Article Text

Abstract
Objective In a recently published 4-year overall survival (OS) update from the phase III clinical trial named HIMALAYA (NCT03298451), single tremelimumab plus regular interval durvalumab (a regimen termed STRIDE) demonstrated significantly improved OS compared with sorafenib in the first-line setting of unresectable hepatocellular carcinoma (uHCC). Although dual immunotherapy represents a novel treatment option for uHCC, the economic implications of these high-priced drugs require further exploration. This study aimed to evaluate the cost-effectiveness of STRIDE in uHCC to inform first-line treatment decisions and help allocate medical resources most effectively.
Design Using a partitioned survival model, we conducted a cost-effectiveness analysis comparing STRIDE to sorafenib in the first-line treatment of uHCC. Clinical information was gathered from the phase III HIMALAYA trial. Costs and health state utilities data were derived from previous literature. Uncertainty of the model was assessed through one-way sensitivity analysis and probabilistic sensitivity analysis.
Outcome measures Total costs, life years, quality-adjusted life years (QALYs), incremental QALYs and incremental cost-effectiveness ratio (ICER).
Setting US payer perspective.
Participants 393 participants in the STRIDE group and 389 participants in the sorafenib group who were diagnosed with uHCC and had no previous systemic treatment.
Interventions Single-dose tremelimumab plus monthly durvalumab (STRIDE) versus sorafenib.
Results Treatment with STRIDE provided an additional 0.51 QALYs at an incremental total cost of United States dollar ($)9812. The ICER of STRIDE was $19 239 per QALY compared with sorafenib, which falls below the willingness-to-pay threshold of $150 000 per QALY. Sensitivity analyses indicated that our results were robust to the variation ranges of key inputs.
Conclusion In this economic evaluation comparing two first-line systemic therapies for uHCC patients, STRIDE was cost-effective compared with sorafenib from a US payer perspective. Our study is the first to demonstrate that immunotherapy can provide both survival benefits and economic viability in uHCC.
- Drug Therapy
- HEALTH ECONOMICS
- IMMUNOLOGY
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study built a partition survival model to evaluate the cost-effectiveness of tremelimumab plus durvalumab against sorafenib in unresectable hepatocellular carcinoma using the most recently published follow-up data from the HIMALAYA study.
We considered drug costs associated with first-line and subsequent therapy, as well as adverse events management costs, administration costs, costs of best supportive care, follow-up costs and costs of terminal care.
In order to explore the long-term cost and health gains beyond the follow-up observation time in the clinical trial, we extrapolated the survival curves through fitting parametric distributions, and this approach may introduce uncertainty.
To simplify the model, we only considered subsequent therapies with frequency greater than 1% and direct medical costs, which may result in an underestimation of overall costs.
Introduction
