Article Text

Abstract
Objective To investigate the correlation between caregivers’ health-related behaviours and the prevalence of overweight/obesity among children aged 2–6 years in Beijing city in China.
Design Cross-sectional study.
Setting Two kindergartens and two community health service centres in Beijing city, China.
Participants A total of 1967 children aged 2–6 years were included.
Primary and secondary outcome measures Children’s height and weight were measured and body mass index was computed. The caregivers’ exercise health behaviours and dietary health behaviours were assessed using a questionnaire, encompassing the frequency of exercise and the duration of each exercise session, as well as the frequency of consumption of desserts, late-night snacks, and fast food, regular eating habits, and the proportion of meat and vegetables consumed daily. Logistic regression analysis was performed to identify relationships between caregivers’ health-related behaviours and overweight/obesity in children.
Results Having caregivers who exercised ≥3 times/week (OR 0.643, 95% CI 0.417 to 0.990) was a protective factor against childhood overweight/obesity compared with having caregivers who exercised <1 time/week; caregivers’ frequent encouragement of children’s participation in physical activity was also a protective factor (OR 0.513, 95% CI 0.352 to 0.749). Additionally, children whose caregivers consumed sweets 2–3 times/week (OR 1.535, 95% CI 1.133 to 2.081) or ≥4 times/week (OR 1.916, 95% CI 1.258 to 2.918), as well as children whose caregivers consumed fast food ≥4 times/week (OR 2.298, 95% CI 1.349 to 3.914), were more likely to be overweight and obesity than children whose caregivers consumed these foods ≤1 time/week. Furthermore, caregivers’ irregular eating habits were positively associated with the occurrence of overweight and obesity in children (OR 1.485, 95% CI 1.056 to 2.089).
Conclusion Caregivers’ health-related behaviours were significantly associated with overweight/obesity among children in China. Substantial measures should be implemented to address caregivers’ health-related behaviours to prevent and control childhood overweight/obesity.
- Child
- Overweight
- Obesity
- Caregivers
- Behavior
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
Participants were randomly selected by stratified cluster sampling in this cross-sectional study.
Classification of nutritional status was based on the body mass index growth curve specifically developed for Chinese children and adolescents aged 0–18 years.
The impact of confounding factors was effectively controlled by the multivariate logistic regression method.
As the design of this study is cross-sectional, it should be noted that establishing causal relationships between factors and overweight/obesity is not possible.
The use of questionnaire surveys in this study may introduce certain subjectivity and recall bias.
Introduction
Overweight and obesity among children have become major public health issues worldwide.1 In China, the prevalence of overweight and obesity among children and adolescents increased 11-fold and 7-fold, respectively, over the past 30 years, from 1985 to 2014.2 3 The latest national prevalence estimates for 2015–2019 in China showed that 6.8% and 3.6% of children younger than 6 years and 11.1% and 7.9% of children and adolescents aged 6–17 years were overweight and obese, respectively.4 Moreover, according to the Global Burden of Disease Study estimates for 2015, China had the highest number of children living with obesity.5 Overweight/obesity in childhood not only has a negative impact on children’s physical and mental health but also may lead to obesity in adulthood. In addition, being overweight or obese in childhood has been prospectively associated with an increased risk of developing non-communicable diseases in adulthood, including cardiovascular disease,6 type 2 diabetes,7 stroke,8 chronic inflammation9 and various cancers,10 imposing a significant economic burden on society.
Overweight/obesity is influenced by both genetic and environmental factors.11 The family environment is the main place of activity for preschool children. Therefore, identifying the factors in the family environment that lead to overweight/obesity and providing early intervention are the keys to preventing and controlling overweight and obesity in preschool children. Among family environmental factors, parental nutritional status,12 knowledge,13 attitudes,14 feeding behaviours,15 16 sleep behaviours17 18 and screen use,19 20 as well as children’s sedentary behaviour,21 dietary patterns22 and sleep duration,23 24 have been studied in the past. However, little attention has been given to the impact of caregivers’ health-related behaviours on overweight and obesity in preschool children.
