Article Text

Abstract
Introduction Menière’s disease (MD) is a multifactorial disease characterised by recurring vertigo, tinnitus and fluctuating sensorineural hearing loss as typical clinical symptoms. For patients with MD with poor response to non-invasive treatments, it is recommended to use intratympanic gentamicin treatment. The destruction of vestibular organs by gentamicin may cause residual vestibular symptoms, notably unsteadiness. However, most previous clinical studies paid little attention to this issue. Currently, vestibular rehabilitation treatment (VRT) has been proven to be an effective method for controlling vestibular symptoms and has been applied to patients with various vestibular diseases. The aim of this study is to investigate the efficacy of VRT versus usual care in MD patients who experience persistent unsteadiness for 1 month after intratympanic gentamicin treatment, in order to understand whether VRT has a positive impact on balance maintenance and vertigo control in patients with MD.
Methods and analysis Randomised, assessor-blinded, controlled clinical trials will be used to compare the efficacy of balance function before and after VRT. Patients with MD who experience chronic unsteadiness for 1 month after intratympanic gentamicin treatment will be recruited and receive VRT, mainly including gaze stability training, gait rehabilitation, vestibular habituation training, etc. The outcomes assessments will be conducted at baseline and at eighth week and sixth month post-randomisation. The primary outcome will be the improvements in vestibular function quantified through the Functional Gait Assessment. The secondary outcomes will include sensory organisation test, vestibular laboratory tests (video head impulse test, caloric test and vestibular evoked myogenic potentials), Menière’s disease outcomes questionnaire, visual vertigo analogue scale and vestibular activities and participation measure.
Ethics and dissemination This trial received ethical approval from the Institutional Review Board of Eye and ENT Hospital of Fudan University (reference number 2024020). The study results will be disseminated via peer-reviewed journals and conferences.
Trial registration number NCT06143462.
- Audiology
- REHABILITATION MEDICINE
- Quality of Life
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study will be the first clinical trial to examine the efficacy of vestibular rehabilitation treatment on chronic unsteadiness after intratympanic gentamicin treatment.
This study is a parallel-group, assessor-blinded randomised controlled trial, which is able to provide a reliable outcome for the study question.
With various subjective and objective outcome measures, this study can adequately reflect the efficacy of the intervention.
The age and duration of the patient’s illness may affect the results.
For the sake of the homogeneity of the study population, only patients with chronic unsteadiness for 1 month after intratympanic gentamicin treatment will be included in the study criteria, but patients with other residual vestibular symptoms will be discarded, which may miss some of the study information.
Introduction
Menière’s disease (MD) is a multifactorial inner ear disease characterised by recurring vertigo, fluctuating sensorineural hearing loss, tinnitus and/or aural fullness. Approximately, 17 to 513 individuals per 100 000 population are affected by this disease.1 The most common aetiology factors are genetics (13.7%), anatomical or structural abnormalities (12.4%), endolymphatic hydrops (ELH) (11.2%) and autoimmunity (11.2%).2 Although the definite cause of MD remains unknown, obstruction of the lymphatic drainage pathway or reduced lymphatic absorption may be the main causes of MD. Pathophysiologically, obstruction or reduced absorption of lymphatic fluid leads to an increase in the endolymphatic system, namely ELH, ultimately resulting in a rupture of the membrane which separates the internal and external lymphatic fluid. Consequently, a definitive treatment strategy has not yet been established.
As a chronic and intermittent disease with uncomfortable symptoms, MD causes considerable social and health problems. These symptoms include hearing loss, vertigo, tinnitus, hyperacusis or migraine. Especially for patients with recurrent vertigo, they always suffer from psychological problems such as depression and distress,3 with lower subjective well-being and quality of life, including impairments in daily behavioural activities, social interaction, interpersonal relationships, employment and income.4 Moreover, some patients with MD may experience vestibular drop attacks or vestibular syncope, which are considered as crucial contributors to injuries.5
Menière’s disease is usually diagnosed based on the patient’s medical history and detailed audiological examination results, and corresponding examinations are required to rule out other causes. At present, the most widely used diagnostic criteria for Menière’s disease were jointly developed by the Classification Committee of the Bárány Society, The Japan Society for Equilibrium Research, the European Academy of Otology and Neurotology (EAONO), the Equilibrium Committee of the American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS) and the Korean Balance Society in 2015.6 The classification includes two categories, namely, definite MD and probable MD.