Liver cancer is the sixth most common cancer and ranks third in mortality rate.1 Hepatocellular carcinoma (HCC) represents approximately 75%–85% of all liver cancers, and more than 60% of HCC patients are diagnosed at an advanced stage, with no opportunity for curative resection.2 3 Targeted therapies, such as sorafenib and lenvatinib, have been the standard systemic therapies for unresectable HCC (uHCC) patients over the past decades, as they significantly improved the overall survival (OS) compared with placebo.4 5 In recent years, the introduction of immune checkpoint inhibitors (ICIs) has shown great therapeutic potential and has changed the clinical practice of many haematological and solid tumours. However, ICI monotherapies failed to demonstrate a survival benefit over sorafenib in randomised trials, prompting further exploration of ICI combination strategies for uHCC.6 7
Tremelimumab is a cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) inhibitor that exhibits complementary mechanisms of action with programmed cell death-ligand 1 (PD-L1) inhibitor.8 Durvalumab is an immunoglobulin G1 monoclonal antibody that blocks PD-L1 binding to PD-1 and CD80.9 The combination of a single high priming dose of tremelimumab (anti-CTLA-4) and regular interval durvalumab (anti-PD-L1) has shown additive antitumour activity associated with complementary immunostimulatory effects.10 11 The HIMALAYA trial, a randomised, multicentre, global, phase III study, was designed to evaluate tremelimumab plus durvalumab (a regimen termed STRIDE) versus sorafenib in patients with uHCC who had not been previously treated with systemic therapy.12 Recently, a 4-year OS update from the HIMALAYA trial revealed unprecedented long-term survival benefits of STRIDE, with one in four participants remaining alive at 4 years.13 Based on these findings, STRIDE is listed as a preferred first-line systemic therapy option for uHCC in the National Comprehensive Cancer Network (NCCN) guidelines of HCC.14
In the coming decade, immunotherapy combinations are likely to become the standard practice for uHCC. Another immunotherapy combination, atezolizumab plus bevacizumab (atezo-bev), was proven to be not cost-effective compared with sorafenib for patients with uHCC,15–18 although it showed survival superiority in clinical trials.19 Therefore, there remains a need to explore more economical immunotherapies which balance efficacy with economic viability. To date, no studies have assessed whether tremelimumab plus durvalumab (STRIDE)’s survival benefits and unique dosing schedule would yield favourable cost-effectiveness in uHCC. This study aims to conduct a comprehensive economic evaluation of STRIDE versus sorafenib from a US payer perspective, providing evidence to inform first-line treatment decisions in uHCC and optimise healthcare resource allocation.
Methods
Network meta-analysis
A systematic meta-analysis was conducted to identify eligible studies using electronic databases including PubMed, Embase and Cochrane Central Register of Controlled Trials until 13 March 2025. Phase III randomised controlled trials that compared immunotherapy combination regimens with sorafenib for uHCC patients in the first-line setting were included. Network meta-analysis was performed using R software (V.4.2.1, http: //www. r-project.org) with the package ‘gemtc’ to obtain the HR for OS between immunotherapy combinations.
