Article Text

Abstract
Objectives The study aimed to describe and compare the clinical physiotherapy management of patients hospitalised due to chest trauma in South Africa (SA) and Sweden.
Design A prospective observational multicentre international study.
Setting Two university-affiliated public sector hospitals in SA and four university-affiliated public sector hospitals in Sweden.
Participants In total, 364 adults, hospitalised due to chest trauma were consecutively recruited of which 179 were from SA and 185 were from Sweden.
Outcome measures Physiotherapy practice was recorded in parallel with standard care. In addition, pulmonary complications and length of hospital stay were collected.
Results Despite differences in the type of trauma between the national cohorts (83% penetrating traumas in SA and 95% blunt traumas in Sweden), most patients received physiotherapy treatment during the first 3 days in hospital. Physiotherapy interventions such as mobilisation (day 1: sit on edge of bed; days 1–3: walking) and exercises to maintain range of motion (days 1–3: shoulder; day 3: trunk) were initiated earlier in SA (p<0.05). Treatment with the active cycle of breathing technique was more used in SA while deep breathing exercises were more common in Sweden and positive expiratory pressure was common in both countries. Length of stay was in mean 5.4 (95% CI 4.8, 6.0) days in SA and 6.6 (5.8, 7.4) days in Sweden (p=0.024).
Conclusions Despite differences in trauma panoramas and the national cohorts there seem to be similarities in clinical physiotherapy practices between the two countries.
- Trauma
- TRAUMA MANAGEMENT
- Physical Therapy Modalities
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The combination of data from the two countries with different trauma panoramas gives a broader perspective of physiotherapy practice.
The large study cohort made it possible to perform subgroup analyses.
There are major differences between the study cohorts from the two countries.
General healthcare practice differs between the two countries.
Background
Worldwide, traumatic injury causes a substantial health risk with subsequent risk of disability and mortality.1 Injuries to the chest may be caused by blunt trauma (eg, road traffic accidents, assault or falls) or penetrating trauma (eg, gunshots, stab wounds) and can include rib fractures, flail chest, pneumothorax, haemothorax and pulmonary contusion.2–4 In the acute phase the injuries cause pain leading to decreased ventilation and oxygenation. Common pulmonary complications that develop following chest injury are atelectasis, respiratory distress, pneumonia and/or respiratory failure.4 Patients who develop such complications are particularly at risk of mortality.5 The aims of physiotherapy interventions for this population include the prevention of development of pulmonary complications and the management of those that are already present. Physiotherapy treatment involves normalisation of lung volumes and compliance; improvement of oxygenation; and optimising physical performance by encouraging active out-of-bed mobilisation away from the bedside as soon as the patient’s condition has stabilised.6 The implementation of appropriate pain relief strategies is also important in the management of such patients.6
Physiotherapists are important members of the multidisciplinary team who care for patients with chest trauma in an acute care setting.7 However, there is a scarcity of research within the field about the use and effects of different physiotherapy interventions for patients with chest trauma. In the 1990s, two studies were published where treatments (including breathing exercises, trunk movements and physical activity) initiated immediately after the insertion of an intercostal drain for patients with penetrating chest trauma were evaluated in comparison to interventions initiated after 9–12 hours8 or after 12–24 hours.9 It was found that the immediate interventions significantly reduced the time for fluid drainage from the intercostal spaces, and the length of hospital stay.
In the absence of evaluations of physiotherapy interventions for patients with chest trauma, our research group performed a survey in 2019 of which the aims were to determine the physiotherapy management of patients having sustained major chest trauma and to investigate how such practices varied internationally.10 The results indicated that most patients received active treatment such as coughing, deep breathing exercises, body positioning and early mobilisation. However, rehabilitation to address longer-term sequelae following hospital discharge was reported to be rare. The results from the previous study were based on questionnaires with subjective responses. There is a lack of observational studies investigating physiotherapy interventions used in clinical practice, and with whom and when they are initiated after chest trauma.
Therefore, the purpose of this paper is to describe and compare the physiotherapy management of patients recovering from chest trauma, the adverse events reported during physiotherapy treatment, and the pulmonary complications that developed during hospitalisation in South Africa and Sweden.
