Article Text

Abstract
Objectives The prevalence of adverse cardiometabolic health markers has increased substantially in UK young adults, and university students now make up a significant proportion of this population. Their health-related behaviours are poorer than age-matched normative data, and students’ anthropometric outcomes deteriorate during their university career. The influence of university on cardiometabolic health markers is unclear, and men and students of Minoritised Ethnicity are often under-represented in student health research. This study aimed to determine the prevalence of adverse cardiometabolic health markers in undergraduate university students and assess differences between genders, ethnic groups and year of study.
Design Observational cohort study.
Setting A higher education institution in Nottingham, UK.
Participants Three independent cohorts of undergraduate university students (total n=1,299) completed five physiological tests and provided demographic information. One-way ANOVAs assessed differences between year of study and ethnic groups, and paired samples t-tests assessed differences between genders.
Main outcome measures Body mass index (BMI), waist circumference, waist to hip ratio (WHR), waist to height ratio (WHtR), blood pressure (BP) and glycated haemoglobin concentrations (HbA1c).
Results 34.5% had overweight or obesity, 7.6% had a ‘very high’ waist circumference, 11.0% had a high WHR, 25.5% had a high WHtR, 12.7% were classified as hypertensive and 3.0% had an HbA1c ≥42 mmol/mol, indicating impaired glucose regulation. Differences between year groups were present for diastolic BP and HbA1c (p<0.01). Gender and ethnic group differences (p<0.05) were present for all variables other than BMI (gender) and diastolic BP (gender and ethnic group).
Conclusion Overall, these data demonstrate the prevalence of adverse cardiometabolic health markers in UK undergraduate university students, highlighting differences between year groups, genders and ethnic groups. These findings should be considered when developing strategies to promote healthy lifestyles in higher education.
- Hypertension
- General diabetes
- EPIDEMIOLOGY
- PUBLIC HEALTH
- Overweight
- Obesity
Data availability statement
Data are available upon reasonable request. The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The current study included an extensive, diverse sample which incorporated substantial numbers of underrepresented subpopulations in health-based research (ie, men and students of minoritised ethnicity).
Data were collected following the COVID-19 pandemic. University stakeholders can therefore use these results to inform health-based initiatives within a post-COVID-19 society.
A limitation of the study is the between-subjects design, meaning longitudinal changes cannot be inferred. Furthermore, biochemical measures were not included in the study but would be informative in enhancing the understanding of students’ cardiometabolic health.
Introduction
In 2021, the UK saw 2.9 million students enrolled in higher education.1 University students currently constitute a considerable proportion of the nation’s young adult demographic, with half of school leavers opting to pursue higher education.2 Worryingly, substantial proportions of university students are reported to have problematic dietary habits,3 4 be physically inactive,3 engage in extensive periods of sedentary behaviour4 5 and partake in high levels of binge drinking.4 Ultimately, these poor behaviours can have negative consequences for cardiometabolic health, with UK students experiencing considerable increases in body mass (+>0.5 kg),6 waist circumference (+1.9 cm)7 and body fat percentage (+0.8%)8 through their university career. Furthermore, the prevalence of students (outside of the UK) presenting with at least one risk factor for cardiometabolic syndrome (MetS) ranges from 0.3% to 13%.9 10 However, within the UK, higher education encompasses unique cultural, social and educational factors (ie, behavioural habits, style of tuition and opportunities for socialising)11–15 that can contribute to the health status of university students. As such, it is unclear whether previous findings are translatable to the UK student population.
Moreover, the context of student health has changed substantially in recent years with significant alterations to the delivery of education and typical daily living routines due to the COVID-19 pandemic.16 17 Indeed, throughout this period, university students developed considerably poorer movement, nutrition and sleeping behaviours18–20 leading to adverse trends in anthropometric outcomes.21 Furthermore, there is evidence to suggest that markers of health and related behaviours remain poorer than prior to the pandemic following the removal of restrictions.22 As such, it is reasonable to suggest that prepandemic data are no longer representative of the current student health landscape and that up-to-date baseline data are required to develop health promotion policy and practices, and longitudinal data collection is needed to assess the efficacy of these.
Additionally, the diversity of the UK student population has increased considerably in recent years.1 From a health perspective, this may be important given that gender and ethnicity play a substantial role in the development of adverse cardiometabolic health markers in the general population.23 24 Indeed, MetS is 0.5–1.5 times more prevalent in minoritised ethnic groups,25 and men observe different anthropometric outcomes to that of women.6 26 However, men and minoritised ethnicity students are often under-represented within these studies, meaning results cannot be generalised to the wider student population.