The goals of MD treatments are primarily to prevent or reduce the severity and frequency of vertigo attacks; alleviate or prevent hearing loss, tinnitus and aural fullness; and improve quality of life.7 Treatment follows a graded manner. Non-invasive treatment is usually the first choice, and destructive treatment can be used when non-invasive management is ineffective. First-line treatments for MD include lifestyle modification (such as adequate rest/lifestyle counselling/low salt diet), conservative medical treatment (such as betahistine/diuretics), local pressure therapy and vestibular rehabilitation treatment (VRT). If medical treatment fails, intratympanic steroid treatment is recommended as the second-line treatment. Third-line treatment options depend on the patients’ hearing function, involving either the endolymphatic sac surgery (when hearing is worth being preserved) or the intratympanic gentamicin treatment (with a higher risk of hearing loss). The final option is the destructive surgical treatment known as labyrinthectomy, which can be combined with cochlear implantation or vestibular nerve section (when hearing is worth being preserved).8 9
Among them, intratympanic gentamicin treatment is the mainstream treatment, which is aimed at achieving long-term, stable and central compensatory peripheral vestibular hypofunction. This treatment refers to the local delivery of medication through the tympanic membrane into the middle ear, from where the drug will be absorbed into the inner ear. Gentamicin can chemically destroy the abnormal labyrinth, to alleviate vertigo at the cost of permanent vestibular deficit. Intratympanic gentamicin treatment has shown class A or B control of vertigo in 75% to 100% of patients with unilateral Menière’s disease.7 Gentamicin can be administered using various doses and regimens. Many studies have advocated the use of low dosages of gentamicin or titrating the dose based on individual response to treatment to reduce the risk of hearing loss.7 Scarpa et al 10 found that low-dose gentamicin treatment for unilateral Menière’s disease can significantly control dizziness without causing cochlear damage. Their injection protocol was as follows: patients received 1–5 intratympanic injections with 0.5 mL of 10 mg of gentamicin (80 mg/2 mL) with a 2-week interval between injections.
However, residual vestibular symptoms and disability are somewhat common in these post-treatment patients. Perez et al 11 showed that 5% of patients with complete or substantial control of vertigo after intratympanic gentamicin treatment manifested chronic unsteadiness. Furthermore, a 5-year follow-up by Boleas-Aguirre et al 12 demonstrated that 81% of patients treated with intratympanic gentamicin achieved complete control of vertigo. In their study, a visual analogue scale (‘DizVAS’) was used to assess the level of disequilibrium or the feeling of unsteadiness after treatment, ranging from 0 mm (no symptoms) to 100 mm (worse than before). ‘Low DizVAS’ was the VAS score below 50, and ‘High DizVAS’ was the score equal to or above 50. And at post-treatment follow-up, 84.5% of patients rated themselves as ‘low DizVAS’, while 15.5% reported of chronic unsteadiness and were considered as ‘high DizVAS’. In our study setting, approximately 20%–50% of the post-treatment patients may experience unsteadiness, which decreases the ability to perform daily activities, quality of life and cognitive and emotional status. Although unsteadiness is an infrequent concern, it demonstrates severe harmfulness similar to other vestibular symptoms.
VRT has been widely used for the management of persistent dizziness and vertigo in patients with vestibular dysfunction. VRT is an exercise-based therapy that promotes vestibular compensation, aiming to achieve a state of vestibular rehabilitation. This therapy improves the patient’s vestibular positional, visual and proprioceptive coordinated control of balance, as well as the compensatory ability of the central nervous system. It is designed to alleviate vertigo, improve gaze stabilisation, enhance postural control, increase functional activities and thereby increase quality of life.13 VRT mainly consists of five exercise components: (1) Gaze stability exercises (GSE), including adaptation and substitution exercises; (2) balance and gait training, including balance exercises, weight transfer exercises and gait training; (3) habituation exercises, including optokinetic exercises; (4) motor endurance training and (5) central vestibular training, including vestibulo-ocular reflex (VOR) suppression, VOR memory, anti-saccade and memory-guided saccade.14 15 VRT has been shown by moderate to strong evidence to be a safe and effective management for unilateral peripheral vestibular dysfunction.16 A recent systematic review of the literature concluded that VRT can improve balance and dizziness-related quality of life in patients with MD immediately after treatment, while as for the short-, intermediate- and long-term effects of VRT, randomised controlled trials with a lower risk of bias and long-term follow-ups are still needed.17 Moreover, Perez et al 11 demonstrated that VRT is helpful for patients with MD previously treated with intratympanic gentamicin. Thus, those patients should be encouraged to accept vestibular rehabilitation.
