Article Text

Abstract
Background Unintended pregnancies pose significant public health challenges globally, particularly in the Middle East and North Africa (MENA) region, where cultural, religious and societal factors play the most substantial role. This systematic review and meta-analysis investigated the pooled prevalence and factors associated with unintended pregnancies in the MENA region.
Methods We conducted a systematic review to identify relevant studies in Medical Literature Analysis and Retriaval System (MEDLINE), Embase and Scopus published on unintended pregnancies until July 2024. We included studies that were conducted on unintended pregnancy prevalence within MENA countries and employed suitable measurement tools. We analysed data from 40 studies involving 34 837 participants across the region, including Egypt, Iran, Saudi Arabia and Qatar. We used a random-effects model to estimate the pooled prevalence of unintended pregnancy.
Results In this meta-analysis, we found that the overall prevalence of unintended pregnancy was 27.0% (95% CI 25.0% to 30.0%) in the MENA region, and the certainty of the evidence was moderate. Saudi Arabia had the highest prevalence of unintended pregnancy at 32.0% (95% CI 27.0% to 38.0%). A lower prevalence, 10.0% (95% CI 8.0% to 14.0%), was found in the studies that used validated tools compared with non-validated tools to measure unintended pregnancy. Between 2006 and 2010, the prevalence was 34.0% (95% CI 28.0% to 40.0%), the highest compared to other time periods . Age, rural areas, education, employment, economic status, parity, gravidity, history of miscarriage, previous pregnancies or abortion, non-use or failure of contraception methods, limited antenatal care, were associated with unintended pregnancies.
Conclusion Our findings suggest that the MENA region faces a substantial burden of unintended pregnancies, with variations among countries and over time. The results emphasise the need for evidence-based interventions to address this issue, focusing on factors associated with unintended pregnancy.
- Pregnant Women
- SEXUAL MEDICINE
- Systematic Review
- Meta-Analysis
- REPRODUCTIVE MEDICINE
- Risk Factors
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Further details can be obtained from the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
Comprehensive search strategies were developed across three major databases without language restrictions.
Two independent reviewers carried out the screening and full-text review processes.
We rated the certainty of evidence using the Grading of Recommendations Assessment, Development, and Evaluation approach.
The review included studies from only four countries in the MENA region, limiting the generalisability of findings across the entire region.
Data collection in some studies relied on surveys, which may introduce recall bias and affect the accuracy of reported unintended pregnancy prevalence.
Introduction
Unintended pregnancies, meaning both mistimed and unplanned pregnancies, have recently emerged as a critical global public health challenge with profound implications for reproductive health and family well-being.1 Despite advancements in modern contraceptive methods, approximately 80 million women worldwide experience unintended pregnancies each year.2 This issue becomes crucial in the Middle East and North Africa (MENA) region. In this predominantly Muslim region, the significance of this issue arises from the intricate interplay between religious beliefs, cultural norms, societal attitudes and legal frameworks.3 4 Unintended pregnancies can have severe negative impacts, including increased risks of maternal depression, anxiety and reduced quality of life for the parent, as well as adverse health outcomes for the baby, such as preterm birth, low birth weight and inadequate prenatal care.5–8 Consequently, unintended pregnancies in the MENA region continue to exert a substantial toll on the well-being of women, their families and overall public health.9
