Article Text

Abstract
Objective Cardiovascular disease is the main cause of death worldwide. The leading risk factor, hypertension, is a major public health issue in Senegal, putting the health system under pressure. This qualitative study aimed to investigate how patients progress along the cascade of care of hypertension screening, diagnosis, treatment and control in Dakar, Senegal, in the context of the CARDIO4Cities initiative—a multisectoral urban population health initiative targeting cardiovascular risk factors in various cities globally.
Design and setting A qualitative case study in Dakar, Senegal, was conducted to map the cascade of hypertension care and identify enablers and barriers for patient progression across the cascade of care.
Participants and analysis Twelve semistructured interviews were conducted with community and healthcare actors in three districts of the city of Dakar. A systems thinking lens and method, called process mapping, was used to guide the qualitative research and the analysis of the results.
Results The process analysis delineated four themes as enablers of patient progression: improved management processes in primary care for hypertension; community outreach and engagement; data generation for healthcare provider monitoring of the hypertension cascade of care; and providing access to hypertension screening, monitoring and management tools. Barriers across the cascade were patients’ low socio-economic status; trivialisation and denial of the disease; systemic challenges in the health system, such as high healthcare provider turnover; traditional gender roles that influence access to healthcare; and inefficiencies of new tools hindering healthcare provider engagement and workflow integration.
Conclusions A wide range of patient, health system and contextual factors were identified as facilitating and hindering the progression of hypertension patients across the cascade of care in Dakar, Senegal. The structural determinants of health and systemic challenges in the health system were highlighted as prominent barriers, suggesting the need for upstream, system-oriented interventions for hypertension care in Dakar.
- Hypertension
- Health policy
- Health Equity
- Health Services Accessibility
- Protocols & guidelines
Data availability statement
Data are available upon reasonable request. Research materials included interview guides and tools are provided in the supplementary materials.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
Applied a systems thinking lens and methods to comprehensively assess the hypertension cascade of care in Dakar, Senegal, including health system, patient and contextual enablers and barriers to hypertension care.
A broad systems thinking lens offered opportunities to connect and pinpoint the influence of the structural determinants of health on the hypertension cascade of care.
Conducted interviews with a diverse range of community and healthcare actors, enhancing the richness of knowledge on hypertension in Dakar.
Lack of direct patient involvement, which limits the findings on patient-specific barriers and the effectiveness of community engagement efforts.
The study was confined to Dakar, which may limit the generalisability of the findings to other regions or contexts.
Introduction
Cardiovascular diseases (CVDs) are the leading cause of death worldwide, accounting for one-third of all deaths globally.1 2 The treatment and control rates of hypertension, a major contributor to cardiovascular morbidity and mortality, have improved in most countries since 1990; however, the same trend is not observed in sub-Saharan Africa (SSA).3 4 Nearly 90% of annual hypertension-related deaths occur in low- to middle-income countries (LMICs)4 and CVDs have replaced infectious diseases as the number 1 cause of mortality in many LMICs as categorised and identified in a worldwide analysis of trends from 1975 to 2015.5 By the year 2030, the burden of CVDs in SSA is expected to almost double in comparison to 2002 WHO estimates.6–9
Senegal is struggling with an increasing double burden of disease, yet non-communicable diseases (NCDs) have not been prioritised and adequately financed compared with communicable diseases. NCDs account for 45% of the overall mortality in Senegal, and the probability of premature death due to NCDs in Senegal is almost double that of high-income countries (20% vs 12% in 2016).10 Particularly, CVD is a major public health issue, but data on the prime risk factor—hypertension—have been sparse.11 Only recently have nationwide data on hypertension become available and indicative of its high prevalence12: almost a quarter (24.0%) of the 18–69-year-old population suffers from the condition, of whom only 13% were officially diagnosed.12 Among the patients aware of their hypertensive status, only 17% reported taking antihypertensive therapy, and hypertension control reached a mere 8% of all patients.13
A multisectoral urban population health initiative, CARDIO4Cities, aimed to address cardiovascular risk factors, such as hypertension, in three cities: Dakar, Senegal; São Paulo, Brazil; and Ulaanbaatar, Mongolia.14 The CARDIO4Cities initiative (or the Initiative herein) is centred around six fundamental pillars: quality of Care, early Access, policy Reform, Data and digital technology, Intersectoral collaboration and local Ownership.15–18 The Initiative was implemented in Dakar, Senegal, and monitored the cascade of care of screened, diagnosed, treated and controlled patients with hypertension.15 A quantitative analysis of the cascade of care for hypertension in Dakar, Senegal, is described elsewhere.15
CVDs result from an interplay of biological, social and systemic factors, wherein the social determinants of health are increasingly recognised to limit individual choices due to social, environmental, economic, political and cultural factors.19–21 To unpack this complexity, system thinking methodologies can be used to investigate the enabling and hindering factors along the cascade of care. System effectiveness is a systems thinking methodology that analyses interventions by qualifying and/or quantifying the effectiveness of an intervention in real-world health systems with a comprehensive systems lens, rather than with a narrow focus on a specific part of the system.22–24 A common application of system effectiveness in hypertension care is to assess the ‘cascade of care’, which is the sequential series of steps that individuals with a disease go through to receive appropriate diagnosis, treatment and management. This contrasts linear or vertical analyses that may not consider the system as a whole but focus on specific interventions or points across the care pathway. The cascade of care approach has been used since the 1980s for various diseases,25–27 including hypertension,28 29 to understand the continuum of care and identify the challenges for effective disease management. This study aimed to analyse the cascade of care for hypertension care in Dakar, Senegal, using a qualitative systems effectiveness methodology and identify health system, patient and contextual factors that enabled or hindered patient progression.