The term ‘caregiver’ is typically defined as the individual responsible for addressing the daily needs of a child within a family context.25 26 In such settings, multiple individuals may take on caregiving roles, such as parents, grandparents, other relatives or nannies. The person who bears primary responsibility for the child’s care and decision-making is referred to as the primary caregiver.27 Previous studies have demonstrated that the primary caregivers of children are predominantly parents, with mothers constituting the majority.28 29 As the primary individuals responsible for children’s daily care, caregivers’ behaviour may have a subtle influence on children’s behaviour. It remains unclear whether caregivers’ health-related behaviours further contribute to overweight and obesity in children.
The term ‘health-related behaviour’ encompasses a range of behavioural patterns that have the potential to impact health outcomes, such as individual exercise regimens, dietary choices, emotional regulation and recreational activities.30 31 The purpose of this study was to explore the influence of the primary caregivers’ health-related behaviours, particularly their exercise and diet-related behaviours, on the prevalence of overweight and obesity, to provide specific and feasible intervention measures for controlling obesity in children by improving family environmental factors.
Methods
Study design and participants
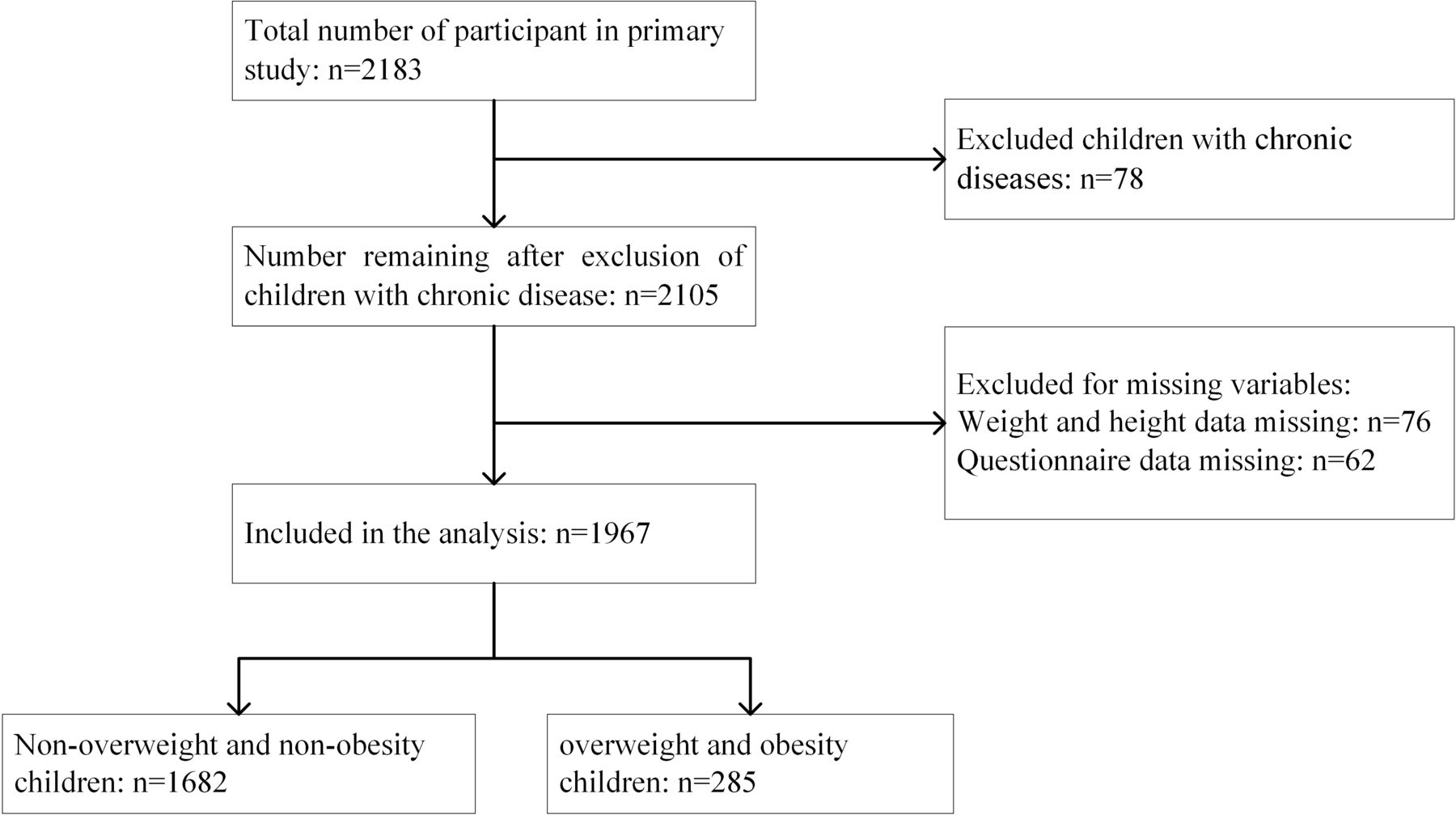
The study was conducted in Shunyi District of Beijing from June to December 2019. A stratified random cluster sampling method was employed, and two community health service centres and two kindergartens were selected. All children aged 2–6 years who had no history of chronic diseases, including cardiopulmonary, endocrine, renal or gastrointestinal diseases, as well as cancer and autoimmune diseases were eligible. In this study, there were totally 2183 children aged 2–6 years from the two community health service centres and two kindergartens, then after we excluded children with chronic diseases (78 cases) and the missing data (138 cases), a total of 1967 children were finally included (see figure 1 for study inclusion process).

