Article Text

Abstract
Introduction The primary caregivers of patients with cancer, especially in advanced stages, experience significant physical and emotional strain and require comprehensive support. Respite care has been acknowledged as an effective strategy to aid primary caregivers, and different models have been established in Western nations. However, implementing these models poses challenges due to notable cultural, social and healthcare system variances between Western and non-Western regions like Iran and other Middle Eastern countries. It is crucial to develop a model tailored to the country’s specific needs, culture and resources to systematically support caregivers and ensure care continuity. Hence, this study aims to develop and validate a respite care model for adult patients with cancer in Iran.
Methods and analysis This study will use a multimethod approach across three stages. In the first phase, a scoping review will be conducted to identify, describe, conceptualise and implement the respite care system based on available documents and evidence. Then, a directed content analysis will be carried out to clarify care requirements and system establishment needs from stakeholders’ perspectives. Data from the scoping review and directed content analysis will be integrated to identify the crucial components of the model using the Delphi method in the second phase. In the third phase, another Delphi study will be conducted to assess the importance, scientific credibility and feasibility of the model, with the aim of finalising it.
Ethics and dissemination This research project has received the code of ethics (IR.TBZMED.REC.1402.720) from Ethics Committee of Tabriz University of Medical Sciences. The findings of this study will be published in reputable journals and disseminated in accessible formats through various media channels.
- Adult oncology
- Nursing Care
- Health policy
- Caregivers
- Research Design
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The multimethod approach, including a scoping review, directed content analysis and Delphi study, ensures the development of a comprehensive context-based respite care model.
Engaging stakeholders through a qualitative study and Delphi rounds ensures that the model is tailored to the actual needs and perspectives of those involved in caregiving and healthcare.
While reliance solely on expert opinions in the Delphi study may introduce bias, the use of a scoping review to gather existing data and evidence provides a solid foundation for the model, ensuring it is grounded in current knowledge and best practices.
Engaging different stakeholders, including patients, formal and informal caregivers, and policymakers, can help collect data using a triangulation method from different points of view, aiding in the development of comprehensive models.
Introduction
Primary caregivers, often family members, relatives or friends, shoulder significant physical, emotional, social or financial caregiving responsibilities.1 While caregiving can foster feelings of value and enhance self-esteem, it can also exert considerable pressure on these individuals.2 With the evolution of end-of-life care, there has been a shift towards providing care in homes,3 4 leading to an increase in the complexity and duration of primary caregiver duties.5 Primary caregivers of patients with cancer, in contrast to caregivers of individuals with other chronic diseases such as dementia, diabetes, or elderly care, often experience a significant decline in their health.6 Consequently, the risk of health decline in these primary caregivers is elevated compared with the general population.7–9 Similarly, cancer caregivers in Iran tackle numerous challenges, including anxiety,10 11 fear of losing a loved one, role conflict, fatigue, burnout,12 13 feeling of hopelessness,14 a sense of absence in life,15 high caregiving burden,15 16 low quality of life10–12 16–18 and financial hardships.10 11 13 18 Therefore, family caregivers themselves also need support from the healthcare system to be able to maintain their quality of life while providing caregiving.19
Respite care is an effective model of care developed to support cancer primary caregivers.20 It is assumed that short-term and timely interruptions in caregiving responsibilities help caregivers provide long-term and effective care.21 This care system allows for a short break in care responsibility, ranging from a few hours to a few weeks, enabling primary caregivers to recharge their energy.22–24
Respite care can have positive outcomes for the patient, primary caregiver, other family members and society.25 26 Primary caregivers view this care model as a necessary way to enhance their quality of life as well as preventing fatigue and burnout,27–29 boosting resilience, alleviating distress and collapse,19 30 reducing stress and caregiving pressure,31 and decreasing patients’ admission to hospices.32
The concept of respite care has been described differently in various healthcare systems.25 32 As a result, respite care delivery models vary across countries and even within countries based on key variables such as environment, scheduling, geographical access, service providers, care approaches and financial arrangements.25 33 34 Research emphasises that respite services should be flexible35 and tailored to community resources and cultures to avoid a one-size-fits-all approach across countries.36 37
In Iran, however, there is limited availability of facilities for offering palliative care,38 39 and no provision for respite care.40 Family caregivers are often overlooked in the Iranian healthcare system, lacking specific support services.41 Nevertheless, researcher experiences indicate that in many cases, other family members try to support primary caregivers and that some caregivers take on responsibilities informally.