Findings from a recent study conducted across six MENA countries, namely Algeria, Lebanon, Morocco, Palestine, Syria and Yemen, revealed an alarming number of unintended pregnancies of approximately 1.2 million.1 Another investigation of unintended pregnancy in the MENA region reported a prevalence of 40% in 2017, with about 50% and 11% of these being terminated through abortion and miscarriage.10 Notably, the prevalence of unintended pregnancies in the MENA region was found to have significant variability over the past decade, ranging from 15% to 58%.9 In the Arab region, one in four births was attributed to unintended pregnancies, which signified the extensive impact of this issue.9 A recent study in Saudi Arabia reported that over half (53.4%) of current pregnancies were unintended, reflecting a mistimed circumstance.11 Moreover, concern repeats, as Jurdi et al reported that approximately 40% of unintended pregnancies occurring within the past 5 years were identified as second- or higher-order pregnancies in Jordan.12
A recent study conducted in Saudi Arabia revealed that approximately one-third of the participants had an unmet need for family planning services, with major reasons for non-utilisation of contraceptives including inaccessibility of family planning methods (68.0%), insufficient knowledge (59.5%), adherence to religious beliefs (49.6%) and resistance from husbands (42.7%), which highlighted a significant demand for contraception there.13 Another study conducted in Jeddah, Saudi Arabia, found that women had lower knowledge about contraception, with considerable misconceptions and concerns.14 Moreover, a recent study conducted in Riyadh, Saudi Arabia, observed that a majority (82%) of the study participants had a lack of awareness regarding emergency contraceptives, with only a limited (18%) possessing some level of knowledge.15
Unintended pregnancies are associated with adverse maternal behaviours, stress, depression, quality of life, marital conflict and violence.6 16 17 Unintended pregnancies also affect children, including childhood mortality, premature birth, inadequate prenatal care, inadequate immunisation, remaining stunted, maltreating behaviours and several distressing consequences.9 18–20 Furthermore, the occurrence of induced abortions resulting from unintended pregnancies may increase the risk of maternal mortality and morbidity.3 In the Arab region, unsafe abortions contribute to approximately 10% of maternal deaths, highlighting the urgent need for safe alternatives.9
A lack of knowledge and awareness among reproductive women in the MENA region may act as significant impediments that may enhance the higher prevalence of unintended pregnancies.3 6 9 16–20 Despite the high prevalence and burden of unintended pregnancies in the MENA region, data investigating this issue remain relatively limited. Investigating the pooled prevalence and factors of unintended pregnancies is crucial to identifying areas of concern and informing targeted interventions to reduce the consequences. Therefore, we aimed to conduct a comprehensive systematic review and meta-analysis to determine the overall prevalence and factors associated with unintended pregnancies in the MENA region.
Methods
Search strategy
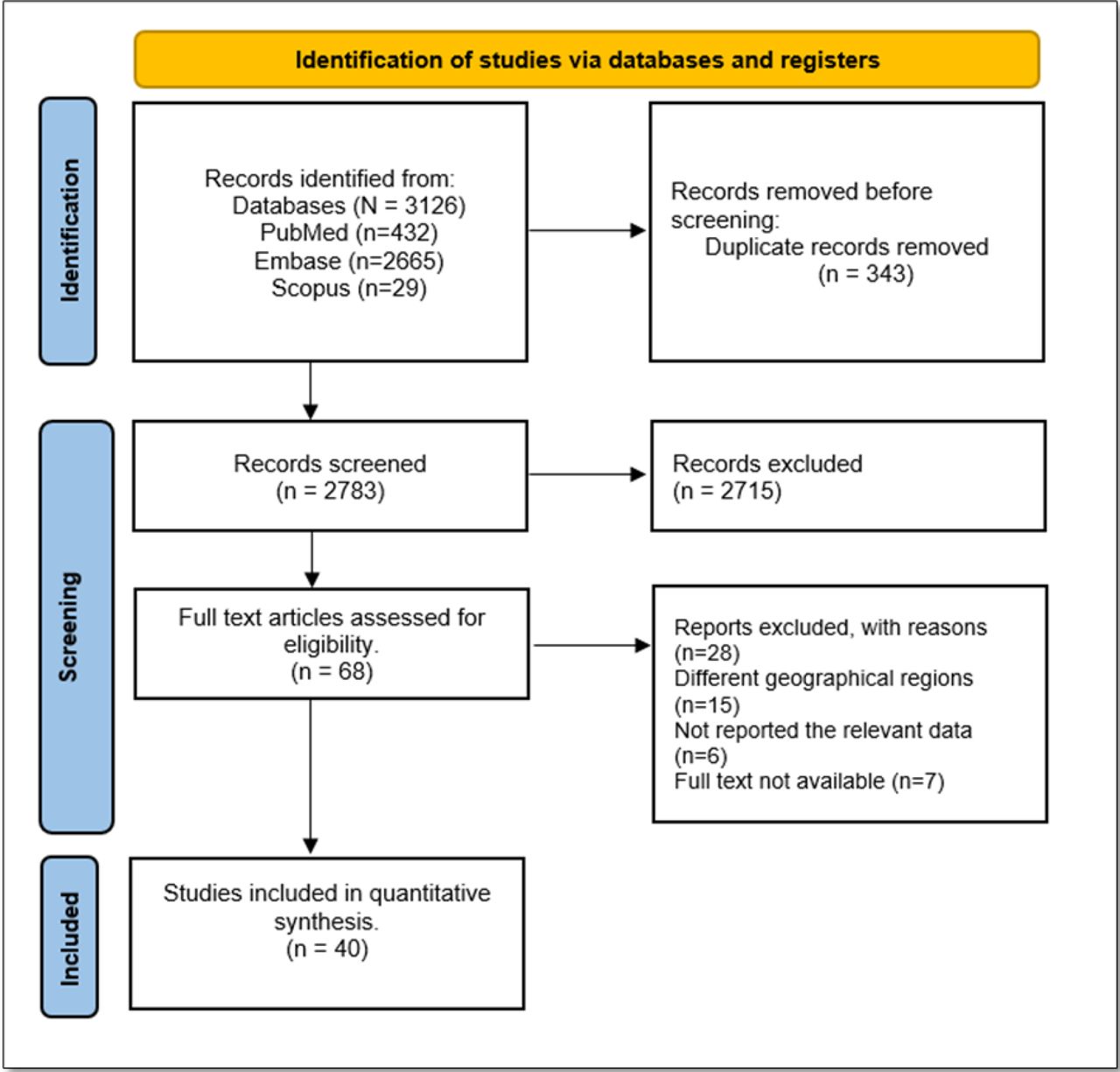
We developed a comprehensive search strategy to identify all relevant studies on unintended pregnancy in the MENA region. The search strategy incorporated a combination of carefully selected keywords and Medical Subject Headings terms specifically focused on capturing relevant literature on unintended pregnancy in MENA countries. We conducted the search in MEDLINE, Embase and Scopus from inception to July 2024. Furthermore, a manual search included looking for relevant studies in the reference lists of the included papers. Details of the search strategies are provided in the online supplemental table 1 of online supplemental file 1. The outcomes of the search strategy and the subsequent study selection process are presented in figure 1, employing the widely recognised Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) format.
