Article Text

Abstract
Introduction Identifying individuals at risk of suicide remains an ongoing challenge. Previous research investigating risk factors for suicidal thoughts and behaviours (STB) has been informative for assessing suicide risk. However, the complex biological, psychological and sociocultural factors underlying STB have not been comprehensively captured to date, which has limited our understanding of how these factors interact to influence STB. Moreover, acute care settings, such as emergency departments (EDs), are often first points of contact for individuals with STB, highlighting a need for more research in these settings.
Methods and analysis We aim to (1) characterize a cohort seeking care for STB and their clinical trajectories; (2) situate the cohort by comparing its characteristics and outcomes to other groups seeking emergency care; (3) explore their experiences of seeking care; and (4) examine blood-based biomarkers modulating risk for STB. Using a multimethod, prospective cohort design, we will follow up to 500 people aged 16 or older presenting to the ED with STB at a psychiatric hospital over 1 year. Analyses will involve descriptive statistics and latent profile analysis to characterize the cohort, hypothesis tests and regression models to situate the cohort, qualitative analysis based on a realist research framework to understand experiences, and within-participant comparisons of proteins, mRNA and epigenetic DNA modifications to examine biomarkers of contrasting states of STB.
Ethics and dissemination This study was approved by the hospital’s Research Ethics Board with safeguards in place to ensure the well-being of participants and research team. An integrated knowledge translation approach will be used for dissemination, wherein patient and family advisors are engaged throughout each study phase. Findings will enhance our understanding of the multifactorial nature of suicide risk, inform strategies for prevention and provide important insights into characteristics, experiences and outcomes of individuals with STB, who are under-represented in mental health research.
- Suicide & self-harm
- Emergency Departments
- Emergency Service, Hospital
- PSYCHIATRY
- MENTAL HEALTH
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study adopts an integrated approach (i.e., biological, clinical, psychological, sociodemographic and qualitative) to study suicidal thoughts and behaviours in an emergency department (ED) setting.
Its design assesses cohort representativeness in relation to other individuals seeking care within the ED, hospital, and province.
We adopt a patient-centred approach by focusing on participant perspectives and including patient advisors as full and equal members of the study team.
The longitudinal design may result in participants lost to follow-up and associated data loss, leading to difficulties in achieving the target sample size.
The study setting is limited to an urban psychiatric hospital in a high-income country, lending the possibility that results are of limited applicability to other settings.
Introduction
Suicide is a significant public health problem and has been the focus of increasing attention in research and public awareness campaigns.1 Each year, about 703, 000 people die by suicide worldwide, the equivalent of one death every 40 seconds.2 According to the World Health Organization, the countries with the highest suicide mortality rates are low-income countries. The rates, however, are generally lower in low-income countries compared with high-income countries.3 4 In Canada, approximately 4500 people die by suicide every year, equating to about 12 people dying by suicide every day. These numbers are likely an underestimate, given hesitancy to report, due to stigma and other factors.5 Suicide has devastating consequences, contributing not only to the premature death of individuals but also to long-lasting, negative impacts on families, loved ones, and communities. For every death by suicide, up to 135 people are estimated to be exposed,6 with at least 6 individuals predicted to be most directly affected.7 Unfortunately, determining who is at risk of dying from suicide is not straightforward, due to its low base rate, which presents a challenge for suicide prevention. Risk for suicidal behaviour (SB) is also multifactorial and linked to a complex array of psychological, clinical and sociocultural factors.
A meta-analysis of studies from multiple countries found that people who have serious mental illnesses are at high risk for suicide, with major depressive disorder being attributed to the highest pooled suicide rate.8 Another meta-analysis reported that individuals with a mental illness—particularly psychotic, mood and personality disorders—had a nearly eightfold heightened suicide risk compared with those without a mental illness.9 Authors of a meta-review analysing 20 systematic reviews and meta-analyses observed that depression, bipolar disorder, borderline personality disorder, anorexia nervosa, and schizophrenia diagnoses resulted in the highest risk for suicide mortality compared with the general population. This review also reported greater suicide mortality rates for opioid and alcohol use in females.10 Other meta-analyses have identified strong associations between substance use disorders and suicidal ideation (SI), attempts, and death.11 12
Furthermore, findings from studies following large samples for periods ranging from 1 month to several years have found that sociocultural factors, such as disability,13 lack of social support,14–16 male sex,17–19 single, separated, divorced, or widowed marital status,15 20 21 loneliness or social isolation,15 22 23 not living with a close relative,24 childhood adversity,25 financial stress and unemployment,26 low socioeconomic position22 27 alienation,15 and racism28 29 also increase suicidal risk. Some reports have pointed to the cumulative and interactive effects of more than one factor for SB. For instance, although male sex and marital status represent individual risk factors for suicide, the risk is exacerbated when combined, as men who have never been married, widowed or divorced are found to have higher suicide risk compared with women with equivalent marital statuses.20 21
Studies have identified subgroups of individuals at risk for suicide, by clustering their sociodemographic, clinical and psychological characteristics.30 One common subgroup is defined by severe symptoms, multiple prior hospitalizations, childhood trauma and emotional instability.30 Several studies report at least one subgroup composed of individuals with mild symptoms, no mental illnesses,30–33 or no prior treatment, who are more likely to be men.34 Another subgroup, denoted as ‘depressive’, comprises high hopelessness, lack of social support, relationship difficulties, unemployment and comorbid alcohol use.30 34 35 Other common subgroups are defined by externalising conditions, including personality disorders, antisocial behaviours and substance use,30 and by internalising conditions, including anxiety, avoidance, rumination, social withdrawal, and low cognitive ability.30 32 These studies altogether highlight the heterogeneous nature of suicide risk.
