Article Text

Abstract
Objectives To evaluate the associations between alpha-lipoic acid (ALA) intake and intermediate disease markers in overweight or obese adults.
Design Systematic review and meta-analysis.
Data sources PubMed, EMBASE, Medline, APA PsycINFO, SocINDEX, CINAHL, SSRN, SocArXiv, PsyArXiv, medRxiv, and Google Scholar (from inception to October 2024).
Eligibility criteria This study included English-language randomised controlled trials (RCTs) on adults (body mass index ≥25 kg/m²) to assess the impact of ALA on intermediate disease markers. Studies lacking outcome data, duplicates or inaccessible full texts were excluded.
Data extraction and synthesis Paired reviewers independently extracted the data. We used frequentist meta-analysis to summarise the evidence, employing the DerSimonian and Laird estimator to account for heterogeneity across study designs, settings and measurement methods. Heterogeneity was assessed via the I² statistic with CIs and τ² values. The risk of bias was independently assessed by two reviewers according to the Cochrane Handbook, covering domains such as randomisation, blinding and data completeness. Publication bias was assessed using Begg’s test, while funnel plots and Egger’s test were applied to outcomes with 10 or more studies.
Results This meta-analysis included 11 RCTs from an initial screening of 431 studies, encompassing a total of 704 adults. The meta-analysis results revealed no significant associations were detected between ALA supplementation and changes in intermediate disease markers, including triglyceride (TG) (standardised mean difference (SMD): −0.08, 95% CI: −0.24 to 0.09, p=0.36, I²=0.00%, τ²=0.00), total cholesterol (TC) (SMD: 0.08, 95% CI: −0.55 to 0.71, p=0.80, I²=87.50%, τ²=0.52), high-density lipoprotein cholesterol (HDL-C) (SMD: −0.05, 95% CI: −0.22 to 0.11, p=0.52, I²=0.00%, τ²=0.00), low-density lipoprotein cholesterol (LDL-C) (SMD: −0.13, 95% CI: −0.40 to 0.15, p=0.37, I²=0.00%, τ²=0.00), homeostasis model assessment of insulin resistance (HOMA-IR) (SMD: −0.23, 95% CI: −0.60 to 0.15, p=0.23, I²=26.20%, τ²=0.05) and fasting blood glucose (FBS) (SMD: 0.13, 95% CI: −0.16 to 0.41, p=0.39, I²=29.40%, τ²=0.04). According to the Grading of Recommendations Assessment, Development and Evaluation bias assessment approach, eight studies were rated as having low bias (grade A), and three studies were rated as having moderate bias (grade B). Begg’s test indicated no evidence of publication bias.
Conclusions No significant associations were detected between ALA intake and intermediate disease markers, including TG, TC, HDL-C, LDL-C, HOMA-IR and FBS levels, in overweight or obese adults. Further research is needed to explore the potential associations of ALA, especially in high-risk populations with metabolic disorders, by employing longer intervention durations, higher dosages and optimised formulations.
PROSPERO registration number CRD42023450239.
- Obesity
- Meta-Analysis
- Other metabolic, e.g. iron, porphyria
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Further details can be obtained from the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study focused on overweight or obese adults, assessing the relationship between alpha-lipoic acid supplementation and intermediate disease markers.
The study used a rigorous, multidatabase search strategy to encompass all relevant studies.
Study design heterogeneity affects comparability of findings.
Introduction
The global prevalence of overweight and obesity has become a major public health concern. In 2022, approximately 2.5 billion adults worldwide were classified as overweight, with over 890 million adults being obese, accounting for 43% of adults being overweight and 16% being obese.1 With changes in lifestyle and dietary habits, projections suggest that by 2025, the global obesity rate will rise to 18% in men and over 21% in women.2 Obesity has a detrimental effect on almost all physiological functions of the body, increasing the risk of developing various chronic diseases such as diabetes,3 cardiovascular diseases,3 4 multiple cancers,5 musculoskeletal disorders6 and poor mental health.7 These conditions significantly affect quality of life, work productivity and healthcare costs.