Although previous studies have elucidated the benefits of VRT in patients with MD, to date, no randomised clinical trial has been conducted specifically to investigate the effectiveness of VRT in treating unsteadiness after intratympanic gentamicin treatment in patients with MD. The purpose of this study is to explore the efficacy of VRT for patients with MD with chronic unsteadiness after intratympanic gentamicin treatment.
Methods and analysis
Study design, setting, participants
This study is designed as a single-centre, randomised, prospective single-blinded, controlled trial with two parallel interventional groups in a 1:1 allocation. Because VRT is a physical intervention, it is not possible to be blinded to either the physical therapist or the patients. However, researchers responsible for outcome assessments are blinded to group allocations.
Patients will be recruited from outpatient clinics of the Eye and Ear Nose Throat (ENT) Hospital of Fudan University, having the specialised doctors, staff and facilities needed for this clinical trial. The number of patients with MD with unsteadiness after intratympanic gentamicin treatment accounts for approximately 20%–50% of patients in the study setting. It is expected to enrol 48 subjects over a 12-month period.
Patients who meet all of the following criteria will be included:
Adults aged between 18 and 60 years old.
Conformed to unilateral Menière’s disease.
Reported of persistent unsteadiness for 1 month after intratympanic gentamicin treatment.
Be willing to sign the informed consent of the study.
Patients with any of the following conditions will be excluded:
Conformed to neuromuscular disease.
Conformed to severe cervical spine disease.
Conformed to other inner ear disease.
Conformed to bilateral Menière’s disease.
Conformed to comorbidities or potential comorbidities (eg, overlapping Menière’s disease and vestibular migraine).
Concurrent manifestation of psychiatric or psychological disorders.
Previously received intratympanic steroids treatment or other surgical treatments that affect vestibular function.
Sample size calculation
The study sample size is based on the Functional Gait Assessment (FGA) measure. The minimum detectable change (MDC) for the FGA is reported to be 6 points, with an SD of 5.5, as reported by Marchetti et al.18 In this study, we assume an FGA difference of 6 will be considered clinically meaningful. Thus, to detect an MDC of 6 for the FGA with 90% power (alpha level of 0.05, two-tailed test, beta level of 0.10), 19 subjects per group will be required as calculated by Two-Sample T-Tests Assuming Equal Variance in PASS15. Allowing for a 20% dropout rate, we will assign 24 subjects to each group (48 in total).
Procedure
Intratympanic gentamicin treatment protocol19 is as follows: The patient is placed in a supine position with the affected ear upwards, anaesthetised with 1% bupivacaine on the surface, and a small hole is punctured above the posterior tympanic membrane under the microscope. Slowly inject 0.5 mL of 30 mg/mL of gentamicin (take 1.5 mL of 40 mg/mL gentamicin and add 0.5 mL of 5% sodium bicarbonate) into the tympanic chamber. After injection, the patient is asked to remain supine with their head on their side and the affected ear up for 30–45 min, and swallowing movement is prohibited. The patient will have a follow-up visit at the outpatient clinic 3 weeks after treatment. Then, these patients will regularly come to the hospital for follow-up visits.
