Article Text

Abstract
Objectives To explore Aboriginal and Torres Strait Islander Australians’ perceptions of telehealth general practice consultations and elements required for a culturally safe telehealth consultation.
Design Qualitative study.
Setting Primary care telehealth in three centres in regional and remote Australia.
Participants Seventeen Aboriginal or Torres Strait Islander individuals participated in semistructured interviews exploring the experiences of telehealth in general practice settings. Participants were eligible for inclusion if they were Aboriginal or Torres Strait Islander, over 18 years of age and had experienced at least one telehealth appointment with their general practitioner in the preceding 12 months. Data were collected in the form of short surveys and semistructured interviews. Data collection occurred between June 2022 and August 2023. Data were analysed using thematic and content analysis techniques.
Results Participants had experienced telephone (88%) and videoconference appointments (12%). Reasons for choosing telehealth included being unable to attend due to respiratory symptoms and/or COVID-19 restrictions on in-person consultations (reflecting the study period) and issues of access (eg, availability of doctor, convenience of hours). Participants described benefits of telehealth around reduced barriers to care but also described practical and communication challenges experienced during telehealth. Elements of culturally safe telehealth identified included: consultation skills, a pre-existing doctor-patient relationship and local knowledge (including knowledge of the local cultural and community context).
Conclusion This study demonstrates the benefits of telehealth and its ability to reduce barriers to care for Aboriginal and Torres Strait Islander Australians. However, the identified disadvantages demonstrate that this modality should be considered as an addition to, rather than a replacement for, face-to-face consultations. The elements identified interact as part of a complex interplay of factors contributing to cultural safety in the telehealth context. These elements provide useful recommendations for practice and policy.
- Primary Care
- Telemedicine
- Safety
- Australian Aboriginal and Torres Strait Islander Peoples
Data availability statement
Data are available upon reasonable request. The datasets analysed during the current study are not publicly available due to participants’ potential identifiability because of the small dataset. Data are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study sought Aboriginal and Torres Strait Islander individuals’ experiences and perspectives to explore how cultural safety can be enhanced within telehealth.
In-depth data were obtained from participants (n=17) in both regional and remote Australia.
Study participants had predominantly experienced telephone consultations (rather than videoconference or other telehealth modalities). Cultural safety within telephone consultations has not been significantly explored in the previous telehealth literature.
Participants were predominantly women (n=15), which may be due to the influence of a female interviewer.
Introduction
The medical system, and society more broadly, experienced significant shifts from 2020 due to the COVID-19 pandemic. One such change was the widespread introduction of telehealth, including in primary care.1 In Australia, telehealth was relatively rare within general practice prior to COVID-19.1 2 However, expanding telehealth funding to include general practitioners (GPs) in response to the COVID-19 pandemic altered this picture significantly.1
Australian healthcare is funded under Medicare; a government-funded universal health insurance scheme that subsidises medical consultations, investigations and procedures.3 Prior to COVID-19, Medicare funding of telehealth was limited to specialist or Royal Flying Doctor Service consultations and only in restricted situations (eg, significant geographical distance to services).1 4 5 While the informal use of telehealth was relatively common (eg, in follow-up of results), the lack of funding meant that telehealth was not economically feasible in private general practice based on fee-for-service.4 As a result, telehealth accounted for only 0.1% of all government-funded consultations.2
Expansion of funding due to COVID-19 caused a rapid uptake of telehealth in general practice. This increase in telehealth usage continued into the post-COVID-19 era. In 2023, 33.5 million telehealth consultations were conducted in Australia, constituting 17% of total Medicare-funded services. Within general practice, telehealth represented 20% of funded services (27.8 million consultations).6 Significantly, the majority of telehealth consultations conducted in Australia were conducted by telephone (87%), with videoconference making up the remaining 13%.6
Medical professional bodies have released best-practice telehealth guidelines in response to the increased popularity of this form of healthcare.7 8 However, these guidelines do not explore how cultural safety can be achieved in the telehealth setting.
What is cultural safety?
Cultural safety is recognised as a vital aspect of medical care, improving healthcare access and reducing health inequities. The health of Aboriginal and Torres Strait Islander Australians continues to be impacted by the ongoing effects of colonisation and experiences of racism and inequality.9 Thus, ensuring culturally safe health services is one way to improve access to care and improve health outcomes.