There are various interventions available for managing overweight and obesity, which are typically divided into behavioural lifestyle interventions, pharmacotherapies and bariatric surgery.8–10 While lifestyle interventions can effectively control weight, long-term adherence remains challenging.8 The benefits of pharmacotherapies are somewhat constrained by their limited efficacy and potential side effects.9 Bariatric surgery, although effective, is expensive and not easily accessible.10 Therefore, there is an urgent need for interventions that are more accessible, have fewer side effects and are sustainable. Alpha-lipoic acid (ALA), a potent antioxidant,11–13 has garnered significant interest because of its potential to regulate body weight,14 improve endothelial function,15 16 and enhance glucose and lipid metabolism.17
Recently, several meta-analyses have reported the associations of ALA supplementation with selected health outcomes. For example, Akbari et al 18 explored the associations of ALA with lipid profiles, particularly in patients with metabolic diseases and reported reductions in total cholesterol (TC) and triglyceride (TG) levels. Rahimlou et al 19 investigated the associations between ALA and glycaemic markers and reported significant reductions in fasting blood glucose (FBS) and homeostasis model assessment of insulin resistance (HOMA-IR). Similarly, Kucukgoncu et al 20–22 highlighted the association of ALA with obesity treatment and weight loss. However, these reviews focused mainly on patients with specific metabolic conditions, such as diabetes or metabolic syndrome, and the results varied among different outcomes.
The latest research suggests that obesity should not merely be regarded as a condition of excessive weight but rather be recognised as a chronic disease.23 Therefore, the use of simple measures such as body weight and body mass index (BMI) has significant limitations in the assessment of ALA intake in this population and cannot effectively reflect individual health risks. Given the strong association between obesity and chronic diseases, intermediate disease markers can effectively reflect the biological indicators of individual health status, disease risk or disease progression and are used to evaluate the likelihood or severity of chronic diseases.24 25 This approach is expected to provide a more comprehensive assessment of health risks in overweight or obese adults following the use of ALA.
High-density lipoprotein cholesterol (HDL-C) and low-density lipoprotein cholesterol (LDL-C) are cornerstone biomarkers for cardiometabolic risk assessment, endorsed by guidelines26 27as key predictors of atherosclerotic cardiovascular disease (ASCVD): elevated levels of LDL-C directly promote atherogenesis and are an independent risk factor for ASCVD.28 29 Meanwhile, low levels of HDL-C correlate with insulin resistance, metabolic syndrome and are associated with an increased risk of cardiovascular disease.30 Dyslipidaemia is a hallmark of metabolic syndrome in overweight/obese individuals and is strongly linked to intermediate conditions like type 2 diabetes.31 Changes in these markers thus reflect ALA’s modulation of lipid metabolism and its potential impact on long-term clinical outcomes.
Moreover, there is currently a dearth of comprehensive analyses on the associations between ALA and intermediate disease markers such as TG, TC, HDL-C, LDL-C, HOMA-IR and FBS in overweight or obese individuals who are otherwise healthy. The existing gap in the literature underscores the necessity for a comprehensive meta-analysis that examines the associations between ALA and these markers within a broader population.
Through incorporating updated and more comprehensive evidence from randomised controlled trials (RCTs), the objective of this study was to perform a systematic review and meta-analysis to assess the associations of ALA with these intermediate disease markers in overweight or obese adults. The present study contributes to the literature by expanding its focus to a distinct population, specifically targeting otherwise healthy adults who are overweight or obese, and by encompassing a wider range of intermediate disease markers.
Methods
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting guidance.32 The registration of this systematic review was prospectively recorded in August 2023 in the PROSPERO database (https://www.crd.york.ac.uk/) (review register: CRD42023450239).