Supplemental material

PRISMA flowchart depicting the total number of studies screened, selected and included. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study selection
The study selection process consisted of two stages: (a) initial screening based on titles and abstracts and (b) a comprehensive evaluation of the full-text articles in any language. We used Google Translate to translate studies published in languages other than English. To ensure the careful assessment of each identified article following the inclusion criteria, two independent reviewers (SM and MSI) scrutinised the titles, abstracts and the full text. The objective was to determine the relevance of each study to ascertain its potential eligibility for inclusion in the systematic review. A collaborative discussion ensued in disagreements between the reviewers’ assessments, involving a third reviewer (NI) when necessary. This approach assisted in fostering consensus and maintained the consistency of the selection process. The studies that passed the initial screening phase underwent a thorough full-text assessment.
Inclusion and exclusion criteria
To include studies in the systematic review, studies had to meet specific criteria. These included reporting the prevalence of unintended pregnancy in the MENA region, conducting the studies within MENA countries, using measures of unintended pregnancy (eg, self-report, surveys and medical records) and providing information on sample size and the characteristics of the included sample. These criteria ensured the inclusion of studies directly relevant to the research question and allowed for a comprehensive examination of unintended pregnancy within the MENA region. We excluded studies if they were not peer-reviewed or relied on non-primary sources such as editorials, letters, commentaries or reviews.
Data extraction
Two reviewers (NA and UE) conducted data extraction independently using a standardised data extraction form. We thoroughly examined each of the included studies. We extracted the following information: titles, authors, year of publication, country, study design, source of the sample, settings, area of study, mean ages, description of the sample, status of the sample (general or high or special risk), number of children, marital status, definition or measure of unintended pregnancy, data collection methods and point of unintended pregnancy evaluation. Throughout the data extraction process, reviewers provided attention to maintaining consistency. In cases where discrepancies arose between the reviewers’ extractions, rigorous discussions took place to reach a consensus. When necessary, the third reviewer (NI) was consulted to resolve any disagreements in the data extraction.
Risk of bias assessment
Reviewers assessed the risk of bias in the included studies using the tool put forward according to Hoy et al.21 This tool comprises 10 distinct items designed to assess a study’s external validity (questions 1–4) and internal validity (questions 5–10). Each question is assigned a binary score, denoting either ‘yes’ (indicating a low risk of bias) or ‘no’ (indicating a high risk of bias). Consequently, for a study to be classified as having a low risk of bias, it must achieve a score of eight or higher. Studies scoring between six and seven are categorised as having a moderate risk of bias, while those scoring five or fewer are considered to have a high risk of bias. Two independent reviewers (NWH and UE) assessed the risk of bias of included studies in this review. In cases where discrepancies emerged between their assessments, comprehensive discussions were held to achieve consensus. When required, the third reviewer (NI) assisted in resolving disagreements regarding the risk of bias.