The term ‘cultural safety’ was coined in the ‘90s,10 but the elements required for a culturally safe consultation remain difficult to define.11 Identifying elements of cultural safety is complicated by the diversity of terms and definitions in use, as well as the intrinsic differences between what individuals, communities and countries may consider to be culturally safe.11 12
The term ‘cultural safety’ is one of many terms which have been used in the literature and practice. Other terms in use include cultural sensitivity, cultural competency, cultural respect, cultural humility, cultural security and cultural appropriateness, among many others.10 13–16 However, the distinctions between these terms are not always clear or consistent.10 11
For example, the authors of one review proposed that cultural competency was predominantly related to building cultural knowledge and developing an awareness of one’s own background.17 Cultural safety was seen as a higher level of skill, which included both practical skills and knowledge, as well as considering patient-defined outcomes of care.17
Other authors have proposed that cultural awareness, safety and security reflect a sequence of skills which build on one another.15 Through this lens, cultural awareness is seen as knowledge-based (eg, understanding an aspect of culture). Cultural safety is then viewed as the application of this knowledge into practice. Cultural security is considered the highest level of skill, integrating individual knowledge and actions and incorporating appropriate policies and procedures.15
By contrast, some authors have identified cultural humility (rather than security) as the highest level of skill. Cultural humility is defined as a transformative process by which a person’s perspective is changed, becoming aware of power differentials and acting with humility at all times.18 These conflicting views on terminology and definitions can create uncertainty and contribute to a lack of clarity in this field.
However, since this research is situated within an Australian context, we will use the definition developed by the Aboriginal and Torres Strait Islander Health Strategy Group for the Australian Health Practitioner Regulation Agency. This definition, included below, was developed in consultation with the community and uses the term ‘cultural safety’. Thus, the term cultural safety was used in this study and is defined as below.
‘Cultural safety is determined by Aboriginal and Torres Strait Islander individuals, families and communities. Culturally safe practise (sic) is the ongoing critical reflection of health practitioner knowledge, skills, attitudes, practising behaviours and power differentials in delivering safe, accessible and responsive healthcare free of racism.’19
This definition recognises first the importance of cultural safety being determined by Aboriginal and Torres Strait Islander individuals and communities. It also identifies elements that contribute to cultural safety, for example, knowledge, skills and attitudes. This definition has been recognised by medical regulators and colleges, including the Australian Medical Council and the Royal Australian College of General Practitioners.20 21
Culturally safe telehealth
Practitioner and environmental attributes contributing to culturally safe telehealth for Indigenous people have been explored previously.22 Practitioner attributes for culturally safe care included their community and cultural knowledge, building and maintaining of clinician-patient relationships and communication skills.22 Environmental factors included technology, the availability of support staff and the telehealth setting (eg, soundproofing, ensuring privacy and confidentiality).22 Importantly, few studies have explored the cultural safety of telehealth in primary care, with most studies situated within a specialist mental health context. In addition, most studies explored videoconferencing or store-and-forward consultations (where data are transmitted to a remote clinician who replies with a plan).22 Thus, current literature has not investigated cultural safety in telehealth relevant to the Australian general practice context.
The aim of this project is to explore the experiences of Aboriginal and Torres Strait Islander people with telehealth in primary care and understand perspectives on what makes a telehealth consultation culturally safe in this setting.
Methods
This study used a constructivist framework23 to allow exploration of patient preferences and experiences of telehealth with their GPs through a narrative qualitative approach. The concept arose from a concurrent study exploring cultural safety within face-to-face consultations, derived from experiences of staff at a participating Aboriginal Community-Controlled Health Organisation (ACCHO).24 The onset of COVID-19 prompted the need to explore cultural safety within telehealth.
Participants were required to be Aboriginal and/or Torres Strait Islander, over 18 and have had at least one experience of telehealth in the preceding 12 months. Inclusion criteria did not set a minimum number of telehealth experiences to avoid excluding participants who may have had a negative experience and thus not proceeded with further telehealth appointments. Participants were recruited within participating ACCHOs, identified through partnerships developed in the research team’s previous work. The study was conducted from June 2022 to August 2023.
