Article Text

Abstract
Objective This study aimed to investigate the incidence of overweight in patients with major depressive disorder (MDD) comorbid anxiety during the acute phase and to explore associated factors.
Design Cross-sectional study.
Setting Wuhan Mental Health Center, China, from July 2017 to August 2022.
Participants 737 hospitalised patients diagnosed with MDD in the acute phase with comorbid anxiety symptoms.
Primary outcome measures Incidence and clinical correlations of overweight (body mass index (BMI) ≥ 24).
Results Among the study population, 55.63% were classified as overweight. Binary logistic regression analysis revealed that being married (B=0.28, p value=0.018, OR=1.10), thyroid-stimulating hormone (TSH) levels (B=0.10, p value=0.001, OR=1.10) and low-density lipoprotein cholesterol (LDL-C) levels (B=1.61, p value=0.045, OR=1.18) were significant positive predictors of overweight. Additionally, multiple linear regression indicated that TSH levels (B=0.16, t=3.17, p value=0.002) were positively associated with higher BMI values.
Conclusion Over half of the hospitalised MDD patients with comorbid anxiety are overweight. Thyroid function emerges as a crucial clinical factor for overweight in this population. Targeted interventions focusing on thyroid function may be a promising approach for managing overweight in these patients.
- Cross-Sectional Studies
- Overweight
- Depression & mood disorders
- Anxiety disorders
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study includes a relatively large sample, ensuring the stability of the results.
The biochemical indicators analysed are commonly used in clinical practice, making the findings easily applicable.
The cross-sectional design limits the ability to infer causality.
Unmeasured confounding factors may have influenced the observed associations.
Introduction
Major depressive disorder (MDD) is a common psychiatric disorder characterised by marked depressed mood, diminished interest and decreased energy.1 Although anxiety disorders and MDD are two distinct diagnostic entities, anxiety and depression comorbidity is a relatively common syndrome.2 In Western countries, the prevalence of comorbid anxiety in patients with MDD ranges from 11% to 80%,3–5 and in China, similarly, upwards of 70% of patients with MDD have comorbid anxiety symptoms.6 7 Comorbid anxiety symptoms are frequently associated with lower treatment response rates, lower remission rates, diminished quality of life, an increased likelihood of suicidal behaviour and a higher risk of cardiovascular disease in MDD patients.2 8 9
Mood disorders and obesity appear to be twins, often acting as risk factors for each other and were once collectively referred to as the ‘metabolic-mood syndrome’.10 Previous studies have shown that patients with MDD frequently experience overweight and obesity.11–13 The presence of obesity in individuals with MDD can have detrimental effects, affecting their clinical outcomes by prolonging recovery time and increasing suicidal ideation.14 15 Additionally, both overweight and obese individuals are vulnerable to mood disorders.16 17 Studies have demonstrated that weight reduction is crucial for alleviating anxiety and depressive symptoms in patients.18 19 Several pathways have been identified that connect obesity and mood disorders, such as lifestyle behavioural habits,20 21 hypothalamic-pituitary-adrenal axis disorders,22 altered glucocorticoid receptor function,23 inflammation24 and genetic variations,25 26 among others. Given the complex relationship between overweight and mood disorders and the negative empowerment on the efficacy and prognosis of patients with MDD, actively clarifying the clinical characteristics of obesity in MDD populations and exploring the potential biomarkers that can be used for clinical interventions are very critical tasks.
Up to now, although there are many studies related to being overweight in MDD patients, there are not enough studies on overweight in MDD patients with comorbid anxiety, and the results of the few studies are inconsistent due to issues such as sample size, population characteristics, cultural and geographic differences.27 28 More importantly, comorbid factors such as obesity are important factors in treatment interruption and disease relapse in the MDD population.29 This study examined the incidence of overweight in a sample of hospitalised Chinese Han patients in the acute phase of MDD with comorbid anxiety. It also explored the factors influencing both the occurrence and severity of overweight, offering valuable insights and warnings for proactive weight management in this target population.
Subjects and methods
Subjects
The sample size prediction was based on the following formula:
where n=sample size, Z=Z-statistic for the chosen level of confidence (1.96 for a 95% confidence level), p=expected prevalence or proportion (with reference to the prevalence of overweight in the Chinese general population, the value of 0.5 was taken here),30 d=precision or margin of error (equal to 0.05) and the statistical power (1-β) was 0.90. Thus, the estimated sample size required was 384 participants.