Data synthesis and analysis
We conducted the meta-analysis while the included studies were considered sufficiently homogeneous regarding study design, population characteristics and outcome measures. In terms of statistical analysis, we employed appropriate methods, such as random-effects models with logit transformation, to pool the prevalence of unintended pregnancy and to estimate the overall prevalence. We assessed heterogeneity between studies using the Cochrane Q test and Higgin’s I² value. Smaller p values and I2>50% indicate significant heterogeneity. Forest plots display the prevalence of unintended pregnancy with corresponding 95% CIs. We used funnel plots to assess the publication bias. For all the statistical analysis, we used Stata V.16.
Certainty of the evidence assessment
We rated the overall certainty (quality) of the evidence for prevalence as high, moderate, low or very low using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach.22 23 The GRADE approach involves assessing imprecision, inconsistency, risk of bias, indirectness, publication bias and factors for rating up (eg, large effects, dose-response and accounting for plausible residual confounding). We presented the review’s findings in the evidence profile table as suggested by Cochrane.24
Subgroup and sensitivity analysis
We conducted a predefined subgroup analysis based on the countries in the region, source of the sample (population vs hospital/healthcare centre), study period or recruitment, sampling methods (probability vs non-probability), the sample of women included (postpartum women with live births vs postpartum women with any birth vs all pregnant women), point of unintended pregnancy evaluation (during pregnancy vs right after birth vs 6 months after birth vs 3 years after birth) and assessment method (validated instrument, ie, London Measure of Unplanned Pregnancy (LMUP) vs no validated instruments). We excluded the moderate or high risk of bias studies for sensitivity analysis. The sensitivity analysis was conducted based on methodological considerations that studies with moderate or high risk of bias may introduce potential sources of systematic error or confounding into the analysis, affecting the robustness of the findings.
Metaregression
We performed a-priori planned meta-regression to evaluate if the publication year impacts the variability of the prevalence and as a possible cause of heterogeneity. We assumed the importance of understanding the trend in the prevalence of unintended pregnancy, which may rise or decline over time.
Reporting
We followed the PRISMA guidelines to report the findings of this systematic review and meta-analysis (online supplemental file 2). We created a flowchart to illustrate the study selection process and the number of studies included at each stage, providing a clear overview of the review’s progression. The characteristics of the included studies, including study design, sample size and prevalence of unintended pregnancy, were summarised and presented in the online supplemental table 2 of online supplemental file 1. We generated forest plots to present the meta-analysis results visually, facilitating the interpretation and comparison of prevalence estimates across studies.
Supplemental material
Patient and public involvement
This study is a systematic review, and as such, it did not involve the collection or analysis of individual patient data. A comprehensive literature search was conducted using predefined databases. Consequently, patients were not involved in the design, conduct, analysis, or dissemination of this research.
Results
Characteristics of the included studies
The characteristics of the included studies are presented in the online supplemental table 2 of online supplemental file 1. The initial literature search identified 3126 records, and after removing 343 duplicate records, 2783 articles underwent title and abstract screening. Among these, we excluded 2715 articles from further consideration. We found 68 full-text articles for eligibility; ultimately, 40 articles met the criteria for inclusion in the analysis (figure 1). Overall, the included studies involved a combined sample of 34 837 participants from four different countries: Egypt, Iran, Saudi Arabia and Qatar. Most included studies, accounting for 84.6% (n=33), employed cross-sectional methods. Most of the included studies were conducted in Iran (n=35 studies). The sample sizes of the studies ranged from 102 (Azizi 2011) to 5152 (Almasi-Hashiani 2019), and 90.0% (n=36 studies) of the included studies recruited samples from hospital/healthcare settings. The publication year of the studies ranged from 2002 to 2022, but the majority were carried out after 2010 (n=30 studies).