{kind=link}
Flow diagram of the participants selection process. This figure shows the criteria that were used to selected the study participants in our study and the numbers that were affected by these criteria and the final sample size of the study.
All participants were assured of the confidentiality of their data.
Patient and public involvement
No patients were involved.
Anthropometric measurements
Anthropometric measurements were carried out at the community health service centres and kindergartens included in the survey. All personnel conducting physical measurements were qualified doctors or nurses, trained in standardised procedures. Height and weight measurements were conducted using standardised protocols. The measuring instruments were all checked and calibrated before use. Children were instructed to remove their shoes, socks, hats and coats, and only wear lightweight underwear. Each measurement was conducted twice, and the average value was recorded for analyses. Each child’s body mass index (BMI) was calculated based on their height and weight, with the formula being weight divided by the square of height (kg/m2).
Definitions of overweight and obesity
In this study, the determination of overweight and obesity in children was based on the BMI growth curve for Chinese children and adolescents aged 0–18 years,32 with a diagnostic cut-off value of P85≤BMI<P95 for overweight and BMI≥P95 for obesity. After screening out children with overweight and obesity, the remaining participants were classified into non-overweight or non-obese groups. The nutritional status of the parents was evaluated using the diagnostic cut-off values from the Working Group on Obesity in China,33 with BMI values between 24 and 28 indicating overweight, values ≥28 indicating obesity and values <24 indicating non-overweight or non-obesity.
Questionnaire
In this study, a self-administrated questionnaire was used to investigated the health-related behaviours of caregivers, specifically focusing on exercise-related behaviours and diet-related behaviours. First, questions were selected based on previous studies34–36 and the exercise promotion guidelines outlined in the Healthy China Initiative (2019–2030), which was issued by the Chinese government in 2019.37 Furthermore, three senior professionals specialising in lifestyle and obesity aided to review the questionnaire. Ultimately, we conducted a pilot study involving 30 participants. Each primary caregiver was required to complete the questionnaire twice, with an interval of 2 weeks between each completion. The reliability coefficient is 0.889.
The final questionnaire comprised two primary sections (see online supplemental file 1). Part 1 contained inquiries regarding the sociodemographic characteristics of children and their families (children’s gender, date of birth, chronic illnesses, primary caregivers, parental heights and weights, educational attainment of parents, and annual family income), some variables were recoded using specific cut-points of grouping. Part 2 focused on investigating the caregivers’ exercise health behaviours and dietary health behaviours. In this context, exercise referred to aerobic activities of moderate intensity or higher, including brisk walking, running, cycling, jump rope exercises, swimming and more. The exercise frequency was categorised into three levels: <1 time per week, 1–2 times per week and ≥3 times per week. Additionally, the average duration of each exercise session was classified into three categories: <30 min, 30–60 min and ≥60 min. Furthermore, caregivers’ dietary health behaviours were assessed based on their frequency of consumption (≤1 time/week, 2–3 times/week and ≥4 times/week) of desserts (such as pies, cookies, cakes, ice cream and chocolate beverages), late-night snacks and fast food. In addition, the caregivers’ diet regularity and the frequency of promoting physical activity for their children were evaluated using a 5-point Likert scale. The frequency of these behaviours was categorised as never, rarely (<1 day/week), sometimes (1–2 days/week), often (3–5 days/week) or always (≥6 days/week). Responses indicating ‘always’ or ‘often’ were considered positive, while all other responses were deemed negative.