Genetics and epigenetics also play a major role in suicide risk; both twin and family studies have found suicide tends to cluster within families36 and the genetic heritability of suicide is estimated to be 43%.37 Several biological markers have been associated with suicide, including those involved with the serotonin (5-HT) neurotransmitter system and the hypothalamic-pituitary-adrenal axis.38–45 More recently, epigenetic studies have indicated that environmental stress can alter gene transcription regulation in people at risk for SB within GABAergic and dopaminergic pathways.46 47 Also, members of our team previously identified two protein interactions (elevated GR-FKBP51 complex levels in people with psychological trauma and increased D1-D2 receptor complex levels in depression),48–50 which are a focus for further study, provided growing literature regarding these associations.46 51–54
Death by suicide can be categorised under the construct of self-injurious thoughts and behaviours (SITB).55 However, despite multiple attempts to develop a taxonomy with respect to SITB,56–59 there remains a lack of consensus on nomenclature.60 61 Table 1 outlines the taxonomy that will be used for the purposes of the current study. According to this taxonomy, SITB includes suicidal ideation (SI), SB, and non-suicidal self-injury (NSSI).59 SI, also known as suicidal thoughts, encapsulates a range of wishes, contemplations, and preoccupations with suicide.60 SB refers to suicide attempts, interrupted attempts, aborted attempts, and preparatory acts with at least some intent to die, or self-injury of undetermined intent. SB is among the strongest known predictors of death by suicide,59 62 with attempts occurring at a rate up to 30 times higher than suicide death.63 Suicidal thoughts and behaviours (STB) are distressful and require prompt identification and intervention. STB are associated with high rates of mental health comorbidity and marginalization.64–68 The presence of STB has been associated with poorer access to high-quality mental healthcare and patient-perceived barriers to mental health.65 69
Terms and definitions related to self-injurious thoughts and behaviours (SITB)
Although prior research has greatly informed our understanding of STB, this research also has limitations. Studies investigating psychosocial determinants of suicide have predominantly used register data and surveys. Though these methodologies are informative, they often restrict researchers to examining a limited set of sociodemographic characteristics or STB-related factors. Some studies have also tended not to include gold standard approaches to capturing mental illness and STB (i.e., clinician-rated measures). Another issue is that prior suicide research has often captured participant data at a singular time-point or else have had minimal follow-up; unfortunately, these study designs may fail to capture participants’ experiences more broadly, as their STB may fluctuate over a prolonged period. Consequently, the multifactorial nature of STB has not yet been captured comprehensively within one study over time, limiting our ability to understand how various factors interact to impact the risk of death by suicide.
Moreover, most studies have not addressed the issue of selection bias. There is evidence that institutional mistrust, experiences of trauma and oppression within healthcare settings, and lack of attention towards systemic causes of STB may result in the undersampling of racial minorities.70 71 These patient groups may also be more reluctant to disclose SI or SB,72 resulting in less accurate rates of suicide. Clinical severity may be a source of bias as well. More severely distressed or acutely ill patients may be less likely to participate in research; therefore, outcomes for those who do participate may not be representative of all patients with STB.73 Finally, due to concerns regarding adverse events, individuals with STB are frequently excluded from research studies.74 This practice has restricted our understanding of their characteristics, trajectories and outcomes, as well as interventions that are likely to be helpful.
