Article Text

Abstract
Background Hospital-acquired venous thromboembolism (HA-VTE) is a significant patient safety concern contributing to preventable deaths. Internationally, estimating HA-VTE relies on administrative codes, in particular the International Classification of Disease (ICD) codes, but their accuracy has been debated. The Irish Health Service Executive (HSE) launched a National Key Performance Indicator (KPI) in 2019 for monitoring HA-VTE rates using the Australian Modification of ICD-10 (ICD-10-AM) codes.
Objectives This study aims to (1) describe the development of the national HSE KPI and determine the national HA-VTE occurrence rate per 1000 discharges in 2022; (2) assess the contribution of each VTE ICD-10-AM code to the national HA-VTE figure; (3) estimate the positive predictive value (PPV) of the HSE KPI against true HA-VTE, in a single large tertiary (Irish Model 4) hospital.
Methods A retrospective observational study used national data from Irish publicly funded acute hospitals, focusing on discharges from 2022. The HSE KPI was based on an assessment of HA-VTE as a rate per 1000 hospital discharges (as per the national metadata). Inclusion criteria were inpatient only, length of stay ≥2 days, age ≥16 years and non-maternity admission type (elective or emergency only). Maternity and paediatric hospitals were excluded.
The PPV was determined through a detailed review of HA-VTE cases identified through the HSE KPI from April 2020 to October 2022 in a single large tertiary referral centre and determining the proportion indicating a true HA-VTE. Data analysis employed GraphPad Prism (Horsham, PA, USA).
Results The national mean monthly HA-VTE rate was 11.38 per 1000 discharges in 2022. Pulmonary embolism (PE) without acute cor pulmonale (I26.9) was the most frequent contributor (59%). The mean PPV in the tertiary hospital was 0.37, with false positives attributed to acute illnesses, historical VTE coding errors and dual VTE diagnoses at admission.
Discussion HA-VTE is a preventable cause of morbidity and mortality, necessitating accurate measurement. Administrative codes, while cost-effective and timely, reveal limitations in precision. This study identifies opportunities to improve code accuracy, address coding challenges and enhance the PPV.
Conclusion This study provides valuable insights into estimated HA-VTE rates, the contribution of each individual ICD-10-AM code to the overall HA-VTE rate and the PPV of the measure. Ongoing refinement and quality enhancement are needed.
- Quality Improvement
- Quality in health care
- Information Extraction
- Ireland
- Retrospective Studies
- HAEMATOLOGY
Data availability statement
Data are available upon reasonable request. Data may be obtained from a third party and are not publicly available. All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Quality Improvement
- Quality in health care
- Information Extraction
- Ireland
- Retrospective Studies
- HAEMATOLOGY
STRENGTHS AND LIMITATIONS OF THIS STUDY
The study includes all adult medical and surgical patients discharged from publicly funded hospitals in Ireland during a 12-month period, providing a broad and representative sample for assessing the occurrence of HA-VTE.
This study introduces the development and implementation of a national KPI for estimating the HA-VTE rate in Ireland. It provides insights into the overall annual HA-VTE occurrence rate per 1000 discharges, the contribution of different VTE ICD-10-AM codes and the PPV of the HSE KPI in a single large hospital.
Estimating HA-VTE using this administrative dataset has a poor PPV; therefore its strength is largely in measuring rates of HA-VTE over time to identify patient safety concerns and monitor quality improvement efforts.
The estimation of the PPV is based on a sample of patients from a single large tertiary referral centre, potentially limiting the generalisability of the findings to other healthcare settings. The findings may not be generalisable to other countries, due to differences in clinical management, coding and data processing.
The determination of the PPV involves a thorough chart review by a multidisciplinary team, enhancing the accuracy and reliability of the PPV estimation.