Materials and methods
A prospective observational multicentre study, using a clinical record review of adult patients with a traumatic chest injury, was conducted in these two countries with different trauma panoramas and patient groups to be able to capture a wider perspective of the phenomenon. Chest trauma was, in this study, presented as a blunt or penetrating injury resulting in pneumothorax, haemothorax, fractures of the ribcage, fractures of the sternum, and/or pulmonary injuries.
Ethical considerations
Permission to conduct this study was obtained from the trauma unit managers and physiotherapy heads-of-department at Charlotte Maxeke Johannesburg Academic Hospital (CMJAH) and Chris Hani Baragwanath Academic Hospital (CHBAH) South Africa and Sahlgrenska University (SU) Hospital, Karolinska University Hospital/Solna (KS), Umeå University Hospital (UU) and Skåne University Hospital/Lund Sweden. The Gauteng province of the South African National Department of Health provided permission for data to be collected from participants admitted to CMJAH and CHBAH. In South Africa, the University of the Witwatersrand Faculty of Health Sciences Human Research Ethics (Medical) committee provided ethical approval to conduct this study (clearance number: M200222). In Sweden, ethical approval was obtained from the Regional Ethics Committee for the region of Västra Götaland (clearance number: Dnr: 2019–04848). The ethical principles related to the conduct of research on human subjects outlined in the Declaration of Helsinki were observed. The patients were included after oral and written information was provided and written consent was obtained.
Context of the study
The South African patients approached for participation in this study were managed in the trauma intensive care units (ICUs), high dependency units (HDUs) and wards of CMJAH and CHBAH situated in Johannesburg, Gauteng. The Swedish patients were managed either in trauma centres (HDUs) (Stockholm and Gothenburg) or surgical wards with trauma profiles (Umeå and Lund). All participating hospitals are university-affiliated public sector hospitals and government-funded. In all hospitals, eligible patients in ICU or HDU were assessed daily to ensure that no complications arose before they were transferred to the ward. Patients with shorter ICU stays were transferred directly from the ICU to the wards but some who needed longer ICU stay were cared for in the HDUs before transfer to the trauma wards. Participants were treated according to standard physiotherapy practice at all participating hospitals. Physiotherapy was provided during regular working hours, which differed between the hospitals. All hospitals had physiotherapists on duty in the wards on weekdays, and at CHBAH, CMJAH, SU and KS there were also physiotherapists on duty on weekends, but then only for a selection of patients who were newly admitted or had existing acute respiratory symptoms. Other hospitals did not have physiotherapy on weekends, so their patients continued with their treatment independently or with the support of nursing staff.
Study setting and population
Patients who were 18 years or older and had been diagnosed with traumatic chest injury, with or without additional injuries, were consecutively screened for participation. They were admitted to and included in the trial while being cared for at the trauma ICU, HDUs or the surgical and trauma wards of the participating sites. Those with dementia, acute or previously diagnosed spinal cord injury or traumatic brain injury (Glasgow Coma Scale <12), complex fractures of the pelvis or lower limbs, amputation of the lower limb/s that restricted active mobilisation, and those with extensive abdominal trauma (open laparotomy managed in the ICU) were excluded from participation.
On average, 100 patients with thoracic trauma were referred for physiotherapy at CHBAH and CMJAH per month prior to COVID-19. The anticipated study population across these two South African participating sites was thus 1200 patients over a 12 month period. At the hospitals in Sweden, the average monthly patient admission rate for those with traumatic chest injuries was approximately 40 patients (combined) prior to COVID-19. Thus, an anticipated study population of 480 patients per year. A sample size estimate of 304 patients was calculated and was informed by an expected incidence of 45% pneumonia as described by Dhar et al11 in patients with a traumatic chest injury, 95% CI and a margin of error of 5%.
