Article Text

Abstract
Introduction Maxillary transverse deficiency (MTD) is a common type of malocclusion. For adult MTD patients with highly ossified midpalatal sutures, surgically assisted rapid palatal expansion (SARPE) has been the conventional method of maxillary expansion. However, SARPE has the disadvantages of significant trauma, high cost and a high incidence of adverse events. Therefore, we proposed a novel minimally invasive method for maxillary expansion, which is midpalatal suture osteotomy combined with microimplant-assisted rapid palatal expansion (MSO-MARPE). The results are expected to confirm MSO-MARPE as a novel minimally invasive alternative to SARPE in skeletally mature MTD patients.
Methods and analysis A prospective, single-centre, parallel-group randomised controlled trial will be conducted, enrolling 20 adult MTD patients. Participants will be randomised equally to the control and experimental groups. The control group will undergo a Lefort I and median osteotomy and postoperative maxillary expansion with a tooth-borne Hyrax-type expander. The experimental group will undergo a midpalatal suture osteotomy and postoperative maxillary expansion with a microimplant-assisted expander. A series of linear and angular parameters will be measured in the pre- and post-coronal planes before treatment (T0), immediately after expansion (T1) and 6 months after expansion (T2) to evaluate the efficacy of skeletal expansion and dental side effects. The study aims to compare the clinical and cost-effectiveness of SARPE and that of MSO-MARPE. The primary outcome is the contribution of posterior midpalatal expansion immediately after expansion. The secondary outcomes include nasal, sutural, alveolar and dental expansion, pain intensity, operative time and treatment costs. The safety indicator will be the number and incidence of adverse events. The interaction between the control group and the experimental group will be analysed using two independent-sample t-tests or Mann–Whitney U test, and the paired data at different time points will be analysed using paired t-test.
Ethics and dissemination The trial protocol (version 6.0 13 December 2024) has been approved by the Institutional Review Board of the Ninth People’s Hospital of Shanghai Jiao Tong University School of Medicine (approval number: SH9H-2023-T309-3). Results will be disseminated through peer-reviewed publications and presentations at scientific conferences.
Trial registration number ChiCTR2400081545.
- Adult orthopaedics
- Randomized Controlled Trial
- ORAL MEDICINE
- ORAL & MAXILLOFACIAL SURGERY
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study will employ a single-centre, parallel-group, randomised controlled trial design.
A series of outcome measures will provide a comprehensive assessment of skeletal expansion, alveolar remodelling and dental buccal tipping in both the sagittal and vertical dimensions for the two maxillary expansion protocols.
Pain intensity, operative time, cost-effectiveness and adverse events will also be evaluated.
The efficacy of maxillary transverse deficiency correction will be assessed both immediately and 6 months after treatment.
Blinding of the participants, surgeons, orthodontists and outcome assessors is not possible.
Introduction
Maxillary transverse deficiency (MTD) is characterised by a mismatch in the width of the maxilla and mandible, mainly attributable to the constricted width of the maxillary base bone. MTD is one of the most pervasive skeletal problems in the craniofacial region and accounts for approximately 10% of the general population and 30% of adult orthodontic patients.1–5
MTD is typically presented as a posterior crossbite or dental compensation, with crowd dentition, wide buccal corridor and narrow upper airway.1 If left untreated, it is very likely to result in poor occlusal function, unfavourable smile appearance and respiratory problems.6 Although MTD can be easily masked by sagittal and/or vertical malocclusion, it is generally advisable to address the issue before other types of malocclusion.7
The midpalatal suture is the transverse growth centre of the maxillary complex. As the direct target and one of the most significant skeletal resistance regions of the maxillary expansion, the separation of the midpalatal suture is a fundamental prerequisite for the success of the treatment.8 9
Orthopaedic maxillary expansion is the result of skeletal (sutural opening), dental (buccal tipping) and alveolar (bending and remodelling) alterations.10–13 A tendency of dental tipping and alveolar bending to relapse was significant after appliance removal.12 Therefore, the objective of maxillary expansion is to achieve the optimal width of maxillary basal bone through as much pure skeletal expansion while limiting the buccal inclination of the anchor teeth.
In more than half of skeletally mature adults, the midpalatal sutures are highly interdigitated and fused, with a stage of maturation of D or E.14–16 This makes it challenging to split the midpalatal suture and expand it to an adequate amount in adult MTD patients through non-surgical maxillary expansion.17 18
Surgically assisted rapid palatal expansion (SARPE) has been accepted as a routine treatment strategy in adults with MTD of more than 5 mm.19 The common protocol for SARPE includes Lefort I and median osteotomy, performed under general anaesthesia, and tooth-borne maxillary expansion after surgery.19 Nevertheless, 22% of patients presented various operative complications, including nasal septum deviation, epistaxis or intraoral bleeding, pterygoid plexus nerve injury, oculomotor paralysis, pterygoid process fracture and skull base fracture.20 Additionally, the utilisation of a tooth-borne expander frequently results in dental complications, including anchor tooth tipping and elongation, atrophy of the periodontal ligament, buccal root resorption, buccal cortical perforation and relapse.19 20
In recent years, microimplant-assisted rapid palatal expansion (MARPE), with four microimplants implanted in the hard palate to generate strong expansion forces, has emerged as a new non-surgical expansion method that has replaced some SARPE cases, with a reported mean success rate in opening the midpalatal suture of more than 80% in late adolescents and young adults, but only 76% in patients up to 37 years of age and only 50% in adult male patients.6 21–24
Although the rate of successful midpalatal suture opening was relatively high in young patients, the failure rate of MARPE cases in adult patients should not be overlooked, especially in males aged over 25 years.25 Moreover, even in those with successful suture opening, amounts of expander activation were inevitably dissipated due to excessive skeletal resistance, resulting in tilting or loosening of the microimplants and ultimately presenting as inadequate skeletal expansion.17 18 According to Yoon et al,25 approximately 30% of the patients did not get adequate expansion in the initial attempt, and in the subset of patients who subsequently underwent a secondary expansion, an additional 38% exhibited inadequate expansion. For skeletally mature adult patients presenting with moderate to severe MTD, a certain degree of surgical intervention is still indicated.19 26
Consequently, the trend in adult MTD correction is to establish a relatively minimally invasive expansion protocol that can effectively expand the maxilla in patients who conventionally require SARPE.27–30
In view of these, we proposed a modified method of minimally invasive midpalatal suture osteotomy combined with MARPE (MSO-MARPE). The midpalatal suture was split completely to relieve the major skeletal resistance under local anaesthesia, and then microimplants will be inserted bicortically to provide stable anchorage. To date, no prospective clinical study has demonstrated whether this modified method could be an alternative to SARPE.