Understanding suicide risk in acute care settings: context, challenges and opportunities
Acute care settings, such as the emergency department (ED), are a frequent first point of contact for individuals with STB.75 According to a review of literature published in North America, the UK, and Australia, several demographic and clinical factors are associated with higher risk of ED presentations for STB.76 In Canada, females comprised 51% of all ED visits for STB, and individuals aged 15 to 24 were the most frequently seen out of all age groups, regardless of sex.77 Mental illnesses, primarily mood, anxiety, psychotic, personality, and substance use disorders represented risk factors in individuals presenting to the ED for STB.76–80 In another review, individuals who presented to the ED on more than three occasions died by suicide significantly sooner than those with fewer visits.78 Results from a multicentre cohort study from the UK indicated that NSSI presentations to the ED worsened suicide risk; attendees who presented more than once for self-harm, lived in areas of socioeconomic deprivation, and were older in age conferred greater risk of death by suicide.81–84
Among those admitted for psychiatric hospitalization after presenting to an ED, the period immediately following discharge from psychiatric hospitalization is characterized by extraordinarily high suicide risk, persisting for a year following discharge and beyond.85–87 According to a study that followed up after 21–32 years with individuals who attempted suicide, the risk for subsequent suicide attempts often persisted over several decades. However, the highest incidence of subsequent attempts occurred within a year following the initial attempt.87 In an analysis of Toronto-based deaths by suicide from 1998 to 2011, 66% of people had a mental health contact within the year prior to death, and of those with a mental health contact, 21% had a mental health hospitalization.88
Rather than an emphasis on prediction, new research suggests an approach to suicide prevention that focuses on all recently discharged patients, whether from an inpatient unit or the ED, and includes more intensive interventions (i.e., home visits and accompanied visits to outpatient appointments), which may be more promising.89 90 Overall, acute healthcare settings provide a unique opportunity to characterize and understand help-seeking individuals with SI and/or SB using a range of clinical, health service utilisation, qualitative and biological data. An ED visit represents a key time to initiate suicide prevention efforts, due to the number of individuals at risk for death by suicide presenting to ED care.73
However, suicide research in acute care has faced unique obstacles. Healthcare institutions in North America do not typically receive information on death by suicide or non-fatal SB occurring outside of their institution for patients they previously served, making it difficult to track outcomes. Intervention research in acute care settings has also struggled to disentangle the effects of specific components of suicide prevention interventions because evaluations have focused on the overall effect of the intervention. Interventions across studies also fluctuate significantly and can lead to varying outcomes in different populations and settings.91 92 Moreover, the development of trusting relationships with patients is central to suicide risk assessment and prevention, yet research on this is limited, especially in acute and high-intensity settings (e.g, EDs). Findings from qualitative research suggest that patient assessments need to focus not only on risk but also on the deep psychological pain driving suicide, treatment options, and ways to offer hope.93 Future research on a patient-centred approach in acute care settings is needed.
Given the widespread and devastating impacts of STB, including premature mortality, gaining a comprehensive and representative understanding of the characteristics of individuals with STB over time is of vital importance. Suicide prevention research that focuses exclusively on one form of data collection does not integrate knowledge in the way that is required to understand this complex problem. Suicide prevention research must: (a) develop a better understanding of outcomes and trajectories of care for those at risk for suicide, through individual-level and population-level investigations; (b) involve close engagement with patient, family and care providers to understand the lived experiences of those navigating the system and cocreate potential interventions as a next step; and (c) explore novel biological avenues for understanding suicide risk, and advance innovative interventions. Following this context, this paper describes the rationale, methods, and potential impact of a new cohort study that improves on limitations of prior work and incorporates key advances in suicide research.
Overview and objectives
The Centre for Addiction and Mental Health (CAMH) Suicide Prevention Cohort Study (CAMH-SPCS) is a novel, integrated cohort design that addresses four areas of inquiry: characteristics, trajectories, perspectives and outcomes of people experiencing STB who present to the ED at a psychiatric academic hospital in Toronto, Canada. This study aims to characterize and understand these individuals by using a range of clinical, health services, qualitative, and biological data. Our goal is to understand the longer-term trajectories of a well-defined cohort and provide crucial infrastructure to develop and test future interventions.
We conceptualise the study objectives through the following four integrated study projects:
Characterizing the cohort: we aim to characterize the clinical, psychological, and social characteristics of people presenting to emergency care with suicidality, and their clinical trajectories after seeking care. This work will provide a foundation for future studies and establish a novel, systematized approach for capturing data among individuals with STB.
Situating the cohort: we aim to describe the study cohort characteristics and outcomes in comparison to other groups who are not enrolled in the cohort (ie, other patients with STB presenting at CAMH, all CAMH ED patients, and those who present to other EDs in Ontario with and without SB). This study will allow us to thoroughly assess the generalizability of the CAMH-SPCS cohort.
Understanding lived experiences and perspectives: we aim to explore qualitatively the experiences of people who seek care for STB, proximal to the visit, and 1 year later. This study explores perspectives of participants on current standard of care practices in the ED to support the codesign of a suicide prevention intervention that can be piloted in the CAMH ED.
Explore novel biological markers: we aim to identify blood-based biomarkers that potentially modulate risk for SI and SB, by analysis of proteins, protein complexes, RNA transcripts and the epigenome, as well as future genetic analyses. This study will provide the basis for establishing molecular biomarkers to monitor STB in ED patients.
Methods and analysis
Reporting of our methods is informed by the Strengthening the Reporting of Observational Studies in Epidemiology checklist for observational studies.
Study design
Objective 1 (Characterizing the cohort). In a prospective cohort study design, we will recruit participants presenting with STB for services within CAMH’s ED (i.e., the CAMH-SPCS cohort) and follow them over 1 year.