Methods
Conceptual framework
The cascade of care for hypertension30–33 describes the key milestones for a person at risk of hypertension to obtain care and control their condition through the health system. Reaching each of the milestones is influenced by individual patient factors, system components and contextual factors34 35 (figure 1). Individual factors pertain to patient-level characteristics, such as their demographics, behaviour, attitudes and personal experiences. System-level factors pertain to the health system, such as how hypertension care is delivered. Contextual factors pertain to broader social, cultural, economic and political phenomena and their impact on individuals or the system. Figure 1 describes the examples of each of these types of factors from the literature.30–33

Patient, health system and contextual factors along the cascade of care for hypertension patients. The figure also demarcates in brackets what type of factor is listed—patient, health system or contextual. CVD, cardiovascular disease.
Study setting
Senegal is a lower middle-income country with a population of 18 million,36 of whom more than 49% reside in urban areas.37–39 Dakar, the capital of Senegal, is among the largest cities in Africa, with significant population growth (3.11% annual change in 2022).40 41 By 2035, it is estimated that more than 60% of the Senegalese population will be living in urban areas.37 According to the last general population census in 2023,36 the city of Dakar was estimated at about 1.18 million inhabitants and the region of Dakar had 3 896 564 inhabitants on an area representing only 0.3% of the total surface of the country.36 40
Dakar is administratively divided into four districts. The health system operations and health programmes are implemented at the district level, with each district having at least one health centre and multiple health posts staffed by nurses or midwives aimed to be the first point of contact for the population.42 Tertiary facilities include hospital centres that provide specialised care. In addition to the public sector facilities, there are private clinics spread throughout the country.42 This study focused on the public health system, in which the CARDIO4Cities initiative was implemented at the time of study.
In 2018, the initiative started in Dakar with a focus on improving hypertension control43 in close collaboration with the Ministry of Health and Social Action, particularly the NCDs division (in French, Division de la lutte contre les maladies non-transmissibles).13 The initiative aimed at reducing the burden of hypertension by strengthening the provision of health services in an interdisciplinary way. In partnership with the local government, healthcare providers (HCPs), private sector actors, non-governmental organisations and other stakeholders, a comprehensive multisectoral action plan was developed that focused on health sector improvements, community engagement activities and digital solutions to improve hypertension and CVDs.18 44 Specifically, the NCDs Division of the MoH, the Direction on Private Health Facilities of the MoH, the Senegalese Society for Cardiology, the Chair of Cardiology at Cheikh Anta Diop University in Dakar, Health District cardiologists and general practitioners, the Research Centre for Human Development and the non-governmental organisations PATH and IntraHealth were involved. The list of interventions and activities per CARDIO4Cities pillar implemented in Dakar up to the date of data collection for the present study (March 2022) can be found in online supplemental file 1.
Supplemental material
Sampling strategy
Purposive sampling was used to recruit community health and other healthcare actors who have considerable experience in delivering hypertension care in Dakar. The interviewees had to have been engaged in the CARDIO4Cities initiative for the majority of its implementation (ie, approximately 2018–2022) and be a community health or healthcare actor working in a clinic in which the CARDIO4Cities initiative was active. Interviewees were selected to represent high- and low-performing facilities in three of the four Dakar city districts (North, Centre, West; omitting South due to logistical and feasibility challenges during the data collection period) and were contacted and confirmed through phone by local implementation partners. Twelve semistructured interviews were held with 4 healthcare managers (who were also physicians), 3 physicians (one being an assistant manager), 2 nurses and 3 managers of community health organisations or programmes. Seven of the interviewees were from health centres, two of the interviewees were from health posts and three interviewees were from community-based organisations.
Data collection
The interviews were conducted in person by two data collectors (first two authors; PhDs/research associates) at the interviewees’ place of employment (clinics and community-based organisations) in March 2022. Interviews were structured around two main objectives: (1) describing the hypertensive patient pathway and (2) identifying enabling and hindering factors at each step of the cascade of care, including exploring which patients may be most disadvantaged along the patient pathway through an equity lens. The interview guide was rigorously reviewed by all authors to ensure fit and feasibility. The interviews were held in French, conducted until saturation and took approximately 1 hour. Data saturation was considered reached when no new themes were emerging from the interviews and the same themes were continuously reinforced. French was used as it is the official language of Senegal. Informed consent was obtained verbally, and the interviews were audio-recorded and analysis sheets translated into English. The short time frame for data collection was suitable given the focused interview guide developed for a rapid qualitative research approach as further described below.