Search methods for the identification of studies
PubMed, EMBASE, Medline, APA PsycINFO, SocINDEX, CINAHL, SSRN, SocArXiv, PsyArXiv and medRxiv were searched from inception to October 2024 via a comprehensive strategy developed with an information scientist. We thoroughly examined the initial 30 results on Google Scholar. This strategy was informed by its ranking algorithm to identify the most relevant literature, despite broad indexing criteria that often yield less pertinent outcomes. We meticulously reviewed reference lists of included studies and relevant systematic reviews and proactively consulted subject matter experts to identify any additional, planned, ongoing or unpublished research, ensuring a thorough and targeted review process. Filters for study types and geographical locations were not applied. Details of these literature search strategies are reported in the online supplemental file.
Supplemental material
Study inclusion and exclusion criteria
Our population of interest was overweight or obese adults, defined as those aged ≥18 years with a BMI ≥25 kg/m² for overweight and ≥30 kg/m² for obesity, according to the WHO definitions.1 RCTs that used ALA as an intervention and published in English were included. Those who could not extract effective outcome data from the text, repeated published studies and studies without access to the full text were excluded.
Whether comorbidity is involved or not is not regarded as a restrictive condition.
The comparator group included individuals with no intervention or placebo intervention.
Eligible outcomes were intermediate disease markers such as TC, TG, HDL-C, LDL-C, HOMA-IR and FBS.
Adverse reactions were considered as a primary outcome in the inclusion criteria. However, only three studies reported data on adverse reactions, limiting our ability to comprehensively assess this outcome.
The studies reporting quantitative data from primary research were considered eligible by us.
Selection of studies
The records were deduplicated via Endnote V.X9 and then imported into Covidence for screening. The eligibility criteria were piloted on 100 studies, and all titles, abstracts and full texts were independently screened by YL and a second reviewer (JZ). Conflicts were resolved through consensus or discussion with a third reviewer (HG). In eligible studies that contained overlapping or duplicate data, a set of decision rules was used to select unique data for synthesis on the basis of alignment with our population, exposure, comparator and outcome criteria (see online supplemental file).
Data extraction and risk of bias assessment
Data were extracted via YL in Microsoft Excel (Microsoft Excel in version 2020) and checked by a second reviewer (JZ). In addition to the primary outcomes (TC, TG, HDL-C, LDL-C, HOMA-IR and FBS), we also extracted data on adverse reactions reported in the included studies to assess the safety profile of ALA. We further collected information on author and publication year, study country, participant characteristics, age, sample size, intervention and control measures. The risk of bias assessment was independently conducted by YL and a second reviewer (JZ) using the Cochrane Handbook 5.0, covering six domains: random allocation method, allocation concealment, blinding method, integrity of result data, selective reporting and other sources of bias. All RCTs were assessed for low, high or unclear risk of bias, and conflicts were resolved via consensus or discussion with a third reviewer (HG).
Our risk of bias assessments guided the synthesis of data and informed the certainty of evidence, which was evaluated via Grading of Recommendations Assessment, Development and Evaluation.33 The studies were classified into three levels: grade A (low bias, meeting four low-risk criteria), grade B (moderate bias, meeting 2–3 low-risk criteria) and grade C (high bias, with one high-risk criterion or meeting only one low-risk criterion).
Data synthesis
We conducted meta-analyses for each outcome, including TC, TG, HDL-C, LDL-C, HOMA-IR and FBS. We used frequentist meta-analysis to summarise the evidence. Given the expected heterogeneity in study designs, settings and measurement methods, we used random effects models employing the DerSimonian and Laird estimator. The I² statistic, along with its CI, was used to assess the proportion of total heterogeneity attributable to between-study variability, whereas τ² provided an estimate of the absolute between-study variance in effect sizes. As all outcome variables were continuous, we pooled the data to generate standardised mean difference (SMD) as effect size estimates without converting these continuous data into binary forms, in line with the Cochrane Handbook’s guidance for continuous variables. To visually display and summarise the results of individual studies and syntheses, forest plots were used to illustrate the effect sizes and CIs for each study. Additionally, summary tables were used to present detailed study characteristics and outcome data in a structured format. At the same time, we conducted subgroup analysis of the characteristics of different obese populations, ALA administration mode, dosage and duration to further evaluate heterogeneity. For studies that reported only standard errors, we followed the Cochrane Handbook’s recommendation to convert standard errors to SDs (SD=SE×√n, where n is the sample size). All the statistical analyses were performed via Stata V.15.0.
