 The predictive finding of short waiting time is expected, as patients do not want to pay much higher economic costs while accessing health services. This is an important opportunity cost in a developing country, such as Sierra Leone. The finding of cost of services as a predictor of PS is in accordance with a report from Nigeria18 where high cost was found to be a negative determinant of PS.
In this study, lower educational status of a patient is significantly associated with higher PS level (p<0.05, 95% CI 0.28 to 0.98). Studies in primary care services also indicated that there were significant differences in satisfaction with health services in terms of educational level.7 14 22 This suggests that the 5S model has its intended outcome as it was designed to increase access to and quality of care for the poor (who have fewer options for care). It may also be explained by the exaggerated expectations for high standard of care among the educated respondents.
Distance to health facility was associated with PS that is consistent with a finding reported from a primary healthcare facility.22 Similarly, the patient’s perceived accessibility of health service was the strongest predictor of general satisfaction reported by a study conducted in Uganda.23 This could be explained by the effect of distance on travel costs, time and productivity related to inaccessibility of health service. A study by Dibba et al. also reported that distance to health facility posed a significant challenge for many patients in rural contexts of Sierra Leone where transportation costs made it difficult for patients to attend health facility appointments.15 The study also emphasised that patients were willing to walk long distances to the PIH-supported health facilities to obtain free medication.15
Among the socioeconomic variables, a study by Geberu et al. reported that OPD PS was significantly affected by age and gender.7 However, our study reported that the association was not statistically significant.
This study also pointed out that some major motivations for visiting the health facilities were availability of medicines, accessibility, good service provision, and availability of friendly and qualified health workers. A study from Nigeria also indicated that the ability of the healthcare provider to offer explanations clearly to patients was a predictor of PS.17 Another study from India reported that friendliness of the care provider, explanations the care provider gave about the problem and information the care provider gave about medications and follow-up care are among the major reasons for good satisfaction after receiving health service.8
Implications for policy and practice
Patients seek timely and convenient services when using healthcare. Though the findings from this study highlighted relatively better levels of PS, this study pointed out the factors that need to be considered to further improve PS in primary healthcare facilities. With this, health facilities leadership needs to give attention to improve their patient’s positive experiences when they use their health facilities.
In recent years, there has been a growing interest in PS as a measure of outcome and quality of care as it provides information on how well health service providers meet patients’ values and expectations. This study pointed out that the major motivations why patients visit health facilities are availability of medicines, accessibility, good service provision and availability of friendly and qualified health workers, highlighting the need to improve quality of care and service characteristics to optimise the PS level at the PHU level. This implies that PS structured interventions should be put in place in a systematic way according to the MoH standards of care. This will improve treatment adherence3 and, by extension, health outcomes.
The amount of time spent to see a health worker was also a significant predictor of PS. This also demands appropriately addressing the patient flow, staffing, and service expansion to improve both accessibility and quality of care. These call for refocusing to improve the overall patient care in the local context and meet the patient needs at the PHU level.
Our findings also show that PIH interventions in augmenting MoH healthcare service delivery by the 5S model are highly effective in improving PS with respect to healthcare system performance.
Limitations
This was a facility-based cross-sectional study conducted in selected health facilities from one district. This might limit generalisability to the national Sierra Leone context. The finding of this study might also be subjected to recall bias and social desirability bias because the respondents were interviewed within the health facilities compounds. Despite this situation, participants still shared important critiques of their experiences at the selected facilities and services. Even though the sample size included all patients who visited the five facilities during the study period, we acknowledge that the characteristics as well as the findings from these patients might not be representative of the general population.
Furthermore, perceptions of patients potentially affected by their cultural beliefs and previous experiences were not captured qualitatively. Future studies should look into these. We used multivariable logistic regression model to control for confounding, but we also acknowledge that it cannot control for residual confounding and other uncaptured risk factors.
Finally, we chose dichotomisation of the outcome variable (satisfaction level) to provide a clear and interpretable division of satisfaction levels, particularly to give more insightful information in a clinical context where clear thresholds can aid in decision making. However, we acknowledge that PS may not be fully captured by a binary categorisation, and also, dichotomising the outcome variable can cause information lost.
Conclusions
The overall PS level was relatively high and PIH-supported health facilities have better PS as compared with non-PIH-supported health facilities. Patient’s educational status, distance to health facility and waiting time were negatively associated with PS level. Therefore, we recommend that adequate attention should be paid to the expansion of advanced primary care to improve service accessibility and improving several aspects of service provision, such as waiting time and staffing in a way that addresses high patient flow. Moreover, PIH’s philosophy of targeted investment can be scaled up and the MoH should implement policies for improving the quality of services provided by primary healthcare professionals. Further, large-scale studies that include qualitative perspectives of health workers and patients are recommended.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. This study was approved by The Sierra Leone Ethics and Scientific Review Committee (SLESRC). Approval by: efoday@mohs.gov.sl. Regarding the reference number, the SLESRC was not issuing reference numbers to approve ethical clearance letters during this period. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to thank the Ministry of Health, Partners In Health and health facilities leadership for supporting this research work. We are also grateful to the data collectors and study participants. Finally, we extend our gratitude to Emily Dally, Chiyembekezo Kachimanga, Mohamed Bailor Barrie, Pierre Ricard Pognon, Jourdan McGinn, Annie Michaelis and Jean Claude Mugunga for their technical support during the conduct and write-up of this study.
Footnotes
X @siwatson
YD and FB contributed equally.
Contributors YD, FB, JGJ, VC, SJ and ZAM conceived and designed the study. YD, FB, SIW, LC, JH, KPM, JM and ZAM performed the data analysis, data interpretation and drafting the manuscript. All the coauthors reviewed and approved the final manuscript. YD is the guarantor of this manuscript.
Funding This study was conducted with support from Wagner Foundation. We will also want to thank Burroughs Welcome Fund for supporting ZAM as a Research Specialist supporting this study.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.