Article Text

Abstract
Objectives Unlike comparable countries, acute coronary syndrome (ACS) mortality is similar among patients who present to rural and urban hospitals in Aotearoa New Zealand (NZ). The aim of this study was to determine whether differences in ischaemic heart disease (IHD) deaths that occurred without a preceding hospital admission in rural and urban populations explained this finding.
Design Retrospective observational study using the National Mortality Collection (MORT) and National Minimum Dataset (NMDS) for hospital discharges datasets.
Setting People in NZ who died from IHD were categorised based on their rural–urban status (U1 (major urban), U2 (large urban) and rural) using the Geographic Classification for Health and prioritised ethnicity (Māori—NZ’s Indigenous population and non-Māori).
Participants All people 20+ years who died from IHD between July 2011 and December 2018.
Primary and secondary outcomes The outcome was the lack of a hospital admission preceding IHD death, identified by linking the NMDS with MORT. This was measured for the 30 days and 1 year prior to death and for all-cause and IHD hospitalisations separately.
Results Of the 37 296 deaths, a similar percentage of rural and urban residents died without an all-cause (rural 63.2%, U2 60.8%, U1 62.8%) or IHD (rural 70.9%, U2 69.0%, U1 70.1%) admission in the preceding 30 days, or without an all-cause (rural 32.8%, U2 35.5%, U1 35.5%) or IHD (rural 52.7%, U2 52.6%, U1 51.9%) admission in the preceding year. Exceptions were deaths that occurred without a prior admission for rural non-Māori aged 55–64 (higher odds) and 75+ years (lower odds) compared with U1 non-Māori 55–64 and 75+ years, respectively, across all four outcome measures.
Conclusions This study suggests that the lack of difference in ACS mortality for patients who present to NZ rural and urban hospitals is not explained by IHD death that occurred without a recent preceding hospital admission.
- Hospitals
- Cardiovascular Disease
- Mortality
- Primary Prevention
- PREVENTIVE MEDICINE
Data availability statement
Data may be obtained from a third party and are not publicly available. Data can be made available by a request to Te Whatu Ora—Health NZ and the Ministry of Health.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
Linked national datasets (mortality and hospital discharges) to determine the outcomes of interest.
Use of a geographic classification taxonomy specifically designed for health purposes.
Use of proportional mortality study design does not consider underlying differences in rural–urban mortality rates.
Only health encounters that resulted in admission to hospital were able to be considered, which may underestimate people who had significant health interventions by general practitioners.
Introduction
Ischaemic heart disease (IHD) is a major, largely amenable cause of hospitalisation and death.1 2 The majority of deaths attributed to IHD occur out of hospitals;3 however, little attention has been paid to these deaths in the international literature. The focus has been on deaths that occur in hospital or very shortly (within 28 days) after the admission.3–7 Rates of out-of-hospital deaths have been reported to be higher in Indigenous populations, and those with less access to hospitals (especially hospitals with routine access to interventional facilities), such as people who live in rural areas.5–7
In Aotearoa New Zealand (NZ), mortality from IHD has consistently been shown to be higher for Māori (NZ’s Indigenous people) compared with non-Māori.6 Māori who live in rural areas have the highest rates of amenable and all-cause mortality.1 Cardiovascular mortality is also higher for approximately 20% of the non-Māori and 25% of the Māori who reside in rural areas of NZ compared with those who live in urban areas.1 2 8
Although overall mortality due to cardiovascular disease in NZ has been shown to be higher for people aged less than 75 years who live in rural areas compared with those of the same age living in urban areas,2 and short-term mortality rates were similar for patients with an acute coronary syndrome (ACS) who presented to either rural (with no on-site access to interventional cardiology services) or urban hospitals with or without routine access to percutaneous intervention (PCI).9 10 This is contrary to findings from other countries with comparable health systems.11 12 It has been postulated that this lack of difference in mortality for hospitalised patients was because people who lived in rural areas may have died before accessing a hospital.10
Māori and Pacific peoples were found to be more likely to die from IHD outside of the hospital compared with non-Māori non-Pacific peoples, but rurality was not identified as a contributing factor.6 However, this study used an older geographic classification system (the Urban Rural Experimental Profile) that has been shown to systematically underestimate rural–urban health disparities.13 A novel geographic classification system, the Geographic Classification for Health (GCH) has recently been developed specifically for health policy and research purposes in NZ.8 The GCH uses people’s geographic location of residence to assign urban and rural status. Use of the GCH has uncovered rural–urban health disparities (particularly for rural Māori) that were previously hidden by the use of older geographic classification systems.1 2 13
The aim of this study was to determine whether the lack of differences in IHD mortality between patients who presented to rural and urban hospitals was explained by differences in IHD deaths that occurred without a preceding hospital admission in rural and urban populations.
