Article Text

Abstract
Introduction Pulmonary complications frequently occur as comorbidities in individuals with transfusion-dependent thalassaemia (TDT). Despite their clinical significance, the existing literature lacks a systematic review and meta-analysis examining the prevalence and risk factors for pulmonary dysfunction in this patient cohort. Therefore, we propose to conduct a systematic review and meta-analysis to report the prevalence and associated risk factors of pulmonary dysfunction in TDT patients.
Methods and analysis This systematic review and meta-analysis will adhere to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols guidelines. We will search PubMed, EMBASE, the Cochrane Library, Scopus and Web of Science to identify English-language literature from the inception of each database up to 31 May 2024. We will include studies that involve TDT patients and report on the method of pulmonary function assessment, the proportion of pulmonary dysfunction and the analysis of risk factors for pulmonary dysfunction. The study designs included will be cohort, case-control and cross-sectional studies. Exclusions will apply to studies on non-TDT or patients with other diseases, reviews, case reports and animal experiments, as well as duplicated published studies, studies without full-text availability or studies from which raw data cannot be extracted. The screening process, including title, abstract and full texts, will be conducted independently by two reviewers. Data extraction will be performed following standardised protocols. The quality of the included studies will be assessed using the Newcastle-Ottawa Scale and the Agency for Healthcare Research and Quality criteria. The meta-analysis will be conducted using Stata 14.0 and Review Manager (RevMan) 5.4 software, incorporating subgroup analyses, heterogeneity assessments and publication bias evaluations to ensure the robustness and reliability of the findings.
Ethics and dissemination As the data for this systematic review and meta-analysis are sourced exclusively from previously published literature, there is no requirement for ethical approval. The dissemination of the results will occur through publication in a peer-reviewed scholarly journal and presentations at relevant scientific conferences.
PROSPERO registration number CRD42024504353.
- Health
- Pulmonary Disease
- Meta-Analysis
- HAEMATOLOGY
- Anaemia
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
Employing a broad search strategy encompassing various databases and applying the application of standardized quality assessment instruments facilitates rigorous and uniform data analysis.
The engagement of two independent reviewers in data extraction and quality appraisal significantly reduces the potential for bias, thereby bolstering the reliability of the study.
We plan to conduct subgroup and sensitivity analyses.
The review is limited to paper reported in English.
Introduction
Transfusion-dependent thalassaemia (TDT) is a prevalent single-gene hereditary disorder characterised by an imbalance in globin synthesis, leading to clinical manifestations such as anaemia, haemolysis and ineffective erythropoiesis.1 It poses a significant public health challenge, with thalassaemia gene carriers estimated to be 1%–5% of the global population,2 highlighting the scale of this health issue.3–5 Patients are classified based on their blood transfusion dependency into TDT and non-TDT (NTDT). TDT patients typically present with more severe symptoms and rely on regular blood transfusions for survival, imposing a considerable economic burden on both the patients’ families and healthcare systems.6 Moreover, recurrent transfusions, increased intestinal iron absorption and haemolysis in TDT patients can lead to secondary iron overload, causing excess iron deposition in various organs and consequent organ dysfunction.7
Pulmonary dysfunction, encompassing ventilatory impairments (obstructive, restrictive and mixed) and diffusion abnormalities, can arise from diverse pathologies. TDT patients are at an increased risk of pulmonary dysfunction for several reasons. Extramedullary haematopoiesis can induce hepatosplenomegaly and atypical thoracic morphology, limiting respiratory movements. Additionally, splenectomy in TDT patients may lead to hypercoagulability, increasing the risk of microthrombi formation in the pulmonary vasculature, which can obstruct the air-blood interface.8–10 Iron overload can also result in iron deposition within the lungs, potentially causing tissue damage,11 and animal studies suggest that such accumulation may induce pulmonary fibrosis.12 Notably, impaired pulmonary function is independently associated with increased overall and cardiovascular mortality.13–15 Given that cardiovascular complications are a leading cause of death in TDT patients, understanding the prevalence and risk factors of pulmonary dysfunction is crucial for early detection and management.