Patients who visit doctors from the outpatients and are suspected of MD with vestibular dysfunction are potentially eligible for this study. The diagnosis tests for MD include detailed history taking, pure tone audiometry and contrast-enhanced MRI.20 Patients with unilateral MD who do not respond to conservative medical management can receive intratympanic gentamicin treatment.21
Intratympanic gentamicin treatment protocol19 is as follows: The patient is placed in a supine position with the affected ear upwards, anaesthetised with 1% bupivacaine on the surface, and a small hole is punctured above the posterior tympanic membrane under the microscope. Slowly inject 0.5 mL of 30 mg/mL of gentamicin (take 1.5 mL of 40 mg/mL gentamicin and add 0.5 mL of 5% sodium bicarbonate) into the tympanic chamber. After injection, the patient is asked to remain supine with their head on their side and the affected ear up for 30–45 min, and swallowing movement is prohibited. The patient will have a follow-up visit at the outpatient clinic 3 weeks after treatment. Then, these patients will regularly come to the hospital for follow-up visits.
If patients report of chronic unsteadiness for more than a month after intratympanic gentamicin treatment, we will require the patient to conduct a self-assessment through the visual vertigo analogue scale (VVAS), scoring from 0 to 10 points, and a score of 3 or above is considered consistent with unsteadiness. Those who meet the inclusion criteria will be invited to participate in this study, sign informed consent forms (online supplemental file 1) and complete subsequent screening and baseline assessments. If the unsteadiness does not exceed 1 month, a prescription can be issued and the patient will be asked to have regular follow-up visits.
Supplemental material
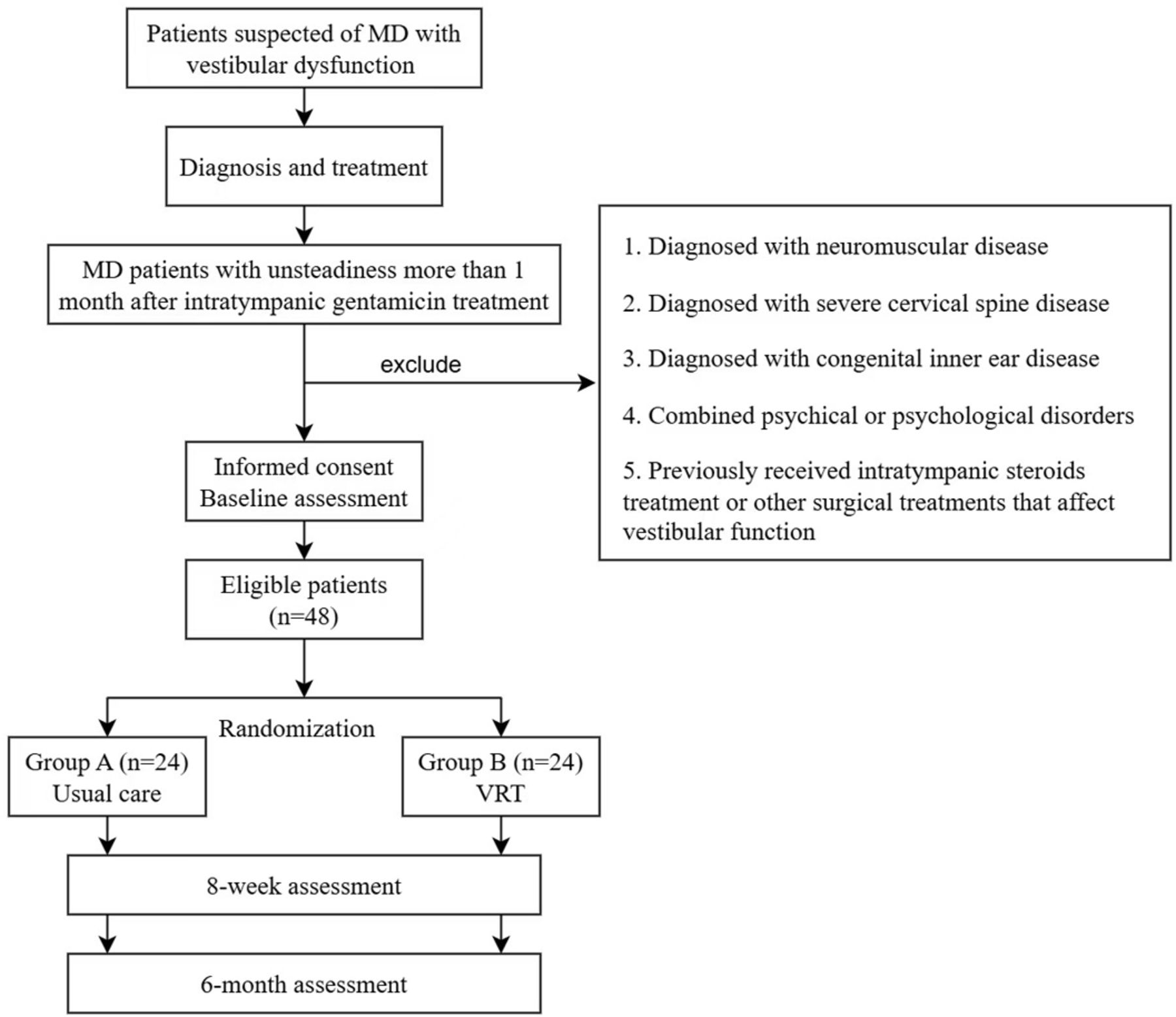
After providing completed informed consent forms, participants will be randomised into two treatment groups: Group A, referred to as usual care (UC), will receive conventional medications; Group B (VRT) will receive outpatient VRT in combination with home practice based on conventional treatment. According to the updated US clinical practice guidelines, patients with chronic unilateral vestibular hypofunction may be advised to complete static and dynamic balance exercises for a minimum of 20 min per day for at least 4 to 6 weeks.22 Thus, outcomes will be assessed at baseline, at 8 weeks and 6 months after randomisation. Figure 1 provides the study flowchart.

{kind=link}
Study flowchart. MD, Menière’s disease; VRT, vestibular rehabilitation treatment.
Randomisation and blinding
The total sample size is 48 and participants will be randomly divided into two groups of 24 persons each. The randomisation sequence will be generated through Excel: Input the formula=RAND() to generate random numbers between 0 and 1 for 48 participants, then sort the random numbers in ascending order and number the participants in order. The first 24 are Group A (UC), and the last 24 are Group B (VRT). Participants will be randomly allocated at a ratio of 1:1 and stratified by gender. The physical therapist will be notified of group allocation after obtaining consent forms, enrolling and numbering the patients and completing the baseline assessments. Due to VRT being an operational intervention, both patients, physiotherapists and physicians will be aware of the assignment result. However, researchers independent of treatment will contact the patients and collect subjective and apparatus-based data. The statistician of our trial team will remain blinded until the statistical analyses are complete.
Interventions
The two treatment groups are the UC group and the VRT group.