Supplemental material
All individuals conducting the survey were required to have a medical background and complete standardised training before the investigation. They needed to clearly explain the questionnaire’s content and filling methods to participants. These questionnaires were completed by the primary caregivers, reflecting their actual circumstances over the past month. These main caregivers were selected by the family based on their role as the individual primarily responsible for the child’s care and decision-making.
Statistical analysis
The data were analysed using SPSS software V.22. The count data are described in terms of cases and the constituent ratio (n (%)). Potential confounders were evaluated using a directed acyclic graph based on prior knowledge (online supplemental file 2). The final model included the following factors: parental education, nutritional status, annual family income, as well as the children’s gender and age. χ2 test was applied for comparisons between different groups of children, while a non-parametric test was used for ordered classified data. Additionally, variables with significant differences (p<0.05) in the univariate analysis were further included as covariates in multivariate analysis. A logistic regression model was used to determine the ORs and 95 CIs, for which overweight and obesity were used as the dependent variables, and the health-related behaviours of caregivers were used as the independent variable, after adjustment for potential confounding variables. In each case, a p<0.05 was considered to indicate statistical significance.
Supplemental material
Results
Study population characteristics
Table 1 presents the characteristics of the study population, taking child age and sex, primary caregiver, annual family income, and parental nutritional status into account. Among the 1967 participants, 986 (50.1%) were male and 981 (49.9%) were female. The proportions of participants aged 2–3 years, 3–4 years, 4–5 years and 5–6 years were 510 (25.9%), 729 (37.1%), 414 (21.0%) and 314 (16.0%), respectively. The caregivers included parents (n=1084, 55.1%), grandparents (n=863, 43.5%) and others (n=20, 1%). Among the included children, 102 (5.2%) were overweight, 183 (9.3%) were obese and 285 (14.5%) were overweight and obese. The distribution of overweight and obese did not show statistically significant differences between boys and girls. In terms of age distribution, the observed differences between various age groups were statistically significant (p<0.05). Children whose parents were overweight or obese had a greater prevalence of overweight or obesity than did those whose parents were not overweight or obese (p<0.05). There were no statistically significant differences in the prevalence of overweight/obesity among children with different caregivers or varying annual family incomes or among children whose parents had different education levels (p>0.05) (table 1).
Demographic characteristics of participant
Differences in childhood overweight and obesity among children whose caregivers had different health-related behaviours
Table 2 illustrates the disparities in childhood overweight and obesity based on caregivers’ health-related behaviours. The prevalence of overweight and obesity decreased with increasing caregiver exercise frequency(p<0.05), but no significant differences were found regarding caregivers’ duration of each exercise session. Besides, children whose caregivers frequently encouraged exercise had a lower prevalence of overweight and obesity than those whose caregivers did not (p<0.05). Additionally, caregivers who frequently consume sweets and fast food, as well as those with irregular diets, had children with higher rates of overweight and obesity (p<0.05). No significant differences were found in caregivers’ weekly late-night snack consumption or the proportion of vegetables and meat in their diets concerning childhood overweight and obesity prevalence (p>0.05).
Differences in overweight and obesity among children whose caregivers had different health-related behaviours
Logistic regression analysis of the relationship between caregivers’ health-related behaviours and overweight and obesity in children
After adjusting for the age of the children and parents’ nutritional status, logistic regression analysis was employed to assess the associations between caregivers’ health-related behaviours and the prevalence of overweight and obesity in children. Our findings revealed that compared with children whose caregivers exercised <1 time/week, those whose caregivers exercised ≥3 times/week had a lower likelihood of being overweight or obese (OR 0.643, 95% CI 0.417 to 0.990), while no significant association was observed for caregivers who exercised 1–2 times/week. Additionally, frequent encouragement from caregivers for children to engage in exercise was negatively correlated with childhood overweight/obesity (OR 0.513, 95% CI 0.352 to 0.749).