Keens et al first reported pulmonary dysfunction in TDT patients in 1980.16 Several studies have emerged over the subsequent four decades, yet there is a lack of large-sample studies in the existing literature. The reported prevalence of pulmonary dysfunction varies widely,17 18 and there is no consensus on the risk factors, with conflicting results among studies.18–20 This study aims to determine the prevalence of pulmonary dysfunction and its risk factors in patients with TDT.
Methods and analysis
Study design
The protocol for this study was registered in the PROSPERO database on 13 June 2024 (registration ID CRD42024504353). The study adheres to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols statement21 and the Meta-analysis Of Observational Studies in Epidemiology reporting guideline.22 Any amendments to the protocol will be documented, and the rationale for these changes will be updated on the PROSPERO platform.
Review questions
What is the prevalence of pulmonary dysfunction in patients with TDT?
What risk factors are associated with an increased prevalence of pulmonary dysfunction in patients with TDT?
Data sources and search strategy
We will search PubMed, EMBASE, the Cochrane Library, Scopus and Web of Science to identify English-language literature from the inception of each database up to 31 May 2024. The search strategy will utilise a combination of Medical Subject Headings terms and free-text keywords, including ‘pulmonary dysfunction’, ‘respiratory function’, ‘respiratory performance’, ‘prevalence’ and ‘thalassaemia’. Although ‘transfusion-dependent thalassaemia’ is theoretically a more specific term, ‘thalassaemia’ will be used to broaden the search and maximise the retrieval of relevant articles. The full search strategy is outlined in box 1.
Search terms
(“Prevalence” OR “Prevalences” OR “Period Prevalencer” OR “Period Prevalences” OR “Prevalence, Period” OR “Point Prevalence” OR “Point Prevalences”) AND (“Thalassemia” OR “Thalassemias”) AND (“Pulmonary Dysfunction” OR “Lung Dysfunction” OR “Pulmonary Abnormalities” OR “Lung Abnormalities” OR “Lung Function” OR “Pulmonary Function” OR “Respiratory Function” OR “Spirometry” OR “Respiratory Performance”.
Eligibility criteria
Inclusion criteria
Studies involving transfusion-dependent thalassaemia patients.
Reports on the method of pulmonary function assessment, the proportion of pulmonary dysfunction and the analysis of risk factors for pulmonary dysfunction.
Study design—cohort, case-control and cross-sectional studies.
Exclusion criteria
Studies on NTDT or patients with other diseases.
Reviews, case reports and animal experiments.