Objective 2 (Situating the cohort). We will examine the representativeness of the CAMH-SPCS cohort in a cross-sectional design, by comparing its characteristics to four other cohorts during the 18-month study recruitment period. For three cohorts, we will employ a longitudinal design to examine associations between their characteristics and outcomes.
Objective 3 (Understanding experiences). To better understand experiences of patients with STB, we will use a qualitative design, completing two rounds of interviews with the same subset of 30 participants (at 4 and 12 months). Each participant can also suggest one family member or friend to complete a qualitative interview at 12 months.
Objective 4 (Exploring biomarkers). In a longitudinal design, we will explore molecular biological markers (i.e., proteins, protein complexes and changes in the RNA transcriptome and epigenome) modulating risk for STB, by collecting blood samples from cohort participants at baseline and 2 months later.
Setting
CAMH is an academic mental health and addictions hospital, located in downtown Toronto, Canada. The CAMH ED provides emergency psychiatric and substance use assessments and services 24 hours a day, 365 days a year, for individuals aged 16 and over and has over 14 500 visits per year. Admissions are often voluntary; patients can present by themselves or with referral from a healthcare provider. However, they can also be involuntary, such as when patients are apprehended by police for admission. Many patients present for services with STB, which is initially identified during triage. After their assessment in the ED, individuals with STB are either admitted to the hospital or discharged with a referral to resources, including outpatient follow-up for mental health and addictions.
Participants
Objective 1 (Characterizing the cohort). The CAMH-SPCS cohort will consist of 500 participants presenting with STB for services within CAMH’s ED, recruited over 4 years (December 2024–December 2028). Inclusion criteria for this cohort include age 16 years or older, STB documented at triage (i.e., those involving a self-reported wish to die and excluding NSSI), capacity to consent and stated willingness to comply with study procedures, and an available provincial health card number required for ICES linkage. Our study does not involve altered consent procedures or caregiver involvement for participants under 18 (i.e., the legal age of adulthood in the province), given that in Canada, there is no specific minimum age at which consent for research can be obtained. Individuals aged 16 or older can seek ED care independently at CAMH, suggesting a capacity to understand study procedures and provide informed consent. Patients admitted in any manner (e.g., on an involuntary basis or accompanied by police) are also eligible. However, patients requiring chemical or physical restraint in the past 8 hours, those unable to provide consent (i.e., due to intoxication, severe thought disorder, or aggression), or with an unsurmountable language barrier will not be eligible to participate. For patients who remain in the ED, eligibility will be reassessed each morning, with the option to participate if their status has changed. As part of our recruitment strategy, ED clinicians identify all individuals presenting with STB who may be safely approached, who are then provided with information about the study from dedicated research staff based in the ED.
Objective 2 (Situating the cohort). The CAMH-SPCS cohort will be compared against the following four cohorts:
All patients presenting for services in the CAMH ED for STB (excluding NSSI);
Patients presenting for any services in the CAMH ED (to capture individuals potentially unwilling to disclose STB);
All patients presenting for services for SB, with intent to die or undetermined intent, from any ED in the province of Ontario; and
All patients presenting for any mental health services in any ED in Ontario.
Inclusion criteria for these cohorts include service utilization during the 18-month study period and a valid provincial health card number. For CAMH ED patients with multiple visits, only data from the first visit will be analyzed. Exclusion criteria include enrolment in the CAMH-SPCS cohort.
Objective 3 (Understanding experiences). We will use a non-random, maximum variation qualitative purposive sampling approach to select participants from the CAMH-SPCS cohort for qualitative interviews using age, self-identified gender, ethnicity, diagnosis, and STB as categories of interest.94 During data collection, coding and analysis, we will use theoretical sampling to seek variation in perspectives based on emerging themes, with the aim of reaching saturation.
Objective 4 (Exploring biomarkers). All CAMH-SPCS cohort participants will be invited to provide blood samples. It is expected that about half will consent. A subset of 30 participants with the largest changes in STB between the baseline and follow-up (month 2) visit will be selected for biomarker analysis. Samples from the remaining participants will be stored for future analyses.