The establishment of a respite care model for adult patients with cancer in Iran is essential, as there are currently no standard protocols for such care in the country or the Eastern Mediterranean region, according to conducted searches.40 The proposed models for respite care are primarily based on advanced countries, which differ significantly from Iran and other Middle Eastern countries in terms of human and non-human care resources,19 42–44 as well as social, cultural and socioeconomic settings.25 33 Studies conducted emphasise the necessity for care models that are customised to the distinct cultural, social and health needs of patients with cancer and their caregivers in Iran.45–47 This protocol addresses this gap by providing a comprehensive and multifaceted approach to respite care, serving as a foundational framework for research and implementation in similar contexts. With the release of this protocol, our goal is to encourage the reproduction and adaptation of the final model, ultimately improving the quality of life for patients with cancer and their caregivers.
The necessity of employing a multimethod approach in presenting research protocols for cancer respite care is underscored by the complexity of cancer care dynamics and the diverse needs of patients and caregivers.48 A multimethod framework allows for the integration of various data, thereby offering a comprehensive understanding of the experiences and challenges faced by individuals dealing with cancer.49 This approach not only facilitates the triangulation of data, enhancing the validity and reliability of findings, but also enables researchers to capture the nuanced perspectives of participants, which are essential for designing effective respite care interventions.50 By addressing the multifaceted nature of cancer care through various methodological lenses, researchers can better inform practice, policy and future studies, ultimately leading to improved quality of life for patients and their families.
Objective
The aim of this study is to offer methodological protocol for the development and validation of the respite care model for adult patients with cancer in Iran. The steps in this protocol will include the following:
Phase 1
Identifying, describing, conceptualising and implementing the cancer respite care system by reviewing relevant studies and other sources (scoping review).
Exploring perspectives of different stakeholders (including healthcare providers, patients, primary caregivers, policymakers and experts) on care requirements of primary caregivers for patients with cancer in Iran, especially their involvement with informal respite care.
Phase 2
Developing the initial model by integrating data gather from phase 1 and identifying the crucial components of the model.
Phase 3
Validating and finalising the model by determining the importance, scientific credibility and feasibility of the developed model using the Delphi method.