Participants completed a short survey including demographic information and questions about identity, followed by a semistructured interview exploring preferences and experiences of telehealth consultations and cultural safety in this context. The interview also explored the importance of factors identified within cultural safety literature (eg, use of traditional language, including family in consultations, or the practitioner’s knowledge of Australian history). The full interview guide can be found in online supplemental appendix 1. This was based on the protocol used in the study by Brumpton et al exploring cultural safety in face-to-face general practice consultations.24
Supplemental material
All participants provided written informed consent to participate in this study. Member checking of transcripts was offered to all participants. Seven participants requested a copy of their transcript, which was sent by email or registered mail depending on participant preference. None of these participants made any changes to their transcript.
The interview was conducted in person for 16 participants and via telephone for one participant. The choice of in-person versus telephone was dependent on participant preference. Interviews were conducted by HW, who is not Aboriginal or Torres Strait Islander. The advisory group determined that HW was an appropriate person to conduct the interview.
Demographic data were analysed using descriptive statistics. When exploring the reason for telehealth consultation/s, any reason provided by the participant was coded. More than one reason could be provided by a participant. Interview data were transcribed using Sonix. Thematic and content analysis was conducted by two independent researchers, facilitated by NVivo and informed by Braun and Clark’s methodology.25
HW, TSG and LM are academic GPs with clinical and research experience in Aboriginal and Torres Strait Islander health. KB is a clinician researcher and senior GP within a participating ACCHO. RE is a health services researcher with experience in qualitative and mixed-methods research. RW is an Aboriginal health academic from Kunja Nations.
This study received ethical approval through the James Cook University Human Research Ethics Committee (H8296).
Patient and public involvement
This project was developed from another which explored cultural safety in face-to-face general practice consultations. This initial project was developed in partnership with a local ACCHO. The COVID-19 pandemic began during this initial study, causing the question of telehealth to be raised.
Through this study, an advisory group of local leaders and community members provided oversight and review of the project and associated processes. The advisory group was formed within the ACCHO with whom the study was designed. The group included patients, local leaders and health professionals, all of whom identified as Aboriginal and/or Torres Strait Islander.
Results
Seventeen participants were recruited from three ACCHOs within southern Queensland (table 1). Participating ACCHOs were spread over a large geographical area (750 km between the most distant sites). The data were felt to have reached thematic saturation after 17 participants, and thus data collection was ceased.
Participant demographics
Reasons for telehealth
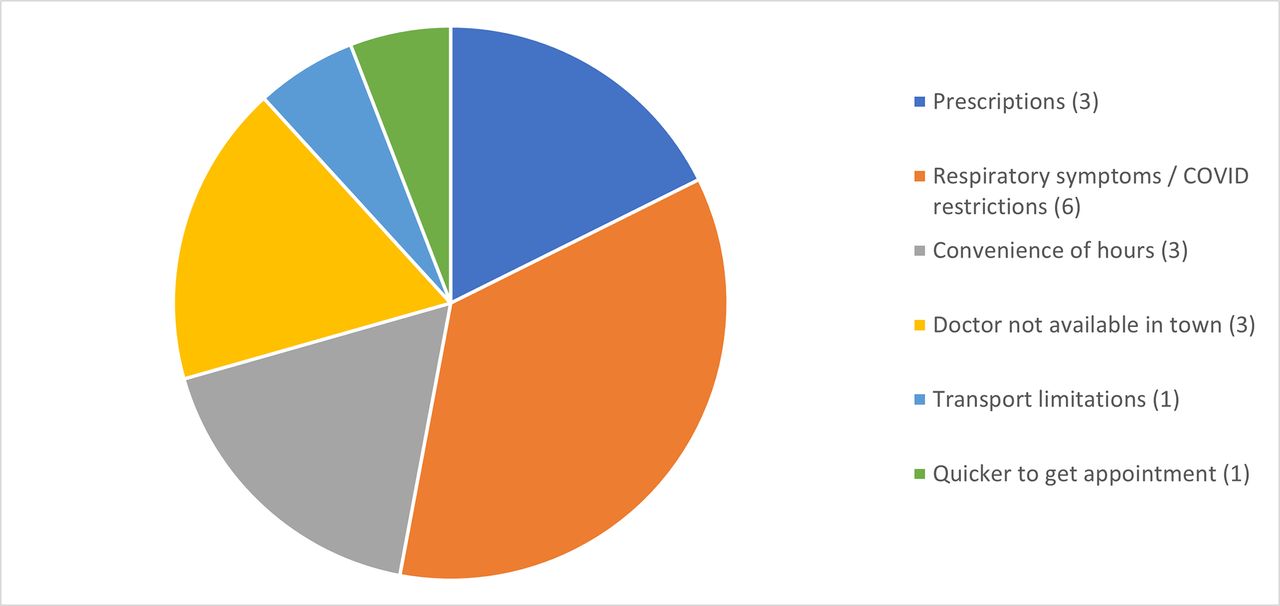
Participant reason/s for using telehealth consultations are outlined in figure 1. Some participants used telehealth because of the nature of their presenting complaint. This included being unable to attend due to respiratory symptoms and restrictions on in-person consultations due to COVID-19 public health recommendations. Some participants also indicated they would preferentially select telehealth if they only required prescriptions.

