Article Text

Abstract
Objectives To explore husbands’ views on breast cancer screening, risk-based screening and their role in influencing their wives’ health-seeking behaviours.
Design Qualitative focus group discussion (FGD) supplemented by quantitative data from a cohort study using a structured questionnaire.
Setting This study was conducted in a community-based setting, with participants recruited online through non-profit organisations via social media and email.
Participants Nineteen husbands of women without breast cancer history participated. The questionnaire data were completed by 3395 women with no breast cancer history.
Interventions Not applicable.
Primary and secondary outcome measures Not applicable.
Results Six key themes emerged from FGDs regarding husbands’ attitudes towards women’s breast cancer screening practices: awareness, priorities, social support structures, fears, incentives and attitudes towards risk-based screening. These themes were supported by the questionnaire data, which also identified additional concerns not raised in FGDs, suggesting a gap in the husband’s awareness and limited health-related communication between spouses. While husbands expressed interest in their wives’ health and provided support in making screening appointments, their influence may be limited by these communication gaps. Most husbands were receptive to risk-based screening but raised concerns around the testing frequency and result interpretation.
Conclusions This study highlights the need to actively engage husbands in breast cancer screening discussions and develop support strategies that enhance their involvement. Strengthening spousal communication on breast health may increase screening uptake among women.
- Mass Screening
- Risk Factors
- ONCOLOGY
- Primary Prevention
- Percieved Social Support
- Breast tumours
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This qualitative study provides in-depth insights into husbands’ perceptions of breast cancer screening, but it cannot establish causal relationships between spousal support and screening attendance.
The cross-sectional nature of the study captures existing behaviours and attitudes without follow-up assessments to examine changes over time.
Most participants’ wives had not yet undergone mammography screening, thus limiting generalisability to routine screeners.
Recruitment through online platforms may have introduced selection bias, potentially favouring participants who are more engaged with health-related discussions.
Focus group discussions were conducted online, which may have influenced participant dynamics compared with in-person settings.
Introduction
Mammography screening attendance varies due to factors such as individual choice, service accessibility and societal influences.1 2 Women who attend screenings generally have higher social support levels.3–6 Marital status is linked to preventive healthcare behaviours and emotional support.7 A cohort study of 1 733 906 cancer patients found that being married was associated with increased survival, partly due to early breast cancer diagnosis.8 Spousal encouragement has been shown to motivate mammography screening participation, with spouses significantly influencing each other’s behaviours.9–11 Women without a partner tend to have the lowest screening attendance rates.12
In collectivistic Asian cultures, family decisions, including health behaviours, are often made collectively. Studies in Malaysia and Saudi Arabia found that spousal and family support predicted breast cancer screening uptake.13 14 An intervention in married couples showed women were twice as likely to undergo mammograms after increasing spousal support.15
Although positive spousal relationships are linked to higher mammography uptake, the specific mechanisms of spousal influence on screening attendance remain unexplored. This includes emotional, informational and practical support. Understanding the impact of spousal support is essential for designing effective interventions to improve screening rates, especially in Singapore, where the marriage rate is high, with 61.8% of those aged 15 and above married as of July 2022.16 Singapore’s 2021 marriage rate of 6.5 per 1000 exceeds that of the USA (6.0), EU countries (3.9) and several developed Asian countries.17–23
Singapore has adopted a family health unit approach, with initiatives like the ‘Korang OK?’ campaign by the Health Promotion Board (HPB) promoting healthier lifestyles for families and couples. The campaign offers resources on eating, mental well-being, health screenings and physical activities.24 Emphasising family and collective well-being, central to Singapore’s culture, these programmes can be leveraged to support breast cancer screening, particularly in delivering new risk and prevention approaches to communities.
Currently, most countries still follow an age-based model for breast cancer screening.25 However, as our understanding of risk factors grows, some are exploring risk-based approaches.26–29 For example, the BREAst screening Tailored for Her (BREATHE) pilot study in Singapore uses both genetic and non-genetic tools to customise screening based on individual risk profiles.30 Educating spouses can help to familiarise the public with this personalised approach.
This study explores views on breast cancer screening, the role of husbands in health-seeking behaviour and how spousal support may boost mammography rates in Singapore, especially for a new risk-based approach. We examined reasons for screening attendance from the BREATHE study and conducted focus group discussions (FGDs) with husbands to understand their perspectives on screening, their role in supporting attendance and their concerns about risk-based screening.