Data analysis
Rapid qualitative analysis, a proven and effective qualitative approach for generating timely and focused insights45 was applied. This method uses various approaches to streamline the process of qualitative research while maintaining rigour.45 This method was considered suitable for investigating the patient pathway and perceptions of influential factors.
Using this method, full transcription of audio-recorded interviews was omitted by preparing a clear framework for note-taking that directly fed into the analysis (rapid assessment process (RAP)46 47). An interview guide listed the consent process and the interview questions, and is included in online supplemental file 2 (English translation in online supplemental file 6). A RAP sheet is a working document to collect and analyse data in parallel and is included in online supplemental file 3 (English translation in online supplemental file 7). The RAP sheet was organised according to the cascade of care: screening, diagnosis, treatment and control (deductive codes). Secondary deductive codes were enablers and barriers of hypertension care for each step of the cascade. Two researchers listened to the audio interview recordings, coded the interviews and ensured accuracy and completeness of the RAP sheet. The completed RAP sheets were translated into English. Thereafter, both researchers conducted a thematic analysis by inductive coding of the interview notes in the RAP sheet. Inductive coding was used to generate themes within each step of the cascade of care and across the cascade of care. To facilitate the inductive analysis across the cascade of care, the data were organised according to the WHO health system building blocks framework.48 The two investigators jointly reviewed emerging findings following the independent analysis. Rigour and validity were established through independent coding, followed by discussions. A validation meeting (partial member checking) with local programme managers was held to obtain feedback on the preliminary findings of the interviews. The immediate results of the research were shared for supporting programmatic work and improvements of care in Dakar, and programmatic staff were included and consulted throughout all the stages of the research. Furthermore, the final paper was translated and shared with interviewees.
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Enablers were defined as the factors or elements of the patient, health system or context that enabled positive progress in hypertension care, that is, enabling a patient to progress along the patient pathway. Barriers were defined as the contrary—factors or elements that hindered progress in hypertension care. Both enablers and barriers were loosely categorised as system or step-specific; if categorised as systemic, this indicated they had an impact across the entire or majority of the cascade of care, and if categorised as step-specific, this indicated their impact was mostly concentrated at a specific step in the cascade.
The care cascade of hypertension patients during the CARDIO4Cities initiative was mapped based on the qualitative interviews. The Business Process Map (BPM) (using Bizagi software) was used to visualise and evaluate the detailed process of screening, diagnosis, treatment and control. BPM, also known as discrete event simulation, is a systems thinking tool used to find the system bottlenecks and discuss solutions to improve the performance of systems. This method helps capture the complexity of the systems at play in a simple diagram called a process map by visualising the main stakeholders, system processes and information flows from end-to-end. It provides insights into stakeholder relationships and system bottlenecks, inefficiencies and design flaws that limit system performance. BPM stems from the field of enterprise architecture,49 and details of application of this method to other systems can be found elsewhere.50 The software Bizagi Modeler was used to visualise the flow of activities and stakeholders involved throughout the system.
Author reflexivity statement
The first author is a white woman from outside of Dakar, Senegal, leading her to view the challenges described herein from an inherently outsider’s perspective. The second author is a Senegalese woman who led the interviews and collaborated intensively on the analysis. The first author is experienced in qualitative research methods complementing the expertise of locality and context of the second author. This ensured the analysis and results were socioculturally attuned. Further, the findings were reviewed and interrogated by all authors, some of whom are Senegalese colleagues.
Of relevance to the analytical lens applied, the first author’s epistemological perspective on health systems is that they are predominantly socially constructed, with context taking a vital explanatory role in health status and the determinants of health, which can be outside of an individual’s control.
Patient and public involvement
The research questions were developed in collaboration with local implementation partners; however, patients and the public were not consulted at this stage. The preliminary results of the research were summarised, circulated in plain language and presented to programmatic partners and governmental officials in Dakar, including a quasi ‘member checking’ effort. The final paper was translated and shared with interviewees. Future research studies should collaborate with patients and public directly.