Variables
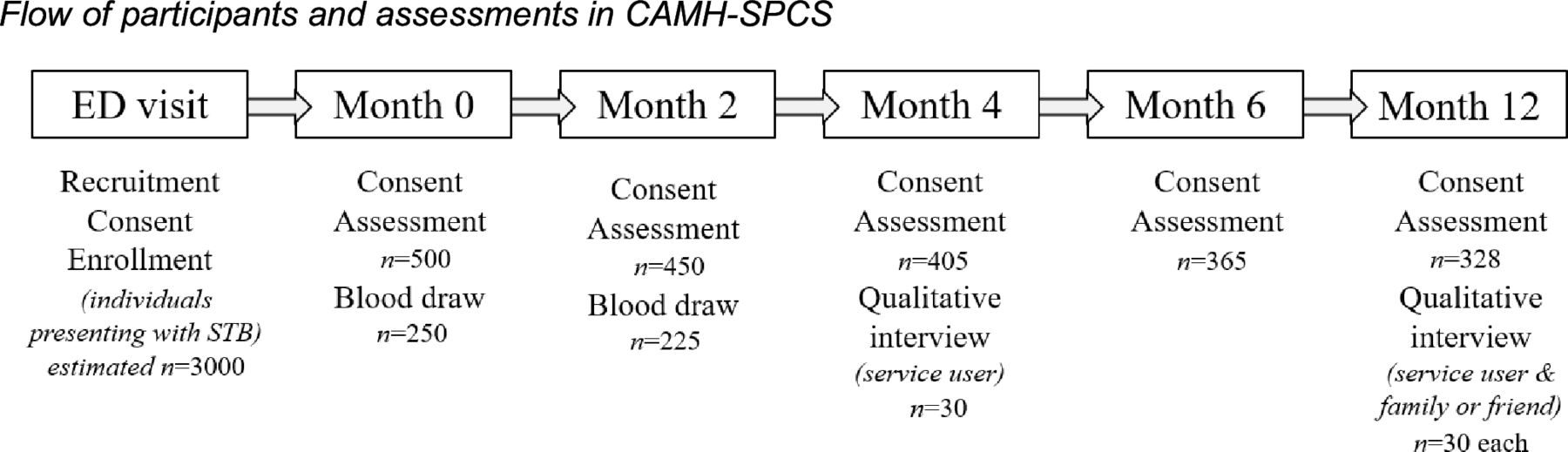
Objectives 1–2 (Characterizing and situating the cohort). Measures of STB, clinical, psychological, and sociodemographic characteristics will be administered at baseline and follow-ups over 1 year (i.e., at 2, 4, 6 and 12 months) (depicted in figure 1). Table 1 provides measures administered at each follow-up, their rationale for inclusion and psychometric properties. Measures of cohort participants’ health service utilisation for STB over the follow-up year will be derived using data from ICES, a provincial health administrative data research institute in Ontario (described in online supplemental appendix D).
Supplemental material

{kind=link}
Consent is reviewed at all study visits. Sample sizes at follow-up months are estimated based on a 10% attrition rate at each study visit. CAMH-SPCS, Centre for Addiction and Mental Health Suicide Prevention Cohort Study; STB, suicidal thoughts and behaviours.
Outcomes of interest include:
Self-reported STB, including NSSI;
Mental health service utilization, including ED and inpatient care;
SB requiring ED care; and
Death by suicide and all-cause mortality (i.e., to capture deaths related to substance use, traumatic injuries, and other causes of death not classified as suicide).
Objective 3 (Understanding experiences). The guides used to collect qualitative data during semi-structured interviews are provided in online supplemental appendix A. Interviews at 4 months will focus on experiences with STB, and interviews at 12 months will focus on preventative interventions (i.e., risk screening, psychotherapies, safety planning, and means restriction). In interviews at 12 months, family members or friends will offer their perspectives on supporting individuals with STB.
Objective 4 (Exploring biomarkers). For biomarker exploration, we will use liquid chromatography-mass spectrometry to identify proteins that are significantly elevated or decreased with STB, by comparing the two time points from each participant. We will also focus on two known protein interactions plausibly related to STB: the dopamine receptor D1-D250 and the GR-FKBP51 complexes.48 49 For mRNA biomarkers, we will similarly conduct a hypothesis-free transcriptome screen using RNAseq, as well as targeted transcription analyses with candidate genes identified from the proteomic analysis. Also, we will interrogate DARPP-3295 and SRR mRNA96 to examine whether these transcript levels in peripheral blood leukocytes are correlated with STB. Finally, using methods established in prior work, we will examine genomic DNA extracted from peripheral blood leukocytes, to determine whether STB is associated with altered DNA methylation patterns in peripheral blood.97 We will also perform a targeted examination of glucocorticoid receptor gene NR3C1 methylation in relation to STB.
Data sources/measurement
Data sources include evaluator-rated and self-rated measures (table 1) as well as health administrative data from ICES (table 2). For outcomes, self-reported STB is measured with the Columbia-Suicide Severity Rating Scale (C-SSRS)98 and the Self-Injurious Thoughts and Behaviours Interview-Non-suicidal Self Injury section (SITBI-NSSI).99 Mental health service utilization is measured with ICES data (table 2) and self-report (table 1), which captures non-public forms of support (e.g., psychotherapy). ICES data also measures SB requiring ED care, and death by suicide and all-cause mortality, based on libraries and codes provided in table 2.