Procedure
Meetings were held with the clinical physiotherapy staff who worked in the trauma units and wards of the respective study sites to explain the study aims and objectives. These clinicians were asked to fill in participant details on study-specific data capture forms. Information collected included demographics (age, gender, height, weight, smoking history and presence of chronic pulmonary disease), clinical presentation (type and mechanism of a traumatic injury sustained), physiotherapy management received during the hospital stay, pulmonary complications that developed during hospitalisation and discharge information (length of stay, discharge destination, physiotherapy follow-up). The physiotherapists who oversaw the trauma ICUs, HDUs and surgical/trauma wards at the participating sites were responsible for recruiting participants, according to the set inclusion and exclusion criteria, as they screened the wards and units daily (Mondays to Fridays) for new admissions. All clinical physiotherapists provided the standard physiotherapy care of their institution to participants who provided consent. They were expected to record the specifics regarding their daily patient management and patient responses to treatment on the study-specific data capture forms. Participant recruitment and data collection occurred over a total of 18 months at the participating South African sites (October 2020 to October 2021 (CHBAH); August 2022 to February 2023 (CMJAH)) and over 12 months in Sweden (September 2021 to September 2022). Data were captured onto two electronic databases (REDCap at the University of the Witwatersrand (as per https://redcap.core.wits.ac.za/redcap/) for South African data and Google Drive for the Swedish data).
The STROBE checklist was used in reporting this study (as per https://www.strobe-statement.org/strobe-publications/)
Statistical analysis
Continuous variables are presented as mean (SD) or median (min-max) and categorical variables with numbers and percentages. Differences between the countries were analysed with a Student’s t-test for continuous variables and with a Pearson χ2 test for categorical variables. The χ2 test with the Phi coefficient was used to determine the association and correlation between the development of pulmonary complications and the type of injury sustained, deep breathing exercises performed, and active coughing performed during physiotherapy on days 1–3. Interpretation of the size of the correlation was made using the guidelines provided by Akoglu.12 Binomial logistic regression was used to predict if distance walking influenced the development of pulmonary complications. IBM SPSS (V.29.0) was used for the statistical analyses. A p<0.05 was considered significant.
Patient and public involvement
Patients or public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Results
Demographics
During the study period, 364 patients were included in the study. Of those, 179 (49.2%) were from South Africa, see flowchart in figure 1. The demographic data is presented in table 1. The study cohorts from the two countries were significantly different. The patients in South Africa were more often male (Δ 27.4%), were, in mean, 23.3 years younger, had a lower BMI (−3.6 kg/m2), smoked more often (Δ 40.6%), but less frequently had a diagnosed pulmonary disease (Δ −10.2%).

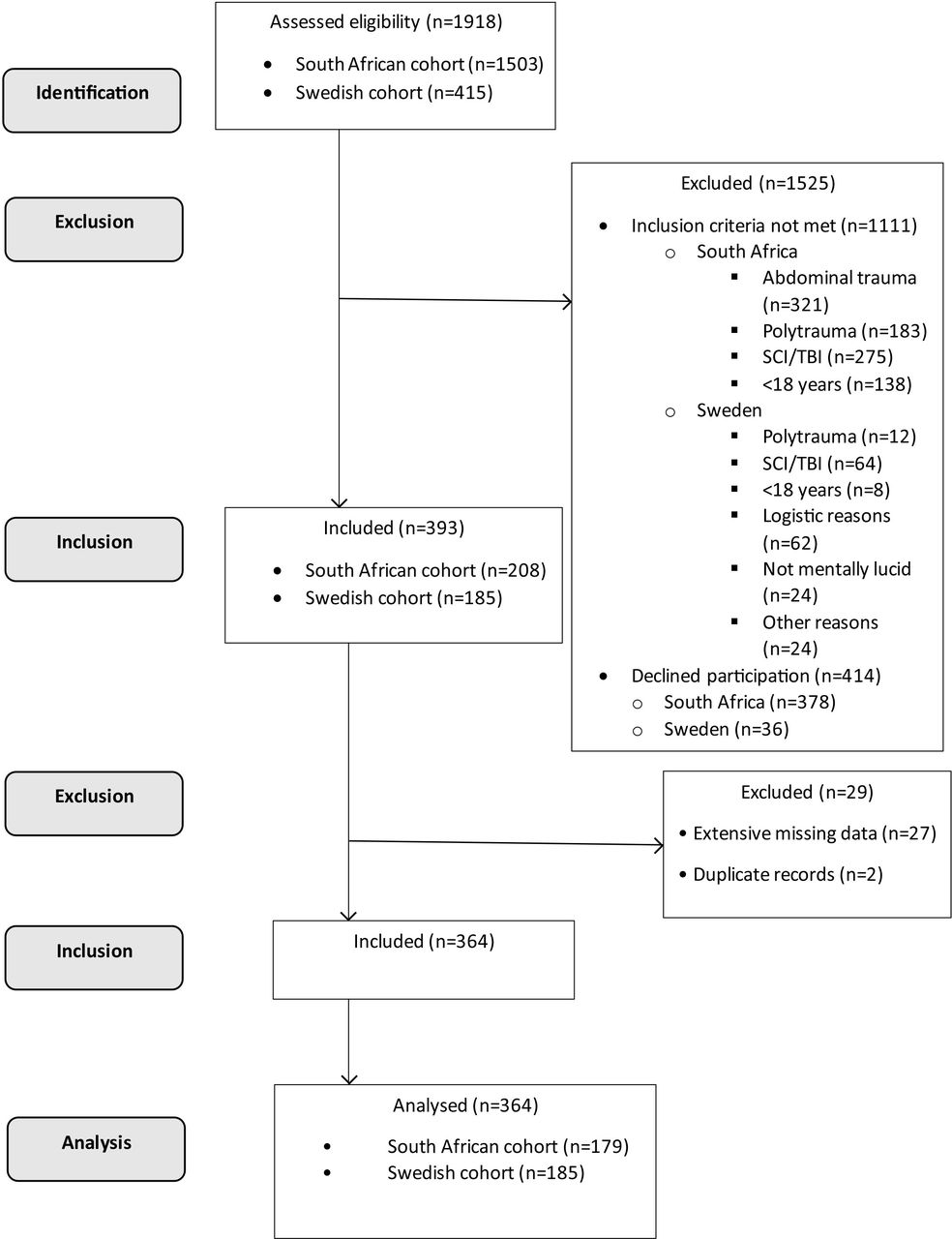{kind=link}