Aim and hypothesis
This study protocol describes the objectives and methods of an ongoing randomised controlled trial (RCT) comparing the clinical and cost-effectiveness of SARPE and that of MSO-MARPE in adult patients with MTD. It is hypothesised that the results will provide an evidence-based basis for the clinical application of MSO-MARPE as a novel minimally invasive treatment for adult with moderate to severe MTD.
Methods and analysis
Study design
This is a single-centre, parallel group, open RCT and is now being carried out in the Department of Oral and Cranio-maxillofacial Surgery, Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine (Shanghai, China). The study was scheduled to start in August 2023 and is expected to end in July 2027. The first subject was enrolled in March 2024, and the final date for subject enrolment is set for January 2027. This protocol was written in accordance with the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) guidelines for protocol reporting.31
Initial cone beam computed tomography (CBCT) scans or CT scans and dental casts will be together used for MTD diagnosis. Patients will be equally divided into two groups, both including surgery and maxillary expansion session, with a 7 day interval between two sessions.
Patients in the control group will be treated with traditional SARPE, which consists of the Lefort I and median osteotomy and the following tooth-borne rapid maxillary expansion. Patients in the experimental group will be treated with the midpalatal suture osteotomy followed by MARPE treatment.
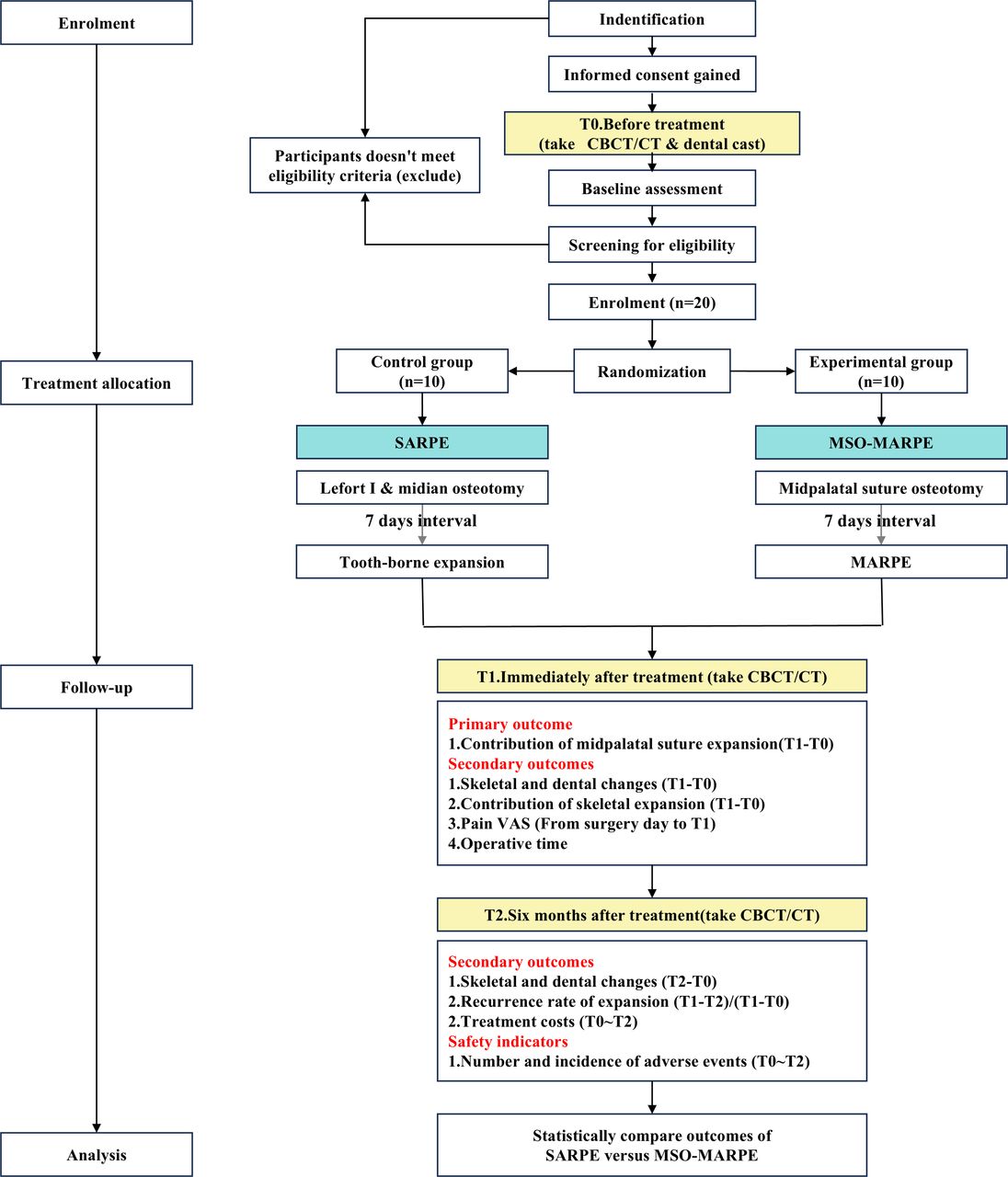
For each participant, CBCTs or CTs will be taken before treatment (T0), immediately after expansion (T1) and 6 months after expansion (T2) to quantify the skeletal and dental changes. In addition, a visual analogue scale (VAS) for pain will be recorded every 3 days throughout the maxillary expansion process. The operative time, treatment costs and the number and incidence of adverse events will also be recorded. Participant timeline and trial design are described in figure 1.