Publication bias was evaluated via Begg’s test, with funnel plots and Egger’s test additionally applied for outcomes with 10 or more studies.
Patient and public involvement
This study is a systematic review protocol, which means that individual patient data was not included. A thorough search of the literature will be conducted via specified databases. As a result, there will be no engagement of patients in the planning or application process of the study or during the analysis or dissemination of the findings.
Results
Search results
From a total of 431 references identified in our literature search,34 studies were initially selected for potential inclusion. Of these, 31 studies were excluded on the basis of predefined criteria (see figure 1 for reasons for exclusion). Ultimately, 11 parallel-design RCTs were included for qualitative analysis. The PRISMA flow chart in figure 1 provides an overview of the literature selection process. The included studies14 35–44 included patients with a mean age range of 36–58 years, intervention durations ranging from 2 weeks to 6 months, and ALA doses varying from 300 mg/day to 1800 mg/day.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram.
Studies and patient characteristics
Data from 704 patients across 11 RCTs were included, with most participants being overweight or obese without comorbidities. Some studies also included participants with specific medical conditions, such as hypertension, diabetes, hypercholesterolaemia and non-alcoholic fatty liver disease. The administered doses of ALA varied, with five studies using doses ≥1200 mg/day and seven studies employing intervention durations longer than 8 weeks. The majority of trials used oral administration, with one trial involving intravenous injection. Additionally, dietary control was implemented in both the intervention and control groups in several studies. Further details on the characteristics of the trials are summarised in online supplemental table S1.
Supplemental material
Risk of bias within studies
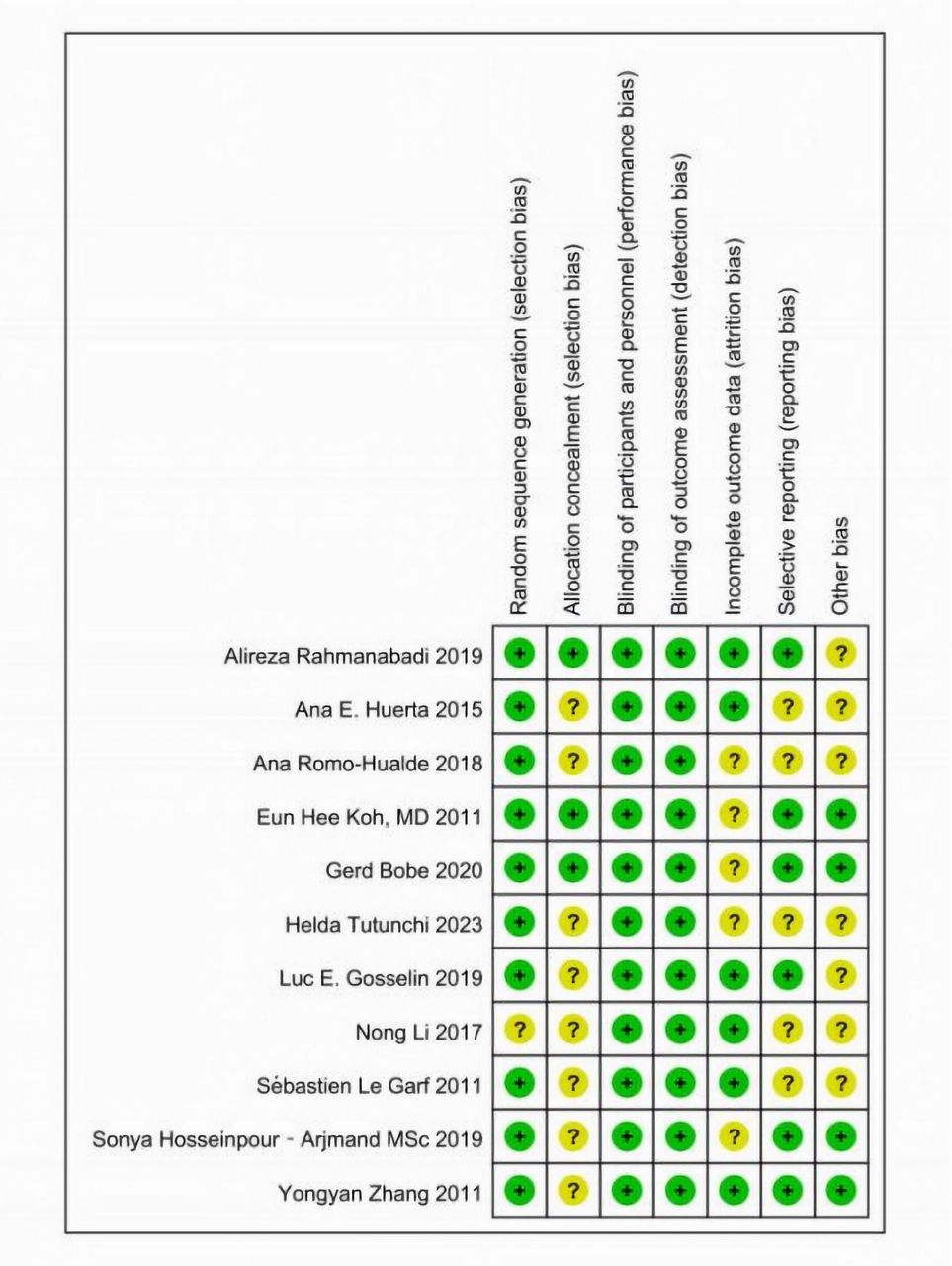
We evaluated the risk of bias across multiple domains and observed a low risk in the majority of areas. Specifically, all studies demonstrated low risk in terms of participant and personnel blinding, as well as outcome assessment blinding. In total, eight studies were classified as having an ‘A’ rating (low risk of bias), whereas three studies received a ‘B’ rating (moderate risk of bias). The detailed results of the risk of bias assessment are presented in figures 2 and 3.