Methods
Study design
This was a retrospective observational study of IHD deaths that occurred in NZ between 1 July 2011 and 31 December 2018.
Data sources
Mortality collection
Demographic (including ethnicity) and clinical information for all IHD deaths were obtained from the National Mortality Collection (MORT) that Manatū Hauora (Ministry of Health) and Te Whatu Ora (TWO—Health NZ) are responsible for maintaining. MORT contains demographic information as well as the cause of death for all deaths that occur in NZ.14
National Minimum Dataset (NMDS)
The National Health Index (NHI) was used to link individuals in MORT to the National Minimum Dataset (NMDS). The NHI is a unique identifier that is used throughout the health system. The NMDS contains information on all discharges from NZ public hospitals, as well as some information from private hospital discharges.15 This dataset was used to identify those people who had at least one admission to hospital prior to their death and to identify comorbidities.
Admission and discharge events for each person that occurred within 1 day of each other were bundled together to account for the often rapid movement between and within hospitals for further treatment and investigations.10 16
Although not all private hospital admissions are in the NMDS, nearly all acute admissions related to IHD in NZ are to public hospitals.16
Geographic Classification for Health
The GCH groups people into one of the five rural–urban categories.8 It has two urban categories (major urban (U1) areas, which represent major cities and smaller urban areas (U2), which represent NZ’s regional cities) and three rural categories that range from R1 (least rural) to R3 (most rural). For this study, to minimise the effects of small numbers in the most remote regions of NZ, the three rural categories (R1, R2 and R3) were condensed into one rural category.
The usual residential address of an individual at the time of death is assigned to a small geographic unit that is recorded within MORT. Like many countries, geographic units are available in a range of sizes and in NZ the smallest of these is the ‘meshblock’; each contains 20–60 dwellings and 60–120 residents on average.17 Statistical Area 1 units (SA1) are slightly larger geographic units and are built by grouping related meshblocks. Since the GCH was defined at SA1 level, meshblocks were mapped into SA1s and the SA1:GCH concordance file was used (https://rhrn.nz/gch/resources).
Inclusion and exclusion criteria
All people 20 years and older who died from IHD causes were included. People who could not be assigned a GCH category (eg, people who died at sea or usually lived in another country) were excluded from the analysis.
Outcome measures
The outcome of interest was the lack of a hospital admission preceding a death from IHD. This was compared with a hospital admission occurring preceding IHD death and was measured for two different time intervals (30 days and 1 year) and for both all-cause and IHD-specific hospitalisation. Therefore, there were four outcome measures:
No all-cause admission to hospital in the 30 days prior to death.
No IHD-related admission to hospital in the 30 days prior to death.
No all-cause admission to hospital in the year prior to death.
No IHD-related admission to hospital in the year prior to death.
For each outcome measure, three categories of the GCH were compared. These are described in more detail below.
All-cause admissions included any admission with a treatment time longer than 3 hours captured by the NMDS. A 30-day time period was selected to capture hospital admissions that occurred within the period that is considered to be part of the same initial acute myocardial infarction (AMI) encounter (ie, a further admission within 28 days of the index AMI is not considered a new AMI),18 and also to maintain consistency with previous studies.9 10 The 1-year time period was chosen to examine hospital utilisation over a longer period of time. Both all-cause and IHD-specific admissions were considered to capture all contact with inpatient hospital services and also to minimise the effect of variation in coding practices between rural and urban areas.
A secondary objective was to determine the cause of any admission in the year prior to a death from IHD.
Diagnoses
People who died from IHD were identified within MORT as those with the International statistical Classification of Diseases and related health problems 10th edition Australian Modification (ICD10-AM) code in the primary cause of death field within the code range I20–I25.19
Hospital admissions related to IHD were identified in the NMDS using the same ICD10-AM codes. The primary and all secondary (non-primary) diagnosis codes were considered for all admissions that occurred within the specified time period.20 IHD deaths that occurred without a hospital admission were assigned ‘TRUE’ and IHD deaths that did have an admission were assigned ‘FALSE’.