Flowchart of the study. SCI, Spinal Cord Injury; TBI, Traumatic Brain Injury.
Characteristics of all patients included in the trial and divided into the cohort from South Africa and Sweden
Traumas
The traumas differed between the national cohorts (table 2). Penetrating chest injury was more frequent among South African participants (82.7%) and in Sweden, blunt trauma was mostly the cause of injury (94.6 %, p<0.001). The injury with the highest incidence in South Africa was assault (89.9%) and in Sweden, falls (42.1%). The number of patients with rib fractures and flail chest was significantly higher among the Swedish patients (93% and 11%, respectively) while none of the patients from South Africa reported flail chest and 83.8% reported no rib fractures (both p<0.001). In addition, 26 patients in Sweden had sternal fractures compared with none of the patients from South Africa (p<0.001). Most of the participants sustained unilateral haemopneumothorax. As a reflection of the many patients with rib fractures, the proportion of patients with pulmonary contusion was higher in the Swedish cohort compared with their South African counterparts (p<0.001); however, the incidence of lung laceration and diaphragm injury was reported to be low in both groups, with no significant difference. In addition, other types of orthopaedic injuries and mild traumatic brain injuries were also more common in the Swedish cohort (p<0.001). There were no significant differences between the cohorts concerning injured internal organs. Details of the orthopaedic and neurological injuries are presented elsewhere.13
Types and mechanisms of injury sustained n (%)
Physiotherapy intervention used and adverse events
Results concerning physiotherapy interventions given in the two countries are presented in table 3. As there was a large difference regarding type of injury (blunt vs penetrating trauma) between the countries, data was also analysed between these groups and results are given in online supplemental table 1. Most of the patients received physiotherapy treatment during the first 3 days in hospital. A significantly larger group received interventions among the South African cohort on the first day after admission (92.7 vs 73.1%, p<0.001). These patients more often received multiple treatments per day (p<0.001).
Supplemental material
Number and content of physiotherapy treatments on days 1 and 2 after chest trauma divided into the cohorts from South Africa and Sweden
Several respiratory physiotherapy interventions were reported (table 3 and online supplemental table 1). In South Africa, positive expiratory pressure (PEP), active coughing and the active cycle of breathing technique (ACBT) were most often prescribed and in Sweden deep breathing exercises and PEP (p<0.05). Incentive spirometry was used more often in Sweden compared with South Africa. Manual suction, manual or ventilator hyperinflation, intermittent positive pressure breathing or inspiratory muscle training were rarely prescribed.
Exercises to maintain range of motion in the trunk and shoulders were more frequently used in South Africa than in Sweden (shoulder p<0.001 all 3 days: trunk <0.030 day 3). Strength training was performed by a few patients in both countries while exercises in bed were more used, especially on the first day after admission in the Swedish cohort (p<0.001).