Participant flow diagram.
Eligibility criteria
Inclusion criteria for participants
Diagnosed with 5–12 mm MTD based on the combined evaluation of both Yonsei Transverse Index on CBCT or CT and ‘Element III’ of ‘The Six Elements of Orofacial Harmony’ (‘Andrews analysis’) on dental cast (figure 2).32 33
Aged 18 to 45.
Midpalatal suture maturation belongs to stage D or E, according to the classification method proposed by Angelieri et al.16

Diagnostic criteria for maxillary transverse deficiency. Normal Yonsei Transverse Index = Mx.CR W - Md.CR W = (-0.39±1.87) mm. Normal maxillomandibular difference of Andrews analysis = 16-26 FA W - 36-46 FA W = 5 mmNote. Mx. CR W represents the width between the centres of resistance of the bilateral maxillary first molars; Md. CR W represents the width between the centres of resistance of the bilateral mandible first molars; FA W represents the width between the facial-axis point of the bilateral first molars. The value of 36–46 FA W is equivalent to the ‘horizontal distance of bilateral WALA ridge − 4 mm’.
Exclusion criteria for participants
Presence of cleft lip and palate, severe craniofacial anomalies or sydromic conditions.
History of orthodontic or orthopaedic treatment.
History of maxillofacial trauma.
Moderate to severe periodontal disease.
Maxillary first premolar and/or first molar missing.
Preoperative examination indicates unsuitability for surgery.
Unable to cooperate with treatment.
Eligibility criteria for intervention performers
Orthognathic surgeons and orthodontists with over 3 years of experience.
Participant identification and enrolment
The trial is open for recruitment throughout China, and a fee waiver of RMB 1500 will be provided to all patients enrolled in the trial. Screening and enrolment will continue until the target number of participants is achieved.
Initial identification will be carried out by the centre’s clinical team, mainly based on demographic information, intraoral examination and preliminary analysis of dental casts. Potential participants will then be screened by experienced orthodontists in the research team according to combined evaluation of the scans and dental casts.
CBCT has been widely used in the dental field in recent years due to its low radiation dose and significant advantages in three-dimensional craniofacial analysis.34 And for patients deemed likely to require subsequent orthognathic surgery, CT is routinely taken for the purpose of surgical planning. Meanwhile, dental casts are almost always taken for malocclusion diagnosis and treatment planning.
For those potential participants who have had their CBCT or CT scans and dental casts taken within 6 months prior to the screening time point and who have had no orthodontic or orthopaedic interventions during the period, the previously taken scans and dental casts could be used for screening.
Patients who have been screened and confirmed to be eligible will be offered opportunities to participate in the trial and be provided with all relevant information both verbally and in writing.
Randomisation and blinding
All participants will be registered on the screening entry form and numbered from 1 to 20 according to the time of registration. First, a random number of 0 or 1 will be generated for each participant using the RANUNI function (one for the experimental group and 0 for the control group). Then, the random numbers will be sorted by PROC SORT and then grouped in parallel in a 1:1 ratio. The process of randomisation will be conducted by a statistician, independent of the research team. The allocation results will be recorded by the statistician and sealed in envelopes, one at a time, with the entry number written on the outside before being handed to the research team.
Participants are at liberty to withdraw from the entire trial or from follow-up only, at any time without impacting their standard of treatment. Withdrawals occurring post-randomisation will be monitored by the oversight committee.
This is an open RCT. The participants, surgeons and orthodontists cannot be blind to the assignment of interventions. Given the fact that the incisions of osteotomy can be observed on the scan images, it is also impracticable for the scan assessor to be blinded to the assignment result.