Other data collected
The following variables were collected from MORT: age at the time of death, sex (male or female), prioritised ethnicity and meshblock.
Age was considered as both a continuous variable and also categorised into the following groups: <55 years, 55–64 years, 65–74 years and 75+ years.
Ethnicity was prioritised according to the Ministry of Health’s guidelines, where people were considered Māori if this was identified in any of the three (level 2) available ethnicity fields within MORT.21 Ethnicity was dichotomised into Māori and non-Māori due to small numbers of other ethnicities who live in rural areas of NZ.8
History of IHD, revascularisation or heart failure (HF) requiring hospitalisation within the last 7 years were collected from the NMDS.
The Charlson score was used to quantify multimorbidity. The Charlson score is a weighted scoring system based on 17 conditions that predict 1-year survival. It is commonly used in studies examining patients with acute and chronic cardiovascular disease.22 23 A non-cardiac Charlson score removes the scores and weighting for cardiac comorbidities.9 Consistent with previous studies, ICD10 codes from all hospitalisations within the last 7 years found prior to an individual’s death were considered to derive the Charlson score.22
For the secondary objective, the primary diagnosis for the last discharge event in bundled admission encounters in the year prior to death was obtained from the NMDS. These were categorised based on the WHO’s ICD10 chapters.19 The number (and percentage) of diagnoses within each chapter were calculated for the three GCH categories. The ICD10 chapters and their codes are presented in online supplemental table 1.
Supplemental material
Statistical analysis
A proportional mortality design was used, which included only those who had died from IHD and compared the proportion of deaths that occurred without a preceding hospital admission across the three rural–urban geographic categories (U1, U2 and rural). Accurate denominator data for the hospitalised and non-hospitalised population within each of the three geographic regions were not available, precluding other study designs.
Data were summarised using mean and SD for continuous variables, and frequency and percentage for categorical variables.
Separate logistic regression models were used to estimate the unadjusted and adjusted ORs with a 95% CI for the association between rurality (three-level variable) and each of the four outcome measures (lack or absence of a hospital admission prior to IHD death at each of the time periods). The rurality variable compared people who lived in rural areas (R) and less urban areas (U2) with those who lived in major urban areas (U1)—the reference category.
For all outcome measures, age, ethnicity, sex, non-cardiac Charlson score and previous admission with IHD, revascularisation, coronary angiogram or heart failure were considered as potential confounders.
All model assumptions were checked. Linearity for the variable age (the only continuous variable) was assessed in the final model; if complex non-linear associations were identified, the variable was categorised as described above. Backward elimination was used to reduce the number of variables in each model, with each step manually reviewed. However, important potential confounders were kept (age and ethnicity). Likelihood ratio tests were used to assess the statistical significance of each variable (p<0.05) in the models. Only a priori interactions (GCH, age and ethnicity) were investigated.
Data management, analysis and visualisation were done in the open-access R statistical language (V. 4.1.1) using the R-studio integrated data environment (Posit software, Boston, USA).
Patient and public involvement
Māori consultation was undertaken with the Ngāi Tahu Research Consultation Committee. There was no other patient or public consultation undertaken.
Results
There were 37 530 IHD deaths that occurred between 1 July 2011 and 31 December 2018. Of these, 234 (0.6%) people were excluded from the analysis as a GCH category was unable to be assigned, leaving 37 296 (99.4%) people who died from IHD. The majority of these deaths (19 764/37 296, 53%) occurred in people who lived in U1 areas; nearly a quarter occurred in people who lived in U2 (9109/37 296, 24.4%) and 22.6% in people who lived in rural areas (8423/37 296). A higher percentage of people who lived in U2 (1078/9109, 12%) and rural (1221/8423, 14%) areas were Māori compared with people who lived in U1 (1394/19 764, 7.1%). Population characteristics are shown in table 1.
Characteristics (n=37 296) of people who died of IHD between 1 July 2011 and 31 December 2018
Outcome measures
Since there was a non-linear relationship with age for all outcomes, age was categorised in all models.
For each of the outcome measures, there was a significant interaction identified between GCH, age and ethnicity (p<0.05), and results are therefore presented in GCH, age and ethnicity strata.