Mobilisation to sit on the edge of the bed or to stand at the bedside was significantly more often performed on the first day after admission in South Africa (p<0.001) as was walking away from the bed (p<0.01 day 1–3) (table 3 and online supplemental table 1). None of the Swedish patients climbed any stairs or were cycling on a stationary bike during the first 3 days after the injury in contrast to the patients in South Africa where these activities are used in standard care to evacuate pleural fluid. Mobilisation was, however, included as a frequently used treatment intervention in both countries.
The additional analyses between the type of injury presented the same pattern between blunt and penetrating injury as between the Sweden and South African cohorts (online supplemental table 2).
Supplemental material
Adverse events during the physiotherapy interventions are presented in table 3 and online supplemental table 1. No major adverse events, such as falls or disconnected attachments, were reported. Drop in peripheral oxygen saturation and dizziness were rarely reported. Some patients experienced severe pain during physiotherapy sessions and this was more common in the Swedish cohort.
Pulmonary complications, length of stay, discharge destination and referral to out-patient physiotherapy
Pulmonary complications during hospital stay were rare (table 4). Atelectasis was reported in four patients in South Africa and 16 in Sweden (2.2 vs 8.6%, p=0.007). None of the patients developed pneumonia during the hospital stay in South Africa compared with eight (4.3%) in Sweden (p=0.005). Among the patients in South Africa, seven needed non-invasive ventilation compared with four in the Swedish cohort. In both South Africa and Sweden, three participants needed mechanical ventilation.
Pulmonary complications, length of stay, discharge destination and referral to out-patient physiotherapy
Length of stay was in mean 5.4 (95% CI 4.8, 6.0) days in South Africa and 6.6 (5.8, 7.4) days in Sweden (p=0.024) (table 4). Most patients were discharged to their homes (98.8% in South Africa and 55.7% in Sweden, p<0.001). Thirty-five of the remaining Swedish patients (19%) were transferred to another ward/hospital, 32 (17%) to follow-up rehabilitation and seven (4%) to convalescence care. The out-patient follow-up rate by a physiotherapist was 34.6% in Sweden compared with 1% in South Africa (p<0.001) (table 4).
The type of injury (blunt or penetrating) was compared with the development of pulmonary complications (yes or no). The results showed that the type of injury was associated with the development of pulmonary complications (p=0.04) with blunt trauma having a weak negative correlation (Phi=−0.159) with pulmonary complications. Deep breathing exercises and active coughing were not associated with the development of pulmonary complications. Distance mobilised away from the bedside also had no effect on the development of pulmonary complications.
Discussion
Chest injuries occur all over the world and affect many patients each year. Despite this, there is limited evidence of the treatment and care provided to these patients. Pain is often reported after this kind of injury, especially when ribs are fractured.10 The risk of pulmonary complications is therefore high, and such complications ought to be prevented and treated.5 6 There are only a few previous reports evaluating very specific practices.8 9 In these reports, specific interventions with patients having had penetrating trauma with no or minor injuries to the ribs were included. These patients were also common in the South African cohort in the current trial. Such injuries were mostly seen following assaults on younger men. Penetrating trauma in the South African context is often seen in young male working-class individuals and is linked to alcohol abuse and interpersonal violence.14 The Swedish cohort was, on average, more than two decades older, and their trauma panorama differed significantly. In the Swedish cohort, falls were more often the reason for the injury, resulting in blunt trauma which caused more fractured ribs and more often internal injuries. Differences which probably all have a different impact on the physiotherapy given.