Prevalence of unintended pregnancy
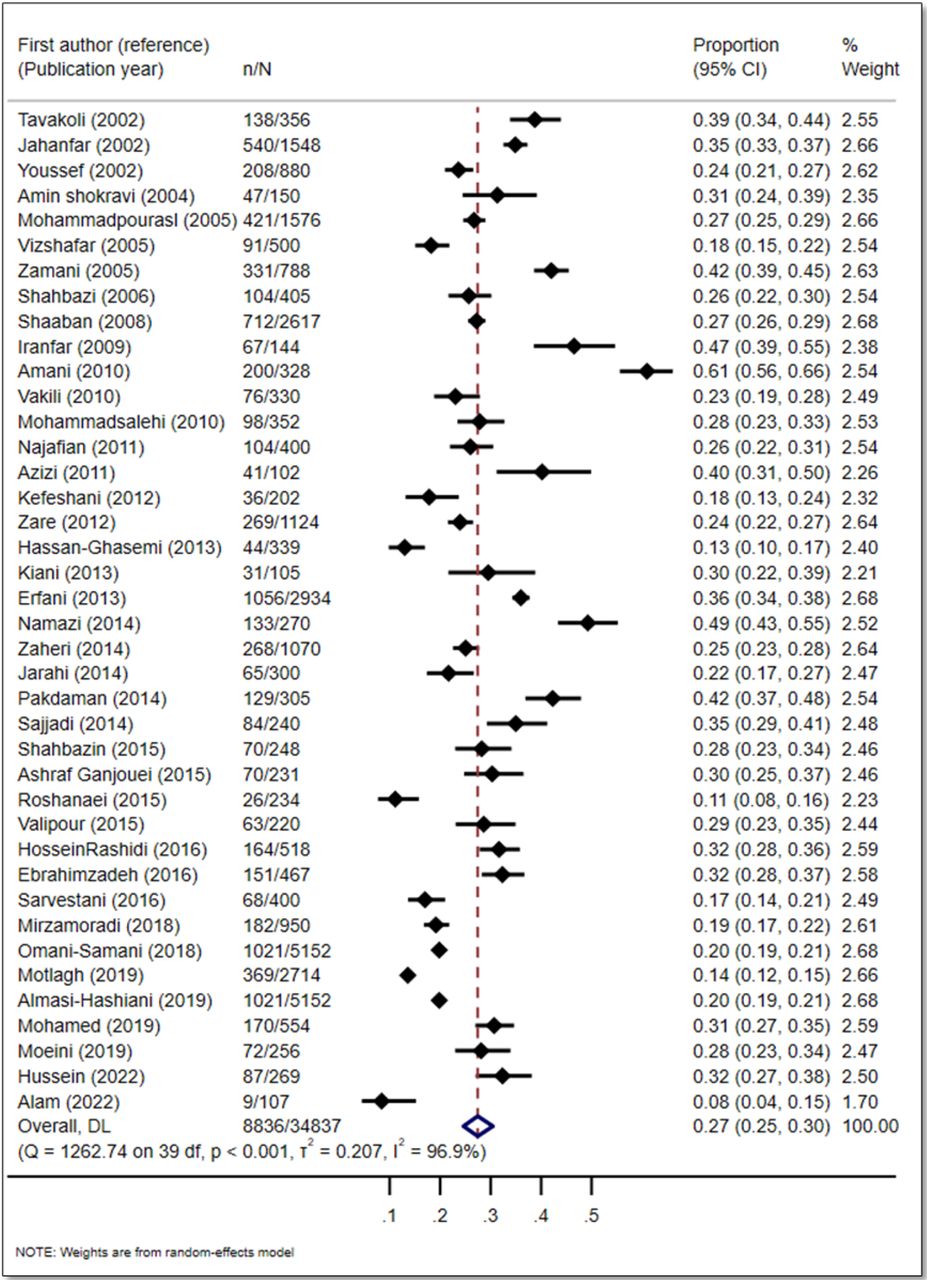
We found that the overall prevalence of unintended pregnancy in the MENA region was 27.0% (95% CI 25.0% to 30.0%; I2: 96.9%), and the certainty of the evidence was moderate due to inconsistency. The prevalence across studies ranged from 11.0% to 49.0% (figure 2, table 1).

Forest plot showing the pooled prevalence of unintended pregnancies.
GRADE evidence profile: prevalence of unintended pregnancy in MENA regions
Publication bias
This funnel plot shows was used to assess publication bias inn the main outcome (figure 3). The data points in the funnel plot exhibit a roughly symmetrical distribution, suggesting the absence of conerns about substantial publication bias.

{kind=link}
{kind=link}
{kind=link}
Funnel plot showing the publication bias of the review.
Assessment of risk of bias
Of the 40 included studies, 20 had a low risk of bias. The details of the risk of bias are presented in the online supplemental table 3 of online supplemental file 1.