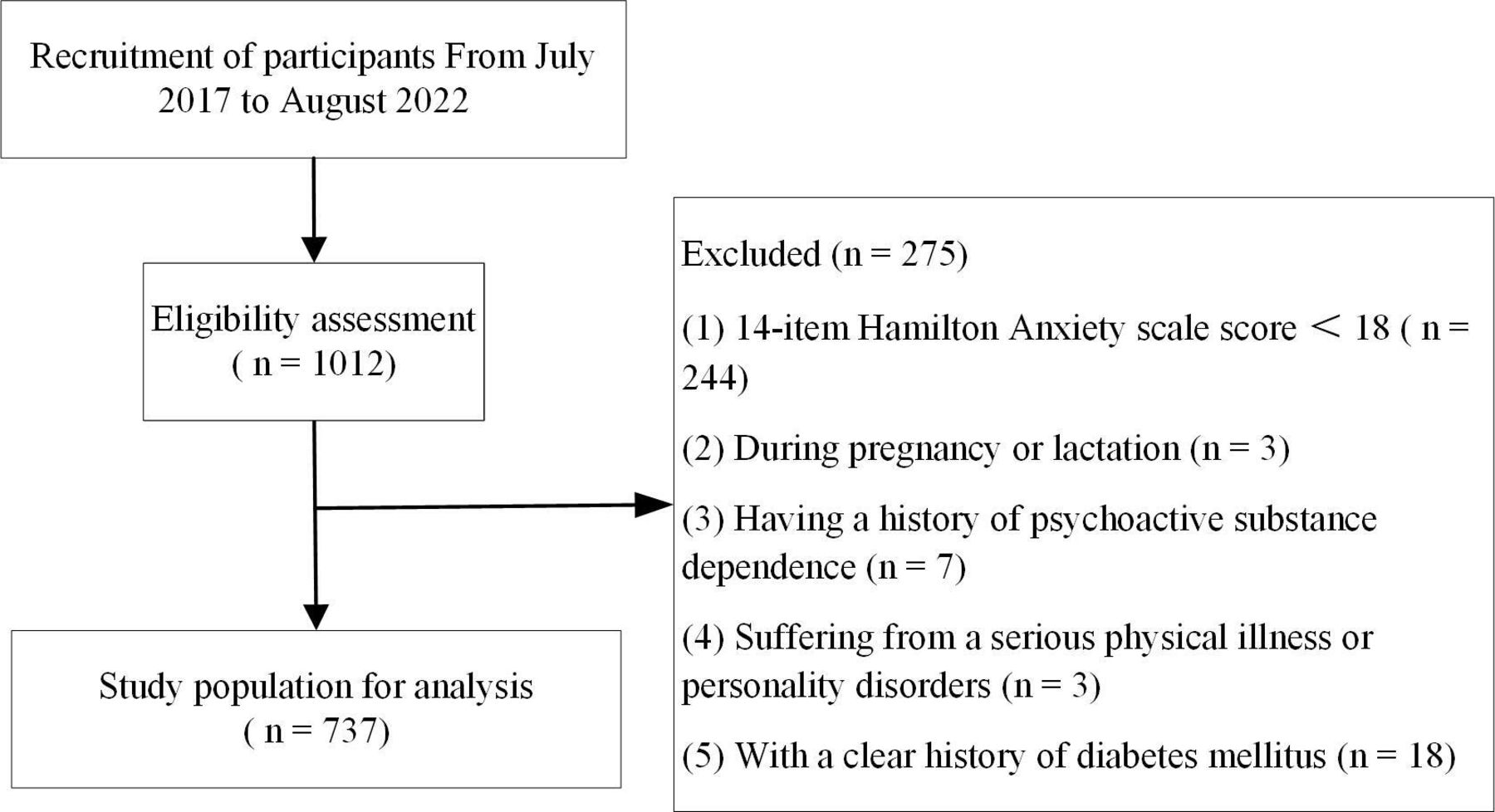
In this study, 737 individuals with MDD who also presented with comorbid anxiety symptoms were enrolled. These participants were admitted to Wuhan Mental Health Center, the foremost public tertiary psychiatric hospital in central China, due to an acute episode of their mental health condition, spanning from July 2017 to August 2022 (the flow chart is shown in figure 1).

{kind=link}
Flowchart for study sample inclusion.
The study included patients who fulfilled the following criteria: (1) met the diagnostic criteria for MDD as per the International Classification of Diseases, 10th edition; (2) were aged between 18 and 60 years; (3) were of Chinese Han nationality; (4) either male or female; (5) scored ≥24 on a 17-item Hamilton Depression Scale (HAMD-17); (6) scored ≥18 on a 14-item Hamilton Anxiety scale (HAMA-14).
Patients who fulfilled any of the following criteria were excluded from the study: those diagnosed with other severe mental illnesses, pregnant or breastfeeding individuals, patients with a history of substance abuse, those with a documented diagnosis of a serious physical illness or personality disorder, those with comorbid diabetes mellitus and those who were unable to cooperate in completing a psychological evaluation for any reason.