Usual care
Participants allocated to Group A (UC) will receive conventional therapeutic interventions encompassing the following:
Medication: Patients will receive pharmacological treatment, including anti-dizziness medications, diuretics or hormone therapy, contingent on the patients’ specific clinical presentation.
Health education: Comprehensive health education will be imparted to enlighten patients about the intricacies of the disease, incorporating aetiology of MD and underlying mechanisms. The instruction will encompass the interrelation between the vestibular system and the body’s equilibrium. Patients will be advised to remain calm and gradually squat down during vertigo episodes to forestall inadvertent accidents such as falls. Further instructions will encompass lifestyle adjustments including smoking cessation, abstinence from alcohol, limited consumption of tea and coffee, consumption of a light diet, prioritisation of adequate sleep and rest, cultivation of a positive emotional state and the identification and avoidance of potential triggers that precipitate vertigo attacks.
Vestibular rehabilitation treatment
Participants allocated to Group B (VRT) will undergo a structured regimen of vestibular rehabilitation. This will encompass office-based sessions of VRT once weekly, supplemented by home-based exercises conducted two or three times daily for the remaining duration of the study. Each home-based exercise session is anticipated to last approximately 20 min, with the regimen spanning over a course of 6 months. Throughout this intervention period, patients in Group B will be provided with rehabilitation training resources, including instructional forms and videos, ensuring clear guidance and continuity. To increase adherence, patients will be tasked with maintaining comprehensive exercise records. Concurrently, meticulous monitoring of adverse events (AEs) occurring during the trial will be undertaken.23
The protocol mainly consists of three categories: gaze stabilisation exercises (GSE), balance and gait training and habituation training, aiming to treat vertigo and balance disorders. Patients in group B will be given individualised VRT: Select appropriate exercise according to the patients’ balance function status and clinical symptoms, (1) if there are symptoms such as vertigo and visual instability, GSE can be selected to improve vestibular-ocular reflex (VOR) gain; (2) if there are symptoms such as swaying and balance instability, balance and gait training can be selected to improve vestibular-spinal reflex (VSR) gain; and (3) if there are symptoms such as head movement sensitivity or visual vertigo, habituation training can be selected to improve sensitivity to provoking movements.24 In addition, the exercise protocol can be changed with the rehabilitation process.25
Adverse events
AEs are defined as any unfavourable symptoms that participants experience during medical procedures. Actually, VRT rarely causes AEs. Patients will be asked to report any symptoms or conditions that occur during or after the exercises. VRT protocol should be discontinued or modified if the following symptoms occur: vomiting, nausea or muscle soreness; a sharp or prolonged pain sensation in the neck, arms or legs; a sensation of aural fullness, hearing loss or tinnitus; double vision or fainting. The physical therapist will contact the subjects by phone once a week to ask if they have any adverse experiences. All unexpected symptoms that occur during this trial, whether or not considered related to VRT, will be recorded and reported to the trial steering committee and Adverse Drug Reaction Administration of the Eye and ENT Hospital of Fudan University.