Interventions
Control group procedure
Surgery session
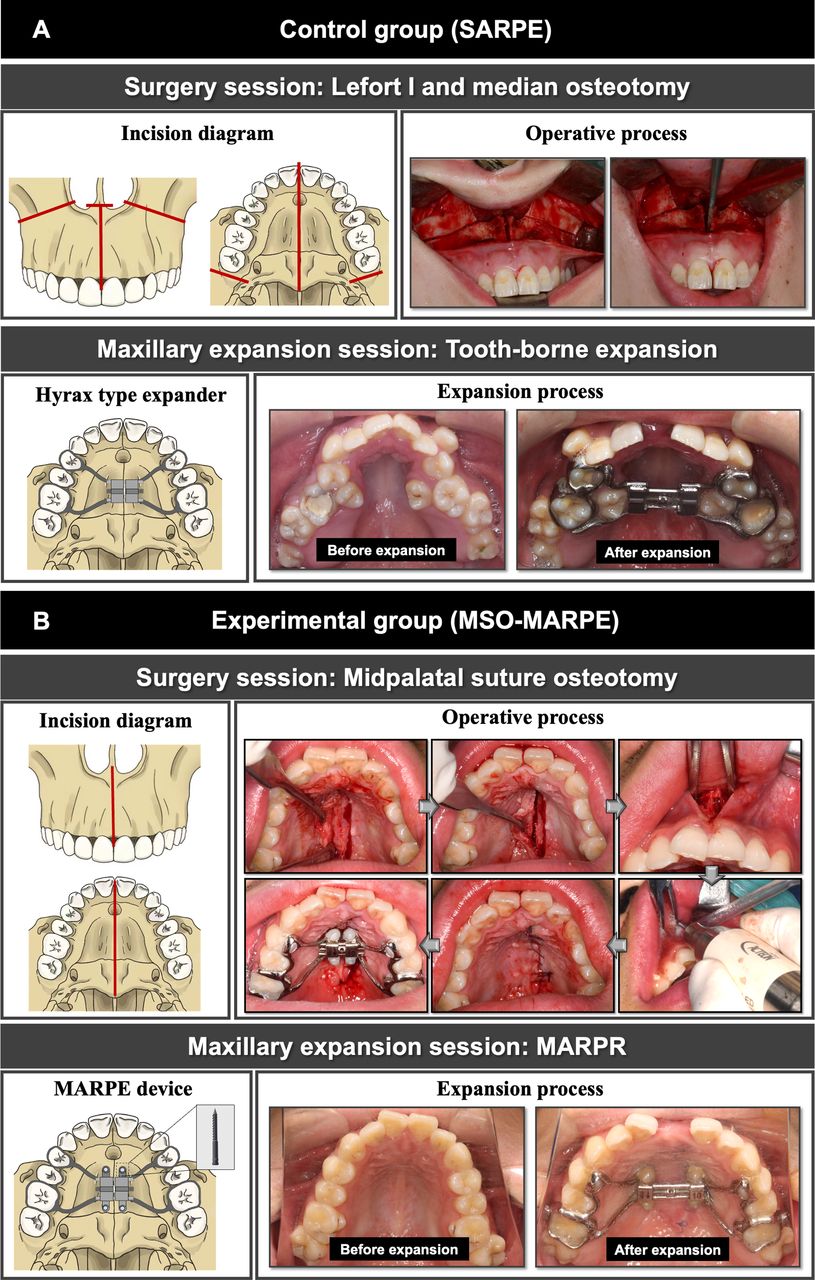
For the SARPE group, patients will first be conducted Lefort I and median osteotomy under general anaesthesia. The surgery included Lefort I osteotomy performed bilaterally by reciprocating saw; midpalatal suture splitting, which is achieved with blunt chisels directed at the palate, but not rupture the palatal mucosa; pterygomaxillary disjunction and nasal septum disruption performed by chisel figure 3A.

Interventions. (A) Interventions of the control group (SARPE); (B) Interventions of the experimental group (MSO-MARPE).
Maxillary expanding session
The Hyrax tooth-borne expander is installed by cementing the device to the maxillary first premolars and first molars immediately after surgery and the activation of the expander begins 7 days postoperatively at an activation rate of 0.2–0.4 mm per day until the MTD is fully corrected or the expanders have reached their limit. On completion of activation, the Hyrax expanders will remain blocked for a minimum of 3 months.
Experimental group procedure
Surgery session
For MSO-MARPE group, patients will first be conducted midpalatal suture osteotomy under local anaesthesia. The minimally invasive surgery consists of two incisions: one is to incise the palatal mucosa 2–3 mm adjacent to the palatal suture, flip the flap along the bone surface and incise the midpalatal suture from the posterior margin of the incisal aperture to the posterior nasal spine; the other is to make a longitudinal incision along the labial band in the vestibular sulcus, flip the flap to expose the bone surface and incise the bone from the anterior nasal spine to the top of the alveolar ridge, deepen it to the palatal cortex of the mesial incisal teeth and then reach to the front margin of the incisal aperture at the posterior side. Thus, the midpalatal suture is separated completely. The scalpel is used to incise mucosa, while bony splitting is performed by piezo-bone scalpel figure 3B.
Maxillary expanding session
The MARPE device used in this study consists of four microimplants and an expander connected to the anchor teeth. Based on the patient’s palatal bone thickness and the shape of the palatal vault as shown on the initial scans, the MARPE device will be custom designed using a digital workflow to position the microimplant in an area with bone thickness greater than 2.5 mm and to ensure that it can be anchored bicortically. As in the control group, the MARPE device will be installed immediately after surgery, and the activation will begin 7 days postoperatively at an activation rate of 0.2–0.4 mm per day. Activation termination criteria and retention time will be the same as for the control group.
Intervention modifications
In the event of the participant experiencing serious complications, such as loosening of the anchor teeth by more than 2°, it is necessary to interrupt the treatment. The major investigator will make the final decision to terminate the trial.
As with all patients receiving SARPE or MSO-MARPE, enrolled participants will be asked to have their efficacy and oral health checked by the orthodontists when about half of the expansion limit of the expander has been activated, and the orthodontists will make appropriate adjustments to the expansion strategy.
Measurements on CBCT or CT
In this study, the difference of values of the same parameters measured on CBCT or CT at different time points will be used to describe skeletal and dental changes. The data management group will code the scan file, and then experienced assessors A and B will independently perform the scan measurements and the results will be recorded as the average of the two. If the difference between assessors A and B is greater than 0.5 mm or 3°, it should be measured by assessor C and compared with the previous measurements.
Measurement planes
A series of skeletal and dental parameters will be measured in post- and pre-coronal planes. Both post- and pre-coronal planes will be set perpendicular to the Frankfort plane (FH plane), passing the bilateral infraorbital lower margins and the right portion. Meanwhile, the post-coronal plane will cross the centres of resistance (CRs) of bilateral maxillary first molars, and the pre-coronal plane will cross the CRs of bilateral maxillary first premolars (figure 4).