Introduction
Venous thromboembolism (VTE) comprises deep vein thrombosis (DVT) and pulmonary embolism (PE) and is a large contributor to global disease burden, affecting millions of individuals every year around the world.1 Hospital-acquired VTE (HA-VTE) is defined as a VTE that happens either during or up to 90 days following hospitalisation.1 It is estimated that up to 50–60% of all VTE cases occur during or after hospitalisation, and HA-VTE is a leading preventable cause of hospital-associated mortality and morbidity.1–4 We have reported that HA-VTE accounts for at least 47% of all VTE events arising within the Ireland East Hospital Group (serving ~1 million individuals).5 VTE also causes serious morbidity in those who survive. Approximately 400 000 Europeans every year are diagnosed with chronic thromboembolic pulmonary hypertension and lower limb post-thrombotic syndrome.6 In addition to harming patients, HA-VTE can also impose increased length of stay.6 VTE is reported to be the leading hospitalisation-associated contributor to disability adjusted life years in middle- and low-income countries and is reported to be the second leading contributor in high-income countries.1
HA-VTE is potentially preventable by identification of patients with risk factors for VTE and bleeding and by administration of appropriate thromboprophylaxis to the patient whose risk profile warrants it.1 7 8
Baseline determination of HA-VTE rates is important when planning quality improvement initiatives aimed at improving patient safety by prevention of blood clots in hospitals.5 Estimation of HA-VTE rates at a population level often employs the use of administrative codes for VTE. International Classification of Disease (ICD) codes remain the most used method.9 Administrative codes are used to derive VTE rates in the perioperative period following hip or knee replacement by the Organisation for Economic Co-operation and Development (OECD)10 and Agency for Healthcare Research and Quality (AHRQ).11 VTE in any adult inpatient is measured as a hospital-acquired complication in Australia.12 Administrative codes are also used in research studies determining the rates of VTE occurrence.3 9 13 14 There is significant variability in the individual codes used in published literature and in patient safety measures. Moreover, while sensitivity of ICD codes for estimation of HA-VTE appears reasonable, and should of course be prioritised from a patient safety perspective, the positive predictive value (PPV) and specificity are reported to be low.3 5 15
The Irish Health Service Executive (HSE) started work towards developing a National Key Performance Indicator (KPI) estimating HA-VTE rate in Ireland in 2017, which was launched in 2019. This aims to provide hospitals with an estimate of their rate of VTE occurring during hospitalisation on a monthly basis and to act as a driver to improve prevention of VTE.
Following a period of data gathering, we aimed to conduct a descriptive analysis of data from the HSE HA-VTE KPI. Our objectives were (1) to determine the national annual estimated HA-VTE occurrence rate per 1000 discharges using the HSE KPI for 2022, (2) to determine the percentage contribution of each VTE Australian Modification of ICD-10 (ICD-10-AM) code to the overall estimated HA-VTE rate and (3) to estimate the PPV of the HSE KPI in a sample of patients from a single large tertiary referral centre (defined as a ‘model 4 hospital’ in Ireland).
For clarity, throughout the manuscript, the constitutional name of the state (Ireland) will be used and refers to the 26 counties also known as the ‘Republic of Ireland’.
Methods
Patient and public involvement
The HSE’s VTE work and this study have been carried out in close collaboration with our co-author AMO’N, representing Thrombosis Ireland. AMO’N has advised on the design and reporting on the study and will share results with patients and the public via Thrombosis Ireland.
Population and study design
Aims 1–3 were achieved with a retrospective observational study design.
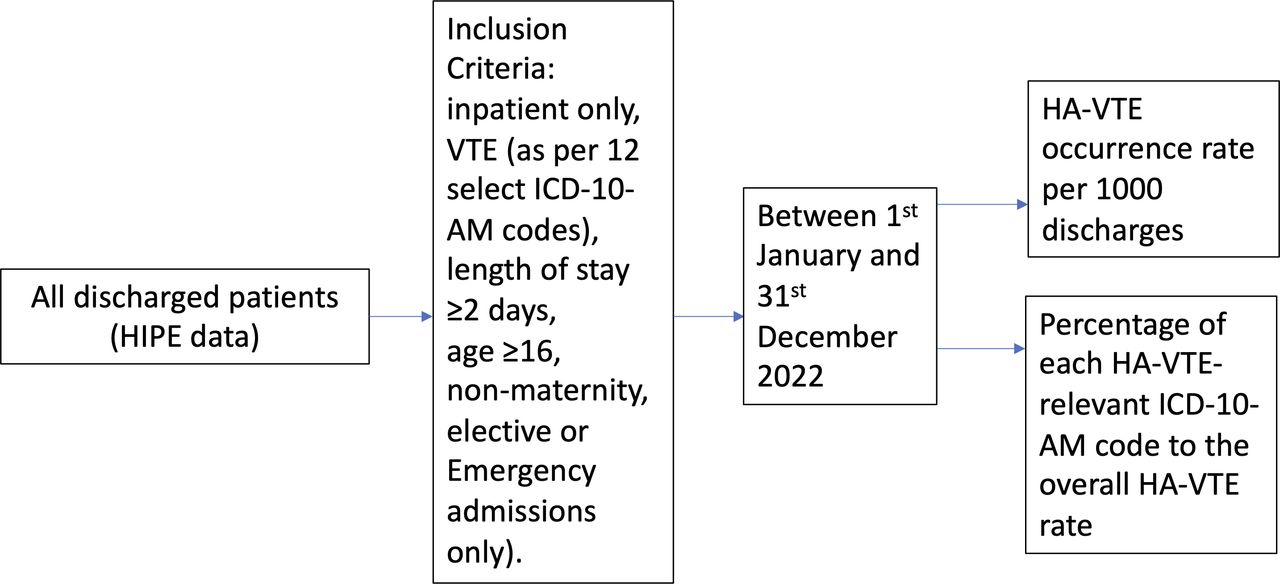
Figure 1 summarises the study methodology for aims 1 and 2, to determine (1) the HA-VTE occurrence rate per 1000 discharges in Ireland and (2) the percentage contribution of each HA-VTE-relevant ICD-10-AM code (table 1) to the overall estimated HA-VTE rate. The population was all patients discharged from a publicly funded hospital in Ireland in 2022, meeting inclusion criteria.