Most of the included patients were given physiotherapy. As earlier trials and guidelines are lacking there is no possibility to compare current routines to earlier evidence. Instead, the rationales behind the treatments should be discussed. For patients with penetrating trauma to the thorax, the pleura and lung parenchyma are often injured. The parenchyma has no pain receptors, in contrast to the pleura, which is innervated by several intercostal nerves.15 Air and blood in the pleural space as well as intercostal drainage tubes compress and irritate the intercostal nerves, leading to inflammation and pain.15 Blunt injuries more often lead to rib fractures and subsequent injuries to thoracic and abdominal tissue and organs. It is well known that rib fractures are painful, and patients therefore breathe more shallowly and avoid huffing and coughing and being active. The aim of the physiotherapy intervention is to increase tidal volume but also the ability to huff and cough. Positioning and mobilisation have an instant effect on lung function by increasing functional residual capacity and tidal volume as the body moves from a reclined to an upright position.16 Mobilisation is therefore an important cornerstone of increasing lung volume. The increased volume but also the activity per se lead to aeration of (partly) collapsed airways which may facilitate the removal of retained secretions. If the effect is not enough, additional deep breathing exercises may be necessary. Ordinary deep breaths, without any devices, increase tidal volume during the treatment but their long-term effects are not known. There are also devices to encourage maximal inspiration, such as incentive spirometry. By using such a device, the inspiration may be slower and therefore less painful. Positive expiratory pressure is another group of techniques and devices that not only increase the tidal volume but also, after specific instructions, increase functional residual capacity.17 According to the results of the current trial several interventions were used, and PEP was the most common. However, there are also differences between the countries in practice. In South Africa, ACBT is common, in contrast to Sweden where the structured breathing cycle is often unknown. On the contrary, in Sweden, incentive spirometry is more common. The use of devices and equipment entails costs that may have had an impact on the practice.
Another aim of physiotherapy practice is to accelerate the removal of fluid from the intrapleural space. This is performed as normal practice in South Africa.6 8–10 Encouraging high-intensity out-of-bed activity leading to deep breathing to expand lung parenchyma, increases intrathoracic pressure and subsequently drainage of fluid into the evacuation systems. It is also necessary to regularly perform supported huffing or coughing when needed. These activities are combined with active trunk movements and stair-climbing and cycling to move the pleural fluid and pressure it towards the evacuation system. In Sweden, no specific instructions are given on how to affect the intrapleural fluid. As found in the results, the Swedish patients started their PEP later than patients in South Africa. The reason may be the practice of pleural drainage and over-cautiousness. Pneumothorax is a relative contraindication for PEP. Therefore, when pneumothorax is diagnosed treatment is often postponed until a drainage system is inserted.
The number of treatments provided in the two countries differed significantly (p<0.001). In South Africa, the nurses per patient ratio is lower in surgical or trauma wards than in Sweden. This influences the level of involvement of nurses and the need for patient education to perform their physiotherapy treatment. In Sweden, physiotherapists more often prescribe the interventions and assist the patients to perform them, but the nurses are actively involved in the treatment to further assist the patients. The patients often also perform their breathing exercises on their own initiative.
A significant association was found between the type of chest injury and the development of pulmonary complications. Atelectasis is a common complication following chest wall injury18 as are pneumonia and respiratory failure, especially in older adults.19 This supports the higher incidence of pulmonary complications in the Swedish cohort who predominantly had blunt chest trauma.
The Swedish patients were significantly more often referred to a physiotherapist for a clinical follow-up after discharge. The reason is unknown, but that cohort of patients was older, had more rib fractures, and also other trauma injuries and further rehabilitation may therefore be needed because of these. Evidence suggests that those recovering from serious chest trauma have chronic pain and limitations in muscle power, active range of motion of the shoulders and trunk, and exercise capacity, which influences their health-related quality of life for up to 6 months and in some cases more than 1 year following hospital discharge.20–22 Neuropathic pain results in significantly poor health-related quality of life, especially for those with blunt chest trauma.23 This underscores the importance of ongoing physiotherapy management of patients’ neuromusculoskeletal impairments beyond hospital discharge, as they recover from chest trauma.