Landmarks for head re-orientation and definitions of measurement planes. Note: Blue line represents the FH plane, yellow line represents the pre-coronal plane; green line represents the post-coronal plane. OR is an abbreviation of infraorbital lower margin; PO is an abbreviation of the portion.
The position of CR is relatively stable and is not readily affected by the simple tilting movement of a tooth; thus, CRs will be chosen as landmarks for the definition of two standard coronal planes in this study.32 For a single-rooted tooth, CR is at the level of the coronal one-third; for a multirooted tooth, CR is at the level of the furcation.32
Head re-orientation will be performed on CBCT or CT of T0. After re-orientation, the scans taken at T1 and T2 will be superimposed on the scans of T0 based on the structure of anterior cranial base using the voxel-based technique.
Measurement parameters
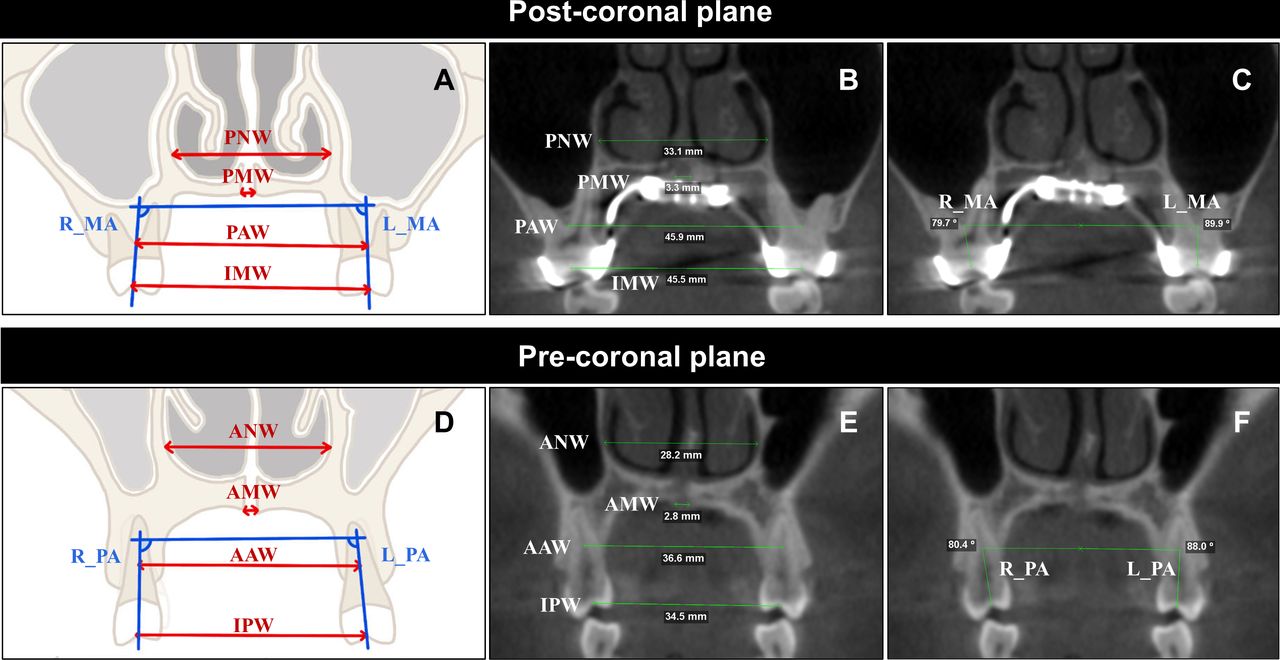
In this study, four linear and two angular measurements will be obtained in each coronal plane at each time point, specific definitions are shown in table 1 and figure 5. When measuring inter-molar/premolar width and molar/premolar angle, adjust the thickness of the coronal slice stacks until the CR and central fossa can be clearly defined in the same view.
Definitions of measurements on scan images

Skeletal and dental measurements (take CBCT of T1, for example). (A) Schematic diagram of measurements in the post-coronal plane; (B) Linear measurements in post-coronal plane; (C) Angular measurements in the post-coronal plane; (D) Schematic diagram of measurements in the pre-coronal plane; (E) Linear measurements in the pre-coronal plane; (F) Angular measurements in the pre-coronal plane.