Risk of bias assessment for different domains across included studies.

{kind=link}
{kind=link}
{kind=link}
Risk of bias evaluation for individual studies across various domains. Notes: low risk (green ‘+’); unclear risk (yellow ‘?’).
Meta-analysis results
The meta-analysis results indicated that ALA supplementation was not significantly associated with changes in intermediate disease markers, including TG, TC, HDL-C, LDL-C, HOMA-IR or FBS (online supplemental figures S1–S6).
The SMDs reported in our meta-analysis were interpreted based on Cohen’s conventional thresholds for effect sizes, where SMD magnitudes of 0.2, 0.5 and 0.8 represent small, medium and large effects, respectively. The direction of the SMD (positive or negative) indicates whether ALA supplementation was associated with an increase or decrease in the biomarker compared with the control group.
For TG, the negligible effect size and CI crossing zero suggest that ALA supplementation has no clinically meaningful impact on TG levels in overweight or obese adults. The negative direction implies a non-significant trend towards slight reduction. In contrast, TC exhibited a near-zero overall effect but with substantial heterogeneity, indicating inconsistent results across studies. The positive directionality here is unreliable due to the wide CI and high variability between trials. For HDL-C, LDL-C, HOMA-IR, and FBS, all effect sizes fell within the ‘small’ range (|SMD|<0.5). The negative SMDs for LDL-C and HOMA-IR suggest a marginal tendency towards improvement (reduction in LDL-C or insulin resistance), whereas the positive SMD for FBS indicates a trivial increase in fasting glucose. However, none of these associations reached statistical significance (p>0.05), and CIs overlapped zero, precluding definitive conclusions.
The low heterogeneity (I²≤29.40%) for TG, HDL-C, LDL-C, HOMA-IR and FBS supports the consistency of these null findings across studies. In contrast, the high heterogeneity observed for TC highlights potential variations in study populations, interventions or measurement methods, necessitating cautious interpretation.
Further details of the meta-analysis results are summarised in table 1.