Study methodology for aims 1 and 2. HA-VTE, hospital-acquired venous thromboembolism; HIPE, hospital inpatient enquiry; ICD-10-AM codes, the Australian Modification of International Classification of Disease-10 codes; VTE, venous thromboembolism.
ICD-10-AM diagnosis codes (encompassing both pulmonary embolism and deep vein thrombosis) in UK NHS and Irish HSE-defined HA-VTE events
For estimation of (3) the PPV of the HSE HA-VTE, all patients from a single large tertiary referral centre (the Mater Misericordiae University Hospital (MMUH), Dublin), identified by the HSE KPI as having HA-VTE and discharged between 1 April 2020 and 31 October 2022, were included (figure 2).

{kind=link}
{kind=link}
Study methodology for aim 3. HA-VTE, hospital-acquired venous thromboembolism; HIPE, hospital inpatient enquiry; ICD-10-AM codes, the Australian Modification of International Classification of Disease-10 codes; VTE, venous thromboembolism.
Data source
The data source for this study was the consolidated hospital inpatient enquiry (HIPE) records of all Irish publicly funded acute hospitals.
HIPE data in Ireland are entered and validated at the time of a patient’s hospital discharge by trained HIPE coders. Data are extracted from medical records and from standardised discharge forms that are completed by a clinician caring for the patient. Following data entry by HIPE coders at the hospital level, further validation is undertaken by the centralised HSE HIPE Healthcare Pricing Office.
The ICD-10-AM codes are used in HIPE coding for all Irish publicly funded acute hospitals. In HIPE, the term ‘primary diagnosis’ is the diagnosis assigned as the principal reason for admission to hospital. The term ‘additional diagnosis’ refers to a diagnosis arising or diagnosed during hospitalisation, which includes hospital-acquired conditions.
Development of a national KPI estimating HA-VTE by administrative codes
In 2017, the Acute Hospitals and Quality Improvement Divisions of the Irish HSE were commissioned to start a work package aiming to estimate HA-VTE rates in Irish acute hospitals using administrative codes. A multidisciplinary team was assembled, and an iterative process was started in order to determine which administrative codes should be included as outlined in the next section.
We based the definition of suspected HA-VTE cases on ICD-10 discharge diagnostic codes for VTE outlined in the UK National Health Service Outcomes Framework (NHSOF) 2013/14 Technical Appendix (table 1), which guided UK-based quality improvement initiatives.3 7 16 We also referred to international VTE measures, including OECD,10 AHRQ11 and Australian12 measures, and studies from the United Kingdom,3 7 Sweden14 and Australia.13
The ICD-10-AM codes used to define HA-VTE in the Irish HSE are outlined in table 1, with UK national recommendations included for context. The rationale for inclusion and exclusion of particular codes is outlined further in online supplemental appendix 1.
Supplemental material
Final HSE definition for HA-VTE
The title of the final agreed HSE HA-VTE estimation method, which forms the national KPI, is ‘Rate of venous thromboembolism (VTE, blood clots) associated with hospitalisation’. The rate was calculated for patients discharged in 2022.