Outcomes
In line with SPIRIT guidance, table 2 provides a complete list of planned outcome measures in this trial.31
Outcomes and assessment schedule for the trial
Primary outcome
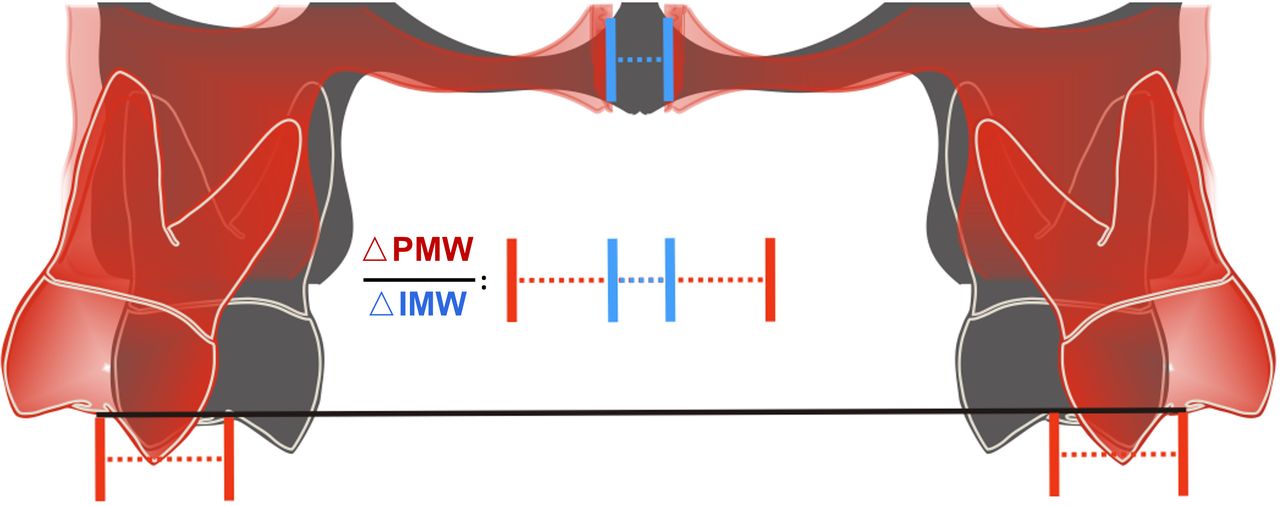
The primary outcome is the immediate contribution of posterior midpalatal suture expansion (CMEpost), defined as the ratio of△PMW(T1-T0) to △IMW(T1-T0)(figure 6). △PMW reflects the pure skeletal expansion of the posterior palatal segment. △IMW represents the total amount of posterior maxillary expansion, consisting of skeletal and dental changes.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Primary outcome: contribution of posterior midpalatal suture expansion.
The reasons for choosing CMEpost as the primary outcome are as follows. First, the skeletal resistance to expansion mainly lies in the posterior segment of the maxillary complex, and the midpalatal suture is the direct target of maxillary expansion, with the posterior segment being more difficult to expand than the anterior segment.35–37 In addition, the amount of expander activation is not the same in different cases; thus, we chose the contribution of skeletal expansion rather than its absolute value as the primary outcome. The higher the CMEpost, the less the unexpected buccal inclination of the alveolar bone and the anchoring teeth would be.
Secondary outcomes
Secondary outcomes include the values of width and angle changes at ‘T1–T0’ and ‘T2–T0’, the contribution of these changes at T1, recurrence rate of expansion at T2, the VAS for pain, operative time and treatment cost. The clinical significance of these outcomes is shown as follows:
Skeletal and dental changes
The absolute values of the series of skeletal and dental changes will directly reflect whether the desired treatment goals have been achieved and whether a second expansion attempt is necessary.
Nasal expansion (△PNW and △ANW): the nasal cavity is located above the palate, and it is accepted that the maxillary expansion treatment could expand the width of the nasal cavity to some extent, which could potentially alleviate the nasal breathing problems, which are prevalent among MTD patients.38
Midpalatal suture expansion (△PMW and △AMW): midpalatal suture expansion represents pure skeletal expansion and is important for the stable skeletal correction of MTD. Considering the bone repair process within the sutural gap is apparent during the retention time, the change at ‘T2–T0’ will be excluded.39
Alveolar expansion (△PAW and △AAW): the change of the alveolar width represents the expansion of maxillary basal bone, consisting of the alveolar remodelling and the lateral movement of hemi-maxillary complex. Alveolar expansion is relatively stable for long-term efficacy compared with buccal tipping of teeth.
Inter-crown expansion (△IMW and △IPW): the change of the bilateral distance of anchor crowns represents the sum of skeletal and dental changes. The expansion forces applied to the anchor teeth cause the anchor teeth to tilt buccally, increasing the inter-crown distance. After removing the metal band attached to the anchor teeth after expansion, the buccally inclined anchor teeth will spontaneously tilt lingually during the retention phase. This leads to a reduction in the distance between the crowns, which is the main cause of relapse.
Buccal inclination of teeth (BIpost and BIpre): BI represents the change in the angle of the anchor teeth. Severe buccal inclination of the anchor teeth is very likely to result in buccal gingival recession and buccal cortical resorption, even perforation and dehiscence.20
Contribution of skeletal expansion
From the apex to the base of the maxillary complex, the contributions of nasal expansion, midpalatal suture expansion and alveolar expansion to the total expansion at T1 (CNE, CME and CAE) are calculated. Among these outcomes, CMEpost was defined as the primary outcome. The consideration of these outcomes as a whole can reflect the vertical expansion pattern of the maxillary complex at both anterior and posterior palatal segments.
Recurrence rate of expansion
Recurrence is inevitable in maxillary expansion treatment.40 In patients with MTD, it is important to achieve stable widths of the nasal cavity, maxillary basal bone and inter-crown distance in the long term, especially the latter two. This study will calculate the recurrence rate of nasal expansion, alveolar expansion (ie, maxillary basal bone expansion) and inter-crown expansion at T2 compared with T1 (RNE, RAE and RME&RPE). These recurrence rates will be an important guide for orthodontists on how much over-expansion to apply.
VAS for pain
Pain intensity postoperatively and during the expansion session is an important factor to consider. The VAS has been widely used to measure pain intensity in adult population.41 42 Pain intensity is classified as mild (VAS score 1–3), moderate (VAS score 4–6) or severe (VAS score 7–10). All participants will be asked to record the VAS every 3 days from the day of the operation to T1.
Operative time
The duration of the surgical procedure, except the time of anaesthesia and awakening. The longer the operative time, the higher the risk.
Treatment costs
As both treatment protocols involve surgery, the costs are relatively high, so the economic burden is a factor that should not be neglected.