Overview of cost-effectiveness analysis
Partitioned survival model was developed to investigate the cost-effectiveness of STRIDE versus sorafenib in uHCC. The outcomes included total cost, life-years (LYs), quality-adjusted life-years (QALYs) and incremental cost-effectiveness ratios (ICERs). We compared ICER between two groups at a willingness-to-pay (WTP) threshold of $150 000 per QALY. Both costs and effectiveness employed a 3% annual discount rate. Statistical analysis was performed in R software (V.4.2.1, https://www.r-project.org/). Our study was conducted and reported in accordance with the Consolidated Health Economic Evaluation Reporting Standards reporting guideline. No patients or members of the public were directly involved in the desigh or conduct of this study, as it is a retrospective analysis of aggregated clinical data.
Population and interventions
The medical information of patients was derived from the phase III HIMALAYA trial.12 Two treatment groups were evaluated in the model: (1) patients in the STRIDE group received 300 mg of tremelimumab for one dose plus 1500 mg of durvalumab every 4 weeks and (2) sorafenib 400 mg two times per day. When the disease progressed, 40.7% of patients in the STRIDE group and 45.0% in the sorafenib group received at least one subsequent treatment, and the remaining patients were considered to receive the best supportive care until death. Distribution of subsequent therapy was obtained from clinical trials,12 and only therapies with a frequency greater than 1% were considered (online supplemental eTable 1). After subsequent therapy, patients were assumed to receive the best supportive care. For drug dosing, a body surface area of 1.79 m2 (weight: 70.32 kg) was used in the mode.20
Supplemental material
Model structure
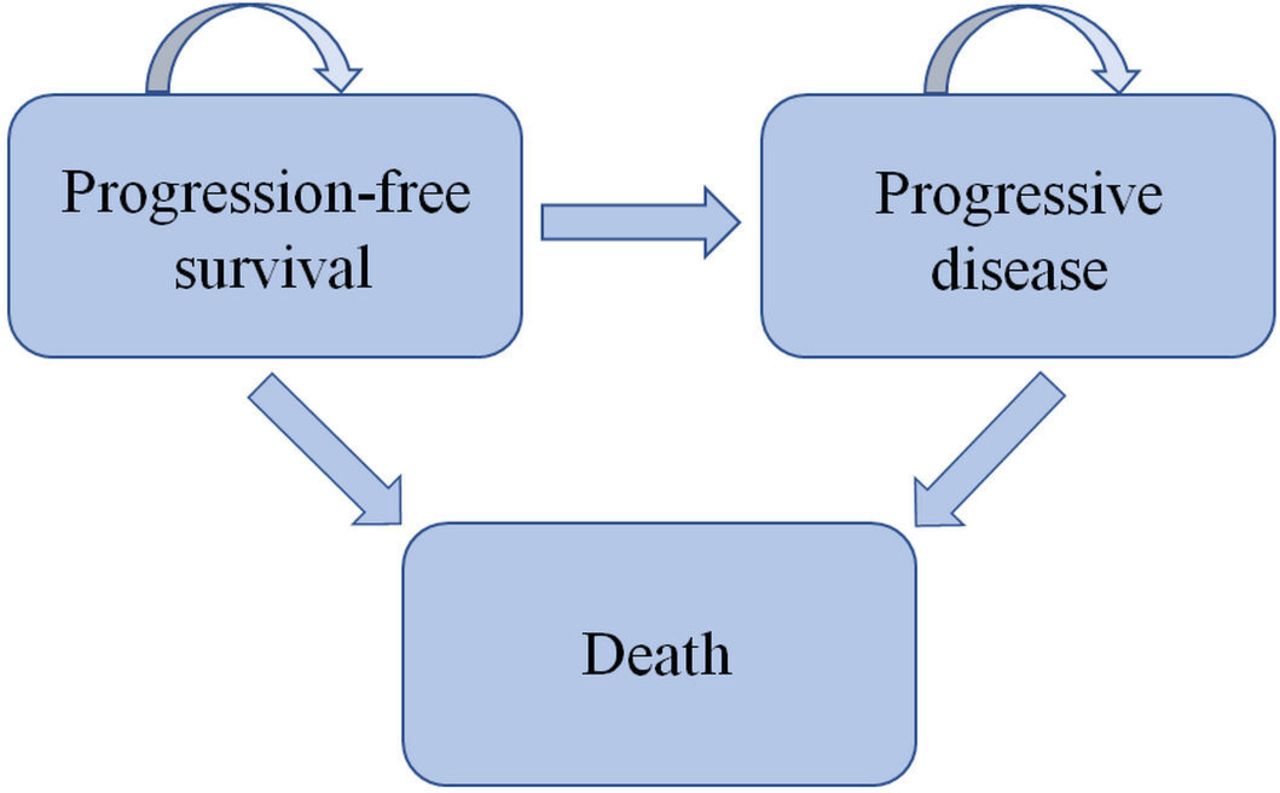
Partitioned survival model over a 20-year time horizon was constructed with a monthly cycle length. The model was developed in TreeAge Pro software (V.2022, https://www.treeage.com/). In this partitioned survival model, the distribution of patients in three independent health states (progression-free survival (PFS), progressive disease (PD) and death, figure 1) was obtained directly from the Kaplan-Meier survival curves of PFS and OS. The number of patients in the PFS state could be provided by the PFS curve, patients in the death state were determined from the remaining part of the OS curve, and patients in the PD state were the proportion between the PFS and OS curves.

Partitioned survival model.
PFS and OS curves were sourced from the HIMALAYA trial. Time-to-event data were extracted by GetData Graph Digitizer (V.2.26; http://www.getdata-graph-digitizer.com) and regenerated in R software using the method described in a study conducted by Guyot et al.21 Survival distribution including the exponential, loglogistic, Weibull, lognormal, Gompertz and generalised gamma distributions were tested according to the Akaike information criterion, Bayesian information criterion (online supplemental eTable 2) and visual inspection. Lognormal distribution was chosen for the PFS and OS data of the STRIDE, and loglogistic is the best fit for sorafenib (online supplemental eFigure).