In contrast, children whose caregivers consumed sweets 2–3 times/week (OR 1.535, 95% CI 1.133 to 2.081) or ≥4 times/week (OR 1.916, 95% CI 1.258 to 2.918), as well as children whose caregivers consumed fast food ≥4 times/week (OR 2.298, 95% CI 1.349 to 3.914), were more likely to be overweight and obesity than children whose caregivers consumed these foods ≤1 time/week. Furthermore, caregivers’ irregular eating habits were positively associated with the occurrence of overweight and obesity in children (OR 1.485, 95% CI 1.056 to 2.089) (table 3).
Logistic regression analysis of caregivers’ health-related behaviours and the prevalence of overweight and obesity in children
Discussion
In the present study, we revealed an association between caregivers’ health-related behaviours and childhood overweight and obesity in Beijing. The development of overweight/obesity is influenced by a combination of genetic and environmental factors. Although an increasing number of obesity-related genes have been identified and confirmed, the significant increase in the overweight and obesity prevalence cannot be explained by genetic factors alone, which also suggests that we need to further explore the related environmental factors. Previous research has demonstrated a correlation between childhood obesity and the environmental factors present in preschools and schools.38–40 Additionally, the correlations between obesity and family factors such as parental nutritional knowledge,13 nutritional status14 and feeding attitudes41 have been studied in recent years. However, limited focus has been given to the impact of the health behaviours of children’s caregivers. In this study, we focused on caregivers’ exercise-related and diet-related health behaviours, and the results showed that both aspects had an impact on childhood overweight and obesity.
This study demonstrated that compared with a caregiver exercise frequency of less than once per week, a caregiver exercise frequency of three or more times per week was a significant protective factor against overweight and obesity in children; however, a caregiver exercise frequency of one or two times per week did not yield improvements in the outcomes of childhood overweight and obesity. In addition, encouragement of physical activity for children also served as a protective factor. Interestingly, the results showed that there was no significant correlation between the duration of each exercise session (<30 min, 30–60 min and ≥60 min) in caregivers and nutritional status in children. This finding implies that the regular exercise habits of caregivers are associated with children’s health outcomes. Garcia et al posited that parents may serve as exercise models, especially for younger children.42 One previous study showed that children with active parents tend to have higher activity levels.43 Another study on the influences of parental behaviour also indicated that increased parental club sport participation was associated with increased children’s club sport participation (OR mother=1.9, OR father=1.7).20 Additionally, shared activities between parents and children have been suggested as possibly increasing children’s physical activity levels.44 Furthermore, it is possible that physically active parents are more likely to provide support, such as transportation to facilities or sport events, as they put a higher value on physical activity.45 These may be the relevant mechanisms by which caregivers’ physical activity influences child physical activity and, ultimately, overweight/obesity risk. WHO recommends that adults have 150 min of moderate-intensity, or 75 min of vigorous-intensity physical activity, or equivalent, per week. However, insufficient physical activity is very common in modern society around the world. New data show that nearly one-third (31%) of adults worldwide, approximately 1.8 billion people, did not meet the recommended levels.46 Similarly, an epidemiological survey of 146 countries and regions revealed that 81% of children and adolescents worldwide have insufficient physical activity.47 Insufficient physical activity and sedentary behaviour increase the risk of overweight and obesity in children.48 WHO is calling on countries to promote and encourage sports through relevant measures. Caregivers must be reminded of their vital role in influencing their children’s health outcomes. It is essential to focus on caregivers’ exercise behaviours to effectively cultivate children’s exercise routines and prevent childhood obesity.