Methods and analysis
Design
A multimethod research methodology has been selected to conduct this study. This approach helps researchers to use more than one research method in one study.51 Unlike the mixed method, this approach is not restricted to combining quantitative and qualitative methods but allows for a wide range of methodological combinations.52 Multimethod research provides creative and opportunistic insights to thoughtful and prepared minds.52
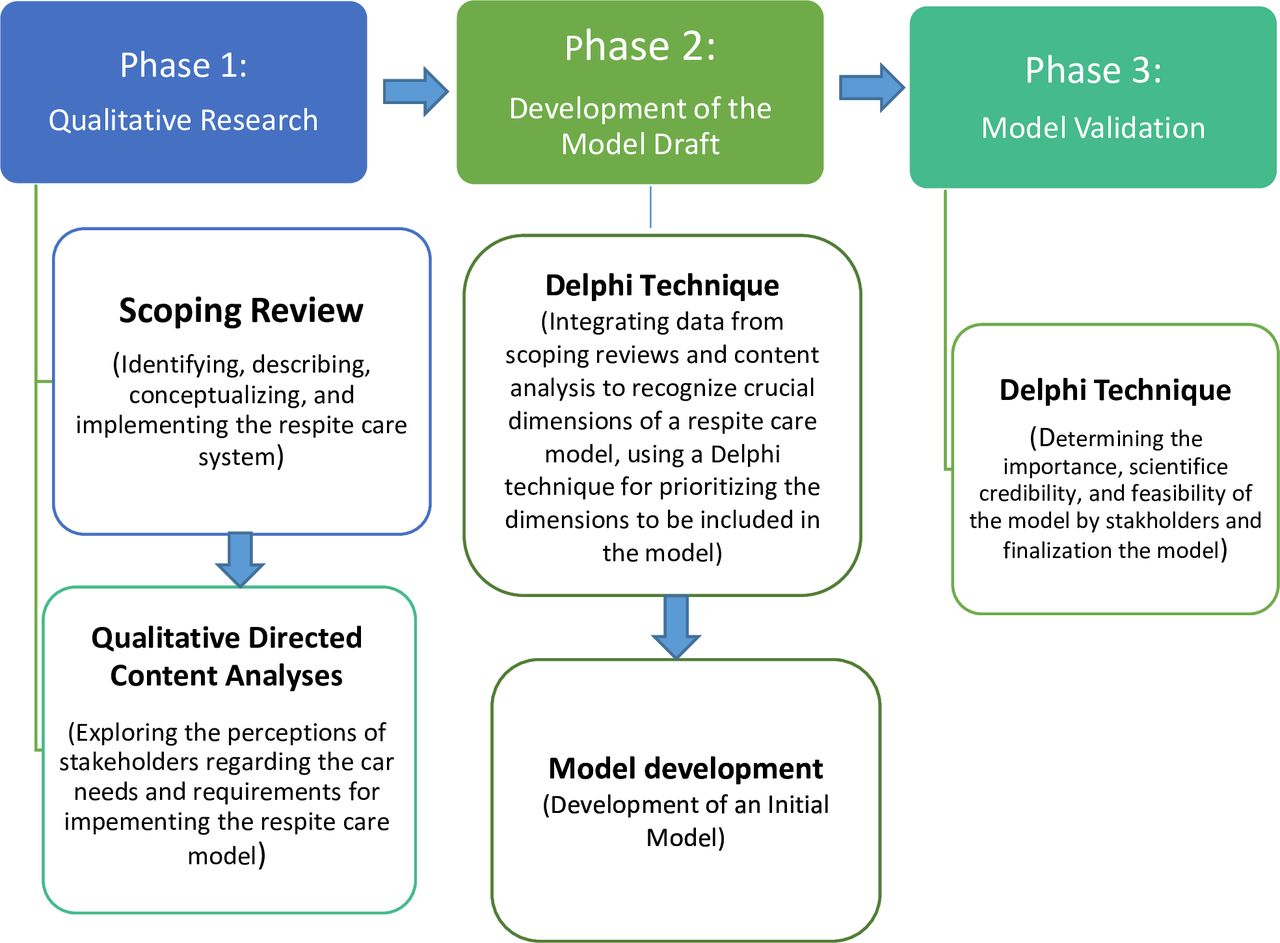
According to the stated reasons and considering the objectives of this study, multimethod approach is suitable for conducting this study. This research will be conducted in three phases. The first phase, consisting of two sections, aims to collect data on existing respite care models (scoping review) and gather experiences from all stakeholders involved in the care of patients with cancer in Iran (patients, primary caregivers, healthcare personnel and policymakers). The second phase aims to develop a draft of the model. Finally, the third phase will focus on validating the developed model using the Delphi technique (Figure 1). The research project will span 24 months, beginning on 20 January 2024. During this time, we will gather and analyse data and publish our findings.

{kind=link}
Research methodology steps.
Setting
This study will take place in the city of Tabriz, a metropolitan city in the northeast of Iran. The research setting encompasses all locations where study participants, including patients, primary caregivers, healthcare personnel and policymakers, are present. This includes patients’ homes, public and private outpatient and inpatient medical centres, physicians’ offices and the Iranian Ministry of Health and Medical Education (MOHME). Additionally, some non-profit centres support patients with cancer by providing free medical, counselling and supportive services to patients and their families.53 54
Phase 1: qualitative research
Scoping review
To achieve the primary goal of ‘identifying, describing, conceptualising and implementing the respite care models in cancer care through a review of studies and resources’, a scoping review will be conducted. This initial step will enable access to the best available evidence, resulting in time and resource efficiency. According to the objective of scoping review, the questions that can be answered by this method are those by which researchers map, explore and document the range of existing knowledge about a phenomenon.55 As opposed to systematic review, scoping review studies tend to address broad topics where many study designs are applicable.56
A preliminary search of MEDLINE, the Cochran Database of Systematic Reviews and Joanna Briggs Institute (JBI) Evidence Synthesis revealed no current or prospective systematic reviews or scoping reviews on this topic.