Results
Hypertensive patient cascade of care
The key stakeholders identified in the process were the patient, community health worker (CHW), nurse, laboratory technician, medical doctor, pharmacist and data clerk from a non-governmental organisation. The full description of the patient pathway, stakeholders and process map can be found in the supplementary material (online supplemental file 4)
Supplemental material
Enablers and barriers for patient progression across the cascade of care
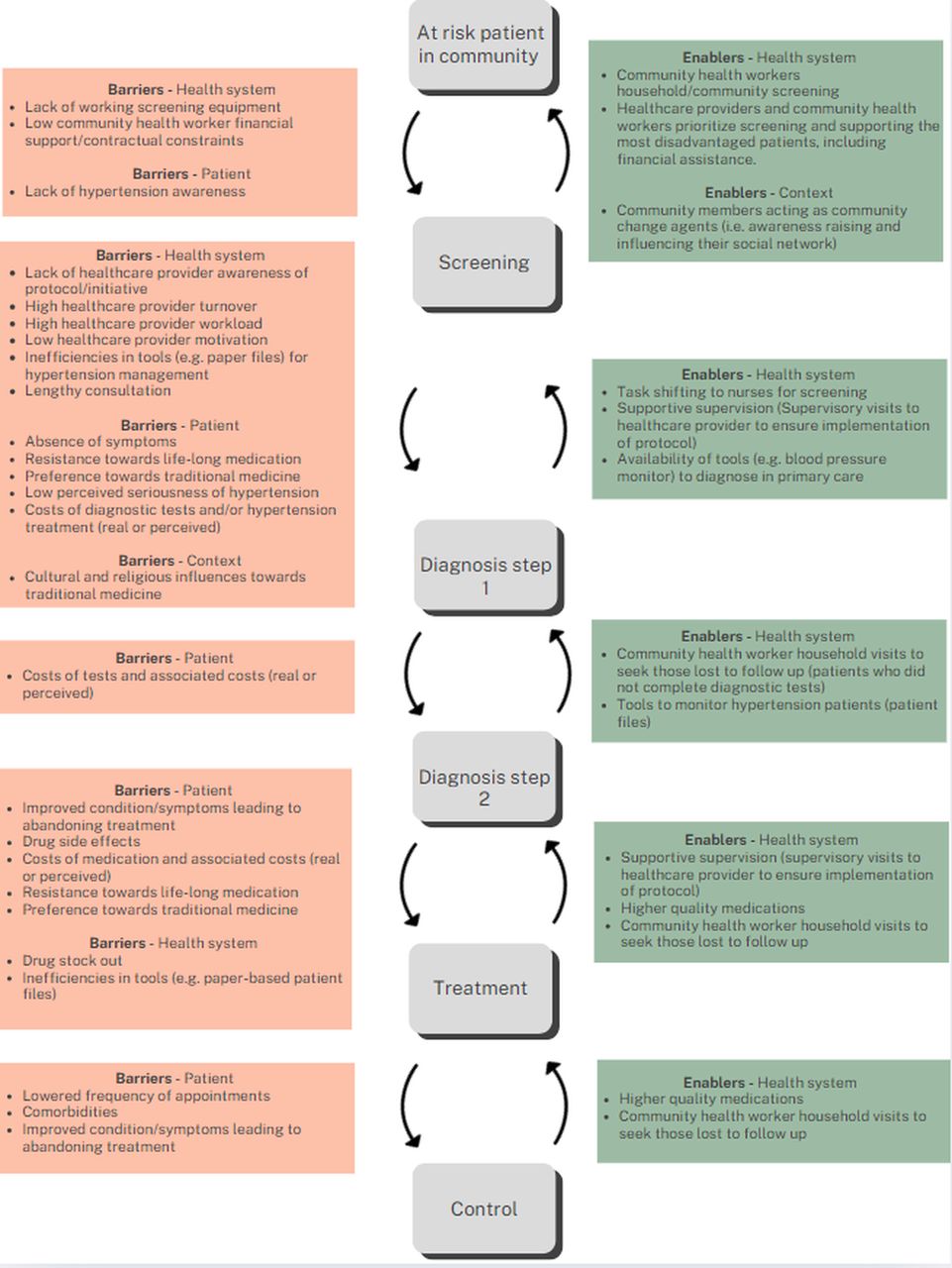
Health system, patient and contextual factors that enabled or hindered the progression of the patient across the cascade of care were identified (see figure 2). It was evident that the most important barrier for a patient were to progress from screening to step 1 of diagnosis. A second step in the diagnosis stage was added to the cascade due to the various sub-processes involved, which are visualised in a detailed process map diagram (French document which can be shared on request). The accompanying description of the process map is included in the supplementary material (online supplemental file 4).

{kind=link}
{kind=link}
Enablers and barriers across the hypertension cascade of care.
Enablers
The qualitative interviews included an investigation of how various factors influenced the cascade as well as what factors were related to the impact of the CARDIO4Cities initiative. Four themes emerged related to what was perceived to be most critical for improving the cascade of care across the course of the CARDIO4Cities initiative: (1) improved management processes in primary care for hypertension; (2) community outreach and engagement; (3) data generation for HCP monitoring of the hypertension cascade of care and (4) access to hypertension screening, monitoring and management tools and technologies.