The research adhered strictly to the principles outlined in the Declaration of Helsinki. The study protocol underwent rigorous review, and approval was granted by the Ethics Committee of Wuhan Mental Health Center. Furthermore, all participants provided their informed consent through a paper-based form.
Research design
This study was conducted as a cross-sectional research design. Initially, the incidence of being overweight within the target population was determined. Subsequently, demographic and general clinical data between two clinical subgroups were compared: those with normal body mass index (BMI) (labelled as normal BMI group) and those with high BMI (labelled as high BMI group). Finally, the authors analysed the factors associated with overweight and its severity.
A self-designed Excel form was used to collect demographic and clinical data of the enrolled patients, including age, age at onset, disease duration, gender, marital status, education, history of suicidal behaviour, history of outpatient treatment, BMI, waist circumference and blood pressure. On admission day, depressive symptoms, anxiety symptoms, psychotic symptoms and illness severity were evaluated using HAMD-17, HAMA-14, positive symptom subscales (P1-P7) of Positive and Negative Symptom Scale and Clinical Global Impression Inventory-Severity of Illness. Then, routine biochemical parameters measured using fasting blood of the patient, including thyroid function, fasting blood glucose levels and lipid levels, were extracted from the electronic medical record system.
The criteria for overweight (high BMI group) were established based on the weight status classification criteria of the Chinese Obesity Working Group.31 Accordingly, all study subjects were classified into two categories: those with a normal BMI (BMI <24 kg/m2) and those who fell into the overweight or obesity category (BMI≥24 kg/m2).
Two psychiatrists conducted the evaluation of pertinent psychological scales, each with a title of attending or higher, who were affiliated with the medical institution from which the sample originated.
Data analysis
Categorical variables were reported as counts, while continuous variables with normal distribution were depicted using mean and SD. Continuous variables that were not normally distributed were expressed using median (p25, p75). The Shapiro-Wilk test was employed to verify the normality of all continuous variables. For both continuous variables, whether normally or non-normally distributed, and categorical variables, statistical comparisons were made using independent samples t-tests, Mann-Whitney U-tests and χ2 tests. To discern differences in demographic and clinical variables between the overweight subgroup and the normal BMI subgroup, χ2 tests were applied to categorical data and independent samples t-tests were applied to continuous variables. Subsequently, the variables that varied in univariate analyses as independent variables were used, and binary logistic regression models with overweight as the outcome variable were constructed to investigate factors influencing overweight within the target population. Ultimately, a multiple linear regression model was developed to identify the factors impacting patients with degrees of overweight, using BMI as the dependent variable and factors affecting overweight from binary logistic regression as independent variables. All p values were two-tailed, with significance set at <0.05. Statistical analyses were executed using SPSS V.27 (SPSS, Chicago, IL).
Patient and public involvement
Patients and/or the public were not involved in this study.
Results
Differences between the high BMI group and the normal BMI group
Of all the MDD patients with comorbid anxiety included in the study, 55.63% (410/737) met the diagnostic criteria for being overweight. The mean BMI in the two subgroups was (25.39±1.15) kg/m2 in the high BMI group and (22.71±1.08) kg/m2 in the normal BMI group. It was found that the following parameters were significantly higher in the high BMI group than in the normal BMI group: onset age (t=−2.14, p value=0.033), proportion married (χ2=4.24, p value=0.039), thyrotropin levels (t=−4.00, p value<0.001), low-density lipoprotein cholesterol (LDL-C) levels (t=−2.51, p value=0.012) and systolic blood pressure levels (t=−2.73, p value=0.006) (table 1).
The demographic and general clinical data in different clinical subgroups
Determinants of overweight in target patients: a binary logic-based model
A binary logistic regression model (backward Wald) using the variables that differed in the univariate analysis as independent variables and overweight as dependent variables was then developed. As the results in table 2 show, being married (B=0.28, p value=0.018, OR=1.10), thyroid-stimulating hormone (TSH) levels (B=0.10, p value=0.001, OR=1.10) and LDL-C levels (B=1.61, p value=0.045, OR=1.18) were positively predictive of clinical factors for being overweight.
Binary logistic regression analysis of the determinants of overweight in major depressive disorder patients with anxiety
Factors affecting the severity of overweight in the high BMI subgroup: a multiple linear regression model
Finally, for the high BMI subgroup of patients, a multiple linear regression model (input) with BMI as the dependent variable and the factors associated with the previous step affecting overweight as independent variables was constructed, and the results are shown in table 3. It was found that TSH (B=0.16, t=3.17, p value=0.002) was a positive predictor of elevated BMI.