Withdrawal/retention of participants
Participation in this study is voluntary and participants have the right to withdraw at any time. However, we will use some approaches to improve adherence and minimise attrition rates. These include data collection without clinical appointments, a reimbursement mechanism for the cost of extra auxiliary examination to encourage study completion, and the provision of weekly telephone contact during the trial. During each telephone consultation, any concerns will be assessed, including unexpected symptoms, as well as logistic issues such as travelling to the clinic, parking issues or making an appointment with the clinical consultant. On rare occasions, participants may withdraw due to unforeseen circumstances, and reasons for withdrawal will be recorded.
Outcome measures
Primary outcome
The FGA, a semi-quantitative measure of walking balance ability, was developed to eliminate the ceiling effect observed in the Dynamic Gait Index. The FGA is a 10-item clinical gait test in which participants are asked to perform the following gait activities: (1) Gait on level surface, (2) change in gait speed, (3) gait with horizontal head turns, (4) gait with vertical head turns, (5) gait and pivot turn, (6) step over obstacles, (7) gait with narrow base of support, (8) gait with eyes closed, (9) ambulating backwards and (10) steps.26 The FGA is scored on a 4-level (0–3) ordinal scale; scores range from 0 to 30, with lower scores indicating greater impairment. FGA with scores less than or equal to 22/30 can effectively classify fall risk in older adults and predict unexplained falls in community-dwelling older adults.27 The FGA has demonstrated acceptable reliability, internal consistency and validity for use as a clinical gait measure for patients with vestibular disorders.28 In this study, we define the primary outcome as the FGA change from baseline to 6 months after assignment.
Secondary outcomes
The sensory organisation test (SOT) is a form of posturography that is designed to distinguish and assess the weight of vestibular, visual and proprioceptive sensations in maintaining balance and is an important indicator for developing individualised vestibular rehabilitation programmes and understanding the efficacy of rehabilitation.29 In the SOT, the patient stands on a force plate that can rotate up and down surrounded by a moveable wall. There are six increasingly challenging conditions (from SOT1 to SOT6) that disrupt portions of sensory input or visual environment designed to assess balance, each condition consisting of three 20 s trials: (1) eyes open on firm surface; (2) eyes closed on firm surface; (3) eyes open with sway referenced visual surround; (4) eyes open on sway referenced support surface; (5) eyes closed on sway referenced support surface; and (6) eyes open on sway referenced support surface and surround. Equilibrium Score (ES) is the average centre of gravity sway for each trial for each condition. The highest theoretical ES is 100 (indicating no sway), and losses of balance were graded as 0. The composite score (CS) is a weighted average of the six conditions and is also calculated as an estimate of overall postural stability.24
The vestibular laboratory tests, including video head impulse test, caloric test and vestibular evoked myogenic potentials, are used to evaluate the changes in vestibular function before and after VRT.
The Menière’s Disease Outcomes Questionnaire (MDOQ) is a comprehensive assessment of patients with MD’ quality of life (QOL) in three dimensions: physical, emotional and social. Wang et al 30 have revised the MDOQ in Chinese, which consists of 19 questions, and the analysis showed that the Chinese version of MDOQ (MDOQ-C) has good reliability and validity, and the composition of the items is different from the original scale. After dimensional reconstruction, it can be used to evaluate the QOL of patients with MD.