Improved management processes in primary care for hypertension
It was echoed across all providers that the collaborative, interdisciplinary update and translation of the existing 2016 NCD National Guidelines into standard algorithms of care for hypertension at the primary health care (PHC) level was a key driver in improving the hypertension cascade of care. As part of the CARDIO4Cities initiative in 2017, the existing 2016 guidelines were adapted to the WHO package of essential non-communicable (PEN) disease interventions for primary healthcare, and extended management of hypertension to primary care, including to nurses and CHWs, which was not the case prior to CARDIO4Cities. Prior to this updated protocol, hypertension management had remained within the scope of tertiary care (ie, cardiologists in hospital settings) and some primary providers who took the initiative to do so. The protocol reorganised management to lower levels of care and addressed the fragmented approach to care implemented previously where everyone ‘worked on their own’:
Before the program, we did not have a specific path for the patient. The patients came from everywhere and then everyone took care of the arterial hypertension [at their] level … So we didn't have a care algorithm so everyone did what they could do on their own and that had a negative impact on the management of hypertension. (Original quotes in the language of interviewees and interviewers included in supplementary material.)
Therefore, the implementation of this protocol, which included task shifting to primary care (nurses, CHWs and primary care physicians), paired with supportive supervision visits to the clinics to improve protocol implementation, were all important features of improving governance and management of hypertension care.
Similarly, interdisciplinary collaboration by way of monthly collaborative meetings appeared to be effective in improving management of care. Monthly meetings were initiated by the CARDIO4Cities initiative for reviewing hypertension data, reflecting on progress and challenges and providing space for information exchange across different HCPs, non-government organisation actors (data collectors and programme managers) and occasionally government officials. Beyond the majority of interviewees who stated the effectiveness of these meetings, evidence of the success of these meetings was the consistency of enablers and barriers noted across the interviewees, which suggested strong dialogue across stakeholders in the health system.
Community outreach and engagement
Across all interviewees, expansion of hypertension care to the wider community (beyond health services) was a major driving force in improving care. A large component of the CARDIO4Cities initiative in Dakar centred around a CHW programme with mass screening and education events to address the lack of hypertension awareness, but also a lost-to-follow-up initiative. This community outreach was reiterated by interviewees as doing monumental work to address one of the main systemic barriers to care—namely, the very prominent culture of resistance to seeking hypertension care (elaborated on in the barriers section). Through community outreach, significantly more people were able to be ‘convinced’ of the importance of managing hypertension and were educated on mitigating risks and common misperceptions. Interviewees noted the evidence of changing mindsets around hypertension care in the community, such as patients seeking out screening regularly on their own or because their social contacts encouraged them to do so—where previously many in the community would pressure others not to seek hypertension care. The reasons for the community pressure towards not seeking care are elaborated in section 2.2 of barriers.
Thanks to the program… it allowed me to spend a lot of time with the patient. This allowed us to convince patients of the need to come regularly to appointments; in any case it fundamentally changed our approach.
Notably, the community initiative involved an informal community engagement mechanism wherein the CHW investigated the worries and barriers a patient was experiencing when lost-to-follow-up. This included many community members who had not yet been through the full diagnosis process (ie, only completing the first step of the two-step diagnosis process); an exploration of patient barriers at this early stage was viewed as an important enabler as many barriers existed before patients were diagnosed. This also created a channel to informally collect knowledge of patient barriers and feed them into the collaborative monthly meetings among providers, and therefore creating opportunities to address these concerns and direct them to programme managers and city authorities.
A related and noteworthy trend was the emergence of physicians as large proponents for community outreach and screening. Physicians saw the immense value of CHWs and screening, stating: “Screening saved lives” or « Le dépistage a sauvé des vies ». They were very cognisant of the financial and sociocultural barriers for patients, and therefore advocated for equity and prioritisation of support for the poorest patients, which the CHWs had the potential to reach.
Data generation for monitoring of the hypertension cascade of care
Data on hypertension were frequently seen as a driver for improving care through increasing knowledge among service providers, programme managers and city authorities on the extent of hypertension and challenges related to care. The CARDIO4Cities initiative in partnership with the government established data collection tools and indicators that constituted the basis for data collection throughout the programme. Interviewees stated they ‘now have the numbers’, signifying the value of data on a neglected issue. It was clear that data on hypertension were used by HCPs engaged in the collaborative monthly meetings.
Access to hypertension screening, monitoring and management tools and technologies
Access to tools and technologies to deliver hypertension care, which was introduced by the CARDIO4Cities initiative, was stressed as an important driver for the improvement of care across the patient pathway. Tools and technologies for providers to deliver care included patient files for monitoring, blood pressure measurement tools, scales and quality medications. Beyond access, the impact of tools and technologies on the psychology and motivation of providers also emerged as an enabler. Many interviewees alluded to the strong influence of tools and technologies to motivate providers to engage in hypertension patient management, and without getting access to the tools, HCPs were less likely to engage in the management of hypertension. Supportive supervision visits to the clinics to improve protocol implementation also assisted in the integration and use of the new tools and technologies.