In terms of caregivers’ dietary health behaviours, the findings of this study indicated that irregular eating patterns among caregivers pose a risk for childhood overweight and obesity. Compared with the consumption of sweets or fast food one time or less per week, the consumption of sweets more than two times per week or fast food four times per week was positively associated with childhood overweight and obesity. However, an increased frequency of having late-night snacks did not contribute to a greater incidence of childhood overweight and obesity. The preschool period plays a pivotal role in shaping children’s eating behaviours.49 A randomised controlled trial showed that parent nutrition patterns significantly influence their preschool-age children’s healthy lifestyle habits. Specifically, parents in the intervention group who received health behaviour education curriculum showed a significant reduction in children’s junk food intake, while those who did not attend the course significantly increased their children’s junk food consumption.50 Sweets have greater appeal to children. Infants possess an inherent inclination towards sweetness from birth, which can be further influenced and reinforced through acquired exposure. In this survey, 33.3% of the caregivers reported consuming sweets two or more times per week, while 8.7% consumed them four or more times per week. The frequent consumption of sweets by caregivers may be easily observed, learnt and reinforced by children, leading to their excessive dependence on such foods. Relevant studies have indicated an excessive intake of sugar among children and adolescents.51 52 Studies conducted in China have also revealed that 25.8% of primary and middle school students consume sweets every day.53 Too much sweet food intake can result in imbalanced nutritional intake, reduced dietary diversity, and an increased risk of childhood overweight and obesity, and other chronic diseases.54 The family environment serves as the primary setting for children’s meals, and the healthy eating behaviours and preferences exhibited by family members and caregivers have a significant impact on children’s dietary habits through modelling.55 As primary role models and mentors for children, caregivers should exemplify appropriate health behaviours in their daily lives, curtail detrimental habits and guide children through personal conduct. Caregivers should be the target of future prevention programmes. This pivotal aspect plays a crucial role in the prevention and management of childhood overweight and obesity.
In this study, all children except those in the overweight and obese group were classified as ‘non-overweight/non-obese’, which included some children with underweight status. Among the 1967 children studied, 151 were underweight, representing 7.7% of the total. We reanalysed the data after excluding underweight children and found that our primary conclusions remained consistent (online supplemental file 3).
Supplemental material
Furthermore, this study was conducted before the COVID-19 pandemic, which has resulted in several long-term changes to individuals’ lifestyle behaviours, including the increased prevalence of online shopping, takeout services, virtual meetings and online learning. These shifts may contribute to a reduction in the level of physical activity that families and children engage in during these activities. Concurrently, the postpandemic era has also seen a heightened emphasis on health among the Chinese population, evidenced by a growing fitness trend and an increased focus on healthy eating.56 57 Although there have been notable lifestyle changes following the pandemic, the basic pattern of the family as an important component of a child’s growth environment has not fundamentally changed. In particular, family exercise and dietary habits, as one of the key factors in health-related behaviours, have existed both before and after the pandemic and continue to have an impact on childhood overweight and obesity. Therefore, we believe our research conclusions remain applicable in the post-COVID-19 context. In future research, these new factors from lifestyle changes after the epidemic should be considered.
Strengths and limitations
This study investigates the relationship of caregivers’ own health behaviours with overweight and obesity among children in China, where the prevalence of overweight/obesity is on the rise due to ongoing rapid development and transformation of social economy. In addition, the influence of confounding factors was effectively controlled by the multivariate logistic regression method.
This study also has several limitations. First, it should be noted that this was a cross-sectional study without longitudinal follow-up of children and caregivers, so causal relationships between risk factors and overweight/obesity cannot be determined. Second, the use of questionnaire surveys in this study may introduce certain subjectivity and recall bias. Additionally, the information collected on health-related behaviours and the family environment was limited in scope. Furthermore, the interactions and influences of multiple caregivers on a given child have not been adequately considered. Future studies should take these factors into consideration to enhance the comprehensiveness of the design and provide more valuable insights for preventing and controlling childhood overweight and obesity.
Conclusion
Our study revealed associations between the health-related behaviours of caregivers and childhood overweight and obesity. These insights suggest that we should pay attention to the influence of caregivers’ own health-related behaviours on children, and comprehensive prevention and control measures that are led by family and caregivers should be developed. Caregivers themselves should adhere to healthy exercise and dietary patterns, play a positive role in family life, and correct family sharing environments that are not conducive to children’s health, with the aim of preventing overweight and obesity in childhood.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Ethics Committee of Beijing Children’s Hospital, Capital Medical University, code no. 2018-k-99. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors thank all team members and participants for their support to this study.
References
Footnotes
Contributors WJ collected and analysed the data, and wrote the main manuscript text. JD and XL participated in the data collection and supervision. YH searched and analysed the relevant literatures. AL and XX designed the study and revised critically the manuscript. All authors reviewed the manuscript. XX is the guarantor.
Funding This study is funded by Beijing Hospital Authority, China (Grant No. XTZD20180404)).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.