Methods and analysis
Overview of study design: questionnaire and focus group discussions
This study used information from two sources: (1) a structured questionnaire from the BREATHE cohort study,30 and (2) FGD. The BREATHE cohort was used to gain an understanding of the barriers and motivators to breast cancer screening in women with no history of breast cancer. The study provided an overview of women’s current perceptions of mammography screening and revealed their general sentiments. On the other hand, the FGDs with husbands (n=19) of women with no history of breast cancer delved deeper into the reasons behind these perceptions and yielded valuable suggestions for improvement. The main objective is to explore the attitudes of husbands of women with no history of breast cancer towards conventional mammography screening and their acceptance of the novel risk-based approach. The findings from both the Questionnaire and FGDs were mapped onto the COM-B model,31 which characterises behaviour as part of a system involving interactions between these three components: ‘Capability’, ‘Opportunity’ and ‘Motivation’. Each component can be further broken down as follows: ‘Physical Capability’, ‘Psychological Capability’, ‘Physical Opportunity’, ‘Social Opportunity’, ‘Reflective Motivation’ and ‘Autonomic Motivation’.
Questionnaire responses from women of the risk-based breast cancer screening study
Data on the questionnaire done at the point of recruitment were obtained from the BREATHE study. In brief, recruitment for BREATHE started in October 2021 at two restructured hospitals (Ng Teng Fong General Hospital and National University Hospital) and two polyclinics (Bukit Batok Polyclinic and Choa Chu Kang Polyclinic).30 The BREATHE study was publicised through community outreach. Although the participants were recruited from healthcare settings, the recruitment was not limited to those actively seeking healthcare services. As of 8 May 2023, 3395 women with no history of breast cancer aged 35–59 were enrolled.
This study focused on the questions about mammography screening attendance. Participants were asked to indicate their reasons for attending and not attending mammography screening. The options are presented in online supplemental table S1. Answers from ‘Others’ (free text) for both questions were sorted, and similar comments were grouped together. Of the 3395 women recruited in BREATHE, 3369 responded to the questions of interest.
Supplemental material
The reasons behind mammography screening attendance were fitted into COM-B constructs (‘Capability’, ‘Opportunity’ and ‘Motivation’) by two independent coders (JJKL and KAK) and categorised into core themes by grouping related options that cover similar topics.31 The total number of participants for each theme was aggregated to identify the most influential factors associated with mammography screening attendance.
FGDs with husbands of women with no history of breast cancer
Participant sampling and recruitment
This investigation is part of a larger study that examines the attitudes of various stakeholders towards mammography screening.32 The study included participants who were 21 years old or older and had access to the Internet. The recruitment process involved the dissemination of flyers through non-profit organisations via social media platforms and email. On signing up, participants provided their verbal consent in a one-to-one online session and were given a comprehensive briefing on the study. By 10 May 2023, the main study had received registrations from 460 individuals. Out of these, 166 participants provided verbal informed consent, while 294 did not respond to our email regarding informed consent. Among the 166 consenting participants, 35 were husbands of women with no history of breast cancer. Out of the 35, 19 participants actively participated in one of the four scheduled FGDs, while 16 participants were unable to attend any of the sessions. Once data saturation was achieved, the decision was made not to proceed with any additional FGDs.33
FGD facilitation
The online FGDs were designed using the consolidated criteria for reporting qualitative research (COREQ) checklist.33 A FGD discussion guide was developed by the research team, consisting of experts in breast cancer, epidemiology, public health and psychology. This diverse group of researchers and clinicians combines extensive expertise in breast cancer risk assessment and devising approaches to enhance participation in breast cancer screening. The sessions started by exploring the husbands’ perceptions regarding the barriers and motivators associated with their wives’ mammography screening attendance. Subsequently, the conversation was steered towards eliciting views on personalised breast cancer risk assessment and its potential impact on their wives’ screening behaviours. Online supplemental table S2 presents a selection of the questions used as a guide. The primary topics addressed in the discussions included the following:
Experiences, knowledge and attitudes on breast cancer and mammography screening.
Potential role of husbands in their wives’ health-seeking behaviour.
Opinions towards risk-based screening.
Four to seven participants were randomly assigned to one of the four FGDs carried out between April 2022 and July 2022 to optimise group dynamics and encourage productive discussions.34 Each FGD was facilitated by two members of the research team, lasting between 60 and 90 min. The main facilitator, a 26-year-old Chinese male (BA), specialising in Psychology and Communication, led the sessions using the same FGD guide. A 24-year-old Chinese female (BSc) with expertise in Public Health and Life Sciences served as a backup facilitator. No prior relationship existed between the facilitators and the research participants. All FGDs were conducted in English. Each participant received SGD20 e-vouchers at the end of the sessions.
Coding and thematic analysis
The FGDs were transcribed verbatim from video and audio recordings. The data were analysed through a five-step process:
Step 1: familiarisation of data. Researchers (JJKL and FG) immersed themselves in the data and recorded their impressions by reviewing transcripts and listening to all audio recordings.