Ultimately, to inform the development of effective strategies to improve health in university students, studies must strive to include participant samples that are reflective of the current student demographic. Therefore, the aim of the present study was to identify the prevalence of adverse cardiometabolic health markers in UK university students and assess gender and ethnic disparities. It was hypothesised that students who are men and students of minoritised ethnicity would have poorer cardiometabolic health outcomes.
Methods
Participants and setting
University students completed a battery of five physiological tests in the first 3 weeks of term one, in one of three academic years (2021–22 n=347; 2022–23 n=422; or 2023–24 n=530). Using opportunistic sampling in communal spaces on campus, 1299 undergraduate students at a single institution in the midlands of England completed the testing and formed the cohort analysed in this study. All participants provided informed consent prior to taking part in the study, and ethical approval was granted by the School of Science and Technology Human Ethics Committee of Nottingham Trent University (application ID: 19/20–76). The study is reported in line with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for observational studies.27
Physiology testing battery
The battery of testing included measurements of height, body mass, waist and hip circumferences to enable the calculation of body mass index (BMI), waist to hip ratio (WHR) and waist to height ratio (WHtR). Height and body mass were measured without shoes or heavy clothing using a stadiometer (Seca, Hamburg, Germany) and a digital weighing scale (Seca, Hamburg, Germany). Waist and hip circumferences were assessed using a flexible measuring tape and in accordance with International Society for the Advancement of Kinanthropometry (ISAK) guidelines.28 Systolic and diastolic BP were determined using commercially available arm and wrist BP cuffs (Omron, Japan). In 2021-22 and 2022-23, BP was assessed from the upper right arm, whereas in 2023-24, BP was measured from the right wrist in an attempt to improve participant experience. Within both methods, BP was determined in accordance with manufacturer guidelines. Agreement between arm and wrist BP has previously been shown to be good,29 and data from our own laboratory showed a strong correlation (r=0.717) between the two methods for systolic BP in undergraduate students. Glycated haemoglobin concentration (HbA1c) was determined using a fingertip blood sample analysed using the Quo-Test HbA1c analyser (EKF Diagnostics, UK).
Data analysis
Descriptive data are reported as mean±1 SD and percentages are presented to demonstrate the proportion of participants classified into ‘risk’ categories for BMI,30 waist circumference,31 WHR,31 WHtR,32 BP33 and HbA1c34 based on well-established global guidelines. To characterise students’ current physical health status, data were combined to form a single cross-sectional dataset. For the purposes of analysis in this study, participants were then categorised by year at university (first, second and third year), gender (men and women) and ethnicity (White, Asian, Black and other minoritised ethnicities). If participants did not state a year group, gender or ethnicity, they were included in overall population data but excluded from analysis between year, gender or ethnic groups.
A one-way Analysis of Variance (ANOVA) was conducted to assess differences between year of study as well as ethnic groups. This test was used despite variables not meeting the assumption of normal distribution, as currently there is not a widely accepted non-parametric alternative for sample sizes substantially larger than n=30.35 36 Group variance was assessed through Levene’s test, and homogeneity among variables was determined when the significance value was greater than 0.05 (p>0.05). To test the assumption of sphericity, Mauchly’s test was employed, assuming sphericity when the test yielded a non-significant result (p>0.05). In cases of violation, the Greenhouse–Geisser correction was applied. Furthermore, for evaluating effect sizes, partial eta squared (ηp2) was used, with effect magnitudes categorised as follows: small (0.02–0.12), medium (0.13–0.25) and large (>0.26).37 Post hoc tests were performed using the Bonferroni correction to determine significant differences between year of study and ethnic groups (p<0.05). Gender differences were examined using an independent samples t-test. Cohen’s d (d) was used to gauge effect sizes, categorised as trivial (<0.2), small (≥0.2), medium (≥0.5) or large (≥0.8) effects.38 Significance was established at p<0.05, and the analysis was conducted using IBM SPSS Statistics (SPSS V.28.0, Chicago, IL).
Patient and public involvement
The study did not include the involvement of participants or the general public in its design. Nonetheless, all participants were informed about the research objectives, and their informed consent was obtained. Participants completed the testing voluntarily, and their input was not solicited for interpreting or writing the results.
Results
The sociodemographic characteristics of the 1299 participants included in the study are presented in table 1.