Subgroup analysis
The results of subgroup analyses are summarised in table 2. We found a significant variation based on the country of study conducted, study period or recruitment and assessment of the unintended pregnancy done by the LMUP. In the MENA region, Saudi Arabia had the highest prevalence of unintended pregnancy at 32.0% (95% CI 27.0% to 38.0%) compared with other countries, but it was based on only one study. The prevalence of unintended pregnancy fluctuated over time. Between 2006 and 2010, the prevalence was 34.0% (95% CI 28.0% to 40.0%), the highest. The lowest prevalence was observed between 2016 and 2020, with a pooled prevalence of 20.0% (95% CI 14.0% to 27.0%). We found that when unintended pregnancy was assessed using the validated LMUP, the prevalence was significantly lower at 10.0% (95% CI 8.0% to 14.0%) compared with 29.0% (95% CI 26.0% to 32.0%) when using non-validated measures. We found no significant variation when subgroup analyses were conducted based on the sample source, sampling methods, sample of women included and point of unintended pregnancy evaluation.
Subgroup analysis by country, source of sample, study period/recruitment sampling methods, sample of women included, point of evaluation and measure of unintended pregnancy by the London Measure of Unplanned Pregnancy (LMUP)
Sensitivity analysis
We did not find any difference in pooled prevalence estimates after removing studies with moderate or high risk of bias (online supplemental figure 1).
Supplemental material
Metaregression
We observed a decrease in the log event rate over time, quantified by the publication year; however, it was not statistically significant (online supplemental figure 2).
Supplemental material
Narrative review of risk factors
We presented the risk factors for unintended pregnancies in online supplemental table 4 of online supplemental file 1. We found several studies investigating factors associated with unintended pregnancy in the MENA region. The age of the woman or the mother’s age was associated with unintended pregnancy.25–38 The age of the father was also associated with unintended pregnancies.25 31 39 40 Women with a higher age at conception were associated with unintended pregnancy.25 41 The included studies reported that the education of the couple was associated with unintended pregnancy.25 28 30–32 35 37–40 42 43 Specifically, the mother’s education was found to be associated with unintended pregnancy.25 26 29 31 34 43 The education of the father was also associated with unintended pregnancy.25 29 40 44 Parents’ occupation was associated with unintended pregnancy.40 42 45 Employment status was also associated with unintended pregnancies.28 30 37 41 46 Several studies reported that the place of residence was associated with unintended pregnancies.27 33 34 42 Specifically, living in rural residences was also associated with unintended pregnancies, according to Youssef et al25 Youssef et al and Almasi-Hashiani et al reported that family size was associated with unintended pregnancies.25 27 The crowding index was reported as a risk factor for unintended pregnancies.25 Youssef et al. reported that the sleeping index was a risk factor for unintended pregnancies.25 Wealth, income or economic status was reported as risk factors for unintended pregnancies in numerous studies.26 27 38 42 46 Several studies reported that a history of previous pregnancies was a risk factor for unintended pregnancies.29–31 35 36 42 44 46 47 History of previous unintended pregnancies was also associated with unintended pregnancies in numerous studies.32 38 39 47 48 Studies reported that the space or interval between pregnancies was associated with unintended pregnancies.26 32 49 A large number of studies reported that a history of miscarriage or abortion was associated with unintended pregnancies.25–27 30 43 44 Several studies reported parity as a risk factor for unintended pregnancies.26 40 44 Non-use, lack of use or failure of contraception methods was reported as risk factors for unintended pregnancies in several studies.25 27 28 33 39 41 43 46 50 Youssef et al reported that antenatal care was associated with unintended pregnancies.25 Several studies reported that having live children was a risk factor for unintended pregnancies.26 32 36 41 49 Mirzamoradi et al and Pakdaman et al reported that gravity was a risk factor for unintended pregnancies.32 43
Discussion
Unintended pregnancy has substantial negative consequences on the health and well-being of the mother and children. The occurrence of unintended pregnancies can be attributed to several factors, including sociocultural, environmental and individual factors. Our systematic review and meta-analysis investigated the prevalence and the factors associated with unintended pregnancy in the MENA region. Our meta-analysis revealed that more than one-fourth, 27.0% of women, experienced an unintended pregnancy in their lifetime. The highest prevalence was estimated in Saudi Arabia (32.0%), while it was 27% in Egypt, 28.0% in Iran and 8.0% in Qatar. The prevalence of unintended pregnancy was highest among the studies published between 2006 and 2010 (34.0%).