Summary of the meta-analysis results
Only three studies included in this meta-analysis reported adverse reactions: one study42 documented a female subject experiencing severe urticaria, whereas another study37 noted that six subjects (four in the intervention groups and two in the control groups) withdrew from the trial because of heartburn, headache or low back pain. The additional adverse events observed were nausea, gastric disorders and pruritus.
Publication bias
The meta-analysis included fewer than 10 articles for each indicator, thus precluding the conduct of publication bias analysis. Nevertheless, we performed Begg’s test and found no evidence of publication bias in our analysis (online supplemental figures S7–S12).
Subgroup analysis
We performed subgroup analyses of low dose (<1200 mg) vs high dose (≥1200 mg) and short intervention (<12 weeks) vs long intervention (≥12 weeks), respectively. The subgroup analysis indicates that the effects of ALA supplementation on the six intermediate disease markers (TC, HDL, LDL, FBS, HOMA_IR, TG) in overweight or obese adults do not show significant differences between long-term and short-term interventions (online supplemental figures S13–S18). Most of the SMDs are close to zero, and the CIs include zero, suggesting no significant effect. The heterogeneity varies across different markers, with some showing low heterogeneity and others showing high heterogeneity. Overall, the results suggest that ALA supplementation may not have a significant impact on these intermediate disease markers, regardless of the duration of intervention.
The subgroup analysis of low and high doses of ALA on intermediate disease markers reveals the following: high-dose ALA may have a slight effect on reducing TC, but the results are highly heterogeneous (online supplemental figures S19). Neither low nor high doses of ALA show a significant impact on HDL, LDL, TG and HOMA_IR (online supplemental figures S20–S23). High-dose ALA might slightly increase FBS, but the effect is not significant and has low heterogeneity (online supplemental figure S24). Overall, the effects of ALA on these intermediate disease markers are inconsistent across different doses, and some results exhibit high heterogeneity.
The subgroup analyses of ALA alone versus ALA combined with other components indicated that there are no significant differences in the effects of ALA on the five intermediate disease markers (TC, HDL, LDL, FBS, HOMA_IR) between the ALA alone and ALA combined with other therapies subgroups (online supplemental figures S25–S29). The CIs for each marker overlap between the two subgroups, and the overall SMDs are not statistically significant. This suggests that the combination of ALA with other therapies does not significantly alter its impact on these intermediate disease markers in overweight or obese adults. Besides, ALA administered alone does not significantly impact TG levels. However, when ALA is combined with other components, it demonstrates a small yet significant positive effect on reducing TG levels (online supplemental figure S30). While the overall effect of ALA, whether administered alone or in combination, on TG levels is not statistically significant, the subgroup analysis indicates that combining ALA with other treatments may offer a modest benefit.
The subgroup analyses of overweight or obese versus obese showed that there are significant differences in the effects of ALA supplementation on TC and FBS between the overweight or obese and obese groups (online supplemental figures S31 and S32). In the overweight or obese group, ALA supplementation is associated with a slight reduction in TC and FBS. While in the obese group, it is associated with a slight increase in TC and FBS. Although the overall effect of ALA on TG levels across all studies is nonsignificant, the subgroup analysis indicates that ALA may be more effective in obese individuals compared with those who are overweight or obese (online supplemental figure S33). For HDL, LDL and HOMA-IR, there are no significant differences between the two groups (online supplemental figures S34–S36).
Discussion
The present systematic review and meta-analysis aimed to assess the associations between ALA and intermediate disease markers in overweight or obese adults. Despite the well-documented antioxidant and metabolic regulatory properties of ALA, our findings did not reveal any statistically significant associations with markers such as TG, TC, HDL-C, LDL-C, FBS and HOMA-IR. These results call for further investigation into the underlying reasons why ALA fail to yield the anticipated outcomes in this particular population.