Barriers
Five themes emerged related to what was perceived to have the most negative influence on the cascade of care across the course of the CARDIO4Cities initiative: (1) patient socio-economic status; (2) trivialisation and denial of hypertension due to sociocultural influences; (3) systemic challenges across the health system, such as high HCP turnover; (4) traditional gender roles influencing access to healthcare; and (5) integration of new interventions into routine system and HCP workflows.
Patient socio-economic status
A strong theme that emerged among the interviewees was the negative impact of the low socio-economic status of many patients, who also had the most need for hypertension care. Medical, indirect and opportunity costs were all mentioned as barriers for many patients; for example, costs of diagnostic laboratory tests, transportation and time away from their job. An interviewee described the challenges: “There is no shortage of difficulties and we often encounter them during diagnosis, analyses, etc. Often we have patients with a very low social level [socio-economic level]. Examinations may be delayed due to patients' purchasing power.” Further, even if patients were able to pay for the first diagnostic steps, some patients took longer to complete the necessary diagnostic exams which then exceeded the recommended time of the diagnosis protocol, or otherwise some patients did not see the value in being diagnosed since they would not have the financial means to support themselves in future steps of care. In some clinics, patients were able to get financial support from the clinic or government funding schemes; however, there was a lack of awareness of these financial supports. Hence, real and perceived costs were a significant barrier for patients.
Trivialisation and denial of hypertension
Another prominent barrier was the tendency to trivialise or deny a diagnosis of hypertension, as well as a reluctance to take hypertension medication. One interviewee said: “The challenge is to be closer to the community and to raise awareness about high blood pressure because it is something that people have trivialised.” Many patients did not want to accept that they have hypertension and have to medicate themselves, and therefore may abort diagnosis or treatment and rather seek traditional medicine. This was seen as a significant challenge, but was improved through community engagement efforts as part of CARDIO4Cities. Nonetheless, challenges persisted and interviewees shared that this trivialisation and denial was related to cultural and religious influences that encourage traditional medicine purported to cure hypertension by prominent community figures. This led to the reluctance to take hypertension medication which was commonly seen as non-curative and to be taken for the remainder of one’s life: “It’s just the brainwashing that’s the problem – they're told you're going to be on medication for life. The brainwashing comes from the community saying don't take this or don't do that, don't take that because the organism will never adapt. What awareness needs to start at the community level … Now there is the marabout who can tell you that he can cure diabetes and hypertension, hepatitis.”
Systemic health system challenges
Broader health system challenges (ie, those that are systemic and not unique to hypertension care) were frequently noted barriers in the hypertension cascade of care; the key systemic health system challenges were lack of support for CHW, high HCP turnover and overburdened HCPs with limited time or motivation to engage in additional demands, such as hypertension care. Pertaining to CHWs, they felt they were not adequately supported in the health system since they worked on short-term, project-based and inconsistent contracts without significant financial compensation. Although their high value to hypertension care was echoed among physicians and various providers, interviewees alluded to the need for further support (eg, financial) for CHWs to boost their morale. Despite CHWs being formally integrated into health system structures since 2015, such as the creation of the Community Health Unit within the Ministry of Health and Social Action and the establishment of a service package for CHWs, there were barriers for them to consistently provide high-quality care.
A recurrent barrier was the high HCP turnover which resulted in HCPs not always being aware of the protocol for hypertension and therefore patients not being enrolled in the hypertension care pathway. The need to institutionalise more regular trainings on the new hypertension protocol was suggested to assist with filling this gap. Further, with the HCPs being overburdened with demands on their time, providers did not always engage in the lengthy consultation and treatment approach for hypertension, which required significant time and convincing of patients.
Traditional gender roles influencing access to healthcare
Interviewees all agreed that women made up the vast majority of hypertension patients; however, the reasons were uncertain to interviewees. Most interviewees assumed that women on the one hand had more contact with and time to visit health centres as a result of the health system being more developed to respond to maternal and child health issues. However, on the other hand, they may have stronger risk factors due to living a more sedentary lifestyle than men. In Senegal, women traditionally assume the domestic responsibilities while men are viewed as the primary breadwinners, although these roles are evolving. Therefore, the interviewees theorised that men had less time to visit health centres due to their employment responsibilities and were thought to be less concerned with health issues than women in general, alluding to gender norms and traditional views of masculinity. Therefore, it was apparent that gender and gender roles may play a role in access to hypertension care and possible risk of hypertension.
Inefficiencies of new tools hindering HCP engagement and workflow integration
HCPs stressed that inefficiencies and lack of integration of specific tasks and tools for hypertension presented obstacles to engage in hypertension care. Specifically, the patient files for hypertension monitoring existed in parallel to the routine patient files. Locating the paper-based hypertension patient file could take a significant amount of time due to the volume of files and the lack of organisation (eg, lack of numerical filing). On top of a lengthy consultation and busy workload for HCPs, these inefficiencies of tools affected HCPs motivation to engage in hypertension care; if there were less HCPs motivated to engage in hypertension management, it seemed likely to lead to less patients being enrolled in hypertension care overall. Further, there was a lack of recurrent training for HCPs on the hypertension protocol and therefore a lack of HCP awareness of the hypertension protocol, which demonstrated a lack of integration of HCP training into routine training for providers.