Step 2: development of codebook. The COM-B framework was applied deductively as overarching codes to serve as a structure for categorisation of data and to help answer the research question on facilitators and barriers to breast cancer screening.31 Researchers (JJKL and FG) inductively created subcodes within each overarching COM-B code based on their impressions of the data and added definitions to all codes and subcodes according to the context of the research question and data (online supplemental table S3). The themes and subthemes were further refined through continued discussions within the coding team and members of the broader research team until consensus on the initial codes and their distinctive descriptions within the codebook was reached. This codebook served as a backbone for coding all transcripts in the QSR Nvivo software package (V.20.7.2, QSR International).
Step 3: piloting codebook. Three independent coders (JJKL, FG and KAK) coded the first two transcripts by categorising participants’ responses to the relevant COM-B codes and subcodes (online supplemental table S3). The coders met to discuss their codes and continued to revise the meaning of all codes and refine the codebook. A fourth researcher (KM) was invited to resolve any unresolved discussions.
Step 4: final coding process. The finalised codebook was used to code the remaining two transcripts by the same independent coders (JJKL, FG and KAK) and all codes were discussed and resolved.
Step 5: thematic analysis. Researchers (JJKL, FG and KAK) individually read through the transcripts coded in each code and grouped the codes based on their similarity. The themes and subthemes were developed iteratively, compared and nominated through collaborative discussion of links between codes among the coding team and the broader research team to encapsulate diverse perspectives. The COM-B constructs from the codes were eventually mapped against the emergent themes.
Patient and public involvement
For this study, patients and the public were not involved in the research process. The research questions, design and outcome measures were developed by the research team, guided by the BREATHE data, but without direct input from participants or community groups.
Results
Women’s attitudes towards mammography screening: results from questionnaire
A total of 3395 BREATHE participants were included in this analysis. The majority of the BREATHE questionnaire respondents were Chinese (n=2626, 77%), followed by Malay (n=369, 11%), Indian (n=228, 7%) and Others (n=172, 5%) (table 1). The median age at recruitment was 48 years (IQR: 43 to 53).
Characteristics of BREATHE participants (women without personal history of breast cancer, n=3395)
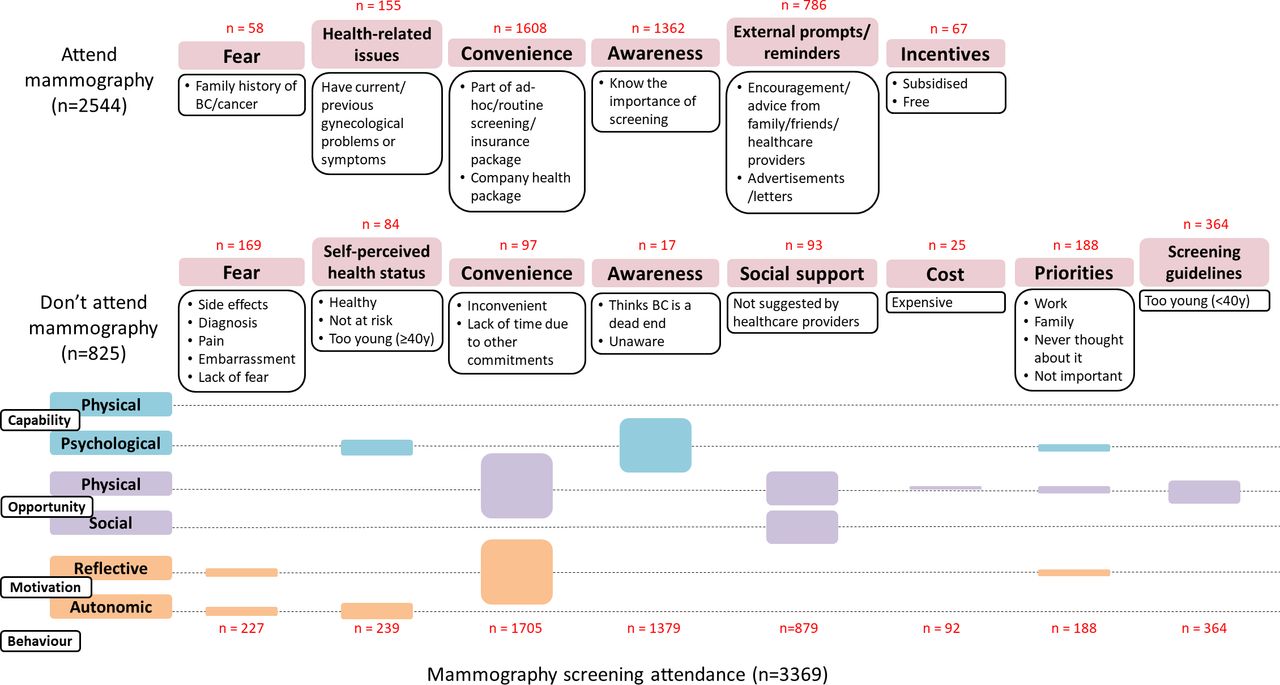
Among the 3369 participants who responded to the question regarding their previous mammography screening experience, 75% (n=2544) reported ever attending mammography screening, while 24% (n=825) indicated otherwise (table 1). The thematic analysis revealed key themes for both groups which are outlined in figure 1. Among those who attended mammography screening, the key themes identified were as follows: fear (2%), health-related issues (6%), convenience (63%), awareness (54%), external prompts/reminders (31%) and incentives (3%). On the other hand, for those who did not attend mammography screening, the key themes identified were as follows: fear (20%), self-perceived health status (10%), convenience (12%), awareness (2%), social support (11%), cost (3%), priorities (23%) and screening guidelines (44%).