Reasons for participant selection of telehealth as a modality for consultation.
Telehealth was also selected due to convenience (accessing an appointment from work or outside of business hours) or due to doctor availability (eg, a GP was not available locally, making telehealth the only local option). All patients who reported using telehealth due to GP unavailability were in a remote location, while all participants citing convenience were from a regional location.
Benefits of telehealth
The benefits of telehealth reported by participants centred around the potential for telehealth to improve access to care. This included reducing practical barriers such as transportation and time efficiency.
The majority of the time I haven't got transport. (1714)
It’s just a lot easier for that script from your doctor’s appointment over the phone to get sent to the chemist. It cuts out a lot of time. (7966)
Telehealth (specifically telephone consultations) also allowed people to access care without their physical appearance being visible, which was felt to reduce fear of judgement or concerns about their image.
I would rather not have them see what I look like sometimes… It avoids them assuming things about my personal life. (5014)
What you’re wearing, your appearance, all of that thing, all of that feels a bit more relaxed on the phone. (7966)
Finally, some participants described feeling that a telehealth consultation was less stressful.
I've actually found it better talking over the phone, to be honest…Maybe because I'm a bit more relaxed. (6892)
Because I don’t have to come into the building and sit around a lot of people. It’s just over the phone, so it makes it a lot easier. (9095)
Disadvantages of telehealth
Participants also described disadvantages of telehealth. Practical constraints of telehealth included the lack of physical examination and potential technological challenges.
I'd like to get my blood pressure checked. All of that kind of stuff. I think the weight checked all of that, sugar tested. Yeah. So that’s the huge disadvantage. (7966)
I'm not very, computer wise. (8609)
Participants also described communication challenges including the lack of translators and the challenges of communication without non-verbal cues.
There might not be a translator that can translate directly if the doctor’s working from home. (4226)
If you're not seeing someone’s facial expressions…you don't know what they're really thinking. (8840)
Some participants described a lack of control in the telehealth setting. Participants felt a lack of control around being able to choose their preferred GP or feared that their concerns may not be heard or acted on. In some cases, this was manifested in the practical fear that the promised script would not arrive.
I suppose with telehealth you just get a random doctor too. (4226)
You can’t see my expression but can you understand my concern?… I’ll just go down there because I probably won't get the outcome I'm expecting (by telehealth). (3218)
You’re getting that script sent to my chemist. It hasn’t arrived. Oh, I shoulda just went to the doctors and got my script in my hand. (7966)
Finally, participants also described feeling overall that telehealth was different. This related to communication, but also to the challenge of the doctor-patient relationship in this setting. Participants described feeling that the experience of seeing a doctor in person was more ‘honest’ than a telehealth consultation. The difference experienced in a face-to-face consultation was partially attributed to the presence of non-verbal communication. However, some participants did not seem able to fully express why a telehealth consultation felt different, only that it felt less real or ‘true’.
There’s something about when you’re sitting with a doctor, it’s a lot more honest and true. (4226)
I always feel weird when I'm not sitting in front of someone talking to them….it just feels like you're not really talking to someone. (5014)
Culturally safe telehealth
Four elements were identified as important for culturally safe telehealth (see figure 2).

{kind=link}
{kind=link}
Elements of culturally safe telehealth. GP, general practitioner.
Consultation skills
Consultation skills, including communication skills, respect and holistic care, were valued by participants. Participants gave specific suggestions about appropriate communication for culturally safe telehealth.
Ask them some indirect questions before you start the direct questions. (4226)
Don't speak above us. Speak at our level where we understand. (8278)
Mutual respect was also valued and expected.