IHD death without an all-cause admission in the preceding 30 days
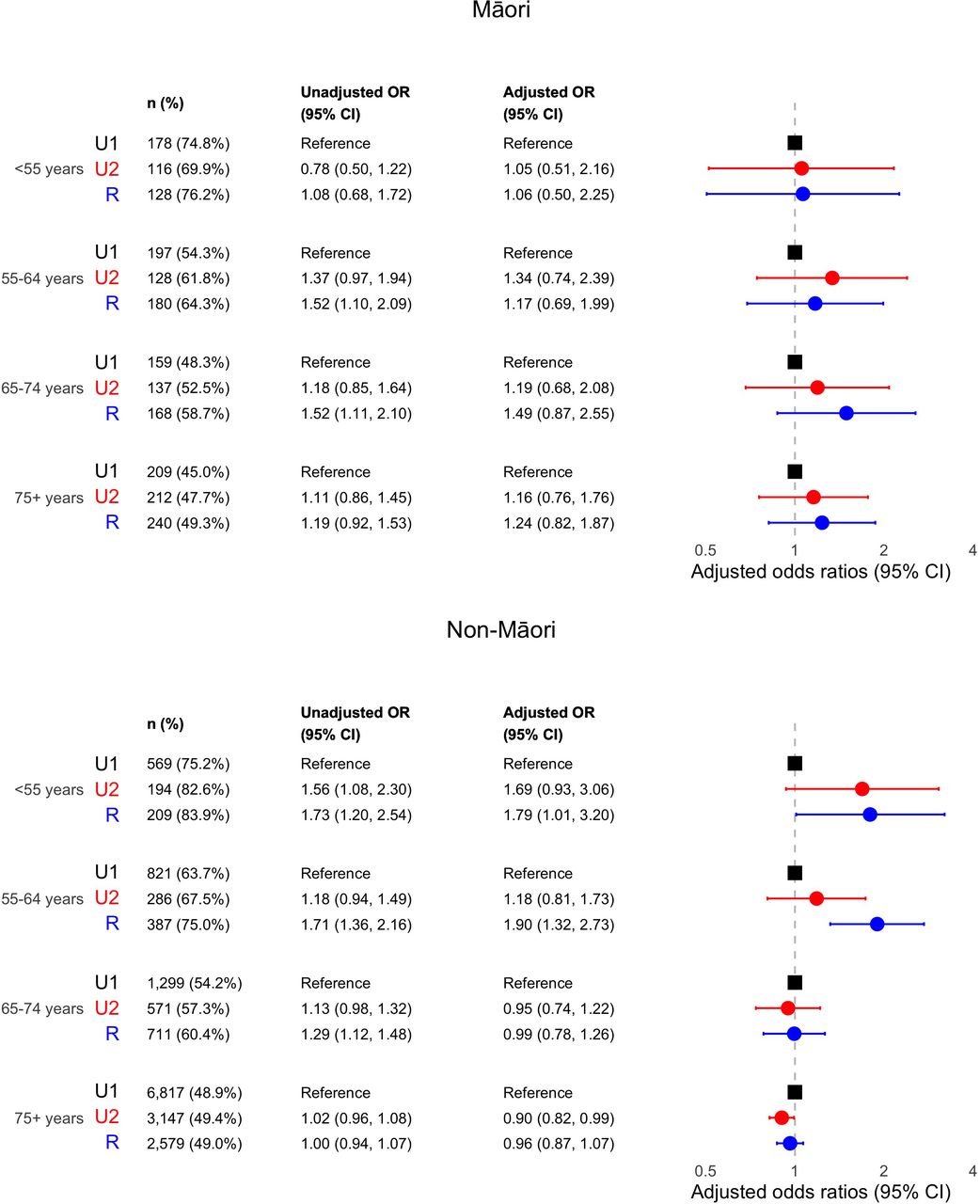
Overall, 23 276 (62.4%) deaths did not have an admission to a public hospital for any reason in the preceding 30 days. This occurred in 63.2% of people who lived in rural areas (5321/8423), 60.8% of people who lived in U2 (5534/9109) and 62.8% of people who lived in U1 areas (12 421/19 674). The number, percentage, unadjusted and adjusted OR with 95% CI comparing people who did not have an admission to hospital, and those who did, in the 30 days prior to their death and the GCH categories for each age and ethnicity strata are presented in figure 1.

The number, percentage, unadjusted and adjusted OR with 95% CI for people who died from ischaemic heart disease (IHD) and did not have an admission to hospital in the preceding 30 days (compared with those who did have a hospitalisation). ORs are adjusted for age, ethnicity, previous admission with IHD, revascularisation and heart failure in the last 7 years and non-cardiac Charlson score. For each age–ethnicity stratum, U1 is the reference Geographic Classification for Health (GCH) category.