Key themes derived from 3369 BREATHE questionnaire responses mapped to the COM-B model. n, total number of individuals within each theme. BREATHE, BREAst screening Tailored for Her; COM-B, ‘Capability’, ‘Opportunity’, ‘Motivation’ - ‘Behaviour’.
FGDs with husbands of women with no history of breast cancer
The 19 male participants had a median age of 41 years (IQR: 35.5 to 51.5) (table 2). The difference in age between the youngest and oldest participants in each FGD ranged from 2 to 42 years.
Characteristics of focus group discussion participants
Husbands’ attitudes towards breast cancer screening
Our analysis revealed six key themes on husbands’ attitudes towards breast cancer screening: awareness of breast health, priorities, social support structures, fears, incentives and attitudes towards risk-based screening. The themes and subthemes are explained below with supporting quotes from the participants and are summarised in figure 2. Online supplemental table S4 provides the thematic analysis table with an extensive list of supporting quotes.

{kind=link}
{kind=link}
Key themes derived from the husbands’ focus group study mapped to the COM-B model. COM-B, ‘Capability’, ‘Opportunity’, ‘Motivation’ - ‘Behaviour’.
Mixed awareness of breast health
Husbands reported mixed understanding of breast cancer and breast cancer screening processes. The theme ‘awareness of breast health’ was mapped onto the psychological capability and social opportunity COM-B constructs.
Some husbands demonstrated an accurate awareness that breast and colorectal cancers are the top two most common cancers affecting women in Singapore, while others identified cervical and breast cancers. Most husbands described lifestyle risk factors associated with breast cancer, and some identified that genetics could play a role in increased risk of breast cancer. Many estimated a Singaporean woman’s risk of developing breast cancer to be at 5%–10% which is similar to current risk levels.
Awareness of mammography screening experiences was relatively poor. Some husbands were aware that their wives experienced pain and discomfort during mammography screening, while others were unaware of the specific procedures involved in breast cancer screening and their wives’ experiences. Husbands were often unsure of certain aspects of mammography such as the cost of screening and the waiting time for appointments. Overall, a lack of awareness could limit the extent to which husbands could discuss breast health issues and procedures with their wives.
M14: I’m not too sure, what is the cost of one mammogram? Costs might be a barrier but I am not very sure.
Priorities
Husbands recognised that breast cancer screening was often underprioritised by some women. This was mostly attributed to the perceived inconvenience of attending mammography screening and the age recommendations from the national screening guidelines. The theme ‘priorities’ was mapped onto the physical opportunity and reflective motivation COM-B constructs.
Husbands recognised that it was challenging for both women and their spouses to make time for mammography-related arrangements and that they likely ‘put it off’ over other activities’. Husbands felt that this could be improved if the entire screening process could be streamlined and expedited. Integrating breast screening with other routine health check-ups, and text message prompts with clear information and appointment booking aids to remind women when they are due for screening were also identified as possible strategies to make screening more convenient.
M19: I think, Singapore, the work life balance is a bit… Because both couples are working to find a time and all that so finding special time for appointments and all this is a bit challenging at times so that’s why some people just put it off, and more emphasis is placed on family than oneself.
M1: I guess you can make it like something routine. So maybe when ladies go to polyclinics then based on the records, the doctor can just see if the screening was done recently, if not, then maybe they can just do the screening as part of the consultation.
Some husbands assumed that breast cancer screening would only be of concern when their wives hit 40 years old due to the current screening guidelines.
M17: Because I assumed the national guidelines pre-40 is not to screen.
M19: same for me, I don't see it (regular mammography screening) as important, as of now yeah.
M18: probably in one or two years time I'll go check up on that (regular mammography screening) yea, once she hits 40 which is in two weeks time.
Social support structures
This theme covered the effects of interpersonal relationships and community engagement on breast cancer awareness and mammography screening attendance. The theme ‘social support structures’ was mapped onto the social opportunity, physical opportunity and reflective motivation COM-B constructs.