In the VVAS, patients estimate the intensity of their symptoms related to dizziness, vertigo and imbalance.31 VVAS is a subjective scale, and the improvement of the scale values and gradual return to the normal value range suggest that the rehabilitation training is effective. The scale ranges from 0 to 10, with 0 being the lowest level of dizziness and 10 being the greatest. The score of 1~3 is mild, 4~6 is moderate and 7~10 is severe.25
The Vestibular Activities and Participation Measure (VAP) is a 34-item self-report questionnaire based on the International Classification of Functioning, Disability and Health (ICF) framework to evaluate the extent of activity limitations and participation restrictions created by vestibular disorders.32 Patients will be instructed to choose none (0 points), mild (1 point), moderate (2 points), severe (3 points), unable to do (4 points) or not applicable to describe the difficulty of performing the related activity. The total score for the VAP is obtained by calculating the average of the item scale values after excluding the ‘not applicable’ items. Mueller et al 33 have demonstrated the reliability and validity of the VAP in people with vestibular disorders across cultures.
Time-points of outcome measurements
Outcome measurements will be performed at baseline and at two follow-up visits. Baseline assessments will be performed at the time of signing the consent form. Demographic and clinical data collection will include: age, gender, education, employment, marital status, coexisting systemic diseases, date of onset, duration of symptoms from onset to treatment and affected ear. Participants are required to return to the clinic at the eighth week and sixth month post-allocation to conduct vestibular functional assessments (FGA, SOT), undergo vestibular laboratory tests (video head impulse test, caloric test and vestibular evoked myogenic potentials), record subjective vestibular questionnaires (MDOQ, VVAS and VAP) and monitor safety outcomes. The timeline is presented in table 1.
Study timeline
Data analysis
Comparisons between the two groups will be made for demographics, clinical characteristics and vestibular function in the baseline data, with Student’s t-test or Mann-Whitney U test for two independent continuous samples and a χ2 test for dichotomous samples. To compare vestibular recovery at eighth week and sixth month from baseline, logistic regression adjustments will be made for age, gender and other baseline potential confounders, while the numerical variables such as FGA, SOT, MDOQ, VVAS and VAP scores will be computed by mixed-model with repeated measures analyses of variance, with group and time as fixed effects and subject as a random effect, controlling for potential confounders. Differences in adherence rate and dropout rate between the two groups will be analysed by using χ2 tests. A two-sided p<0.05 is considered statistically significant. We will calculate relative risks with corresponding 95% CI to compare dichotomous variables and mean difference (MD) for continuous variables.
Statisticians (QT), who are unaware of group assignment and study hypotheses, will statistically analyse the data. To reduce the dropout/attrition rate, an intention-to-treat (ITT) analysis and a per-protocol analysis will be performed at each outcome. Primary analysis of the outcomes will be conducted after group assignment based on their ITT analyses; a per-protocol (PP) analysis will serve as a secondary analysis (defined as completion of at least one follow-up visit). For the missing data in ITT and PP analyses, if appropriate, multiple imputation methods will be used. Up-to-date versions of SPSS (SPSS, Chicago, Illinois, USA) will be used to conduct analyses.
Study status and recruitment
This is protocol V.1, which was completed on 15 February 2024. The anticipated date of first recruitment is 30 June 2025. The estimated enrollment period is 12 months. The total duration of this study, including statistical analysis and drafting of the study results, is expected to be 24 months.
Data management
A data management committee (DMC) will be established and will meet monthly to manage and monitor the daily operation of the experiment, review the accumulated data and check the authenticity, security and integrity of the database. The DMC will consist of a group leader, a statistician, a methodologist, an experienced physiotherapist specialised in vestibular rehabilitation and a patient representative. All members in the group are independent of the study sponsor and declare no conflict of interest. The frequency of the interim analyses will be decided deliberately. We anticipate that there might be two to three mid-term analyses before the final analysis.
Patient and public involvement
Patients have been involved in the design of this study. We have interviewed three patients with chronic vestibular syndrome about their perceptions of the training intensity, the frequency of interaction and instruction. Their views have been incorporated into our revised protocol. Patients and the public will be informed of the study results through peer-reviewed journals or academic conferences.