Clinical care protocols implemented in the respective South African sites for the management of chest trauma include intravenous analgesia, oxygen therapy, nebulisation therapy when needed, mechanical ventilation if indicated, management of associated injuries and active physiotherapy.24 The uptake of active physiotherapy was demonstrated by the findings of the South African centres, indicating alignment with the multidisciplinary care pathway protocol in use at these centres. The beneficial effect of multidisciplinary care pathways in the management of rib fractures as a means of reducing the risk of pulmonary complications for example, pneumonia, was recently published.25 Additionally, an international consensus paper regarding recommendations for respiratory physiotherapy and physical rehabilitation in patients with blunt chest wall trauma has recently become available for review to assist clinicians with decision-making and treatment selection during clinical practice.26 This consensus paper emphasises the importance of early physiotherapy interventions focused on lung volume expansion and removal of retained secretions. Physiotherapists in the current study used ACBT, deep breathing and active coughing in their patient management from day 1 of admission, which resonates with these recommendations.26 The South African physiotherapists mobilised most of their patients out of bed on day 1 after admission and included upper limb range of motion exercises for rehabilitation. These interventions conform to the expert consensus paper that states very early out of bed exercises and upper limb exercises should form part of rehabilitation for patients with chest trauma without fractures to the upper limbs.26
There were only minor adverse events reported from the treatments in the current study. Desaturation was reported in some patients and almost all cases occurred during the first day after the trauma. Dizziness and excessive pain were reported by some patients. There were no reports of falls or pneumothorax. Even if this study was not large enough to fully explore adverse events, the received message is that it seems to be safe when treatment is given according to standard practice. However, the excessive pain may have influenced the physiotherapy given and the patients’ adherence to prescribed self-training which subsequently may have had an impact on recovery.
Strengths and limitations
There are both strengths and limitations of this study. One strength is that data for both cohorts were collected in government funded university-affiliated public hospitals in both countries, thus reflecting the normal flow of patients. These two cohorts might however reflect a more injured population compared with county hospitals in Sweden and regional hospitals in South Africa where those with minor trauma are treated. The data was prospectively collected to mirror the actual clinical practice at the participating sites but some of the patients who fulfilled the inclusion criteria were never recruited due to logistical reasons. Those patients may have been missed during the screening of the respective wards and/or not referred by the multidisciplinary team. In addition, the patients may already have been active on the ward when screening took place and the need for physiotherapy intervention was deemed not necessary. Another strength is that two different cohorts were merged to give the opportunity to analyse subgroups for instance comparing physiotherapy management following blunt and penetrating trauma.
There are also limitations to the study. The study cohorts were significantly different between the countries. The patients in South Africa more often had penetrating trauma with different outcomes than the Swedish patients. Therefore, additional analyses of the differences between the types of injury were performed. The management of the patients in the six hospitals in the two countries also varied and the accuracy of reported data may therefore be questioned. Data regarding physiotherapy interventions was self-reported, which may have impacted the objectivity. In two of the six participating hospitals no regular weekend physiotherapy service was provided. The remaining four hospitals offered a limited physiotherapy service on weekends. This led to limited or no screening for potential participants or inclusion in the study during the weekends. In addition, no participant data was collected during the weekends or service delivered. That patients arriving in the end of or during the weekend did not receive the treatment the other patients received is a shortcoming and needs to be addressed in future trials. Therefore, evaluations and treatments were neither optimally performed nor reported. There was a large amount of missing data for distance mobilised and the use of active coughing during physiotherapy sessions. Moreover, standards for defining/specifying atelectasis and pneumonia might differ between the different settings and countries. All of the above may limit the interpretation and generalisability of the findings. Finally, a limitation was the inclusion period performed during the COVID-19 pandemic which may have had an impact on patient recruitment and flow and care provided.
Conclusion
This study shows that there are differences in physiotherapy practice between the two countries of South Africa and Sweden. The results can partly be explained by the fact that the cohorts differed, both regarding types and mechanisms of injuries and the age of the patients in the two countries. In addition, this study shows international differences in methods, where physiotherapy interventions begin earlier and more interventions with high intensity and active movements are used by physiotherapists in South Africa.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by South Africa- the University of the Witwatersrand Human Research Ethics (Medical) committee (clearance number: M200222), Sweden-Regional Ethics Committee for the region of Västra Götaland (clearance number: Dnr2019-04848).
Footnotes
Contributors MFO and HVA had full access to all the data in the study and was responsible for the integrity of the data and the accuracy of the data analysis. Concept and design: MFO, MSe, AS, RR, MSl, AS-R and HVA. Acquisition and analysis: MFO and HVA. Interpretation of results: MFO, MSe, AS, RR, MSl, AS-R and HVA. Critical revision of the manuscript: MFO, MSe, AS, RR, MSl, AS-R and HVA. Statistical analysis: Statistical consultants, MFO and AS-R. Guarantor: MFO.
Funding This work was supported by the National Research Foundation of South Africa under grant [141963] and by the Swedish state under the agreement between the Swedish government and the county councils, the ALF-agreement under grant [ALFGBG-718811].
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.