Duplicated published studies, studies without full-text availability or studies from which raw data cannot be extracted.
Study screening and selection
All relevant literature will initially be exported to EndNote for organisation and de-duplication. Two researchers will independently review the titles and abstracts of the collected literature for initial screening. Subsequently, the full texts of the selected articles will be retrieved and carefully examined. The literature that meets the inclusion criteria will be included in the study. Any disagreements or uncertainties during the screening process will be resolved by consulting a third investigator. The screening flowchart for the study is presented in figure 1.

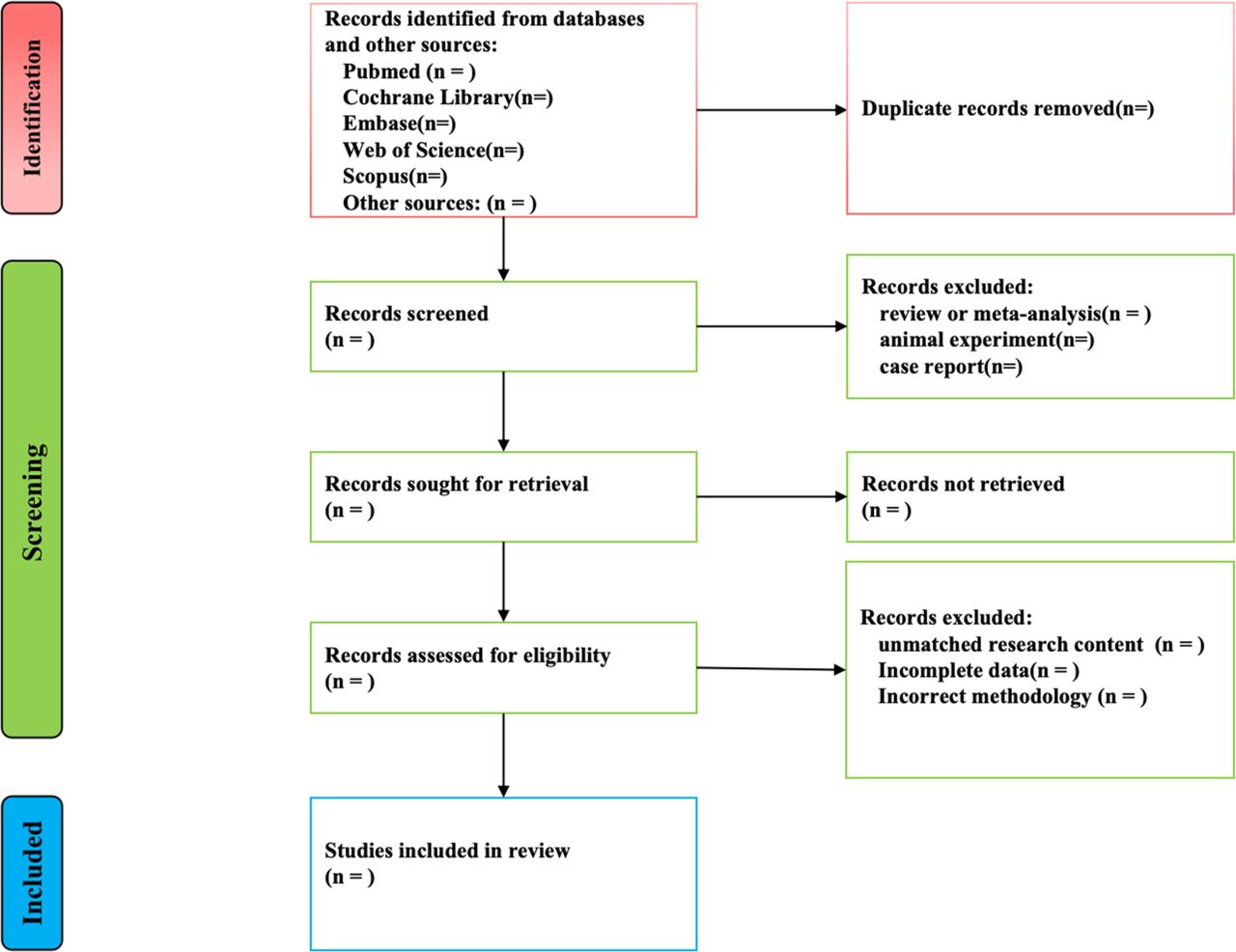{kind=link}
Flowchart for study screening and selection.
Quality assessment
Cohort studies and case-control studies will be evaluated for quality using the Newcastle-Ottawa Scale,23 which consists of the selection of study participants (four entries, 4 points), intergroup comparability (one entry, 2 points) and outcome measurements (three entries, 3 points), with a total score of 9 points, with 0–3, 4–6 and 7–9 points indicating low-, moderate- and high-quality literature, respectively. Cross-sectional research literature will be evaluated using the Agency for Healthcare Research and Quality,24 which consists of 11 entries with a total score of 11. Scores of 0 to 3, 4 to 7 and 8 to 11 indicate low-, moderate- and high-quality literature, respectively. The evaluation of the quality of the included studies will be done independently by two researchers. In case of disagreement, it was adjudicated in consultation with a third researcher.
Data extraction and management
Data extraction will encompass:
Type of study: to understand the design and methodology and ensure correct analytical methods.
Country or region: to consider the potential influence of geographical factors on the prevalence of pulmonary dysfunction.
Number of patients: reflecting the sample size and its impact on study persuasiveness.
Patient demographics: including age, gender, height, weight and body surface area.
TDT characteristics, such as genotypes, haemoglobin levels, serum ferritin, liver iron concentration, grading of iron deposition in the liver and heart, hepatomegaly, splenomegaly, splenectomy, blood transfusion and iron chelation therapy.
Lung function assessment methods: to understand the methodology and facilitate comparison of results across studies and spirometry data.
Prevalence of pulmonary dysfunction: the most direct indicator of the prevalence in the study population.
Predictors of pulmonary dysfunction: to identify potential causative or correlative factors.