Participant information data presented as n (%)
Anthropometric measures
The mean pooled data for body mass, BMI, waist circumference, WHR and WHtR are shown in table 2. The prevalence of students at ‘high risk’ for adverse cardiometabolic health markers is displayed in online supplemental table 1. Having a BMI ≥25.0 was the most common risk factor for poor cardiometabolic health, followed by having a high WHtR (≥0.5).
Supplemental material
Pooled cross-sectional data for all variables
When separated by gender, the prevalence of overweight and obesity was highest in men; however, the prevalence of very high waist circumference, WHR and WHtR was highest in women (online supplemental table 1). When separated by ethnicity, the prevalence of overweight and obesity and very high waist circumference was highest in Black students, whereas the prevalence of high WHR and WHtR was highest in Asian students (online supplemental table 1). Across the year of study, the prevalence of overweight and obesity, and very high waist circumference was highest in third year students, while the prevalence of high WHR and high WHtR was highest in first year students (online supplemental table 1).
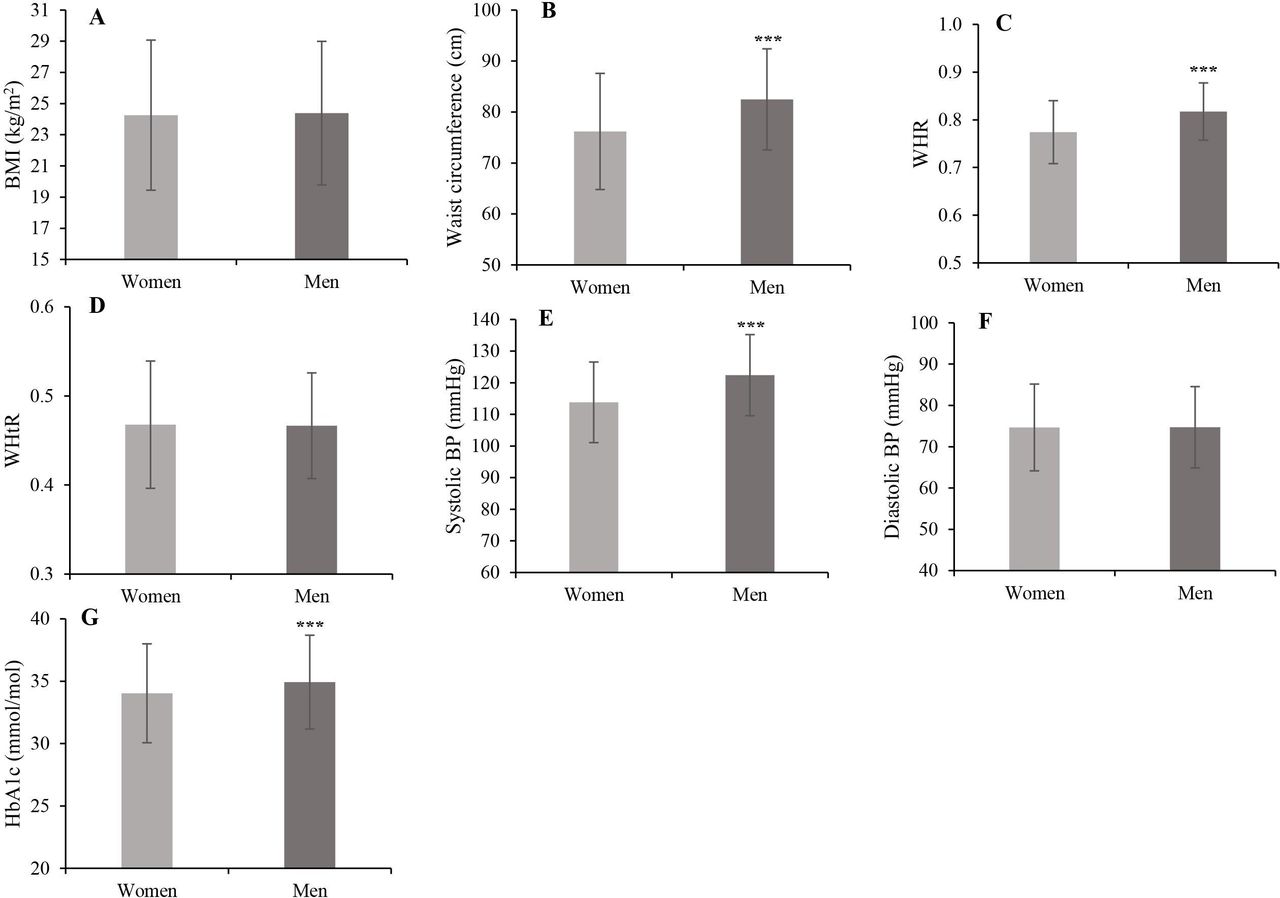
A main effect of gender was observed for waist circumference and WHR. Overall, men had a greater waist circumference (t=−9.10; p<0.001) and a larger WHR than women (t=−10.59; p<0.001) with medium effect sizes (d=0.6 and d=0.7, respectively) (figure 1B,C). No gender differences were observed for BMI or WHtR (p>0.05) (figure 1A,D).