Husbands generally expressed willingness to play a role in their wives’ health, as evidenced by their support during pregnancy care visits and offering practical assistance by arranging their wives’ mammography screening appointments. However, they revealed that they had limited conversations with their wives about breast cancer and breast health, possibly due to the perception that it is a sensitive topic not commonly initiated by men. Additionally, they mentioned that their wives are more likely to discuss breast health with female individuals they are close to, such as their mothers or female colleagues.
M19: yeah for myself actually I mean I follow my wife for the regular checkups and appointments with doctors and all that so that is on that going in and what other medical things she needs to go ahead, go for, but, as of now for a mammogram or something like that, no, no, nothing, as I mean spoken, but never really go in depth with it…
M17: Maternity visits we make it happen. But other than that other than maternity it’s just yeah. She, she goes for her appointments by yourself and, and that’s that…
M18: I don't really talk about it, I think, it is her privacy also, so I leave it to her to discuss if she needs to, can be quite sensitive.
M6: They are going to talk to their mother who doesn't know any better. They will consult their own mother even though as adults, they are well-educated. So then there is this unusual psychology going on there.
Family doctors were identified by some husbands as trusted figures whom individuals turn to when making health-related decisions. This suggests that family doctors could serve as key champions for advocating breast cancer screening in Singapore.
Husbands have vague impressions of existing public health efforts promoting breast cancer and screening awareness, such as posters, social media and pink ribbon campaigns featuring breast cancer survivor testimonies. However, they were unable to elaborate when probed further. Considering the substantial female representation in the workforce, some suggested that workplaces organise breast cancer awareness campaigns. To reduce the inertia of women signing up for mammography screening, immediate actionable steps could be provided (eg, a link to a registration form to book appointments) during such campaigns.
M14: … When you go to the doctor for discussion, both of you need to go together. This way, it might be better because you’re discussing it with the doctor then finally you’re going to come back and discuss it at home.
M11: Maybe there was a period of time, where there were more campaigns or publicity about it. And then they kind of raised a bit of awareness and then it petered off. So people don’t take notice after that.
M6: … bring it into the workplace because most women work nowadays. And then have regular lunchtime talks, maybe at least make sure every company does it twice a year. I mean just half an hour or one hour during lunchtime, and make everyone come.
Fears
The theme ‘fear’ was mapped onto the autonomic motivation COM-B construct. Husbands have reported known/potential fears women might have when contemplating to participate in breast cancer screening. These fears encompass losing insurance benefits, painful mammography screening experiences and receiving bad news of a cancer diagnosis.
M4: From what I understand, a lot of people will try not to do the health screening in Singapore, because they will have to let the insurance companies know (if they have cancer) and then after that there will be some sort of restrictions to their policy.
M7: I think, in my case. Yeah definitely, it is about their experience. She feels it’s very painful so pretty reluctant to go to the next one.
M1: Well, for me, I think my wife isn’t so keen to go for screening. I think she just doesn’t want to find out when there are bad results.
M6: …‘if I don’t screen, I don’t know. If I screen, I’ll find something so it’s better not to screen’. That kind of psychology is in the background…
Incentives
The theme ‘Incentives’ was mapped onto the physical opportunity and reflective motivation COM-B constructs. There was a general consensus from husbands that monetary rewards could increase motivation for women to engage in breast cancer screening.
Some husbands expressed that mammography screening should be free of charge or subsidised, with funding from either the government or women’s workplaces. Additionally, some husbands shared that their wives stopped attending mammography screening when it was no longer covered by their company’s benefits.
Husbands proposed the idea of receiving paid time off to motivate women to prioritise mammography screening participation. For example, companies can provide ‘breast cancer screening leave’.
M6: Have a breast screening leave. Compulsory for women, it’s given by the company. It will be paid. That day that they go for breast screening, they still get a salary. But that day, they don’t have to turn up for work, but they have to file a record that they have done the mammogram….
To encourage Singaporeans and Permanent Residents to attend mammography screening, husbands proposed a reward system under the MediShield programme, a government health insurance scheme that safeguards large healthcare expenses in the event of serious illnesses.
M2: Right, lets say, you go for the screening, they will pay you for, you know how many months of Medishield interest payment, that kind of thing.
Husbands’ attitudes towards risk-based screening
Husbands’ ‘attitudes towards risk-based screening’ were mapped onto the psychological capability and reflective motivation COM-B constructs. Our analysis revealed husbands’ concerns on the reliability of risk-based screening results, preferences in understanding risk reports, reactions from hypothetical risk results and perceptions on the usefulness of risk-based screening.
There were concerns about the possibility of false positives. Husbands shared that false positives may result in an unnecessary alarm and redundant follow-up recommendations, suggesting that the accuracy of risk-based screening is therefore crucial in determining its reliability and effectiveness.
M1: … And then there are a lot of false positives so you end up getting alarmed for no reason, so I think generally it’s not like a routine thing that people do.