Our findings suggest that the relationships between ALA and intermediate disease markers may be highly dependent on specific contextual factors, particularly the baseline metabolic status of the individuals involved. While studies conducted in individuals with metabolic disorders have reported improvements in lipid profiles and glycaemic control,5 45 our analysis did not yield significant results, indicating that the benefits of ALA might only be substantial in populations with pronounced metabolic dysfunction. For example, Pashaj et al 46 emphasised that the lipid-lowering effects of ALA were most noticeable in individuals with elevated TG levels, as the presence of metabolic abnormalities such as hypertriglyceridaemia likely enhances oxidative stress and inflammation, both of which are targets of ALA.47 In the absence of such conditions, which were predominantly observed among participants in our included studies, ALA may not have sufficient pathological targets to exert measurable effects.
In addition to the minimal adverse reactions identified in our analysis, other safety concerns emphasised in prior studies are crucial. A systematic review and meta-analysis by Fogacci et al revealed that ALA supplementation was generally safe across various populations.48 While rare adverse events have been reported in association with ALA supplementation, further research is needed to determine whether these sporadic events are related to the production quality of ALA supplements, other components within mixed supplements, or concomitant treatments or diseases. These findings suggest the importance of considering individual risk factors and supplement quality when recommending ALA.
The inconsistency between our findings and those of previous meta-analyses5 34 can be partially attributed to variances in the study populations. For example, a study conducted by Haghighatdoost and Hariri5 revealed that ALA had a significant effect on reducing TC and LDL-C levels in patients with metabolic diseases. In contrast, our study focused primarily on overweight or obese individuals without a diagnosis of metabolic conditions. It is plausible that the metabolic pathways modulated by ALA, such as those involving lipid metabolism and insulin sensitivity, may be sufficiently disrupted only in individuals with metabolic disorders such as diabetes or metabolic syndrome, thereby allowing for measurable improvements on ALA intervention.45
Additionally, studies such as those conducted by Sun49 have demonstrated that ALA significantly enhances lipid profiles and insulin sensitivity in animal models of insulin resistance. However, it is increasingly acknowledged that findings from preclinical models do not always directly translate into human populations owing to physiological differences, particularly in terms of metabolic flexibility and lipid metabolism.50 The discrepancy between animal studies and human trials may also be due to variations in intervention duration and dose, which will be further discussed.
From a mechanistic perspective, ALA has been demonstrated to activate AMP-activated protein kinase (AMPK), a key regulator of energy balance that enhances fatty acid oxidation and inhibits lipogenesis.16 The activation of AMPK is particularly relevant in the context of metabolic disorders characterised by insulin resistance and dysregulated lipid metabolism.14 However, in metabolically healthy but overweight individuals, dysregulation of the AMPK pathway may not be sufficient to fully harness the therapeutic effects of ALA. The absence of significant associations observed in our study might suggest that the impact of ALA on these pathways requires a greater degree of baseline metabolic impairment, as observed in individuals with type 2 diabetes or severe dyslipidaemia.
Moreover, oxidative stress and chronic inflammation play crucial roles in driving the progression of metabolic diseases.16 The potent antioxidant properties of ALA, which include scavenging reactive oxygen species and regenerating other antioxidants such as vitamin C and glutathione, have been shown to mitigate oxidative damage in metabolically compromised patients.13 However, in a population with relatively normal metabolic function, the role of oxidative stress may be less pronounced, potentially explaining the limited observed associations between ALA and markers such as HOMA-IR and FBS.
Although our results did not demonstrate significant associations between ALA and intermediate disease markers, these findings do not necessarily undermine the potential of ALA as therapeutic agents. Instead, they emphasise the importance of targeted intervention. The benefits of ALA are likely more pronounced in individuals with higher baseline metabolic risk, such as those with elevated oxidative stress, insulin resistance or dyslipidaemia. Future clinical trials should focus on populations with metabolic syndrome or diabetes, where the effects of ALA might be more easily detected owing to greater baseline dysfunction.
The dosage and duration of ALA supplementation varied significantly across the included studies, with doses ranging from 300 to 1800 mg/day and intervention periods spanning from 8 to 24 weeks. Previous research has indicated that achieving significant clinical outcomes may require higher doses of ALA and longer intervention durations.51 Future studies should thoroughly investigate dose-response relationships and explore the potential for longer-term interventions to yield more substantial effects, particularly in terms of reducing lipid levels and improving insulin sensitivity.