At this stage, scoping review will be conducted in accordance with JBI methodology for scoping reviews.57
In 2023, research titled ‘Respite care models and practices for persons with intellectual disability: A scoping review’ was published. While that study aimed at designing a model for individuals with intellectual disabilities, our focus is on developing a model for individuals with cancer.58
Review question
To identify scoping review questions, we will use the PCC (Population, Concept, Context) protocol: ‘How is the comprehensive model of cancer respite care defined, conceptualised and implemented in studies?’ This general question guides the specific questions as follows:
How are different types of formal and informal cancer respite care described, conceptualised and implemented in studies and other sources?
How effective, experiential and satisfactory is cancer respite care?
What are the policies in the field of cancer respite care (laws, policies, guidelines and protocols)?
Eligibility criteria
Eligibility criteria based on PCC framework are outlined as follows:
Articles and documents published in the field of cancer in the age group over 18 years, as well as studies that include cancer alongside other populations.
Evidence entries addressing respite care either separately or as a service package (including respite care).
Evidence that provides respite care at home, in hospitals, and other community settings.
Exclusion criteria
The following exclusion criteria will apply:
Lack of relevant information on respite care.
Invalid content and documents (eg, blogs, online journals that are not peer-reviewed, and absence of author names and addresses).
Studies related to respite care for children.
Types of sources
To access the literature, researchers will systematically search selected data sources. The search strategy will involve electronic databases, reference lists, manual searches of key journals, government websites, other important national and regional websites related to organisations active in cancer care, the WHO’s website, scientific and administrative documents and reports from relevant organisations, cancer specialist journals and other printed materials.
Search strategy
A three-step search strategy will be implemented in accordance with the JBI Reviewer’s Manual.57 The bibliographic databases that to be searched include (but are not limited to) MEDLINE (via OVIDSP), PubMed, EMBASE (www.embase.com), CINAHL (via EBSCO), Cochrane Library, Psych INFOInfo (via EBSCO), Scopus and Web of Science. Supplementary searches will be conducted using Google Scholar to identify any additional studies. Grey literature, reference lists of the included studies and those of relevant reviews will be tracked. A forward citation search will be performed. There will be no restrictions on publication date or language. The main search terms include (but are not limited to) ‘respite care’, ‘short-term care’, ‘daycare’, ‘caregiver relief’, ‘cancer’ and ‘palliative care’. Additional related keywords will be selected according to the aims and questions of the scoping review. The search strategy will incorporate both free text and controlled vocabulary related to selected keywords. A draft search strategy of PubMed is presented in online supplemental appendix I.
Supplemental material
Data extraction
The study selection will be a two-step screening process, starting with a title and abstract screening, followed by a full-text review. In both stages, two independent reviewers (NK and VP) will assess the articles against the established eligibility criteria. Any discrepancies will be resolved through discussion. If a consensus cannot be reached, a third reviewer (AR) will be consulted. Eligible studies will be determined based on the criteria outlined in 'PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for scoping reviews flow diagram).
In the initial step, titles and abstracts of references will be screened using Rayyan platform, a software application tailored for researchers conducting systematic literature reviews and meta-analyses. All identified results from various databases will be entered into the Rayyan platform where duplicates will be identified. The screening stages will be conducted independently by researchers based on title and abstract.
We will include all primary studies, such as experimental, observational and qualitative investigations. Systematic reviews will also be considered for inclusion. The full texts of the included studies will be obtained, and their citation details will be imported. Excluded studies will be outlined in a ‘characteristics of excluded studies’ table, with reasons for their exclusion noted. The final list of included studies will be confirmed by two review authors to facilitate data extraction, specific forms have been designed to capture relevant information from the selected evidence. The research team will determine what information from the available literature should be extracted to answer the research questions. Extracted data will encompass various study characteristics, namely author, publication date, journal type, study location, aim, design, study type, sample size and key findings.
Data analysis and presentation
Whereas a scoping review requires analytical frameworks or thematic structures to present a valid report on existing literature, it does not aim to evaluate the strength of evidence regarding interventions or specific policies. It does not assess the quality of evidence and cannot determine whether specific studies provide strong or generalisable findings.59 Instead, data relevant to the objectives and questions of the scoping review will be extracted, including information on the concept of respite, identification and description of types of respite settings, mechanisms of financial support, training and provision of care providers, care required in respite, experiences and attitudes towards respite care, and policies concerning respite care.