Ethics and dissemination
This study was approved by the Institutional Review Board of Fudan University Eye Ear Nose and Throat Hospital (reference number 2024020). The principles of informed consent and confidentiality will be followed throughout the experimental process. We plan to publish the study findings in peer-reviewed academic journals. We also intend to present this study locally, nationally and internationally.
Discussion
Vestibular dysfunction usually refers to a state of imbalance in vestibular function, including hypo or loss of vestibular function and vestibular hyperfunction. Vertigo, dizziness and unsteadiness are three symptoms that usually occur in various combinations in patients with vestibular dysfunction. Bisdorff et al 34 suggested that these three symptoms may be caused by similar, rather than different, mechanisms, and agreed with the view that vestibular symptoms lack specificity.35
Menière’s disease is a peripheral vestibular disorder characterised by severe episodes of vertigo and hearing loss. Intratympanic gentamicin, the standard treatment for refractory Menière’s disease, can reduce vertigo but may impair vestibular function and worsen hearing. To maintain body balance, a combination of vestibular, visual and proprioceptive senses is required. By destroying the vestibular system in the inner ear through gentamicin, it is hoped that the central vestibular system can compensate to alleviate unilateral vestibular hypofunction (assuming adequate contralateral function).36
However, some patients fail to compensate adequately and experience vestibular symptoms. 27% patients treated with gentamicin in Patel et al’s report37 experienced severe vertigo and vomiting shortly after the injection. 75% patients in Smith et al’s study38 experienced vestibulotoxic effects after intratympanic gentamicin treatment, although this was not associated with the success of treatment. In Murofushi et al’s study,39 20% of patients treated with intratympanic gentamicin showed chronic vestibular dysfunction (ataxia and head movement-induced oscilloscopy) after 1 year of treatment. In Perez et al’s study,11 23% of patients experienced mild or moderate unsteadiness after 2 years of treatment. While few reports mentioned the impairment of postural stability, the reduction in vestibulospinal function after intratympanic gentamicin affects postural stability and gait in daily tasks; this impairment may be temporary and subside within hours or weeks, or it may be long term.40
Due to the plasticity and compensatory capacity of the central vestibular system, vestibular rehabilitation may be able to ameliorate the postural instability that occurs after intratympanic gentamicin treatment by promoting vestibular compensation. The effect of VRT in MD has generally been studied in the previous researches,17 41 42 but little attention has been paid to the effect of VRT on patients with MD with vestibular dysfunction after intratympanic gentamicin treatment. There is a lack of sufficient evidence that VRT has a positive effect on patients with MD with postural instability after intratympanic gentamicin.
Since postural instability/unsteadiness is primarily due to reduced vestibulospinal function,40 balance and gait training may be selected and emphasised in personalised VRT as appropriate to improve VSR. To assess the efficacy of VRT, we intend to perform a series of vestibular function tests, including (1) the SOT, which is used to differentiate and comprehensively assess the static and dynamic postural control ability of somatosensory, visual and vestibular systems and (2) the FGA, an evaluative scale on balance and gait, which is used to assess gait balance and for fall screening in the elderly. In addition, we plan to use three subjective measures, including MDOQ, VVAS and VAP, to assess the severity of unsteadiness symptoms and their negative impact on patients’ daily lives.
In conclusion, our study will be the first to assess and follow up the effect of VRT on vestibular function in patients with MD who feel unsteadiness after intratympanic gentamicin treatment by using multiple tests of vestibular function. Based on our clinical practice experience, we hypothesised that VRT would improve vestibular function and quality of life in patients.
Ethics statements
Patient consent for publication
References
Footnotes
QT and YZ contributed equally.
Contributors HY is responsible for the design. QT and YZ are responsible for the manuscript draft and implementation of the trial. QT, PW and HY are responsible for the implementation of imaging data analysis. All authors contributed to the drafting and approved of the final manuscript. Guarantor is HY.
Funding This study is supported by Excellent Doctors-Excellent Clinical Researchers Program (SYB202008), the National Natural Science Foundation of Shanghai (21ZR1411800), and Fudan-Fuxin Research funding (FNF202237).
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.