All the original quotes in French are provided in online supplemental file 5.
Supplemental material
Discussion
Through process mapping and qualitative interviews, our study describes the structure, processes and factors influencing the hypertension cascade of care in Dakar’s public health system. The factors that improved the system’s performance and the progression of a hypertension patient across the cascade of care entailed improved management processes in primary care for hypertension through the development of a hypertension protocol, task shifting and interdisciplinary collaboration; community outreach and engagement; data generation for HCP monitoring of the hypertension cascade of care; and access to hypertension screening, monitoring and management tools and technologies, which were lacking prior to the CARDIO4Cities initiative. On the contrary, the barriers for hypertension patients to progress across the continuum of care were patient socio-economic status; trivialisation and denial of hypertension due to sociocultural influences; systemic challenges across the health system, such as high HCP turnover; traditional gender roles influencing access to healthcare; and inefficiencies of new tools hindering HCP engagement and workflow integration.
Many of the barriers to hypertension care identified in the study are consistent with those in the literature, such as lack of awareness of hypertension.30 Evidence from the 2015 STEPS survey in Dakar showed similar trends of low awareness, with more than half (54%) of the patients being unaware of their hypertensive condition.13 Our qualitative research echoes that awareness is a challenge in Dakar, but that the Initiative has addressed this topic with community outreach and engagement efforts. Nonetheless, our research has illuminated continuous barriers at the screening and diagnosis stages, such as financial issues. Without addressing the economic barriers to care, the value and impact of community outreach and education are greatly hindered as patients are unable to act on the new awareness and medical advice due to the various structural barriers they face.
The present study found that one of the largest challenges to effective hypertension care was the trivialisation of hypertension among the community due to sociocultural factors, which concurs with existing literature on hypertension barriers in Dakar and West Africa.51–53 For example, in Ghana, it was found that the reasons for bypassing public health facilities and accessing care from alternative providers were the inaccessibility and poor perceptions of the former compared with higher trust, proximity and relationships with the latter.54 Understanding patients’ health-seeking behaviour, priorities, motivations and preferences is key to designing effective interventions, and the integration of traditional medicines into the health system can leverage the potential of this sector to achieve Universal Health Coverage.55 56 These contextual barriers around the sociocultural values, which was a resounding barrier across the interviewees, are a form of structural determinant of health,57 58 like that of socio-economic position.
The results demonstrated that there was an economic burden for many patients to access care and manage their hypertension. The reasons mentioned were direct medical costs, such as the cost of the diagnostic procedures and medication, and indirect costs, such as transport to health facilities. However, implementation challenges for the new financial protection initiatives for higher-risk patients were noted, including a lack of awareness among patients and providers of the scheme. As hypertension requires lifelong medical care, it can cause large economic burden and lead to catastrophic health expenditures over time.59 Financial protection should cover the costs of chronic diseases-related expenses in the most deprived households. Furthermore, future research on the main cost barriers for patients and potential policies and programmes to address this in Dakar would be informative.
Although HCPs were abundantly aware of the financial challenges for patients, they were less aware of how gender influenced the hypertension care cascade. Our results suggest that women make up the majority of hypertensive patients; however, the reasons for this are unclear. A recent systematic review found that awareness and treatment rates were higher among women than men, but this advantage was not often translated into higher control rates among women.30 The literature suggests that the increased awareness among women may reflect more frequent interaction with health facilities, likely due to maternal and child health services, as well as the norms around masculinity that discourage men from seeking care.60–62 Decreased control rates might be a result of higher rates of obesity in women63 and potential differences in prescribing behaviours of HCPs.30 A number of these hypotheses explaining the gender differences that emerged through our interviews, including the potential of gender norms creating barriers for men to seek care and influencing women’s lifestyles, which were said to be potentially more sedentary. It is apparent that gender operates in complex mechanisms and therefore gender differences need to be investigated in future research and accounted for in future action to identify appropriate solutions to address gender equity gaps for hypertension care.
For public health initiatives to be sustainable, they must be locally owned and well integrated into routine practice64; both being goals of the CARDIO4Cities approach. The informal community engagement mechanism that emerged as part of the Initiative is a noteworthy example of local ownership of the programme. Given the CHWs’ close ties with the community, the interdisciplinary monthly meetings in the programme acted as a channel for patient voices to be heard. Although further research is needed on the actions and impact of this mechanism, it appears to be a promising and possible example of an investment into what is referred to as a ‘learning health system’65: a health system that has the ability to create, gather and use relevant knowledge to bring improvements in performance, such as through data-driven decision support and community feedback. Although these ‘softer’ elements of health systems improve sustainability and can become self-perpetuating, they are often overlooked and neglected.65 The importance of community voice and engagement was a resounding theme across interviewees and should be harnessed and capitalised.