In this research, after extracting and charting the data and key items, the study results will be summarised and the data will be categorised. The process of reviewing and examining the categories will continue until all main categories are established. This process will be repeated until all primary categories are identified. To present the data effectively, tables and diagrams will be used.
Directed content analysis
A qualitative study will be conducted using directed content analysis to achieve the second goal, namely elucidating the perceptions of key stakeholders (caregivers, patients, care providers, stakeholders and policymakers) regarding the requirements, barriers and facilitators of implementing a respite care system for patients with cancer.
Qualitative content analysis is a method for analysing texts.60 61 The complexity of meaning, holistic perspective and relevance of content to the context are reasons why content analysis can be employed as a qualitative research method.62 In this approach, researchers identify key concepts or variables as initial coding categories based on previous research and subsequently defines operational definitions for each category.63 In this study, a content analysis will be performed based on the 16 stages of the Assarroudi model, and the steps will be detailed below.64
Participant characteristics
General inclusion criteria:
Ability to communicate verbally and answer questions during the interview accurately.
Willingness to participate in the study and consent to be interviewed.
No history of significant mental disorders (psychosis) or hospitalisation in psychiatric wards (as reported by participants
Caregivers inclusion criteria:
Primary caregiver of patient with cancer.
Having direct caregiving experience of patient for a minimum of 6 months.
Knowing the diagnosis, treatment process and patient’s condition.
Over 18 years of age.
Patients inclusion criteria
Patients with a confirmed diagnosis of cancer (regardless of cancer type).
Knowing about their diagnosis, treatment process and current condition.
18 years and older.
Health care providers inclusion criteria:
Healthcare providers include doctors, nurses, psychologists and caregivers who have at least 1 year of experience in caring for patients with cancer.
Health experts and policymakers inclusion criteria
Having expertise in one of the fields of health sector management
Having a management position in centres such as Cancer Department of MOHME, Cancer Registration Centers, research centres and cancer-related NGOs (Nongovermental organizations).
Among healthcare providers, experts and policymakers, those with experience in caring for patients with cancer have priority for selection.
Recruitment
To select patients, primary caregivers and care providers, the researcher (NK) will be present in the research environment to identify eligible participants based on inclusion criteria. The selection of participants from among policymakers and experts will also be done with the guidance of mentors, advisors and officials of relevant centres. Researchers in the field of cancer and palliative care will also be recognised through their research backgrounds. Considering maximum diversity in sociodemographic and phenomenon characteristics, the participants will be chosen from the research community based on goal-oriented, snowball and convenient sampling methods. Sampling will end when information reaches saturation or, in other words, when all aspects of the phenomenon under study are thoroughly examined and no additional data emerges in subsequent interviews.
Data collection/analysis
Linking raw data with predetermined categories is a significant matter in directed content analysis. To address this issue, Assarroudi developed Elo and Kynga’s (2008) three-step data collection and analysis method.64 This method consists of three stages: preparation, organisation and reporting, which are practically carried out in 16 steps. Therefore, in this research, these 16 steps will also be used (table 1).64
The summary of the steps for conducting content analysis according to Assarroudi
Rigor in content analysis
To enhance the reliability of directed content analysis studies, researchers must clearly define the three stages of ‘preparation’, ‘organisation’ and ‘reporting’.65 These stages are necessary to demonstrate how data categories are developed.62 65 For this purpose, appendices, tables and figures can be used to illustrate the reduction process.66 Furthermore, an honest report of various facts during data analysis should be presented. According to Assarroudi, adopting this 16-stage method can increase the reliability of directed content analysis.64
This study demonstrates rigor through its clear objectives, systematic methodology, comprehensive participant criteria, diverse recruitment strategies, thorough data collection and analysis processes, intercoder reliability checks, ethical considerations and detailed reporting practices. These elements collectively contribute to the credibility and trustworthiness of its findings regarding stakeholder perceptions in respite care for patients with cancer.