Description of data used for cohort comparisons
Bias
To address selection bias, we will take measures to promote inclusive and equitable recruitment and retention of marginalized and underserved groups in the study. Our recruitment strategy ensures that any potentially eligible individuals seeking ED care are approached by dedicated research team members and offered an opportunity to participate. Our study team is diverse, and we will develop recruitment benchmarks to ensure diversity in the CAMH-SPCS cohort, as related to their clinical presentations (i.e., SI, SB) and relevant demographics. We will also follow empirically supported strategies for retention.100 These include reducing barriers to participation (i.e., reimbursements of costs, coordination of study visits with existing CAMH appointments, options for virtual participation), building community (i.e., with a study website, regular updates, and knowledge exchange events), offering follow-up incentives and reminders, and tracking outcomes in patients lost to follow-up with health administrative data. However, it is possible that our inclusion criteria, such as the requirement for a valid health card number, will exclude certain marginalized groups experiencing STB, including those who are not eligible for provincial healthcare, primarily temporary residents, asylum seekers or refugees. To better identify sources of bias and other potential limitations in our study, we will form a diverse Study Advisory Council, made up of people with lived experience of STB, family members or friends of people with lived experience, and frontline clinicians. This Council, recruited with inclusive and equitable search and selection practices, will support the creation of relevant and accessible study educational materials, as well as advise on promoting equity, diversity, and inclusion in recruitment and retention.
Study size
Objective 1 (Characterizing the cohort). A sample size of 500 is similar to samples in other cohort studies and is feasible to attain given an estimated 3000 eligible patients during the study enrolment period.73 101–103 With an expected attrition rate of 10% after each follow-up point, we anticipate 328 participants (65% of the cohort) will complete the study (see figure 1). It would not be feasible to achieve adequate statistical power in detecting the rare outcome of suicide (Outcome 4) with a prospective cohort design, so we focused on powering our study to detect STB (Outcomes 1–3). According to a power analysis based on alpha >0.05, beta of 20%, assuming a compound symmetry covariance structure, and a 0.7 within-person correlation, a sample of 328 participants provides 80% power in detecting a 0.65 relative risk of self-reported STB (Outcome 1).73 We expect increased power in detecting other STB-related outcomes (Outcomes 2–3), which are tracked with health administrative data and should be available for almost all 500 participants, even if they are lost to follow-up.
Objective 2 (Situating the cohort). We estimate that during the study enrolment period, 3000 patients will present for services to the CAMH ED with STB, and an estimated 12, 750 patients will present for services for any reason, calculated from 8500 unique patients seen in 2021. For cohorts of patients presenting for services in any Ontario ED during the study period, we estimate that 2760 individuals will present with SB based on rates reported in a recent retrospective cohort study,104 and an estimated 9, 320, 000 individuals will present for any reason based on ED utilization data reported by the Canadian Institute for Health Information.105
Objective 3 (Understanding experiences). Sample sizes required for qualitative research are difficult to determine in advance, but qualitative interview samples typically reach saturation with 10–20 participants.106 Since our sample includes individuals whose experiences represent the continuum of risk according to STB and sociodemographic characteristics, we expect to reach saturation with a larger sample of 30–40 participants. Nevertheless, we will continue to recruit participants for qualitative interviews until saturation is reached.
Objective 4 (Exploring biomarkers). We aim to investigate changes in protein, mRNA, and DNA methylation associated with STB. We will analyze blood samples from 30 participants selected for maximal differences in STB between the two sample times. This initial sample will serve to demonstrate feasibility of the biomarker analysis. By performing within-subject comparisons on those with the greatest change in STB, we will maximize power while reducing the impact of inter-individual differences unrelated to STB. There will be two parts to this biomarker study: a broad screening component and a targeted study of selected candidate molecules chosen from proteins or genes that we have previously studied. These proteins or genes are related to phenotypes relevant to STB, such as depression or PTSD.
Statistical methods
Objective 1. Characterizing the cohort
Evaluator-rated and self-rated measures (see online supplemental appendix D), linked with health administrative data from ICES (see table 2), will be used to characterize the cohort. We will examine the cohort’s sociodemographic, clinical, and psychological factors using descriptive statistics. We will also use descriptive statistics to examine the four outcomes of key interest occurring at any time in the 12 months following ED presentation. For participants lost to follow-up, outcomes related to health service utilization, SB requiring ED care, and death by suicide or all-cause mortality will still be tracked via ICES linkage.
To examine differences in profiles of cohort participants, we will use mixture modelling, which are a set of techniques for identifying discrete, hidden groups from observed data.107 Mixture models will be estimated by conditioning probabilities of allocating each CAMH-SPCS cohort participant to a group based on data collected at baseline (see online supplemental appendix D). Based on prior work, this analysis will focus on clinical factors, including mental illness, prior SB or NSSI, and related service use,18 59 62 76–80 108–112 as well as sociodemographic and psychological factors, including age, sex, childhood adversity and social and economic marginalization.14–29 81 82 113 Since the data used to capture these factors are primarily continuous (i.e., summed scores or subscale scores), we will use latent profile analysis.107 We will choose the number of profiles based on mixture model fit statistics (log-likelihood, AIC, BIC), with the expectation that four to five profiles may emerge, characterized by differences in the nature and severity of illness, and in sociodemographic and psychological factors.30
To compare sociodemographic, clinical, and psychological characteristics of the emerging profiles, we will generate descriptive statistics stratified by profile. We will also complete a regression analysis to examine the associations of profiles to our four outcomes, with an additional outcome of suicidal ideation in the 12 months following ED presentation, as measured with the C-SSRS. We will repeat analyses for this objective stratified by sex and gender, to account for potential differences in characteristics and profiles between men and women, as well as between individuals identifying as man or woman, and a different gender.