Safety indicators
Safety indicators include the number and incidence of adverse events. An adverse event is defined as an unwanted medical event that occurs during treatment or retention periods that did not occur before treatment or that is worse than before treatment, but is not necessarily causally related to the treatment. An adverse event can be any unexpected and unwanted symptom, sign, disease or abnormal examination result.
The categorisation of adverse events is determined by the level of intervention necessitated for their resolution. Adverse events that can be rectified with minor intervention are designated as mild, while those resulting in hospitalisation, prolonged hospitalisation, injury or disability, impact on the ability to work, threat to life or death are classified as serious.
Reported mild adverse events include nasal septal deviation, epistaxis or intraoral bleeding, wound dehiscence, transient numbness, local infection or inflammation, transient headache or tearing or tinnitus, nausea or vomiting, mild periodontal defect or gingival recession, anchor tooth necrosis, asymmetric or inadequate maxillary expansion and device-related complications. Reported serious adverse events include mucosal necrosis, severe tooth loosening and resorption, tooth loss, severe bleeding, palatal fistula, pterygoid plexus nerve injury, oculomotor paralysis, pterygoid process fracture, skull base fracture, etc.20
Any adverse events and all related symptoms occurring from T0 to T2 will be recorded in detail, including occurrence time, severity, duration and final outcomes (eg, disappearance, remission and persistence).
Statistical analysis
Sample size calculation
The sample size was calculated based on the retrospective data of the primary outcome, that is, CMEpost. CMEpost was (71.69±20.27)% in the MSO-MARPE group and (36.58±10.95)% in the SARPE group.
According to the results calculated by PASS 15.0 software (PASS, Kaysville, UT, USA), a statistical power of 90% and a two-sided type I error of 5% were assumed, and a 20% dropout rate was considered. According to the 1:1 parallel distribution principle, 10 participants will be included in each group.
Statistical analysis plan
A statistical analysis plan will be written by statisticians and reviewed by the oversight committee prior to the final analysis. The primary and secondary outcomes will be analysed following the full analysis set; and the safety indicators will be analysed following the safe analysis set.
In descriptive statistical analysis, the continuous outcomes will be presented as mean, SD, median, minimum, maximum and IQR. The counting data will be presented as numbers and percentages.
Skeletal and dental changes, contribution of skeletal expansion, recurrence rate of expansion, VAS for pain, operative time and treatment costs will be compared between the control group and experiment group through two independent-sample t-test for normally distributed data or Mann–Whitney U test for non-normally distributed data. The paired data (eg, △PNW(T1-T0) vs △PNW(T2-T0)) will be evaluated by paired t-test. All statistical analyses were conducted using two-sided tests, with a p value of less than 0.05 indicating a statistically significant difference.
The inter-assessor consistency of the outcome will be presented as an intraclass correlation coefficient (ICC). The following criteria will be used to determine the degree of consistency: ICC<0.2, poor degree of consistency; 0.2–0.4, fair degree of consistency; 0.4–0.6, moderate degree of consistency; 0.6–0.8, strong degree of consistency; and 0.8–1.0, very strong degree of consistency.
The frequency and pattern of missing data will be rigorously examined, and the reasons for missing data will be recorded wherever possible. Multiple imputation of missing data will be used to deal with the missing data where appropriate, given the specific question and analysis.
Data management
The entire trial process will be conducted in accordance with the clinical trial quality management norms. For participants who discontinue or deviate from intervention protocols, the outcome data will be collected up to the point of discontinuation or deviation.
Following the verification of the completeness, veracity, clarity and objectivity of all paper Case Report Form (CRF) records, the data will be entered into the computer and stored after locking the data.
Completion and transfer of CRF
The CRF will be completed by the investigator for each participant and be submitted to the data manager for data entry and management. The recorders will collect and store the subjects’ imaging data and treatment records at each follow-up time point. All paper documents will be stored in a secure filing cabinet in the department.
Data entry and modification
To ensure accuracy, the data will be entered into the database system and checked by two data entry specialists. All data containing personally identifiable information will be kept in a separate file and identified by individual codes. For queries in the CRF, the data manager will send a query form (QF) to the researcher via the supervisor, which should be answered within 24 hours. The data manager will modify, confirm and enter the data according to the researcher’s response and send another QF if necessary.
Database locking
Once the database system has been confirmed as correct by the data manager, principal investigator, statistician, sponsor and supervisor, the database will be locked and no further changes will be allowed.
Data processing
Once the database has been locked, it will be sent to the statistician for a statistical analysis.
Committees
A data management group and an oversight committee will be established, independent of the investigators. As mentioned above, the data management group will be responsible for data entry, coding, security and storage. The oversight committee will be responsible for quarterly audits and monitoring visits to check for patient information, informed consent form, eligibility criteria, primary outcome and adverse event monitoring and declaration. The declaration of adverse event will be the responsibility of each investigator. In addition, the Institutional Review Board of the Ninth People’s Hospital of Shanghai Jiao Tong University School of Medicine will audit the conduct of the trial every 3 months.
Patient and public involvement
Patient representatives who have undergone treatment for SARPE or MSO-MARPE have been consulted in the design of the study, providing input on secondary outcomes such as pain intensity and treatment costs. They will not be involved in the recruitment of participants or the conduct of the study.
Ethics and dissemination
Ethical approval for the trial protocol (version 6.0 13 December 2024) has been granted by the Institutional Review Board (IRB) of the Ninth People’s Hospital of Shanghai Jiao Tong University School of Medicine (approval number: SH9H-2023-T309-3). The trial has been registered at https://www.chictr.org.cn/ (trial registration number: ChiCTR2400081545) with the registry name of ‘A randomised controlled study of midpalatal suture osteotomy and microimplant-assisted rapid palatal expansion for adult maxillary transverse deficiency treatment’. The trial will be conducted in accordance with the Declaration of Helsinki and Good Clinical Practice.