Cost and utility estimates
This analysis considered only direct medical costs such as drug costs, adverse events (AEs) management costs, subsequent therapy costs, administration costs, costs of best supportive care, follow-up costs and costs of terminal care. Drug costs were collected from the Centres for Medicare & Medicaid Services22 and Drugs.com (https://www.drugs.com/).23 The administration costs were derived from the Medicare physician fee schedule.24 The costs of routine follow-up, including hospitalisations, medical staff visits and lab tests, were differentiated according to the PFS and PD status.25 AEs (≥grade 3) which occurred in more than 5% of the patients or severe immune-mediated AEs which occurred in more than 1% of the patients were covered (online supplemental eTable 3). The cost of AEs management, best supportive care and terminal care was sourced from published studies.22 26 27 All costs were inflated to 2024 US dollars using the Consumer Price Index.
Although the trial protocol specified that quality of life was evaluated with the European Organisation for Research and Treatment of Cancer 30-Item Quality of Life Questionnaire, the clinical effectiveness results were not reported in the article. The PFS and PD utility values of HCC patients were 0.76 and 0.68 respectively, according to a cost-effectiveness analysis.28 The disutility due to severe AEs (grade 3 and higher) was subtracted from the baseline utility.29 Information regarding the key costs and utility is listed in table 1.
Key variables for model
Sensitivity analyses
One-way sensitivity analyses and probabilistic sensitivity analyses were employed to assess the uncertainty in the model. One-way sensitivity analysis was conducted to identify the key factors that influence ICERs. A variance of ±20% of base-case values was employed for parameters. Probabilistic sensitivity analysis was conducted by running 10 000 Monte Carlo simulations with all parameters randomly sampled within a specific pattern of distribution (table 1).
Results
Network meta-analysis
After database searching, two clinical trials involving 729 uHCC patients were identified in the meta-analysis. In the HIMALAYA trial, 393 patients were treated with STRIDE, while in the clinical trial named IMbrave150, 336 patients were given atezo-bev. The control groups for these trials were sorafenib. From the results of the network meta-analysis, HR for OS of STRIDE versus atezo-bev was 0.87 (95% CI 0.70 to 1.09).
Incremental cost-effectiveness ratios
In the base-case analysis (table 2), the STRIDE group showed an additional survival benefit of 0.77 LYs compared to the sorafenib group (2.91 vs 2.14 LYs) in the treatment of patients with uHCC. Accounting for quality of life, STRIDE was associated with improved survivals of 0.51 QALYs (1.98 vs 1.47 QALYs). The total costs were $232 428 and $222 616 for the STRIDE and sorafenib groups, respectively, yielding an ICER of $19 239 per QALY. The results suggested that STRIDE was a cost-effective option compared with sorafenib at the WTP threshold of $150 000/QALY.