The numerator was the number of adult inpatient discharges with a length of stay of ≥2 days with an additional diagnosis of VTE *1000. ‘Additional diagnosis of VTE’ was defined as any of the ICD-10-AM codes listed in table 1 in positions 2–30. If more than one VTE additional diagnosis code was included in the patient’s discharge record, the VTE code in the highest position was the only code included. Inclusion criteria were inpatient only, length of stay ≥2 days (therefore excludes discharges with 0 or 1 overnight stays, as VTE occurring in short stays is unlikely to be HA-VTE), age ≥16 years and non-maternity admission type (elective or emergency only). Maternity and paediatric hospitals were excluded. VTE events managed through an ED-based ambulatory care pathway were not admitted and therefore not captured in the HIPE dataset. The denominator was the number of adult inpatient discharges with a length of stay of ≥2 days in the index month.
Determination of the PPV of the HSE KPI for HA-VTE
In order to estimate the PPV of the Irish HSE-defined KPI, a detailed review of suspected HA-VTE (defined by the HSE KPI) was performed in the MMUH. In this hospital, a VTE committee reporting to the hospital Quality Director performs a monthly detailed multidisciplinary review of all HSE-defined HA-VTE, including a detailed chart review by two consultant haematologists with a specialist interest in VTE, a quality manager, a senior pharmacist, thrombosis nursing staff and multidisciplinary clinical fellows. This represents the gold standard for VTE diagnosis.
The number of true and false positive HA-VTE events are determined on a monthly basis. The PPV was defined as the number of true positive events (predicted by administrative codes to represent HA-VTE and subsequently objectively verified to represent HA-VTE) divided by the sum of true positive events and false positive events (the latter being predicted by administrative codes to represent HA-VTE but subsequently determined not to be HA-VTE on review). The reasons for false positive HA-VTE codes were recorded.
Additional analyses
To estimate the contribution of dual VTE diagnosis at admission (PE and DVT codes, with one coded appropriately in an additional diagnosis position but present on admission) to the national HA-VTE rate, the proportion of patients with a VTE code in an additional diagnosis position but without a VTE code in a primary position were determined for the national VTE data for 2022.
We also reviewed whether the ‘Hospital-Acquired event’ flag available in the HIPE system was a reliable indicator of HA-VTE.
Descriptive statistics
Data were analysed using GraphPad Prism (Horsham, PA, USA). Categorical data were expressed as proportions and continuous data as mean±SD if normally distributed or median±interquartile range (IQR) if non-normally distributed.
Results
Determination of the overall annual estimated HA-VTE occurrence rate per 1000 discharges using the HSE KPI tool
Between January and December 2022, for inpatients ≥16 years discharged from an acute hospital with a length of stay of ≥2 days, the mean (SD) monthly numbers of HA-VTE cases and the number of discharges according to the above criteria were 253 (16) and 22 264 (997), respectively. The national mean monthly HA-VTE rate per 1000 discharges (SD) was 11.38 (1.02).
Determination of the percentage contribution of each VTE ICD-10-AM code to the overall estimated HA-VTE rate
The contribution of each VTE ICD-10-AM code to the overall HA-VTE rate is shown in table 2.
Contribution of each ICD-10-AM code to the overall HSE HA-VTE rate
The most commonly occurring VTE codes were I26.9 (Pulmonary embolism without mention of acute cor pulmonale) accounting for 59% and I80.2 (Phlebitis and thrombophlebitis in other deep vessels of lower extremities) with 22%. I80.1 (Phlebitis and thrombophlebitis of femoral vein) represented 9% and I82.8 (Embolism and thrombosis of other specified veins) accounted for 4%. Although maternity admissions and maternity hospitals were excluded, two cases of obstetric blood clot embolism (O88.2) were recorded, denoting women admitted with a medical or surgical condition while pregnant who developed VTE.
Estimation of the PPV of the HSE KPI in a large tertiary referral centre
Between April 2020 and October 2022 (inclusive), all HA-VTE events reported for the MMUH by the HSE were reviewed as described in Methods section. The median (IQR) number of discharges per month during this time was 1254 (1132–1286). The mean (SD) HSE-defined HA-VTE event monthly rate for the hospital was 18.7 (4.7) per 1000 discharges during this time, and the mean absolute number of events per month was 22.53 (5.78). The mean (SD) PPV was 0.37 (0.1), with a range of 0.22–0.56. The most common reasons for false positive HA-VTE reporting included (a) patients presenting with multiple acute illnesses (including acute VTE), such that the VTE was appropriately coded in an additional diagnosis position, but did not represent a HA-VTE; (b) prior historical VTE (not present on the current admission but erroneously coded in an additional diagnosis position for the current admission); (c) dual VTE diagnosis at admission (PE + DVT, with one coded appropriately in an additional diagnosis position while not representing true HA-VTE).