I treat them with respect and that’s how they treat me. (1714)
My advice is we’re all human. We all get treated the same. It doesn't matter what, just respect is all anyone asks for, not just Aboriginal. (7599)
Participants also preferred holistic and personalised care, considering the priorities and challenges of the individual person.
Don’t make it just like it’s got to be a 15 minute consult. If the consult turns into an hour, it does, because blackfellas like to talk. (4226)
Understanding that, okay, wow, she’s not feeling this good right now. Let’s get her in [arrange for an in-person consultation] and let’s get her to see somebody or, you know, a specialist or something like that. (6892)
Relationship
Participants also highlighted the importance of a pre-existing relationship with the doctor. This relationship contributed to the acceptability and safety of the consultation, with the reverse being true when the doctor was not known to the patient.
We can’t trust him because we don't know him. (7674)
If you’ve got a doctor that’s just knows you just straight off the bat, then you’re comfortable with that doctor. (6892)
Cultural knowledge
Participants identified the importance of cultural knowledge, including understanding the context and culture of the individual patient. An understanding of culture was felt to be important to the patients’ health and for culturally safe care.
Understand their culture, where they’re coming from, their background. If you have to sit and yarn for a little bit then, sit and yarn for a little bit. And take the time to listen to them, really listen because there’s a lot of them are hurting. And that’s all they want is that doctor that will listen, take note, understand their culture, be culturally aware. (6892)
People should definitely be briefed on our culture because it’s very important when it comes to health. (5014)
Community knowledge
Finally, community knowledge was vital, as expressed through the importance of the GP having visited the community to demonstrate commitment to the community and interest in local culture.
I reckon they should come here… they should sit with the people and even part of the community with the Aboriginal people and, and sit with them. And then that’s the only way they’ll know. (7674)
If they’re going to do the telehealth or even in person, they’ve got to want to, want to come and do it and they want to mingle with Indigenous culture. (6307)
Discussion
This study explored Aboriginal and Torres Strait Islander people’s experiences and preferences around telehealth and the features which contribute to a culturally safe telehealth consultation.
Participant preferences
Participant rurality impacted on reasons for accessing telehealth. Remote participants identified having used telehealth because a GP was not physically available in their town. Conversely, regional participants cited accessibility issues related to convenience of hours (rather than the absence of any doctor). This reflects the general maldistribution of the GP workforce in Australia, that is, decreasing workforce with increasing rurality.26 27 The most common reason for choosing telehealth was the presence of respiratory symptoms and/or COVID-19 restrictions, in keeping with the timing of this study.
The impact on barriers to care demonstrates telehealth’s value in primary care provision. However, the challenges of telehealth demonstrate the need for ongoing availability of in-person appointments for those who do not want telehealth or where telehealth is not appropriate. This is a particular challenge in remote areas, where telehealth may at times be the only option available.
The majority (88%) of participants in this study had experienced telephone appointments (rather than videoconference or other modalities), consistent with Australian national data.28 Participants described the lack of video contact as both a potential disadvantage and benefit in this study. These findings are particularly useful in the Australian context where telephone consultations are common. Experiences may vary in regions where videoconference is the more common telehealth modality.
Culturally safe telehealth
A key aim of this study was to identify features contributing to culturally safe telehealth for Aboriginal and Torres Strait Islander people. Several of the identified features are not unique to the telehealth setting. Many of the consultation skills described (eg, respect, communication and holistic care) mirror the consultation skills taught more generally as best practice.29 30 Similarly, the importance of the doctor-patient relationship has been described elsewhere, both by patients and healthcare professionals.31–33 The importance of community visits and cultural knowledge was highlighted in a recent literature review exploring cultural safety for Indigenous peoples in telehealth globally.22
Furthermore, there is likely to be significant overlap between the four features identified as important for culturally safe telehealth. For instance, community visits potentially improve cultural as well as community knowledge. Similarly, a pre-existing relationship is likely to impact communication and both cultural and community knowledge. Thus, these factors should not be seen as separate items on a checklist, but rather as a complex interplay of factors contributing to cultural safety within telehealth.
In addition, incorporating identified elements of culturally safe telehealth may reduce disadvantages of telehealth. For example, knowledge of the person’s computer literacy and context (eg, technology access) may help to reduce and overcome difficulties. Similarly, time constraints may be mitigated by an understanding of the patient, based on pre-existing relationship. Finally, telehealth with a known GP, with good communication and local and cultural knowledge, may decrease any perceived lack of control in telehealth by assisting the practitioner to understand the patient’s priorities and context.