Displays the differences between gender for the reported variables. ***p<0.001; **p<0.01 compared with women. BMI, body mass index; BP, blood pressure; HbA1c, glycated haemoglobin concentrations; WHR, waist to hip ratio; WHtR, waist to height ratio.
A main effect of ethnicity was observed for BMI (p<0.001), waist circumference (p=0.01), WHR (p<0.001) and WHtR (p<0.001) with small effect sizes (ηp2=0.02, ηp2=0.01, ηp2=0.02 and ηp2=0.02 respectively). Overall, Black students and students of other minoritised ethnicities had a higher BMI than White students (p<0.05) and Asian students (p<0.05) (figure 2A). Black students also had a higher waist circumference than Asian students (p=0.02) (figure 2B). White students had a lower WHR than Asian students (p=0.04) and students of other minoritised ethnicities (p<0.01) (figure 2C). White students also had a lower WHtR than all other ethnic groups (p<0.05) (figure 2D).

Displays the differences between ethnic groups for the reported variables aaap<0.001 compared with White and Asian students; aap<0.01 compared with White and Asian students; bp<0.05 compared with Asian students; cccp<0.001 compared with White students; cp<0.05 compared with White students; dd p<0.01 compared with White students; dp<0.05 compared with White students; eeep<0.001 compared with Asian students; eep<0.01 compared with Asian students; ee*p<0.01 compared with Black students; ggg p<0.001 compared with White students. BMI, body mass index; BP, blood pressure; HbA1c, glycated haemoglobin concentrations; WHR, waist to hip ratio; WHtR, waist to height ratio.
No main effect of year of study was observed for any anthropometric variable (p>0.05) (figure 3A–D).

{kind=link}
{kind=link}
{kind=link}
Displays the differences between year groups of study for the reported variables ffp<0.01 compared with second year students and ggp<0.01 compared with second year and third year students. BMI, body mass index; BP, blood pressure; HbA1c, glycated haemoglobin concentrations; WHR, waist to hip ratio; WHtR, waist to height ratio.
Blood pressure
The mean systolic and diastolic BP in 1290 students is shown in table 2, and of these, 12.7% were classified as being hypertensive (online supplemental table 1). The prevalence of hypertension was higher in men compared with women (online supplemental table 1). When separated by ethnicity, the prevalence of hypertension was highest in White students (online supplemental table 1). Across year groups, the prevalence of hypertension was highest in third year students (online supplemental table 1).
Men had higher systolic BP than women (t=−10.52; p<0.001) with a medium effect size (d=−0.7), but no difference between genders was found in diastolic BP (p=0.47) (figure 1E,F). Additionally, a main effect of ethnicity was observed for systolic BP (p<0.001) with a small effect size (ηp2=0.05). Asian students had lower systolic BP than all other ethnic groups (p<0.01) and Black students had lower systolic BP than White students (p<0.001) (figure 2E). No main effect of ethnicity was found for systolic blood pressure (p=0.06) (figure 2F). A main effect of year of study was found for diastolic blood pressure (p=0.03) with small effect size (ηp2=0.01). Post hoc tests revealed third year students had higher diastolic blood pressure than second year students (p=0.01) (figure 3F). No main effect of year of study was found for systolic blood pressure (p>0.05) (figure 3E).
HbA1c
The mean HbA1c in 926 students was 34.0±4.0 mmol/mol (table 2). Of these, 3.0% were classified as ‘high risk’ for developing type 2 diabetes (online supplemental table 1). The prevalence of poor glycaemic control was similar between men and women (online supplemental table 1) and highest in Black students (online supplemental table 1). When separated by year of study, the prevalence of impaired glucose control was highest in first-year students (online supplemental table 1).