Multiple linear regression analysis of factors associated with body mass index in major depressive disorder patients with anxiety
Discussion
In this study, specific clinical characteristics related to being overweight in individuals with MDD comorbid anxiety symptoms were observed. The incidence of overweight in this population was notably high, reaching 55.63%. Additionally, it was found that individuals in the overweight subgroups experienced a later onset of MDD and exhibited more pronounced metabolic disturbances. Furthermore, the analysis revealed that being married and elevated levels of TSH and LDL-C were associated with an increased risk of developing overweight. Notably, TSH levels were also identified as a clinical factor that promotes overweight and greater severity.
The incidence of overweight in patients with MDD comorbid anxiety in this study was 55.63%. Previous reports on the prevalence of overweight in individuals with MDD have shown some variation. For instance, in a study of first episode MDD patients in northern China, the prevalence was reported at 59.72%,32 while a multicentre study in Germany reported a prevalence of 52.16% among first episode MDD patients.13 When the sample extended to multiple European countries, the prevalence of overweight in MDD patients was approximately 48%.14 These studies, although slightly different from the current study, focused on individuals within the general MDD population rather than specifically considering patients with MDD comorbid anxiety symptoms. A recent study that shared a similar study population with this research found a higher prevalence of overweight (68.3%) in patients with MDD comorbid anxiety.33 This rate was higher than in this study, and this heterogeneity may have been caused by the stricter restriction of anxiety symptoms in that study and the fact that some of the patients who were included had a history of outpatient treatment. While the exact prevalence may differ across studies, a consistent finding is that a significant portion of individuals in the MDD population are overweight, focusing on and underscoring the importance of addressing weight concerns in this patient group.
Subsequently, the study examined the clinical factors that contribute to the development of overweight in patients with comorbid anxiety symptoms in MDD. The findings indicate that being married and TSH levels were identified as contributing factors to overweight formation in this population. Marital status has been consistently associated with a higher risk of overweight not only in the general population but also in individuals with MDD.15 34 Even after adjusting for variables such as employment status, stress levels and perceived health status, this relationship persists.35 The gain observed in married individuals may be linked to reduced physical activity,36 and it is also plausible that spouses may provide greater nutritional support during the acute phases of MDD episode. This suggests that spouses of married individuals with MDD may provide more balanced nutritional support during the onset of depression to help prevent obesity.
Elevated TSH levels emerged as a contributing factor for the development of overweight, obesity and elevated BMI in the study population, aligning with numerous existing reports.33 37 38 Another study exploring MDD patients with comorbid anxiety found that anxiety symptoms were associated with an increased risk of being overweight, with thyroid function playing a crucial role as a contributing factor.33 Evidence indicates that MDD patients with anxiety disorders often exhibit heightened levels of antithyroid antibodies due to stress-induced immune responses,39–41 leading to subclinical hypothyroidism and subsequently elevated serum TSH levels.42 43 Elevated TSH levels inhibit triglyceride lipase in adipose tissue via the TSH receptor in adipocytes, promoting adipocyte enlargement and consequent weight gain.44 Conversely, hypertrophied adipose tissue secretes leptin, which activates thyrotropin-releasing hormone (TRH) neurons to stimulate increased TSH levels.45 Collectively, the reviewed studies underscore the importance of maintaining thyroid function within normal limits to help manage overweight in individuals with MDD and anxiety symptoms.
This study possesses several strengths. First, this study included a sizeable sample size, enhancing the stability and generalisability of the results. Second, the target parameters that were investigated are common clinical indicators, which facilitate the generalisability and practical application of the findings at a lower cost. The current study also presents several limitations that should be acknowledged. First, the research design was cross-sectional, precluding the establishment of causal relationships between identified clinical factors and BMI in the study population. Second, the study predominantly focused on individuals with MDD in the acute phase of disease onset, potentially limiting the generalisability of the findings to other subpopulations of MDD patients. Lastly, a considerable proportion of the participants had a history of outpatient treatment, introducing a confounding factor that may have influenced the study outcomes. To address these limitations, the authors’ future research endeavours will aim to undertake more rigorous prospective studies with a broader scope.
In conclusion, over half of patients with MDD comorbid anxiety symptoms develop overweight. Furthermore, thyroid function is a crucial clinical factor for the development and severity of overweight. Therefore, targeted interventions on thyroid function could be potential therapeutic targets for overweight in patients with MDD comorbid anxiety symptoms.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study protocol underwent rigorous review and approval by the Ethics Committee of Wuhan Mental Health Center (KY20170201.01). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We thank all the medical staff and patients in this study for their participation and are very grateful to those who contributed to the diagnosis and clinical evaluation of the subjects.
References
Footnotes
Contributors HZ: writing—original draft. JW: formal analysis and writing—review and editing. WZ: investigation, supervision and writing—review and editing. XL: conceptualisation, methodology, software, investigation and formal analysis. HZ acted as guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.