Phase 2: development of the model draft
This phase of the study aims to develop the initial model by integrating data to determine the key components of the model. The conceptual framework for the respite care model will be developed inductively through a content analysis of data collected from the scoping review and interviews. Inductive conceptual framework is a conceptual model, based on empirical data, that explains the research findings and demonstrates how inductive concepts link together to understand the study phenomenon.67 To identify the crucial components of the model from the many extracted components, a modified Delphi study will be conducted. Experts will be asked to rate the importance and priority of each component using a Likert scale from 1 to 4. They will be provided with a questionnaire containing all extracted data from both the scoping review and the qualitative study. Experts will then determine the priority of each component to be included in the model using the 1–4 scale.
Delphi is a broad, systematic and flexible method.68 This is a research method meant to assess experts’ judgement in decision-making, prioritisation or making predictions.69 This method serves as a means to gather the opinions of a diverse group of experts on a wide geographical scale, providing feedback without the need for group meetings.70
We are planning to conduct a modified Delphi study. This type of Delphi method is often used when the goal is to gather expert opinions and prioritise components rather than reaching a complete consensus.71 Therefore, instead of aiming for full agreement, the modified Delphi method seeks to identify and prioritise key components based on expert input.71 Typically, it involves multiple rounds of surveys to refine and prioritise the components, but the number of rounds can vary based on the study’s needs.72 For our study, two rounds can be sufficient given that the goal is to gather initial opinions and then refine them. The first round can be used to identify and list the essential components, and the second round can help in prioritising these components based on expert feedback. Of course, we are open to conducting an additional round if the second round does not provide clear prioritisation or if significant new insights emerge. Also, the Delphi rounds are independent rounds rather than repeated ones. The implementation will adhere to the model proposed by Boulkedid.73
Questionnaire for the first round
To enhance the clarity and effectiveness of our study, we will organise the sections and components of the model into structured tables and diagrams within the questionnaires. A comprehensive guide will be developed to assist experts in responding to these questionnaires. This guide will outline the study’s objectives, detail the various components of the initial respite care model and provide clear instructions on how participants can engage with and complete the questionnaires.
Experts
Members of the Delphi panel will include health system policymakers, specialist physicians experienced in cancer and palliative care, university faculty members and nursing specialists with both theoretical and practical training in cancer-related and palliative care courses. Additionally, representatives of patients and caregivers will be included to ensure that their perspectives and needs are adequately represented. By bringing together all these stakeholders, the panel aims to foster collaboration and develop well-rounded recommendations for improving cancer respite care model. Experts will be selected using purposive and snowball sampling technique.
To identify these experts, we will conduct searches on the website of the Educational Deputy of Medical Sciences Universities, the MOHME and healthcare service providers related to cancer. Candidates (with the exception of patients and caregivers) will be required to have at least 5 years of relevant job experience.
The credibility of Delphi method does not rely on the number of participants but rather on the scientific qualifications of the experts involved. Typically, Delphi panels consist of fewer than 50 individuals, with most panels ranging from 12 to 20 experts. This smaller size allows for more focused discussions and facilitates consensus-building among participants.74 On the other hand, if the participants in the Delphi panel are from a similar field (15 to 30) or from different fields (5 to 10) for each specialised group,75 this study will include primary groups of policymakers and specialists from the fields of medicine and nursing, comprising a minimum of 15 participants.
Sending questionnaires: first round
The extracted components of the model will be presented in the form of tables in a survey format using online form software electronically, and the relevant link will be provided to stakeholders via email for prioritisation.
In the first round of the Delphi method, experts will evaluate the necessity and priority of each component (indicator) of the cancer respite care model based on their knowledge and experience. They will use a scoring system that ranges from 1 (indicating the lowest priority) to 4 (indicating the highest priority). At the end of the questionnaires, an open-ended question will invite experts to provide additional comments regarding the various sections of the cancer respite care model (table 2).
Questionnaire sample for a survey regarding the necessity and priority of the respite care model
Using the Delphi technique, complete consensus among participants is not expected, as there is no universally accepted standard for defining consensus. Instead, various metrics, such as percentages and average scores, will be employed to assess agreement.76
The quantitative data from the ratings will be analysed using SPSS software, focusing on descriptive statistics to calculate the mean scores and SD for each indicator. Indicators scoring a mean of 3 or above will be retained in the model. Qualitative responses from the open-ended question will undergo content analysis to identify common themes.
Next rounds
Based on the comprehensive feedback received from both quantitative and qualitative analyses in two rounds, the research team will make informed decisions regarding choosing the most important with high priority components which should be inserted in the model.