Men had a higher HbA1c compared with women (t=−3.14; p<0.001) with a small effect size (d=−0.23) (figure 1G). Furthermore, a main effect of ethnicity was observed for HbA1c (p<0.001) with a small effect size (ηp2=0.06). White students had lower HbA1c compared with Asian (p<0.001) and Black students (p<0.001) (figure 2G). A main effect of year of study was observed with a small effect size (p<0.001; ηp2=0.02), specifically first year students had a higher HbA1c than second year students (p=0.001) and third year students (p=0.02) (figure 3G).
Multiple risk factors
The prevalence of multiple adverse cardiometabolic health markers is presented in online supplemental table 1. A greater proportion of men had one or two adverse cardiometabolic health markers compared with women (online supplemental table 1). Additionally, the prevalence of multiple adverse cardiometabolic health markers was similar between ethnicities and year groups (online supplemental table 1).
Discussion
The results of the present study provide comprehensive up-to-date baseline data surrounding the prevalence of adverse cardiometabolic health markers in UK university students. Additionally, the findings demonstrate that year of study, gender and ethnicity all play a substantial role in determining markers.
Comparisons to UK population data
In general, average health data collected for all markers in the current study falls within healthy ranges.30–32 34 39 Encouragingly, the prevalence of overweight or obesity and very high waist circumference among students was somewhat lower than UK age-matched normative data (34.5% vs 37.0%–7.6% vs 16.0%, respectively).40 However, the prevalence of hypertension (9.0%) was slightly higher in students than that of UK young adults,40 as was the prevalence of impaired glucose regulation (1.59–1.77%).41 Comparisons cannot be made for WHR and WHtR due to a lack of population level data. Overall, these data suggest that university life does not substantially impact the health of young adults in comparison to non-students. While this may be interpreted as a positive finding, it should be noted that university campuses are a relatively controllable environment within which key stakeholders are able to provide access to facilities, services and information in a single setting to promote health.42 Therefore, the comparability of poor health markers to that of the wider UK general population may be considered as disappointing.40 41 Additionally, higher education institutions should be cognisant of the substantial negative trends in health-related behaviours of students in recent years,18–20 meaning that it is likely the prevalence of poor cardiometabolic health markers will increase. It is therefore critical that university stakeholders use these data as a baseline to aid in the development of effective surveillance systems and, where appropriate, effective intervention strategies to ensure that optimising student health remains a priority for successive generations.
Gender
In line with previous literature, the current study demonstrates that, on average, men had higher values for waist circumference, WHR, systolic BP and [HbA1c] compared with women.43–46 Additionally, the prevalence of overweight and obesity and hypertension was also greater in men than women, whereas the prevalence of very high waist circumference, WHR and WHtR was higher among women than men. These differences may be explained by genetic factors including differences in the distribution of fat and muscle mass between men and women as well as differences in hormonal concentrations (ie, upregulation of testosterone and downregulation of oestrogen in men compared with women) that mean men are at greater risk of developing adverse markers of body composition and health (eg, BP and HbA1c).47 48 However, previous literature in students has also demonstrated behavioural differences between men and women that could impact these health-related variables. Specifically, men have been shown to engage in poorer eating behaviours4 and greater levels of alcohol drinking in comparison to women,4 49 who develop poorer movement3 4 50 and sleep habits,4 51 as well as having poorer indicators of mental health.4 52 These data add to existing literature by further demonstrating the existence of disparities in health markers between genders in university students. Higher education institutions should therefore adopt a gender-centred approach when developing future initiatives to improve students’ health.
Ethnicity
Data from the current study area are consistent with previous literature, indicating that minoritised ethnic groups experience a greater prevalence of adverse health markers in comparison to White Europeans.24 Specifically, these findings highlight that Black and Asian students are at the greatest risk of developing poor anthropometric outcomes and impaired glycaemic control. This could be because they experience greater barriers to conducting physical activity,53 develop poorer nutrition behaviours54 and have poorer sleep habits55 compared with their White counterparts. In contrast, adverse BP findings were more prevalent in White students compared with minoritised ethnic students, providing conflicting evidence to previous literature.56 Although behavioural factors are important, a plethora of genetic, socioeconomic, religious, cultural, environmental and social differences also likely play a role in determining these health markers. As such, identifying the complex system within which these factors interact is far beyond the scope of the current study. Nonetheless, the present study provides novel information surrounding nuanced variations between students from different ethnic backgrounds.