Overall, the primary barriers identified were rooted in the ‘structural determinants’ of health. Drawing from Marmot and Bell’s seminal conceptual framework for action on the social determinants of health,66 structural determinants of health encompass the socio-economic and political context, including governance structures, cultural and social norms, public policies and individuals' socio-economic status such as social class, gender, race, education, occupation and income.57 66 67 The intermediary determinants of social determinants of health include people’s material circumstances, such as living conditions and food security, alongside behavioural and biological factors, and the healthcare system itself.57 67 68 Our study findings underscore that community and HCPs recognise the notable impact of various CARDIO4Cities interventions in addressing some upstream structural determinants of health; however, the results also highlight that entrenched structural barriers persist as key obstacles to advancing hypertension care locally. The study points to low socio-economic status, traditional gender norms, sociocultural values that trivialise hypertension and limited implementation of public policies aimed at financial protection. Furthermore, within the health system, barriers were largely systemic in nature, such as the lack of integration of CHWs into formal systems, high turnover rates among HCP and overburdened HCPs with limited time or motivation to engage in additional demands, such as hypertension care. These barriers demand system-level interventions in the health system and action towards the structural determinants of health. While historical approaches to NCDs have predominantly focused on individual-level interventions, it is evident that such efforts can only yield limited success when individual choices are constrained by societal, governmental and organisational factors.58 Therefore, an increasing emphasis on the structural determinants of health and systemic interventions at the health system level is suggested in future research and action to effectively alleviate the burden of hypertension.
The limitations of this research are the lack of patient involvement, which limits the findings on the effectiveness of community engagement and the patient barriers. Providers and CHWs provided their perceptions of patient barriers, but direct patient perspectives should be further explored. In line with systems thinking, future studies should also explore other interdisciplinary perspectives, such as social services or governmental actors who would be involved in addressing the barriers described herein. To ensure validity and rigorousness of the findings, the data were coded and analysed independently by two researchers. Further, the preliminary results were presented and validated with two local contacts. Lastly, there is potential for acquiescence bias (the tendency to lean towards positive responses rather than negative ones), despite the interviewers being external to the programme funding body. These power differences were managed by clarifying that all responses remain anonymous and do not impact interviewee involvement in CARDIO4Cities activities.
In conclusion, this qualitative study sheds light on the interplay of health system, patient and contextual factors in influencing the trajectory of hypertensive patients in Dakar, Senegal. It underscores the pivotal necessity for building systems that enable patients to manage their hypertension effectively. The research highlights systemic features of the health system and structural determinants of health, including socio-economic status and sociocultural factors, as significant barriers in the continuum of hypertensive care in Dakar, pinpointing stages where these factors exert influence. These findings provide valuable insights for future research, policy formulation and targeted interventions in Dakar. The study also advocates for the consideration of the structural determinants of health into the design and implementation of hypertension interventions, such as through comprehensive systems thinking approaches.
Data availability statement
Data are available upon reasonable request. Research materials included interview guides and tools are provided in the supplementary materials.
Ethics statements
Patient consent for publication
Ethics approval
All interviewees gave verbal informed consent. Verbal consent was chosen as opposed to written consent given the interviewees were selected and interviews facilitated by the local non-governmental organisation with existing trusting relationships with the clinics and community organisations involved in the Initiative in Dakar. No financial incentives were used. Ethical approval to conduct the study was provided within the framework of the Initiative’s ethical approval, given by the Comité National d’Ethique pour la Recherche en Santé (Protocol SEN19/14).
Acknowledgments
We would like to thank and acknowledge the support of the CARDIO4Cities Dakar team, including IntraHealth, the Novartis Foundation and the Ministry of Health (Division de la Lutte contre les Maladies non transmissibles, Ministère de la Santé et de l'Action Sociale) for their efforts and commitments to this research. We are very grateful to the numerous interviewees who shared their experiences to advance this research.
References
Footnotes
X @annamsocha
Contributors DCM and AS conceptualised the study and developed the methodology, with collaboration and input from representatives across all organisations in the collaboration (JB, KS, PS, JB, SB, MJ). DCM provided project administration and research supervision. AS and ST undertook coding and analysis. AS wrote the original draft of the manuscript. All authors contributed to manuscript review and editing and approved the final manuscript. DCM is the guarantor of the publication.
Funding The CARDIO4Cities initiative is funded by the Novartis Foundation.
Competing interests This publication and the CARDIO4Cities initiative are funded by the non-profit organisation Novartis Foundation. JB, TR and SDR were employed by the Novartis Foundation at the time of the research study. AS, PS, FS and DCM were employed by the Swiss Tropical and Public Health Institute at the time of the research, which receives funding from the Novartis Foundation. JB, SB and MJ were employed by IntraHealth, which also receives funding from the Novartis Foundation. All other authors have no competing interests to declare. These relationships have been disclosed, and all efforts were made to ensure the research was conducted objectively and independently of the funding organisation.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.