Additional analyses
The mean (SD) hospital proportion of VTE cases with a VTE code in an additional diagnosis position but not in the primary position was 0.89 (0.09). Further work could determine whether this represents a method by which the PPV of the KPI could be improved.
The median proportion of cases per hospital that had the ‘hospital-acquired event’ flag assigned was only 0.15 (95% CI 0.05 to 0.2), suggesting that searching only for cases that have been formally assigned a ‘hospital-acquired event’ flag is an unreliable method for HA-VTE case identification currently.
Discussion
In this study, we described the process through which HA-VTE was defined within the Irish HSE and reviewed the use of ICD-10-AM codes in the definition of HA-VTE. We reported that the national mean (SD) monthly HA-VTE rate according to this definition was 11.38 (1.02) per 1000 discharges. Finally, we reported a mean (SD) monthly PPV for the Irish HA-VTE definition of 0.37 (0.1) in a single large tertiary referral centre.
It is well established that healthcare ‘big data’ do not reach the same precision standards as research data.17 Administrative data based on ICD codes are inexpensive and readily available and can provide data pertaining to large numbers of patients with a short time lag before data are available.18 Healthcare ‘big data’ often inform funding decisions.
These ICD codes were developed to describe the prevalence of causes of morbidity and mortality and have subsequently been used for other purposes, including financial reimbursement and as patient safety measures. The accuracy of administrative data in quantifying clinical events may not always be optimal. Major challenges include clinical and coding interpretation and dependency on the completeness and clarity of clinicians’ notes. A lack of overlap between administrative coding and diagnostic test reporting has been reported, with 40% of ICD-coded VTE lacking a positive diagnostic test report and 45% of such reports lacking a corresponding ICD code in one study.17 The HSE KPI is not an absolute measure of true HA-VTE. The rates in a particular setting provide some insights for hospitals in comparision with similar hospitals, and for each hospital tracking its rates over time.
HA-VTE is potentially preventable with risk assessment and implementation of appropriate thromboprophylaxis.2 3 The Department of Health in England mandated the use of a VTE risk assessment tool in 2010 through the Commissioning for Quality and Innovation scheme.7 19 This patient safety programme has significantly reduced the incidence of and mortality from HA-VTE.3 7 An improvement collaborative increased the percentage of patients with appropriate prophylaxis in participating hospitals in Ireland, from 61% to 81%, using a quality improvement approach.20 Introduction of the HSE’s KPI was designed to facilitate monitoring the effect of patient safety efforts over time, with clinical and organisational governance both locally and nationally.
The extent to which administrative data identify HA-VTE correctly and reliably is an important question. To answer this question, VTE events flagged by administrative codes can be compared with a ‘gold standard’, often review of medical records, determining the PPV.21 Low PPVs have previously been reported on many occasions, ranging from ~30 to 80%.15 18 22–30 Even early studies such as Zhan et al suggested that close attention to validity is important when using administrative code-based event rate estimates for safety performance assessment.25 A recent analysis of data obtained from electronic health records found that ICD-10 codes had moderate to high pooled sensitivity (72%) and specificity (82%) for any VTE; higher for PE (91%) than for DVT (58%).31
The national mean (SD) monthly HA-VTE rate according to the current HSE definition was 11.38 (1.02) per 1000 discharges. Although similar data are collected elsewhere, comparison is challenging due to lack of public reporting of data and differences in what is reported. A similar rate was found in a cohort study, where 1.2% of medical non-intensive care inpatients developed HA-VTE during or after discharge, with an increasing rate over time.32 A recent study also reported an increasing incidence over time, with a lower overall incidence of 2.96 inpatient VTE events per 1000 hospitalisations.33Following hip and knee surgeries, Ireland had 597 VTE cases per 1 00 000 patients, which is above the OECD average at 467.10 UK data reported that a VTE rate determined from secondary diagnosis codes of just 1.08 per 1000 discharges in 2006–20o7, which rose rapidly in 2008, 2009 and 2010 and then declined to 1.21 in 2011, attributed to the patient safety programme in place.2 A previous Irish study identified potential HA-VTE by reviewing radiological records, then validating with clinical records, reporting an incidence of 4 cases of true HA-VTE per 1000 discharges.34 Although a mean of 11.38 patients had one or more HA-VTE codes recorded per 1000 discharges in our study, applying the PPV of 0.37 would yield a similar true HA-VTE rate of 4.22. Commentary in OECD reports suggests that some of the observed variations in DVT rates may be due to differences in diagnostic practices and differences in the way that countries report, code and calculate rates of adverse events. Higher rates may indicate more developed safety monitoring systems and a stronger patient safety culture. Improvements in coding and classification may drive the increased rates noted over time in many of the studies cited above. The usefulness of the HSE HA-VTE KPI currently is largely in measuring rates of HA-VTE over time to identify patient safety concerns and monitor quality improvement efforts.