For Māori (in any of the age groups), there were few statistically important differences between the percentage who lived in rural areas who died from IHD without an admission in the preceding 30 days compared with Māori who lived in urban areas (figure 1).
A higher percentage of rural non-Māori aged <55 years (83.9%; OR 1.60, 95% CI 1.08 to 2.42) and 55–64 years (76.9%; OR 1.55, 95% CI 1.20 to 2.02) did not have an admission in the 30 days prior to IHD death compared with non-Māori aged <55 years (74.8%) and 55–64 years (66.3%) who lived in U1 areas.
Conversely, a lower percentage of non-Māori aged over 75 years who lived in rural (60.2%; OR 0.87, 95% CI 0.81 to 0.93) and U2 (60.1%; OR 0.84, 95% CI 0.78 to 0.89) areas died without a hospital admission in the preceding 30 days compared with non-Māori aged over 75 years who lived in U1 (62.4%).
IHD death without an IHD admission in the preceding 30 days
There were 26 127 (70.1%) deaths that occurred without an admission for IHD in the preceding 30 days: 70.9% (5976/8423) for people who lived in rural areas, 69.0% (6288/9109) for those who lived in U2 and 70.1% (13 896/19 764) for those in U1. The number, percentage, unadjusted and adjusted OR with 95% CI for each ethnicity and age stratum are presented in figure 2.

The number, percentage, unadjusted and adjusted OR with 95% CI for people who died from ischaemic heart disease (IHD) and did not have an admission to hospital with IHD in the preceding 30 days (compared with those who did have a hospitalisation). ORs are adjusted for age, ethnicity, previous admission with IHD, revascularisation and heart failure in the last 7 years and non-cardiac Charlson score. For each age–ethnicity stratum, U1 is the reference Geographic Classification for Health (GCH) category.
For Māori, there was no evidence of differences between the GCH categories in any age strata.
For non-Māori aged less than 55 years (89.2%; OR 1.74, 95% CI 1.01 to 3.04) and 55–64 years (82.9%; OR 1.71, 95% CI 1.23 to 2.38) there was a higher percentage of those who lived in rural areas who did not have an admission due to IHD in the 30 days prior to IHD death compared with non-Māori who lived in U1 areas and were aged <55 years (81.8%) and 55–64 years (73.2%).
In contrast, there were proportionally fewer non-Māori 75 years and older who died without an IHD admission in the 30 days prior to IHD death who lived in rural (68.2%; OR 0.89, 95% CI 0.82 to 0.97) and U2 regions (68.2%; OR 0.85, 95% CI 0.79 to 0.92) and compared with non-Māori 75 years and older who lived in U1 (69.6%).
IHD death without an all-cause admission in the 1 year prior to death
There were 12 216 (32.8%) deaths that did not have an admission in the preceding year: 32.0% (6321/19 764) in U1, 35.5% (2908/9109) in U2 and 35.5% (2987/8423) in rural areas. The number, percentage, unadjusted and adjusted ORs with 95% CI for each ethnicity, age and GCH stratum are presented in figure 3.

The number, percentage, unadjusted and adjusted OR with 95% CI for people who died from ischaemic heart disease (IHD) and did not have an admission to hospital in the preceding 1 year (compared with those who did have a hospitalisation). ORs are adjusted for age, ethnicity, previous admission with IHD, revascularisation and heart failure in the last 7 years and non-cardiac Charlson score. For each age–ethnicity stratum, U1 is the reference Geographic Classification for Health (GCH) category.
A higher percentage of Māori (27.3%; OR 1.42, 95% CI 1.01 to 2.00) who lived in rural areas and were aged 75 years and older did not have an (all-cause) admission in the year prior to IHD death compared with Māori aged 75 years and over who lived in U1 (19.8%). There was no evidence of difference between rural and urban Māori within other age groups.
For non-Māori aged 55–64 years (59.5%; OR 1.53, 95% CI 1.20 to 1.95) who lived in rural areas, there was also a higher percentage of people who died without an admission in the preceding year compared with non-Māori 55–64 years who lived in U1 areas (46.9%).