Statistical analysis
Statistical analyses will be conducted using Stata14.0 software. We will assess statistical heterogeneity among studies using Cochran’s Q test and the I2 statistic. A significant heterogeneity will be defined if the Cochran’s Q test yields a p value <0.05 and the I2>50%. In such cases, a random-effects model will be employed; otherwise, a fixed-effects model will be utilised. Publication bias will be assessed using the trim and fill method, Begg’s test and Egger’s test. Subgroup analyses and meta-regression will be conducted to explore potential sources of heterogeneity and to evaluate the consistency of the findings.
Data synthesis strategy
We will use Revman V.5.4 software for data synthesis analysis. The pooled prevalence estimates of pulmonary dysfunction in TDT patients, along with their associated 95% CI, will be calculated. Additionally, the OR and their corresponding 95% confidence interval will be determined for factors linked to the prevalence. The results of the meta-analysis will be displayed in forest plots to provide a clear visual representation of the data. In cases where meta-analysis is not viable due to a lack of homogeneity among studies, we will employ a narrative synthesis to synthesise the findings.
Subgroup analyses
Subgroup analyses will be conducted to comprehensively understand the relationship between TDT and pulmonary dysfunction. These analyses will be stratified by age (adolescents and adults), serum ferritin levels (≤2500 ng/mL and >2500 ng/mL) and the extent of hepatic and cardiac iron deposition (none, mild, moderate and severe).
Sensitivity analyses
Sensitivity analyses will be performed to assess the robustness of the meta-analysis outcomes. This will involve systematically excluding one study at a time and re-conducting the meta-analysis to determine if the exclusion of any particular study significantly affects the overall results. Additional sensitivity analyses may be conducted considering variables such as study quality, sample size or other potential confounding factors that could influence the outcomes.
Patient and public involvement
None.
Ethics and dissemination
As the data for this systematic review and meta-analysis are sourced exclusively from previously published literature, there is no requirement for ethical approval. The dissemination of the results will occur through a publication in a peer-reviewed scholarly journal and presentations at relevant scientific conferences.
Discussion
This systematic review and meta-analysis aim to contribute to the existing body of literature by synthesising findings from a diverse array of studies and patient populations. By integrating data across various studies, we will gain a more nuanced understanding of pulmonary dysfunction in TDT patients, underscoring the necessity for personalised clinical strategies. Furthermore, the review is anticipated to reveal gaps in current research, guiding future investigations. Prospective studies may benefit from exploring the impact of pulmonary dysfunction on survival rates, the caregiving burden and the utilisation of healthcare resources within the TDT patient cohort.
This systematic review and meta-analysis will serve as a valuable resource for clinicians, researchers and healthcare policymakers by thoroughly analysing the prevalence and risk factors of pulmonary dysfunction in TDT patients. The findings will not only inform clinical decision-making but also drive the development of evidence-based interventions aimed at improving the health outcomes of TDT patients.
This study has important strengths and limitations. Our protocol employs a broad search strategy encompassing various databases, which is crucial for ensuring a comprehensive and exhaustive literature search. The engagement of two independent reviewers in data extraction and quality appraisal is a significant strength of our protocol. This dual-review process significantly reduces the potential for bias, as it allows for cross-checking and consensus on the data and quality assessment. The plan to conduct subgroup and sensitivity analyses is another strength of our protocol. These analyses will allow us to explore potential sources of heterogeneity and assess the robustness of our findings. Despite these strengths, our protocol has a limitation in that it confines the inclusion of papers to those published in English. This language constraint may impact the reliability of our conclusions by potentially excluding valuable studies published in other languages, which could introduce a bias towards English-language literature.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors XL initiated the research question and structured the study framework, assisted by other authors. XL and YLu independently devised the search strategy, engaged in the search process, evaluated the article quality and extracted pertinent data. YH, LP and MW undertook the task of analysing and interpreting the findings. RL and YLai supervised the review. All authors read and approved this protocol before sending it for publication. XL is the guarantor.
Funding This study was supported by the National Natural Science Foundation of China (No.81960028), the Guangxi Zhuang Autonomous Region Health Committee self-funded project (Z2014643) and the Advanced Innovation Teams and Xinghu Scholars Program of Guangxi Medical University.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.