Limitations
This study has some limitations. The HSE KPI is not an absolute measure of true HA-VTE, with a high rate of false positives identified in the single-centre study. The KPI examines in-hospital HA-VTE only and does not capture HA-VTE occurring after discharge, resulting in readmission or outpatient management. Readmission to the same hospital with VTE as a primary diagnosis was originally part of the KPI, but data were reported 5 months in arrears, to allow for readmission within 90 days of discharge. This resulted in the KPI being less useful as performance data, and the readmission portion was removed from the KPI. The rate of primary VTE admissions is also captured in HIPE data but not as part of the KPI. A proportion of these are readmissions with HA-VTE which occurred after discharge. Outpatient management of VTE is not captured in the HIPE system. Efforts are ongoing to provide a structure through which to capture such events. Furthermore, the comparison of data with those from other countries has a slight caveat, in that they more often than not have electronic and structured documentation. Much of the Irish documentation is a handwritten format and therefore less structured, so extracting data from this can be a challenge.
Future proposed work
Quality improvement initiatives are dependent on robust data. Our reported PPV for HA-VTE highlights the urgent need to improve coding of HA-VTE events, so that data can reliably inform policy on the success of VTE risk reduction protocols. While validation of each case would increase accuracy, it would not currently be feasible nationally.
A multidisciplinary working group has started a quality improvement initiative aimed at increasing the PPV of our HA-VTE definition, under the auspices of the National VTE Programme. We report that excluding cases in which VTE is also recorded as a primary diagnosis may reduce the number of false positive HA-VTE reports. Initial proposed Plan-Do-Study-Act (PDSA) cycles may include provision of guidance to HIPE coding colleagues and to medical practitioners, the introduction of a mandatory ‘flag’ for HA-VTE and integration with National Medical Imaging reports. Improvements in sensitivity and specificity of administrative codes for VTE are anticipated with wider implementation of electronic health records and the likely introduction of a unique patient identifier, facilitating data linkage.
Conclusion
This study outlines the development and implementation of a national KPI for estimating HA-VTE in Ireland, using ICD-10-AM administrative codes. There are challenges associated with using administrative codes for estimating HA-VTE, revealing the importance of validation and continuous quality improvement initiatives to address national and local variation. Limitations including potential underestimation of cases due to exclusion of readmissions and exclusion of certain DVT events managed in an ambulatory manner are important considerations.
The clinical, patient and economic impacts of VTE are enormous with well-established prevention programmes in other countries. The National Venous Thromboembolism Programme aims to understand and improve VTE prevention, management and treatment. The authors acknowledge the limitations of the current system and highlight the ongoing efforts to enhance the accuracy of HA-VTE data collection in Ireland, anticipating improvements with the future availability of electronic health records. Further examination of national VTE incidence rates and trends is vital.
In conclusion, this study contributes valuable insights into the development, implementation and evaluation of a national HA-VTE estimation mechanism in Ireland, emphasising the need for ongoing refinement and quality enhancement in using administrative codes for patient safety assessments.
Data availability statement
Data are available upon reasonable request. Data may be obtained from a third party and are not publicly available. All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Formal Research Ethics Committee approval was not required, as it was a national work programme commissioned by the HSE, reporting from an existing administrative dataset to improve quality and patient safety.
References
Footnotes
CK and RD are joint first authors.
X @ciarakirke, @fniainle
Contributors Submitting author: RD. CK, RD, TD, JC, RB, DL, MPC, BK, EG, AMO'N, FNA, reviewed and approved the final version of the manuscript. FNA is the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.