IHD death without an IHD admission in the preceding year
Overall, 52.7% (19 642/37 296) of deaths did not have an admission for IHD in the preceding year with 54.6% (4602/8423), 52.6% (4791/9109) and 51.9% (10 249/19 764) in rural, U2 and U1 areas, respectively. The number, percentage, unadjusted and adjusted OR with 95% CI for each ethnicity and age stratum are presented in figure 4.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The number, percentage, unadjusted and adjusted OR with 95% CI for people who died from ischaemic heart disease (IHD) and did not have an admission to hospital with IHD in the preceding 1 year (compared with those who did have a hospitalisation). OR are adjusted for age, ethnicity, previous admission with IHD, revascularisation and heart failure in the last 7 years and non-cardiac Charlson score. For each age–ethnicity stratum, U1 is the reference Geographic Classification for Health (GCH) category.
Within each age group, there was insufficient evidence of differences between Māori who lived in U1 and Māori who lived in U2 or rural areas.
For non-Māori, a higher percentage who lived in the rural areas and were aged <55 years (83.9%; OR 1.79, 95% CI 1.01 to 3.20) and 55–64 years (75.0%; OR 1.90, 95% CI 1.32 to 2.73) died without an admission for IHD in the preceding year compared with non-Māori aged <55 and 55–64 years who lived in U1 (75.2% and 63.7%, respectively) .
However, for non-Māori who lived in U2 and were aged 75 years or older (49.4%; OR 0.90, 95% CI 0.82 to 0.99), a slightly lower percentage compared with non-Māori aged 75 years or older who lived in U1 (48.9%) died without an IHD admission in the prior year.
Reason for admission
A total of 25 080 (25 080/37 296, 67%) people who had at least one admission to hospital in the year prior to IHD death. Primary diagnoses for 65 960 all-cause admissions in the year prior to death are displayed in online supplemental table 2.
Slightly more than a third of the admissions were due to circulatory diseases (38.9%, 38.4% and 39.2%) for U1, U2 and rural areas, respectively. Similarly, there were few differences between the GCH categories for any of the other WHO diagnosis chapters.
Discussion
Main findings
This is the first study to our knowledge that uses a purpose-built rural–urban classification system (the GCH) to examine whether there was a hospital admission in the period prior to IHD mortality in NZ.
The majority of people who died from IHD in this study did not have an admission to hospital in the preceding 30 days and approximately a third did not have an admission 1 year prior. This is a finding consistent with other studies.3 7 Interpreting the overall rural–urban trends was difficult in our study because of the interaction between age, ethnicity and GCH that has previously been demonstrated.2
However, for both Māori and non-Māori people who lived in rural areas and died from IHD aged less than 75 years, there was a trend towards not having an admission (either all-cause or IHD-specific) in the 30 days or 1 year prior to IHD death compared with those who lived in the most urban (U1) areas. There was only evidence of a significant statistical difference across all four outcome measures for rural non-Māori people aged 55–64 years compared with urban non-Māori aged 55–64 years.
Non-Māori younger than 55 years and who lived in rural areas had increased odds of dying from IHD without a hospital admission in the 30 days prior to their death but not in the year before, compared with non-Māori who lived in U1. In contrast, for non-Māori who were 75 years and older, there were decreased odds of not having an admission to hospital (all-cause and IHD) 30 days prior to IHD death in rural and smaller urban centres (U2) compared with U1 areas.
For Māori, while the overall trend was similar, there was no evidence of a significant difference between the three GCH categories in any of the age strata or for any outcome with the exception of Māori aged 75 years or older who lived in a rural area, who had increased odds of dying without an all-cause admission in the year prior to IHD death compared with Māori aged 75 years or older who lived in U1. A previous NZ-based study examining the role of ethnicity in IHD case fatality also found that rurality did not play a contributing role in the increase in out-of-hospital mortality rates seen for Māori, although with an older geographical classification system.6 13
That a clear and consistent difference in hospital admissions between rural and urban populations in all age groups prior to their IHD-related death was not able to be demonstrated in our study is in contrast to findings in other countries, where a higher proportion of rural compared with urban people do not access hospital services before IHD death.7 The reason for these results is unknown and needs further exploration; however, possible contributing factors include a relative lack of defibrillators and emergency responders in rural compared with urban areas and complex migration patterns in older adults.