The frequency of risk assessment was also brought up as husbands believe this would affect the reliability of the risk reports. A few of them emphasised that risk assessment should not be treated as a singular event since a woman’s risk of breast cancer can evolve due to factors beyond genetics.
M19: For myself, I think it’s good to have it so if it’s a yearly thing then no but if it’s like once every 10 years right as you’re saying that… then it looks fine.
Husbands did not show explicit understanding of what the different risk levels indicate (ie, low, medium and high) and most stated that they would prefer more education on it. Additionally, some emphasised that the interpretation of results should be done in the presence of an expert. This is because laypeople may not possess the necessary knowledge to accurately comprehend the results on their own.
M10: Yeah I agree that more information is better, but at the same time, I think if we want to give them. If we want to give numbers as results perhaps like what some of us have already shared. A consultation to explain that numbers would be really helpful instead of, you know, having a number that a lot of people may not understand. I wouldn’t know the technicalities of those numbers, perhaps. Maybe an explanation or short consultation after getting the result might be helpful.
M2: So I would like ’o see that, but I would not like average patients to see this kind of results, because if talking about low to medium and high. That doesn’t mean anything in itself. There needs to be a number. Like what is the incidence? Let’s say per 100k people over a lifetime, for example. People need to know the base rate, what’s the chance of false positives.
M17: I mean, I think it’s okay to offer, but at the same time, I think, education is going to be very important, with the information that you give the patient.
Husbands expressed various reactions to receiving low-risk and high-risk results when presented hypothetically during the FGDs. Some husbands described that receiving a high-risk result may have a profound impact, leading to feelings of fear and anxiety. These responses may either motivate individuals to seek more information on ways to reduce the risk or may evoke a fatalistic mindset that discourages regular breast cancer screening. On the other hand, some husbands expressed an indifferent attitude towards any risk result, embracing the fact that ‘life is unexpected’.
M17: I think I mean the initial thing that comes in, is fear, anxiety. I would hope, and I just hope that after an initial shock that. It comes down and then you are just aware of the tools that you have for annual screening.
M19: I mean when you have this kind of thing you will feel fearful, hey why, from where is this and what’s the reason behind it and how could you prevent it… like I don’t know where this is from, there must be a reason behind it so maybe maybe medications or form of diet or something like that to prevent it yeah.
Regarding low-risk results, husbands generally did not report drastic emotions if the results aligned with their expectations, as some mentioned they had perceived themselves as low-risk by default. However, if they had perceived themselves to be at low risk but received a high-risk report, this could trigger either positive or negative reactions.
M17: So at this point, you know, kind of default think of ourselves as low risk already. So getting a low-risk test score. I don’t think we change anything, compared to the opposite of getting a higher score will probably change a lot… Or at least prevent you know the stir up a lot of feelings.
Husbands mentioned that the usability of risk-based screening is determined by the follow-up actions that are suggested (new screening guidelines, lifestyle changes, etc). The presence of clear and specific actionable steps can alleviate fatalistic attitudes and concerns about being helpless and avoid confusion about the use of risk results. This approach assures participants that there are concrete actions they can take in response to their situations.
M7: I think if we want to show the results, then we better show or give the suggestion as well. Not just give a number, possibility. Tell them what to do next. 25% vs 12%, what’s the difference? What should I do? If we cannot give a clear suggestion, professional suggestion, practical suggestion, then it will make people very worried, think too much, but just don’t know what to do.
M6: Taking input from what has been shared. Sounds like although if you include genetic information that can predict the risk in a more specific way, it may not be helpful if there’s not much that can be done.
Husbands were able to successfully identify certain benefits of risk-based screening. They mentioned that knowledge of their wives’ high-risk status could motivate their wives to prioritise routine screening, allowing for early detection and the prevention of more complex treatments. Others mentioned that receiving a high-risk result could also prompt their wives to take action to improve modifiable lifestyle factors (eg, diet, physical activity and stress).
M6: For example, to give a very specific example, if your risk is high, but then you decided to screen more regularly, that means you are able to take action at an early stage, then the surgery will be a lot simpler…
Some husbands have stated that if their wives were at high risk, this knowledge would allow for advanced financial planning and mental preparedness to deal with a potential breast cancer diagnosis. There was also a suggestion to prevent insurance companies from accessing predictive risk reports to mitigate the risk of discrimination in insurance underwriting.
M14: Plan the insurance as soon as possible and so that you can at least support her financially and it lets you get the proper treatment as soon as possible and in terms of emotional, I think it can help us better prepare ourselves for sort of diverse outcomes.
Husbands also discussed the broader implications of risk-based screening. There is resistance to its widespread implementation as some believe that there is too much room for misunderstanding. These misunderstandings can arise as some people may have lower thresholds for processing new information.