Objective 2. Situating the cohort
First, we will generate descriptive statistics to examine demographic, clinical, and visit-related factors (listed in table 2) in the CAMH-SPCS cohort and each of the four comparison cohorts (which exclude CAMH-SPCS participants). We will also examine three outcomes captured with health administrative data via ICES (i.e., mental health service utilisation, SB requiring ED care, and death by suicide or all-cause mortality). SB will be represented as a binary variable indicating its presence or absence, as well as a categorical variable indicating number of attempts (i.e., 1, 1–3, >3). Death by suicide will additionally be calculated in terms of 100, 000 person-years.
For the CAMH-SPCS cohort and the CAMH ED cohort with STB, we will compare their demographic, clinical, and visit-related factors, in addition to outcomes using t-tests for continuous variables, and χ2 and Mantel-Haenszel tests for dichotomous and ordinal variables respectively. We will calculate effect sizes to quantify differences between cohorts. We will also conduct a multivariable logistic regression to determine factors associated with enrolment in CAMH-SPCS.
In each remaining cohort (i.e., CAMH ED cohort, Ontario ED cohort with SB, Ontario ED cohort), we will examine associations of demographic, clinical, and visit-related factors (table 2) with the three outcomes, using t-tests, χ2 tests and Mantel-Haenszel tests. In each cohort, we will use multivariable regression models to test associations of factors with each outcome. Additionally, we will compare the CAMH-SPCS cohort to each of these remaining cohorts with Cox proportional hazard regression models, which will compare the groups on time to each outcome. We will generate crude models, models adjusted for demographic factors, and models adjusted for demographic, clinical, and visit-related factors. When modelling death by suicide, we will conduct additional survival analyses incorporating time to event measures, censoring cohort members lost to follow-up or those who experience death for reasons other than suicide.
We will repeat all analyses for this objective, stratified by sex, to account for potential differences in SB between men and women. We are not able to account for gender, since ICES does not contain a measure or proxy measure.
Objective 3. Understanding experiences
We will analyze qualitative interview data descriptively and thematically, based on a realist research framework, which seeks to identify what works for whom and in which contexts, with participation from relevant stakeholders in intervention design and implementation (i.e., service users and their family or friends).114–116 Accordingly, analysis will focus on contextual factors, underlying mechanisms and STB outcomes. Transcripts and supplementary field notes will be entered into and analysed using a secure, qualitative software. Transcripts will be coded to reflect references to contexts, mechanisms, or outcomes as per the Realist framework; phrases coded as mechanisms will attempt to distinguish between resource- or reasoning-based mechanisms.117 Three to five transcripts will be independently coded by at least three team members to align on coding strategy, ensure consistency, and resolve discrepancies. Phrases coded as context, mechanism or outcome will be iteratively synthesised and hierarchically amalgamated into dyads and triads of data, to identify relationships between variables (e.g., between two contextual factors, a contextual factor and a mechanism, or a mechanism and a particular outcome,).118 Evidence will be gathered under a particular dyad or triad heading and iteratively synthesised into overarching context-mechanism-outcome conjectures, or theories of change, that describe what may work, for whom, to what extent, how, and under which circumstances.114 117 In consultation with the Study Advisory Council, findings will provide insights into what interventions are likely to be most effective, as well as facilitators and barriers. Insights will be used to inform the design of an intervention, its implementation, and evaluation at CAMH.
Objective 4. Exploring biomarkers
Analysis of blood samples will focus on within-participant comparisons between contrasting states of STB. We will examine protein, mRNA, and epigenetic DNA modifications40–42 between the baseline and follow-up visits for the subset of 30 CAMH-SPCS participants. These particular assays were selected to enable a broad hypothesis-free screen for novel molecular correlates of STB. While there is unlikely to be a specific molecular marker for STB, we hypothesize that there may be novel pathways, protein complexes, or molecular markers that change in concert with fluctuations in STB between study visits that modulate component behaviours contributing to STB. We will combine a broad hypothesis-free screen with focused interrogation of specific predetermined molecular targets. The candidate genes and proteins we mention earlier were selected based on our previous work related to depression and PTSD.48–50 There have been many previous studies of biological markers in suicide, with the serotonin system as perhaps the most well-known example. It is likely that components of that neurotransmitter system will emerge from the screening phase of our experiments. In subsequent studies, we will use the results of our screening experiments as the basis for additional experiments to characterize biological pathways and mechanisms that influence STB, which could be targeted by novel treatment strategies.