Prior to enrolment in this study, participants will be provided with comprehensive information about the clinical trial, including details of the trial content, the purpose of the trial, the expected efficacy, potential adverse events and the proposed countermeasures. Subjects will only be enrolled following a comprehensive understanding of the trial and the signing of an informed consent form. The informed consent form will be signed by both the investigator and the participant, dated the signature date, in duplicate, with each party retaining a copy. In instances where a legal guardian is representing a subject in signing the informed consent form, it is crucial to furnish the subject with all pertinent information regarding the clinical trial in a manner that is comprehensible to them and to encourage them to sign the consent form themselves.
In the event of a serious adverse event occurring during the course of the clinical trial, the oversight committee and the institutional review board must be informed promptly in written form. Furthermore, any modifications to the protocol must be formally amended and approved by the IRB before implementation.
The final results of the trial will be reported in accordance with the Consolidated Standards of Reporting Trial guidelines.28 The findings will be disseminated at international and national scientific conferences and in peer-reviewed journal articles in a timely manner after the completion of this study. Authorship of articles will be determined by discussion within the research team, adhering to authorship guidelines.
Discussion
SARPE is regarded as the standard treatment for adults with moderate to severe MTD. However, its apparent disadvantages, namely, significant trauma, elevated risk and financial expenditure, have prompted many orthodontists and adult patients to forgo MTD correction.19 20 Therefore, in recent years, many researchers and clinicians have devoted to proposing minimally invasive surgery-assisted maxillary expansion methods for adults MTD patients.10 27–29 43 44 The ongoing debate surrounding surgical-assisted expansion protocols primarily concerns the ideal extent of surgical dissection and the appropriate type of anchorage for the application of expansion forces. The ultimate objective is to achieve optimal skeletal expansion in skeletally mature MTD patients while minimising trauma and side effects. In this study, we have drawn on our clinical experience and the retrospective outcome of several cases treated with MSO-MARPE to formulate a scientific hypothesis. The hypothesis suggests that performing a complete incision of the midpalatal suture to induce the surgical trauma of SARPE, while applying MARPE to enhance the expansion force, may be an effective alternative to conventional SARPE.
This study aims to compare the maxillary expansion efficacy of MSO-MARPE vs SARPE for adult MTD patients. In order to achieve this aim and given that MSO-MARPE is a novel treatment protocol, it would be appropriate to firstly conduct a single-centre RCT.
In this study protocol, a series of outcomes reflecting the magnitude and contribution of skeletal, alveolar and dental expansion in different dimensions. A comparative analysis of the parameter values for ‘T1–T0’ and ‘T2–T0’ allows for the evaluation of the relapse tendency, while a comparative evaluation of the parameters measured on pre- and post-coronal planes permits the assessment of the sagittal expansion pattern. Furthermore, the combination of CNS, CME and CAE can be employed to analyse the vertical expansion pattern. It is expected that the series of outcomes as described in the ‘Methods and analysis’ section of this study protocol can also be applied to evaluate the efficacy of other emerging maxillary expansion techniques, such as corticopuncture facilitated MARPE.43
The major limitations of this trial are open label, and the relatively small sample size is conducted at a single centre. Open labelling will inevitably lead to a certain loss of equipoise, whereby trial participants perceive one intervention therapy to be superior to the other. This will introduce factors of difference between the two groups other than the treatment, which in turn will affect the assessment of outcomes, particularly for subjective indicators such as VAS for pain. In addition, while the current sample size is anticipated to be statistically adequate for the analysis of the primary outcome, it should be acknowledged that additional subgroup analyses may not be feasible due to the limited sample sizes at the single centre.
It is anticipated that the results of this study will provide valuable information about efficacious minimally invasive treatment modalities for adult MTD patients. If these results indicate that MSO-MARPE can be an effective alternative to conventional SARPE, a multicentre, large-sample RCT will be conducted in the near future. In the present single-centre RCT, subgroup analyses are not being performed. As a consequence, there are some confounding variables. Subgroup analyses will be performed in the future multicentre RCT. The design of these analyses will be taken into account prior to the multicentre RCT. It is anticipated that the results of the present study will form the basis for sample size estimation in the subsequent multicentre RCT, thus providing a higher-quality evidence-based basis.
Ethics statements
Patient consent for publication
Acknowledgments
We are grateful for the patients' willingness to participate in this trial. We would also like to thank our colleagues at the Department of Oral and Cranio-maxillofacial Surgery, Shanghai Ninth People's Hospital, Shanghai Jiao Tong University School of Medicine for their assistance in conducting the trial.
References
Footnotes
WZ and MC are joint first authors.
Contributors WZ wrote the original manuscript, conducted the retrospective pilot study and contributed to the study design and visualisation; MiC contributed to the study design, visualisation and review; YZ contributed to the study design and development of the proposal; YQ contributed to the statistical analysis; LZ contributed to the design; and LJ is the lead study methodologist, contributed to the supervision and is responsible for the overall content as the guarantor.
Funding This study is funded by Shanghai’s Top Priority Research Center (no. 2022ZZ01017); CAMS Innovation Fund for Medical Sciences (CIFMS) (no. 2019- I2M-5-037); Project of Biobank of Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine (no. YBKB202216); Shanghai Science and Technology Innovation Action Plan-International Science and Technology Cooperation Program (no. 23410713600); 'Two-hundred Talents' Program of Shanghai Jiao Tong University School of Medicine (no. 20221809); 'Star of Shanghai Jiao Tong University' Cross-Disciplinary Research Fund of Shanghai Jiao Tong University (no. YG2023ZD14)
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, conduct, reporting or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.