M17: …So I mean for some people I’m sure it looks great, but for to be to be rolled out en masse, I think there is too much…I think there’s too much room for misinformation or…not even like malicious misinformation, but just misunderstanding about about what to do with the information and then also trust. Trusting the information and you know what to do as follow ups.
Finally, some husbands felt that their wives may prefer not to know their risk, and emphasis was also made on risk results being made optional.
M6: …Which means, maybe I don’t know whether it is possible, to make it optional for those who want to know, they can know. For those that refuse to know, then you don’t tell them.
Discussion
The FGDs revealed six key themes about husbands’ attitudes towards their wives’ breast cancer screening practices: awareness, priorities, social support, fears, incentives and views on risk-based screening. Similar findings have been reported by others.32 35 These themes were also reflected in the questionnaire data, which highlighted additional concerns not discussed in the focus groups. This suggests a gap in husbands’ awareness and limited health-related communication between spouses. While husbands showed interest in their wives’ health and supported them in making screening appointments, the data indicated that husbands’ influence may be limited due to a lack of awareness and communication. Most husbands accepted the idea of risk-based screening, though some raised concerns about the frequency of testing and interpreting results.
Fear was a major theme in both the BREATHE responses and FGDs, covering concerns about insurance, pain and diagnosis. Some husbands noted that women may fear losing insurance benefits if diagnosed with breast cancer, due to a lack of knowledge about coverage. Addressing this by exploring and communicating available financial support could alleviate fear and provide women and their spouses with the information needed to make informed health decisions. Given the fears related to painful mammography experiences and cancer diagnoses, the study team emphasises that the benefits of early detection far outweigh the temporary discomfort. Providing both practical and psychological support can help women overcome these fears. A survey in England found that 63% of people worry about cancer due to perceived threats to life and emotional distress.36 Addressing these concerns with accurate information about breast cancer and treatment options can help women recognise the value of early diagnosis and the possibility of effective treatment and recovery.
The theme of incentives, identified in both the BREATHE responses and FGDs, highlighted husbands’ suggestions to improve mammography attendance, such as offering incentives or credits for participation. Previous studies suggest that such strategies could motivate healthier behaviours.37 38 Husbands also advocated for breast cancer screening to be included in company healthcare benefits. Notably, gig workers may lack access to these benefits,39 which could discourage preventive care. To address this, community organisations, non-profits and healthcare providers could offer low-cost or free screening programmes targeting underserved populations, including gig workers.
While BREATHE respondents recognised the importance of screening as a reason for attending mammography, husbands in the FGDs did not mention this as a motivating factor. This suggests that a lack of awareness may disadvantage husbands’ support for their wives’ screening behaviour. Their misconceptions about barriers like cost and waiting time could also prevent utilisation of existing initiatives such as free screenings and mammobus services. Similar misconceptions have been observed among women in Singapore.40 Increasing awareness can both motivate and improve support for breast cancer screening by correcting misunderstandings about barriers. Our FGD findings also suggest that current public health initiatives may not effectively engage the public on breast health. Despite high internet and social media usage in Singapore (96.9% and 84.7% in 2023, respectively), awareness campaigns often overlook men.41 42 The prevalence of targeted content further limits outreach to men, leaving husbands unprepared to support their wives. Reassessing these strategies, including the use of culturally sensitive messaging, is essential to reach diverse ethnic groups and promote equitable health outcomes in Singapore’s multicultural society.43
The BREATHE results revealed additional insights that are not discussed in the FGDs. Among screening attendees, 6% cited health-related factors like past gynaecological issues or breast symptoms as reasons for screening, while 10% of non-attendees felt healthy and at low risk. Husbands in the FGDs did not mention health status as a factor influencing screening decisions, suggesting a lack of communication between spouses about health-related concerns. This may be due to the younger median age of the FGD participants (41 vs 48 years) and the questionnaire’s ability to highlight new insights. Promoting better communication between spouses can improve understanding and support for screening, which may lead to better screening behaviours.
Husbands are willing to assist with practical tasks like booking or rescheduling mammography appointments, but they need to be informed about the importance of screening and available resources to help their wives make informed health decisions. Research shows that women who have not engaged in specific behaviours often lack motivation to change, and many women would consider screening if encouraged by their husbands.44 45 Including spouses in preventive interventions and providing social and environmental support can drive behavioural change.46
In addition, we explored husbands’ views on transitioning from age-based to risk-based breast cancer screening. They believed the current guidelines primarily concern women of the recommended age, leading to a misconception that younger women are not at risk. This belief may contribute to the low engagement with screening programmes, as women often underestimate their risk.47–52 Notably, about 30% of breast cancer cases in Singapore occur in women younger than the recommended age for screening.53 Most husbands accepted risk-based screening but expressed concerns about the frequency of risk assessments. They emphasised a right balance between test accuracy, frequency, and public confidence.