Ethics and dissemination
This study was approved by the Centre for Addiction and Mental Health Research Ethics Board (REB #2022/222). The CAMH-SPCS cohort study presents ethical challenges given its focus on STB in an acute care population; various safeguards are in place to ensure the well-being of study participants and the research team. Research team members will consult with ED clinicians on the appropriateness and safety of approaching eligible patients for recruitment. All patients approached will be offered an informational resource package for STB. Throughout the study, research team members will monitor changes in SI with a screening tool (see online supplemental appendix B) and follow risk management procedures as needed (see online supplemental appendix C). As part of these procedures, participants may be withdrawn from the study if they require imminent care or further participation is deemed unsafe. Trained interviewers will use qualitative interview guides flexibly to manage risks of anxiety or distress related to discussing sensitive topics and risk of misrepresentation will be attenuated by offering participants opportunities to review interview transcripts prior to analysis. To manage risks to the safety of research team members, ED clinicians will be available to support recruitment of challenging patients, and all team members will follow protocols to manage any challenging or aggressive patient behaviours (see online supplemental appendix C). All non-clinical research team members will have access to urgent support from study psychiatrists or the research coordinator, who will meet with them regularly for debriefing and check-ins.
Patient and public involvement
In our integrated approach to knowledge dissemination and translation, patient and family knowledge users (i.e., Study Advisory Council members) are considered equal partners within each study phase. Study Advisory Council members will provide feedback regarding design, execution, and dissemination of the study. Several members will have leadership positions, be full and equal members of the study team, and receive appropriate financial support. To communicate study updates and results, we will establish a study website, deliver webinars, and participate in media discussions. In the second study year, we will also hold a virtual full-day meeting at CAMH with researchers, policymakers, and Study Advisory Council Members, which will be open to study participants and the broader community. Non-academic modes of dissemination involve broadcasting videos and podcasts with the research team and Study Advisory Council Members.
Impact
The CAMH-SPCS implements key advances for suicide prevention research. The combination of clinical, neuropsychological, and psychosocial assessments with molecular markers will contribute to research on the diverse mechanisms underlying suicide risk and enhance our understanding of its multifactorial nature. Also, incorporating health administrative data will allow us to track outcomes for individuals lost to follow-up, and for longer than the 12-month study observation period. Using administrative data to compare the characteristics of CAMH-SPCS participants against other cohorts is a unique opportunity to gauge the generalizability of our findings, which will elucidate the strengths and limitations of cohort composition and provide an understanding of factors contributing to enrolment in suicide prevention studies. Qualitative interviews will centre experiences of patients and their family members or friends and contribute to the codevelopment of effective preventative interventions, which are attuned to the unique contextual factors impacting their implementation and evaluation. The integration of biomarkers will inform our understanding about the neurobiology of suicide, molecular predictors of suicide risk, and new targets for treatment in the future. Taken together, our findings will provide critical insights into the characteristics, experiences, and outcomes of individuals with STB, who are often under-represented in mental health research. Our findings also have health services implications by informing our understanding of STB rates, the development of suicide prevention strategies, and standards and scorecards for mental health system performance in Ontario, Canada. These findings and best practices will be disseminated in consultations with hospitals and institutions across the province.
Additionally, the CAMH-SPCS aims to be a catalyst for future research. Given that ethical and methodological issues make classic randomized control trials a poor fit for complex applied interventions, data from this cohort can serve as a ‘treatment as usual’ baseline comparison. They can be used to evaluate preventative interventions in future research, such as those codesigned with service users and their family members or friends in CAMH-SPCS. The blood samples collected from the broader CAMH-SPCS cohort will comprise an important biobank for future research and discovery. The study will also create an infrastructure foundation for studying STB in ED settings, with the possibility to expand the suicide prevention cohort approach across other institutions nationally and internationally. The CAMH-SPCS will play a vital role in increasing our understanding of individuals experiencing STB and ways to provide them with the support they need; this understanding is an important step towards reducing rates of suicide and mitigating its devastating impacts.
Ethics statements
Patient consent for publication
References
Footnotes
X @DrDCourtney, @AmyGajaria, @june_sh_lam, @yonalunsky, @juveriazaheer
PB and MM contributed equally.
Contributors JZ and AHCW are the principal investigators who conceived the study design for the research protocol and acquired funding. PB and MMa wrote the initial manuscript draft. All authors (PB, MMa, AHCW, BM, DB, DC, MIH, PK, RAK, AT, AG, AD, AM, AS, AA, AC, AP, BF, CO, DZB, FL, GS, JSHL, MB, MMo, NR, MOH, SA, SM, VDL, VS, YL, JZ) critically reviewed, revised, and approved the final version of the manuscript. JZ is the guarantor of this study protocol.
Funding This work was supported by the Centre for Addiction and Mental Health Discovery Fund. The funder did not play a role in the design of the study and will not contribute to the collection, analysis, or interpretation of the data.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, conduct, reporting or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.