Results of base-case analysis
Sensitivity analyses
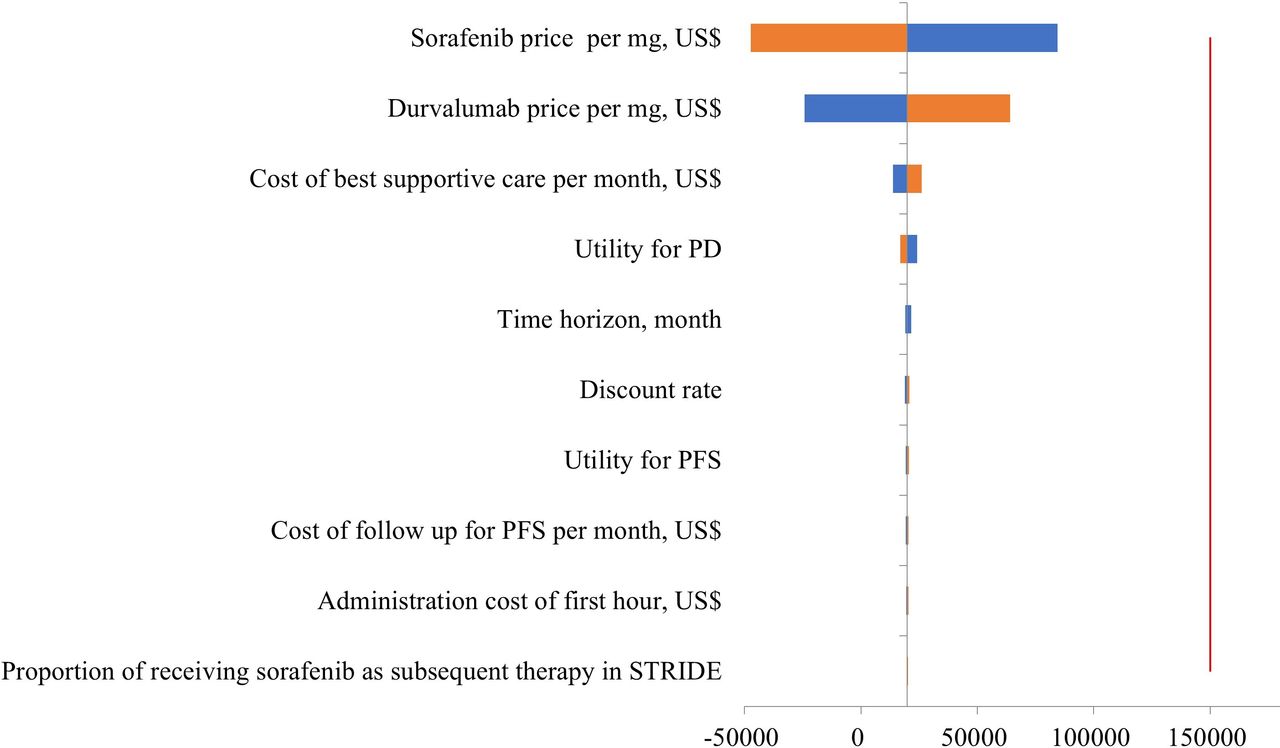
One-way sensitivity analysis showed that across the lower or upper limits of all tested parameters, STRIDE remained cost-effective compared with sorafenib, with ICER lower than $150 000/QALY (figure 2). The most influential variables were the price of sorafenib and durvalumab. But even if sorafenib price decreased to the lower limit ($0.72 per mg, $573.70 daily), or durvalumab price increased to the upper limit ($9.68 per mg, $14 527.08 per 1500 mg), ICER still fell within the WTP threshold ($84 536/QALY and $64 005/QALY, respectively). Other leading parameters, such as the cost of best supportive care per month, utility for PD and time horizon, had a minor impact with total ICER range from $10 000/QALY to $25 000/QALY. All parameters were proved to be unable to change the economic superiority of STRIDE over sorafenib. In probabilistic sensitivity analyses (figure 3), the probability of STRIDE being cost-effective was 99.9% at $150 000/QALY WTP threshold. If we set the WTP threshold at $100 000/QALY, STRIDE would still have a chance of >97% to be a cost-effective option over sorafenib.

Tornado diagrams of one-way sensitivity analysis. The line dividing the upper and lower limit represents the ICER of $19 913 per QALY. ICER, incremental cost-effectiveness ratio; PD, disease progression; PFS, progression-free survival; QALY, quality-adjusted life year; STRIDE, tremelimumab plus durvalumab; WTP, willingness-to-pay.

{kind=link}
{kind=link}
{kind=link}
Cost-effectiveness acceptability curves. QALY, quality-adjusted life year; STRIDE, tremelimumab plus durvalumab.
Discussion
HCC is one of the most common causes of cancer-related deaths globally, with limited treatment strategies. Sorafenib and lenvatinib have been the first-line systemic therapies of uHCC over the past decade. However, the prognosis with multikinase inhibitors remains poor, with a median survival time of approximately 1 year.4 5 Immunotherapies are considered the most promising treatments, but the combination of atezo-bev lacked economic viability towards sorafenib from a value-based perspective.15–18 The STRIDE regimen, which combines a single priming dose of tremelimumab with durvalumab, significantly improved OS versus sorafenib and led to tremelimumab’s approval as the second immunotherapy for uHCC after atezolizumab.30 To our knowledge, this study is the first economic evaluation analysing the cost-effectiveness of the STRIDE regimen, and we found that STRIDE was cost-effective compared with sorafenib at a WTP threshold of $150 000/QALY, with an estimated ICER of $19 239/QALY. Thus, the STRIDE regimen seemed to be an attractive option in the first-line setting of uHCC.