Husbands in our study also expressed concerns about potential misunderstandings of risk-based screening, emphasising the need for expert guidance in interpreting results. Previous studies, such as one by Rainey et al, found that women’s preferences for receiving breast cancer risk results vary.54 High-risk individuals preferred personalised consultations, while low-risk individuals favoured concise written or online summaries. Preferences also differed by country, with Dutch and Swedish women wanting risk assessment integrated into cervical screening, while British women suggested specialised women’s clinics. The effectiveness of risk-based screening also depends on participants’ ability to understand their risk and make informed decisions. Fagerlin et al found that individuals with low risk may avoid beneficial treatments due to biases from additional information.55 When predicted risk does not align with perceived risk, people tend to exhibit strong emotional responses, which could serve as either resistance or motivation towards risk-based screening. A study in Greater Manchester found that women whose predicted risk did not align with their perceived risk had lower intent to undergo screening and lower rates of supplemental mammography.56 This suggests that risk discordance may affect the acceptability of risk-based screening, though further research is needed to explore its role as a barrier or motivator.
The strengths of the study include the large sample size, which enhances generalisability and statistical power, the use of a validated COMB model, ensuring a robust theoretical framework and the detailed description of the qualitative methods, which allows for clear understanding and reproducibility, ensuring transparency and rigour. However, we cannot establish a causal relationship between spousal support and breast cancer screening attendance, as our study focused on existing behaviours without follow-up assessments. Additionally, most wives of our FGD participants had not undergone mammography screening, so our findings may primarily apply to first-time screeners. A study among employed women found that prior screening was a strong predictor of future screening, suggesting the need for tailored interventions for first-time versus routine screeners.57
Involving spouses can help overcome barriers and fears, increasing the likelihood of women undergoing mammography screening. However, the lack of awareness about breast cancer and screening among husbands highlights the need for targeted education.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
The BREATHE study was approved by the National Healthcare Group Domain Specific Review Board (reference no: 2020/01327). Written informed consent was obtained from each participant. The FGD study received approval from the A*STAR Institutional Review Board (2021-077). All participants provided recorded verbal consent before their involvement.
Acknowledgments
We wish to express our gratitude to the Focus Group Discussion and questionnaire participants who shared their valuable insights and experiences. We also want to thank our dedicated research and administrative staff—Ying Jia Chew, Nur Khaliesah Binte Mohamed Riza, Yen Shing Yeoh, Hui Ling Tan, Pooi Yee Wong, Kimiie Wei Lin Chia, Nabilah Binte Supiee, Ganga Devi D/O Chandrasegran, Hui Min Lau, Siti Zulyqha Binte Yazid, Amanda Tse Woon Ong, Jing Jing Hong, Yi Lin Chen, Jinan May Loewen, Alleza Joey Balbanero Aquino, Jolene Lu Yee Poh, Nurfilya Binte Hamdil, Hian Ching Ng, Varshaa D/O Saravanan, Vannevia Jedidiah Shi Tong Foo for their contributions in the planning, preparation, and execution of BREATHE. We would also like to thank Renee Wong Ying Xuan for her help in the editing of this paper.
References
Footnotes
X @J_i_n_g_m_e_i
KAK, JJKL and FG contributed equally.
Contributors Conceptualisation, JL and KM; methodology, JL, JJKL, KM, ZLL, PJH and FG; data curation, JJKL, TMYS, JeL and MH; formal analysis, JJKL, FG, KAK and KM; writing—original draft preparation, JL, JJKL and KAK; writing—review and editing, KAK, JJKL, FG, ZLL, PJH, TMYS, AK, CHC, PTCI, JeL, SCK, ZPZ, BKTT, VKMT, MH, KM and JL; supervision, JL and KM; project administration, JJKL and JeL; funding acquisition, MH, KM and JL. All authors have read and agreed to the published version of the manuscript. JL is the guarantor of this study. ChatGPT and Grammarly were used to refine the language and improve the readability of this manuscript. The authors reviewed and edited all AI-generated content to ensure accuracy and originality.
Funding This study was supported by funding from the following sources: Precision Health Research, Singapore—BREATHE CIP; Agency for Science, Technology and Research—Social Sciences Innovation Seed Fund (C211618001); JurongHealth Fund—JHF-20-RE-003; Ministry of Health, Singapore—National Medical Research Council—Clinician Scientist Award (SI) (NMRC/CSA-SI/0015/2017); National University Cancer Institute, Singapore—Ng Teng Fong General Hospital Collaborative Grant (CGAug16C002) and Centre Grant Programme (CGAug16M005); National University of Singapore—Yong Loo Lin School of Medicine—Breast Cancer Screening Prevention Programme (NUHSRO/2020/121/BCSPP/LOA) and the National University of Singapore—Saw Swee Hock School of Public Health—Asian Breast Cancer Research Fund (SSHSPH-Res-Prog-BCPP). The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.