Moreover, the majority of studies included in our analysis used racemic mixtures of ALA, which include both R-form and S-form of the molecule. The R-form is more biologically active and may have greater therapeutic potential.51 Future trials should consider the use of pure R-ALA to assess whether this more potent form yields different results, particularly in improving metabolic markers.
Additionally, it is important to explore the synergistic effects of ALA in conjunction with other interventions, such as exercise or dietary modifications. Research has demonstrated that lifestyle interventions significantly enhance metabolic outcomes, and it is possible that ALA supplementation could have additive or synergistic effects when combined with these approaches.15
The scope of future research should encompass an exploration into the potential correlation between ALA and inflammatory as well as oxidative stress markers, thereby yielding further insights into its broader metabolic advantages. By comprehending the associations between ALA and these pathways, it becomes possible to identify the subpopulations that are most likely to benefit from its supplementation while also elucidating the contexts in which it exerts its strongest effects.
There are several limitations associated with our study. First, we did not employ advanced statistical methods, such as one-stage dose-response modelling, Galbraith plots or the Hartung-Knapp adjustment, due to limitations in data structure and study design.15 We relied on established traditional meta-analytical methods widely accepted for their reliability. In future research, we may consider adopting these advanced techniques to further improve analytical precision. Additionally, our analysis was limited to English-language publications, which may introduce language bias and restrict inclusivity regarding studies published in other languages. To address this, we conducted thorough searches across multiple major databases to maximise the comprehensiveness of relevant English-language studies. Meanwhile, the time difference between the current date and the literature search may affect the analysis’s timeliness and comprehensiveness. Readers should consider this potential impact when interpreting our results. To maintain the study’s timeliness, we suggest regularly updating the literature search in future research to include the latest evidence. Finally, our study included participants with other existing comorbidities based on the main body of healthy adults who were overweight or obese. We recognise that overweight or obese adults may often have concomitant other health problems that may affect the efficacy of ALA. It is, therefore, hoped that these studies will provide additional insight into the potential impact of ALA on a wider population, although this may increase the interstudy heterogeneity.
Conclusions
In this meta-analysis, supplementation with ALA was not significantly associated with intermediate disease markers, including TG, TC, HDL-C, LDL-C, HOMA-IR or FBS levels, in overweight or obese adults. These findings suggest that the relationships between ALA and intermediate disease markers may be limited within this population lacking underlying metabolic disorders. However, further research is warranted to explore the potential benefits of ALA in individuals exhibiting more pronounced metabolic dysfunction, such as those with metabolic syndrome or diabetes. Future studies should consider longer intervention periods, higher dosages and the use of pure R-ALA to explore its therapeutic potential more comprehensively. Moreover, these trials should target high-risk populations for a more comprehensive assessment of the role of ALA in managing metabolic health.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Further details can be obtained from the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
Our study is a meta-analysis, which synthesizes and analyses data from previously published studies. As we did not collect any new data from human participants or conduct any original experiments, no ethical approval was required for this type of research. All the data included in the meta-analysis are derived from studies that have already obtained ethical approval, as stated in their original publications.
Acknowledgments
We would like to sincerely acknowledge our engagement (PPIE) group for their valuable input throughout the development and review stages of this study.
References
Footnotes
YL and JZ contributed equally.
Contributors YL: conceptualisation, methodology, literature search, full-text reading, data extraction, quality assessment, data analysis, writing-review and editing. JZ: literature search, full-text reading, data extraction, quality assessment, data analysis,writing-review and editing. HG: project administration, validation, supervision and is the guarantor of this work, taking full responsibility for the integrity and accuracy of the research. I used AI technology to assist with formatting adjustments and translation in the submission. The AI was used solely for improving the document’s layout, ensuring consistency with submission requirements and translating content where necessary. No content generation or substantive edits were conducted by the AI.
Funding This work was supported by the West China Nursing Discipline Development Special Fund Project, Sichuan University (grant number HXHL21003) and project of Technology and Training of Sichuan Province under grant number 2021JDKP0043.
Competing interests None declared.
Patient and public involvement None.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.