The components with the highest priority will be included in a draft, which will then be transferred to the third phase for validation. The model development process will be closely monitored and approved by the research team to ensure rigor and alignment with the study objectives.
Phase 3: model validation
This phase of the study aims to achieve finalised validated model by determining the necessity, importance, scientific credibility and practical feasibility of the developed model using the Delphi method.
The objective of this Delphi is to validate or assess the significance, scientific credibility and applicability of the draft model. The draft model will also be formatted as a questionnaire. This form will be distributed to the same participants from the Delphi (in phase 2) (electronically via web-based form software), and if necessary, other stakeholders will also be invited. To evaluate each component, three criteria—importance, scientific credibility and feasibility—will be taken into account, and participants will be asked to provide their opinions on each component for each criterion separately, using a scale from low (1), medium (2), to high (3) (table 3). Furthermore, an open-ended question will be included for each component.
Questionnaire sample for a survey regarding the validity of the respite care model
To facilitate responses, the following explanations regarding each component will be provided to participants:
Importance
Does the specified indicator encompass an important aspect of the designed model?
Is the specified indicator significant for the recipients of care?
Will the evaluation of the specified indicator lead to noticeable changes in patient care?
Scientific credibility
Is there scientific evidence supporting the relationship between the indicator and the model?
Can a precise and clear definition of this indicator be provided?
Is the distinction of this indicator from other indicators clear and evident?
Feasibility
Is the specified indicator practically implementable for planners?
Is the indicator feasible from a managerial and financial perspective?
Is the specified indicator controllable by the authorities?
These explanations will help ensure that experts have a clear understanding of each criterion as they evaluate indicators.
After receiving questioners, the average and SD of the scores assigned to each indicator will be calculated. Given that the scoring system ranges from 1 (the lowest score) to 3 (the highest score), the average scores for each component will fall within this range. Components that achieve higher average scores across the criteria of importance, scientific acceptability and feasibility will be ranked higher, while those with lower average scores will receive correspondingly lower rankings. Items that receive an average rating lower than 2 will be removed from further consideration.77
In the results tables, the average scores, SD and rankings of the questionnaire indicators will be presented separately for each indicator and according to the three specified criteria. This structured presentation will facilitate a clear understanding of how each indicator performs relative to others in the context of the cancer respite care model. Qualitative feedback will also be analysed. The results of this stage will clarify the possibility of implementing different parts and indicators of the model and will be the basis for decision-making for use in practice.
While model testing is one of the other measures that are carried out in order to check the validity of the model and the possibility of its implementation, testing the model of cancer respite care will be performed in another study.
Patient and public involvement
‘None’.
Ethics and dissemination
This research project, which received approval from three reviewers and the nursing faculty at Tabriz University of Medical Sciences, was also sanctioned by the Regional Ethics Committee (IR.TBZMED.REC.1402.720). The timing and location of interviews will be coordinated with the participants to ensure their comfort and privacy, which are top priorities. Participant confidentiality and privacy will be maintained in accordance with the guidelines set by the Regional Ethics Committee. The findings of this study will be shared through publication in a peer-reviewed journal, and all related data will be stored in an appropriate publicly accessible data repository to promote transparency and support future research efforts. Reports and publications will be devoid of any information that could identify the study participants.
At the start of the interview, data collectors will inform participants about the study’s purpose. Participants will then receive an explanatory statement to read and can ask any questions they may have. Following this, they will be asked to read and sign a consent form, indicating their agreement to participate. The consent form, written in Persian, will outline the study’s purpose, emphasise their freedom to participate, and explain how their information will be used while ensuring individual and facility confidentiality.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors All authors contributed to the development of different aspects of the protocol. NK and AR conceptualised the study protocol and the overall research design. VP conducted the literature review and developed the methodological approaches for data collection and analysis. NK, AR and RMR wrote the initial draft of the protocol and created the figures and tables within the document. FS-G designed the methodology for the scoping review and developed the search strategy. All authors contributed to the revisions of the protocol, provided feedback and approved the final version submitted for publication. VP is the guarantor of the study and responsible for its overall integrity and adherence to ethical standards.
Funding This work was supported by Tabriz University of Medical Sciences, grant number 72694.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.