Finally, many of the features described in this study are not unique to the Aboriginal and Torres Strait Islander population. While specific cultural features were identified in this study, the importance of relationship with a GP, good communication skills, holistic care and even community visits is likely to be relevant to a wider population.
Limitations
This study was conducted in an Australian context within rural and regional settings. It is possible that urban contexts may exhibit some differences, particularly in the reasons for using telehealth. In addition, the female predominance (15 of 17 participants) should be noted. This may be related to the use of a female interviewer in this study. While the findings are likely to be transferable, future studies may consider purposively recruiting male participants for balance among participants. Data were not collected on whether families or caregivers were present in consultations. In addition, data were not collected on multiple consultations, and thus reasons for choosing telehealth were coded only once per patient. Finally, this study focused on telephone appointments, as this was the modality experienced by most participants. This focus on telephone interactions may have impacted participants’ attitudes to remote care modalities. Similar studies exploring other modalities of telehealth (such as videoconference or asynchronous telehealth such as store and forward) would be useful.
Recommendations for practice
Rural Aboriginal and Torres Strait Islander patients in this study found telehealth to be a vital healthcare resource.
Recommendations for doctors: doctors should recognise the role of telehealth in healthcare and attempt to offer it where desired/possible.
Recommendations for health systems: Medicare should expand funding to meet the growing needs of historically marginalised communities that may otherwise be unable to access healthcare.
Although telehealth may increase opportunities for access to care, this study identified disadvantages that must be considered.
Recommendations for doctors: doctors should familiarise themselves with the disadvantages of telehealth, such as limitations in access to support (eg, interpreters) and the perceived lack of control over the encounter, and work with health systems to mitigate these disadvantages. Doctors should also recognise that some patients will not prefer telehealth and provide alternatives where possible.
Recommendations for health systems: institutions which offer telehealth should develop robust systems to provide education and support to clinicians to mitigate disadvantages and ensure that non-telehealth appointments remain available.
Culturally safe telehealth is a complex interplay of factors including consultation skills, pre-existing therapeutic relationship/s and local knowledge of culture and community
Recommendations for doctors: doctors should be aware of the factors which make a telehealth consultation culturally safe and strive to put them into place within their daily practice. This may include trying to deliver holistic, person-centred care, communicating clearly without jargon, intentionally developing the doctor-patient relationship and/or seeking to learn about the local community and cultural context.
Recommendations for health systems: health systems should strive to engage GPs who have the necessary consultation skills to provide culturally safe telehealth. Health systems should work to reduce GP turnover in primary care to enhance the development of therapeutic relationships which promote culturally safe telehealth. Ongoing clinician education should be provided to foster development of skills which can improve cultural safety, such as telehealth-specific communication training or education regarding cultural and community knowledge.
Conclusion
Our study identified that Aboriginal and Torres Strait Islander people perceived culturally safe telehealth to include appropriate communication and consultation skills, the building of relationships between doctor and patient and local knowledge (including both cultural and community knowledge).
Future studies exploring whether these findings translate to the urban setting and to a wider population would be of value. More studies focused on cultural safety in other forms of telehealth would be valuable (eg, videoconferencing, asynchronous options).
Implementation of these findings into clinical guidelines and/or telehealth training would be a valuable addition to encourage the cultural safety of telehealth consultations and assist clinicians’ understanding of the benefits and challenges of telehealth for their patients.
Data availability statement
Data are available upon reasonable request. The datasets analysed during the current study are not publicly available due to participants’ potential identifiability because of the small dataset. Data are available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study received ethical approval through the James Cook University Human Research Ethics Committee (H8296). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors wish to acknowledge the work of Dr Sumudu Wickramasinghe who assisted in data analysis for this project.
Footnotes
Contributors HW and KB designed the study with advice and input from all authors. HW was responsible for data collection, analysis and development of the manuscript. KB, RE, LM, TSG and RW were involved in interpreting the data and reviewing the developed manuscript. HW is the guarantor.
Funding The authors wish to thank the Australian College of Rural and Remote Medicine for funding this research through an Education Research Grant.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, conduct, reporting or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.