The base-case analysis showed that STRIDE achieved an incremental effectiveness of 0.51 QALYs with a total cost increase of $9812, producing an ICER below the WTP threshold. One-way sensitivity analysis indicated that the cost-effectiveness superiority of STRIDE was highly unlikely to change in the variation range of any parameters. Drug prices of sorafenib and durvalumab could have a significant effect on ICER. However, testing sorafenib price at its lower limit or durvalumab price at its upper limit did not change the preferred status of STRIDE.
High-priced immunotherapies are often considered to impose a financial burden on patients and the healthcare system. However, the STRIDE regimen has a unique design, with a high priming dose of tremelimumab acting as a ‘trigger’ for the effect of durvalumab. Results from HIMALAYA indicated CTLA-4 inhibition might have driven the long-term OS benefit in the STRIDE arm.12 Considering that the addition of a single dose of tremelimumab was sufficient to add clinical activity to durvalumab, the monthly drug cost of the STRIDE arm was $12 106 (1500 mg of durvalumab every 4 weeks) after the initial tremelimumab cost of $40 827. Meanwhile, the monthly drug cost for sorafenib (two times per day) was $21 514 in the targeted therapy arm. After calculating other medical costs, the total cost difference between these two groups was minimal, yielding an ICER substantially below the WTP threshold. Since there is no consensus on the WTP threshold in the USA, previous studies have used values ranging from $100 000/QALY to $150 000/QALY.31 32 We adopted the most frequently used WTP threshold of $150 000/QALY, at which STRIDE had a 99.9% probability of being cost-effective. Even if the WTP threshold was lowered to $100 000/QALY, probabilistic sensitivity analyses revealed that STRIDE would still have a >97% probability of being cost-effective.
In 2020, the IMbrave150 trial reported superior OS and PFS outcomes for atezo-bev compared with sorafenib, opening a new era of systemic therapy for HCC. However, corresponding cost-effectiveness analyses indicated that the healthcare costs of dual immunotherapy treatment were not balanced with its survival benefits from a value standpoint. Studies by Chiang et al,15 Su et al17 and Zhang et al18 reported ICERs of $179 729/QALY, $169 223/QALY and $322 500/QALY, respectively, all exceeding the WTP threshold of $100 000/QALY or $150 000/QALY. Although HRs were an influential parameter in determining ICERs in some of the studies, they were difficult to change through policy interventions. Consequently, they recommended substantial price reductions for atezolizumab and bevacizumab or capping immunotherapy duration to <12 months for achieving efficient use of this regimen. Moreover, Chiang’s model was sensitive to body weight, suggesting that reducing the dosage of bevacizumab to 10 mg/kg would make atezo-bev to be cost-effective.15 Further optimisation of the price, duration and dosage for atezo-bev is necessary to mitigate the financial burden associated with long-term immunotherapy use. An economic evaluation from the Chinese and American payers’ perspective has taken into account medical insurance policies in different countries.16 China has a relatively low total cost of $95 973 for atezo-bev group because of drug donation programmes. The ICER in China and the US was $145 546/QALY and $168 030/QALY, respectively, exceeding the Chinese WTP threshold of $28 527/QALY and US WTP threshold of $150 000/QALY. This research proved that although affordability patterns vary widely around the world, atezo-bev was not a cost-effective option for countries with different income levels. In the NCCN guidelines of HCC, both STRIDE and atezo-bev are listed as preferred first-line systemic therapy options. Due to the absence of phase III trials comparing immunotherapies head-to-head, we performed a network meta-analysis for an indirect comparison between STRIDE and atezo-bev. The results showed an OS HR of 0.87 (95% CI 0.70 to 1.09) for STRIDE versus atezo-bev. Given STRIDE’s survival advantage and lower total cost, it emerges as the dominant treatment strategy compared with atezo-bev. Other recommended options in the NCCN guideline were also evaluated in pharmacoeconomic research. The cost-effectiveness analyses conducted by Chiang26 and Li33 suggested that pembrolizumab and nivolumab were not a cost-effective therapy compared with sorafenib for HCC in the USA, and a systematic review indicated that most ICIs lack cost-effectiveness in comparison with tyrosine kinase inhibitors.34