Once a major ischaemic heart event results in cardiac arrest, a key predictor of survival is the time to defibrillation.24 25 In NZ, like other countries, access to defibrillators is decreased in rural regions and areas with high levels of socioeconomic deprivation.25–27 Again, similar to other countries, a large portion of rural NZ does not have access to timely emergency medical services.25 28 Ambulances that do respond are more likely to contain a single crew.29 Both of these factors have been shown to decrease survival after out-of-hospital cardiac arrest.28 Patients who present with ST segment elevation MI to hospitals without PCI facilities (rural and urban non-interventional) were less likely to attend hospital via ambulance, indicating that these may have been unavailable or not called.30 The lack of defibrillators and ambulance services in rural areas may account for the findings seen in our study in younger age groups, where rural non-Māori people had slightly higher rates of dying from IHD without a hospital admission preceding death. However, this does not explain the pattern for those older than 75 years where non-Māori people who died were more likely to have an admission in the preceding 30 days.
The contrast observed in our study, where non-Māori aged less than 75 years had increased odds, while those 75 years and older had decreased odds of dying without a preceding admission, is a phenomenon that has also been seen in a prior NZ-based study.2 This difference is likely to be related to complex migration patterns between rural and urban areas in this older age group and needs further examination.2
Slightly more than a third of the all-cause admissions that did occur in the year prior to IHD death were for circulatory system diseases. This highlights the opportunity for and the important role that secondary cardiovascular risk prevention has. In NZ Māori and those who live in more socioeconomically deprived areas are less likely to have aspirin and statins dispensed 3 years after an IHD hospital admission.31 32 Whether this is due to changes in prescribing practices or patient-related barriers to medication use is unclear. Although there are no studies comparing the long-term prescribing of secondary prevention medications between rural and urban NZ populations, a higher percentage of Māori live in rural (compared with urban) areas, and people (particularly Māori) who live in rural areas are more likely to live in areas with greater socioeconomic deprivation.8 Internationally, there is evidence of reduced prescribing of secondary prevention medications for rural people.33 Disparities in the continuation of secondary prevention medications have been postulated as a mechanism for the increased mortality at 2 years seen for people presenting to rural hospitals, compared with urban hospitals after ACS.10
The remainder of the admissions to hospital (approximately 61%) were for other reasons. While primary cardiovascular risk screening in NZ is largely within the domain of general practice rather than secondary hospital care, there is perhaps an opportunity to update or provide cardiovascular risk screening and prevention either as inpatients or soon after discharge.34 Internationally, rural people have a greater burden of both modifiable and unmodifiable risk factors that increase the rates of cardiovascular disease.35 36 Using the hospital admission as a catalyst to undertake this screening is particularly relevant for the approximately 6% of all people in NZ and the 10% of Māori who are not enrolled with general practices in NZ.37
Strengths and limitations
A major strength of this study is that linked national datasets were used. This means that almost all deaths and hospitalisations in NZ were able to be included. The use of a novel geographic classification taxonomy that was specifically designed for health purposes was also a strength.
The predominant limitation of this study was the potential for variability in mortality and hospitalisation within the underlying population that was not accounted for. However, concerns about any underlying variation in mortality rates are tempered by previous studies that show that mortality was similar between patients presenting to rural and urban hospitals with ACSs.9 10 The lack of appropriate and accurate denominator data for the hospital catchments was a particular barrier in performing a mortality rate study. This has meant that underlying mortality rates and mortality rate ratios were unable to be calculated in this study. Future studies are required to determine rural–urban mortality rates.
The reliance on accurate coding of IHD as the cause of death in MORT was an additional limitation. The accuracy of death certificate coding for IHD varies in the international literature,38 with no recent NZ-based study.39 Postmortem examinations are relatively rarely performed in NZ, with 23% of Māori and 11% of non-Māori receiving this examination.40 Internationally, rates of postmortem examinations are lower in rural compared with urban populations.41 It is unknown if the accuracy of death certification differs between rural and urban populations. Differences in coding practices within the NMDS for people who live in rural areas and present to rural health services are also unknown and could be a potential cause of bias.2 10 The potential for miscoding in the NMDS was mitigated by including an admission for any reason as an outcome measure.
A further limitation is that only healthcare encounters that resulted in admission to hospital were considered. Emergency department stays greater than 3 hours are included in the NMDS, but contact with general practitioners, ambulance, other prehospital care providers or short emergency department stays are not recorded.15 In rural NZ, as in other countries, there is a blurring of the roles provided by rural healthcare workers, and patients may receive emergency care without being included in national datasets.42 Therefore, there might be some people who died and may have had recent contact with rural clinicians who will not have been included in the NMDS.