While numerous systematic reviews estimated the prevalence of unintended pregnancy in other regions,51–53 to our best knowledge, no prior reviews specifically focused on the MENA region. Consequently, the findings of our comprehensive review carry significant implications for future decision-making, considering the sociocultural aspects specific to this region. Most of the studies included in our review have a low risk of bias, and a few studies have a moderate or high risk of bias.
A previous study on the global prevalence of unintended pregnancy revealed that 44.0% of pregnancies were unintended in 2010–2014.54 On the other hand, our review suggests that 27.0% of the pregnancies in the MENA region were unintended. Our findings are consistent with the study conducted in the Africa region. A systematic review and meta-analysis that included the studies conducted in Ethiopia estimated the prevalence of unintended pregnancy at 28%.51 Another systematic review of the studies conducted in Sub-Saharan Africa reported the mean unintended pregnancy rate at 33.9%.52 Nevertheless, our study revealed a higher prevalence of unintended pregnancies compared with other high-income countries, such as Britain, where a survey showed a 16.2% prevalence.55
In our review, Saudi Arabia had the highest unintended pregnancy with a prevalence of 32.0%, and Qatar had the lowest prevalence of unintended pregnancy at 8.0%. However, this finding is based on a single study in each country with several limitations that may have contributed to the vice-versa prevalence, including the study’s single-centre design and small sample size derived from convenience sampling. The variation in the prevalence among the countries might be attributed to sample and methodological differences in assessing pregnancy intention. Another potential reason for the variation in unintended pregnancy prevalence could be attributed to the individuals involved in the studies’ differing socioeconomic and cultural characteristics. For example, socioeconomic factors such as income level, education and employment status can significantly impact access to reproductive health services, including contraception. In some countries within the MENA region, women with lower income or education levels may face barriers to accessing modern contraceptives due to cost, limited availability or lack of information. Additionally, cultural differences, such as attitudes towards family planning, gender roles, and the influence of religious beliefs, can also play a critical role. In more conservative settings, there may be societal pressure to avoid discussing or using contraception, leading to higher rates of unintended pregnancy. These disparities in access to and acceptance of contraception across different countries and communities within the MENA region can contribute to the observed variation in unintended pregnancy prevalence.56–58
The prevalence of unintended pregnancy was the highest (34.0%) in the studies conducted in 2006–2010; however, it was close in studies conducted in 2001–2005 (30.0%) and 2011–2015 (26.0%); then, it declined to 20.0% in the studies conducted in 2016–2020. The findings from a previous study support this trend, such as the unintended pregnancy declined by 30% in developed regions, from 64 per 1000 women aged 15–44 in 1990–94 to 45 in 2010–14. In developing regions, unintended pregnancy fell by 16%, from 77 per 1000 women aged 15–44 to 65.54
Our review suggests that the pooled prevalence of unintended pregnancy was the same in the studies conducted in community settings (28.0%) and the studies conducted in hospital settings or healthcare facilities (27.0%). We must consider a few factors that may affect the generalisability of the results between these two settings. First, the community-based findings are based on only four studies. The two categories of studies involve different samples of women, surveyed at various times after pregnancy and delivery, using different methods to measure unintended pregnancy. Additionally, data collected in community settings relied on surveys, which may introduce recall bias in the assessment of unintended pregnancy.
Similarly, we did not observe significant differences in the prevalence of unintended pregnancies between studies employing probability sampling and those using non-probability sampling methods, although non-probability sampling studies tended to focus more on specific groups of women. Additionally, the inherent nature of non-probability sampling methods makes them susceptible to selection bias.
The pooled prevalence of unintended pregnancy was notably lower at 10.0% when assessed using the LUMP, compared with 29.0% using other methods. This discrepancy may be due to the LUMP’s validated approach, which evaluates pregnancy planning and intention through detailed questions on timing, desire and preconception actions, providing a more nuanced understanding of pregnancy intendedness.59 In contrast, simpler methods that rely on binary questions may overestimate unintended pregnancies by failing to capture the complexities of human intention and ambivalence, leading to a higher reported prevalence.
Unintended pregnancies can be attributed to several factors. Research conducted in the MENA region indicates that women with higher age tend to have a higher likelihood of experiencing unintended pregnancies.25–27 Similar results were observed in some other studies that indicated a lower occurrence of unintended pregnancies among younger women.51 55 This phenomenon can be attributed to the fact that younger women often plan their first pregnancies based on their preferences, but as they age, this tendency may reverse for subsequent pregnancies.