Another potential way to improve economic outcomes is to select certain patient populations who respond well to immunotherapy. Su et al17 conducted subgroup analysis and found several subgroups in the atezo-bev arm, including patients with hepatitis B or C and patients with low α-fetoprotein level, were associated with better incremental net health benefits and >50% probability of being cost-effective in comparison with sorafenib. HCC is now increasingly recognised as a heterogeneous tumour with diverse tumour biology and immunotherapy responses.35 Analyses of tumour tissues from patients enrolled in the IMbrave150 trial reported several biomarkers linked to better clinical response to atezo-bev combination, such as CD274, T-effector signature and CD8+T-cell density.36 To date, no biomarkers have been validated for predicting survival benefits in routine clinical practice. Future adoption of molecular correlates of clinical response to immunotherapies may improve their economic value as first-line systemic therapy for uHCC.
Our study had several limitations. First, to explore the long-term cost and health gains beyond the follow-up observation time in the clinical trial, we extrapolated survival curves through fitting parametric distributions, a method that may introduce uncertainty. However, given that we updated OS data to the latest 4-year analysis of the HIMALAYA trial,13 which is the longest follow-up to date in uHCC, the robustness of the model can be guaranteed by the application of mature and reliable survival data. Some studies have shown that flexible parametric survival analysis models demonstrate higher credibility in extrapolating complex functions compared with standard parametric models.37 38 When further real-world data become available, we will consider hybrid models to enhance alignment with real-world treatment patterns. Second, the distribution of subsequent therapy was obtained from the HIMALAYA trial. Subsequent therapies with a frequency >1% were considered, and remaining patients were assumed to receive best supportive care. Although practice patterns at centres enrolling in pivotal clinical trials are representative, subsequent therapy options may vary according to clinician judgement and the specific situation of patients. To address this limitation, we performed one-way sensitivity analysis and Monte Carlo analysis, which indicated that the subsequent therapy costs had little influence on our results. Third, this analysis considered only direct medical costs. Since direct non-medical costs and indirect costs (eg, transportation costs and loss of productivity) are difficult to study, most cost-effectiveness analyses only include direct medical costs, which may result in an underestimation of overall costs. In the USA, when formulating coverage policies, payers primarily prioritise direct medical costs which impact budget allocation and reimbursement decisions. As we focused on the US payer perspective, direct non-medical costs and indirect costs have a relatively small impact on our results.
Conclusions
In conclusion, tremelimumab plus durvalumab (a regimen termed STRIDE) was cost-effective compared with sorafenib in the first-line setting of uHCC at a WTP threshold of $150 000/QALY from a US payer perspective. Sensitivity analyses showed that the results were robust and not substantially changed across the variation ranges of parameters. This study demonstrated that STRIDE was the first immunotherapy to achieve both survival benefits and economic viability in uHCC.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
I certify that no individuals other than the listed coauthors contributed to this publication.
References
Footnotes
Contributors Study conception and design were contributed by JX and SL. Data collection was contributed by BL and LT. Data analysis and interpretation were contributed by SC. Manuscript preparation was contributed by SC. JX acts as guarantor of the paper. All authors have critically revised the manuscript for important intellectual content, approve of the final version to be published and agree to be accountable for all aspects of the work. Final approval of the manuscript was contributed by all of the authors.
Funding This research was funded by the Natural Science Foundation of Hunan Province, grant/award number: 2022JJ80114.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.