The data used in this study were from 2011 to 2018. This is because of the delay in updating NZ’s National MORT. It is possible, but unlikely, that these findings would be different if more up-to-date data were available. There was a smaller number of Māori in this study compared with non-Māori, which led to a small increase in the uncertainty in the ORs that were calculated for each of the four outcome measures. This lack of power makes it harder to draw conclusions; however, it remains essential to present results separately for Māori as part of the commitment to Te Tiriti o Waitangi and Māori data sovereignty principles to ensure that disparities are not missed. To decrease the effect of small numbers in rural populations, the three rural classifications (R1, R2 and R3) were grouped together. It is possible that there are large variations in IHD mortality and hospital admissions between residents of the three rural categories, especially for Māori, that were not able to be considered in this study.1
The NZ deprivation index (NZDep) was not included as a potential confounder when estimating the adjusted ORs for outcomes of interest. This was because the effects of socioeconomic deprivation and rurality are difficult to separate, and the sparse data for people who lived in both rural and low socioeconomic areas. Therefore, the inclusion of NZDep in the model would likely remove some of the effects of rural–urban differences that we want to estimate. NZ’s administrative datasets, including MORT, have been shown to misclassify and undercount Māori, which may result in an underestimation of the frequency of IHD death and admission for Māori.43 44
Policy and practice implications
Improving access to prehospital emergency services and defibrillators in rural and socioeconomic deprived areas, as well as better education on the signs and symptoms of acute IHD, have previously been highlighted as interventions to reduce unexpected out-of-hospital death.27 45 Ensuring that these interventions are contextually and culturally appropriate is essential.27 46 Using every opportunity, including hospital admissions not directly related to IHD, to ensure that primary and secondary prevention screening and management of cardiovascular disease is also warranted.31 32
While the trend in younger people cannot be ignored, this study suggests that the lack of difference in ACS mortality found for people who present to rural and urban hospitals in NZ is unlikely to be due to people dying before they are able to be admitted to a hospital facility.9 10 In fact, there is evidence of increased hospital use for rural non-Māori compared with urban non-Māori 75 years and older—an age group that contributes most to overall cardiovascular mortality rates.2 The findings in our study are also unlikely to explain the increase in cardiovascular mortality and all-cause and amenable mortality for rural Māori.1 13 A better understanding of the healthcare needs and consumption patterns across the age groups in rural areas is required.2
Conclusion
Of people who died of IHD in NZ, those who lived in rural areas had similar odds of dying without having a hospital admission in the preceding 30 days or 1 year to those who lived in more urban areas. The major exception to this was rural non-Māori who were aged 55–64 years and rural Māori aged 75 years and older who had slightly increased odds of not being admitted to hospital compared with urban non-Māori aged 55–64 years and urban Māori aged 75 years and older, respectively.
In contrast, rural non-Māori aged 75 years and older were less likely to die without a hospital admission than urban non-Māori aged 75 years and older. Acknowledging the limitations of the proportional mortality study design, this study suggests IHD death that occurs without a preceding hospital admission is unlikely to influence the interpretation of rural–urban differences in current mortality data following admission with ACS. There is an opportunity for health professionals to improve primary and secondary cardiovascular risk assessment and management for those who are admitted to hospital.
Data availability statement
Data may be obtained from a third party and are not publicly available. Data can be made available by a request to Te Whatu Ora—Health NZ and the Ministry of Health.
Ethics statements
Patient consent for publication
Ethics approval
The University of Otago Human Research Ethics Committee approved the study (reference number HD19/069). As de-identified data from national routinely collected datasets were used in this study, informed consent was not required.
References
Footnotes
X @StokesTim63, @tiekemanu
Contributors RM: conceptualisation, data curation, formal analysis, investigation, methodology, project administration, supervision, validation, visualisation, writing—original draft, writing—review and editing. RT: conceptualisation, data curation, formal analysis, investigation, methodology, supervision, validation, writing—review and editing. TS: conceptualisation, investigation, methodology, supervision, writing—review and editing. GD: conceptualisation, data curation, formal analysis, investigation, methodology, supervision, validation, visualisation, writing—review and editing. SC: conceptualisation, formal analysis, investigation, methodology, supervision, writing—review and editing. AM: conceptualisation, investigation, methodology, writing—review and editing. TT: conceptualisation, investigation, methodology, writing—review and editing. GN: conceptualisation, formal analysis, investigation, methodology, supervision, validation, writing—review and editing. RM is the lead author and guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design or conduct or reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.