Additionally, the higher prevalence of unintended pregnancies among women with lower levels of education can be linked to their limited awareness of the potential consequences and their restricted knowledge about contraceptive methods.51 55 It stands to reason that higher education levels correspond to increased reproductive health awareness. Moreover, among spouses with higher education levels, there is typically improved communication about pregnancy, greater awareness of family planning and an increased likelihood of receiving adequate antenatal care.25 51 However, one study in the MENA region indicated that women with comparatively higher education levels were more prone to experiencing unintended pregnancies.43
A study conducted in Iran indicated an association between unintended pregnancy and parity, showing an increase in unintended pregnancies with higher numbers of previous pregnancies.26 This finding aligns with a similar study conducted in Egypt.60 Moreover, the reported higher prevalence of unintended pregnancies among women with a history of abortion or miscarriage can be attributed to the fact that many unintended pregnancies ultimately lead to such outcomes.25 55
Research implications
Our review found a high prevalence of unintended pregnancies in the MENA region that calls for a comprehensive intervention that not only encompasses public health policy and education but also urges potential practice changes in healthcare delivery. Healthcare systems should adapt to include more patient-centred care, emphasising empathetic counselling and support in reproductive health in the region. This may involve training healthcare providers to be sensitive to cultural and individual needs, integrating reproductive health services into primary care, and ensuring easy access to a variety of contraceptive methods. Community health initiatives should also break down cultural and societal barriers and promote open dialogue about reproductive health. The findings also suggest the need for broader research focusing on under-represented areas and factors. Implementing these practice changes, alongside policy reforms and educational efforts, is vital for effectively reducing the high prevalence of unintended pregnancies in the MENA region.
Strengths and limitations
We conducted a comprehensive systematic literature review following rigorous methods, searching the eligible articles from three major databases and the reference lists of eligible studies without language restrictions to minimise the potential for publication and selection bias. Two review authors independently completed the study selection, including title and abstract screening and full-text review.
Our review has several limitations. First, due to the heterogeneity among the studies, we could not synthesize pooled estimates for risk factors related to unintended pregnancy. This heterogeneity stemmed from several methodological differences, such as variations in how unintended pregnancy was measured, the timing of when women were asked about their pregnancy intentions (whether during pregnancy, immediately after delivery or later) and the different samples of women included in the studies (eg, postpartum women vs all pregnant women). Additionally, data collection in some settings relied on surveys, which may introduce recall bias. These differences may affect the comparability of the results and should be carefully considered when interpreting the meta-analysis findings. Moreover, our study identified relevant research from only four countries in the MENA region—Egypt, Iran, Saudi Arabia and Qatar—out of a region comprising 19 to 21 countries, depending on the definition. This limited geographical scope raises concerns about the generalisability of our findings to the entire MENA region. The countries included in our study may differ from those not included in terms of socioeconomic factors, cultural attitudes towards family planning, and access to reproductive healthcare. For instance, countries not represented in this study may have differing levels of access to contraception, variations in healthcare infrastructure or cultural and religious influences that could impact unintended pregnancy rates. Therefore, our results should be interpreted with caution, and there is a clear need for future studies focusing on a broader range of countries within the MENA region to provide a more comprehensive understanding of unintended pregnancy prevalence and its associated factors across diverse contexts.
Conclusions
In this systematic review, a high prevalence of unintended pregnancy was observed in the MENA region. The highest prevalence of unintended pregnancy was observed in Saudi Arabia. Despite a noted declining trend, the prevalence remains concerningly high. The findings underscore the urgent need for strategies focused on enhancing understanding and use of contraceptives and also emphasise the importance of culturally sensitive, patient-centred healthcare practices in the region. These strategies may include comprehensive sexual and reproductive health education, improved accessibility to a variety of contraceptive methods and training healthcare providers to offer empathetic, individualised counselling and support. There may also be a need for community engagement initiatives that address cultural and societal barriers, promoting open and effective communication between partners regarding pregnancy and family planning. Implementing these strategies would be crucial for effectively reducing the prevalence of unintended pregnancies in the MENA region.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Further details can be obtained from the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Footnotes
X @TChivese
Contributors NI, SM, and TC contributed to the conception and design of the study. NI, SM, UE, NA, MSI, and MJT performed the screening and data extraction. NI conducted the formal analyses. NI, SM, and HK contributed to the interpretation of the results. HK, SRC, SM and NI prepared the original draft. All authors participated in reviewing and editing. NI served as the guarantor for the study. The corresponding authors attest that all listed authors meet authorship criteria.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.