Year of study
Findings from the current study show a main effect for year of study on body mass, with an overall trend towards higher body mass from first year to third year. Additionally, third-year students had higher diastolic BP than second-year students. These findings are supported by data indicating that the prevalence of overweight and obesity, very high waist circumference and hypertension were highest among third-year students. Taken together, these findings align with previous literature indicating that students observe substantial weight gain throughout their university career6 57 as well as increased BP during periods of critical assessment.58 Previously, this has been attributed to the development of poor behavioural habits and psychological markers while at university.57 59 However, no effect of year of study was observed for any other anthropometric outcome in the current data. Hence, this may be attributed to the typical age of university enrolment often coinciding with the latter phases of adolescence during which physical maturation may still be occurring due to neurological development.60 Alternatively, this could be owing to positive health behaviours leading to increased skeletal muscle mass.61
Mean [HbA1C] was higher in first year students compared with second and third year students, and the prevalence of impaired glycaemic control, high WHR and high WHtR was greatest in first year students. These data may be considered surprising given that evidence suggests behavioural outcomes become poorer during the transition to, and across the first year of university.7 62 However, the context of health behaviours in early adulthood has shifted dramatically in recent years with technological advancements in conjunction with the COVID-19 pandemic promoting poorer behaviours such as reduced physical activity, increased screen-time, increased snacking and emotional eating that have all become habitual.20 63–65 It is therefore possible that attending university provided students with an opportunity to engage in a positive lifestyle shift which incorporated more social opportunities to engage in healthful movement behaviours and less reliance on food as a means of combating boredom or improving emotional states. Additionally, despite a plethora of literature demonstrating that health status and behaviours in youth influence health later in life,66 it is plausible that the window during which these poor behaviours are developed while at university (~3 years) is not chronic enough to begin negatively influencing physiological markers of health in young people. However, there is currently not enough robust longitudinal data to quantify whether this is an accurate assumption. Regardless of the reason, the findings of the current study provide vital insight into how markers of cardiometabolic health may be altered across the timeline of an undergraduate degree. However, there is a distinct need for need for further longitudinal studies that incorporate substantial sample sizes in order to adequately assess the impact of university life on health and behaviours. This will ultimately provide vital insight into health and lifestyle factors that require targeted initiatives to aid higher education institutions in producing healthy and economically active alumni that will positively contribute to the wider UK society.
Strengths and limitations
A major strength of the current study is the extensive, diverse sample of UK undergraduate students. This included large numbers of men and students of minoritised ethnicities who have previously been underrepresented in the research area.6 50 As such, these findings provide vital, novel insight into the health status of different gender and ethnic groups of students. Furthermore, data were collected during the years following the COVID-19 pandemic. These results can therefore be used as a current baseline by key stakeholders to inform future decisions surrounding the development of initiatives to improve the health of university students and track changes in a post-COVID-19 society.
The between-subjects nature of the study design means that longitudinal changes cannot be inferred, but the large sample size within each year of study provides much-needed insight into potential differences across the timeline of a typical undergraduate degree. Nevertheless, future longitudinal studies with large student numbers should be developed to gain an in-depth understanding of trajectories in students’ cardiometabolic health throughout an undergraduate degree programme. While the current study has excellent representation within students of minoritised ethnicity, the more complex distinction between ethnicity and culture, including potential differences for international students, was not within the scope of this study and should be investigated in the future. Finally, the current study did not include biochemical markers (ie, HDL-cholesterol, LDL-cholesterol, total cholesterol and serum triglyceride) that have been shown to be important in the screening of poor metabolic health in university students.10 However, the processes required to collect such data would require participants to be fasted, which could substantially reduce the study sample size.
Conclusion
The current study provides up-to-date data surrounding markers of cardiometabolic health in university students. On average, data falls within healthy ranges and the prevalence of adverse outcomes is largely similar to that of age-matched young adults in the UK. While encouraging, the relatively controllable environment in which many undergraduate students reside provides university stakeholders with opportunities to optimise health in their student populations. The current data demonstrate that gender and ethnicity play a key role in determining markers of cardiometabolic health, and therefore these factors must be considered when developing and implementing interventions. Furthermore, researchers in student health should work together to collect representative data within this population, to further elucidate differences between student populations, and to develop, test and implement successful health interventions for students.
Data availability statement
Data are available upon reasonable request. The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was granted by the School of Science and Technology Human Ethics Committee of Nottingham Trent University (application ID: 19/20-76). Participants gave informed consent to participate in the study before taking part.
References
Footnotes
Contributors MJS, RMJ and PH were responsible for study conceptualisation, data collection, data analysis and drafting of the manuscript. ELP and AGP contributed to data collection and drafting of the manuscript. DM contributed to drafting of the manuscript. All authors have read and agreed to the published version of the manuscript. MJS acted as the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.