Article Text

Abstract
Objectives Public safety personnel (PSP) are responsible for ensuring the safety and security of communities, often putting their own lives and well-being at risk by performing dangerous and demanding work. As a result, these workers are particularly vulnerable to workplace-related physical and mental traumatic injuries. Research is needed to understand the mental health of PSP following traumatic physical injury to inform effective prevention programmes and interventions. The objective of this study was to investigate whether PSP with traumatic physical workplace injuries requiring surgery with anaesthetic have higher post-injury rates of mental disorders compared with the general population with similar non-workplace injuries.
Design Retrospective longitudinal cohort study.
Setting Population-based study using linked anonymised administrative data for PSP and the general population in Manitoba, Canada.
Participants This study compared two groups hospitalised for a traumatic physical injury requiring surgery with anaesthetic between 1 January 2002 and 31 December 2018: (1) PSP (n=293) injured in the workplace and matched 1:5 on sex, age, geographical region and surgical procedure code with (2) individuals in the general population (GenPop) injured outside the workplace (no Workers Compensation Board claim) (n=1198).
Primary and secondary outcomes and measures As planned in the study protocol, the prevalence of mental disorders including anxiety, depression and substance use was measured in the cohorts 2 years pre- and post-injury.
Results This study found an elevated unadjusted risk of depression in PSP compared with the general population in the 2 years post-injury, adjusting for pre-injury mental health (rate ratio, 1.49; 95% CI, 1.02 to 2.17; p<0.0001). After adjusting, there were no significant differences in rates between the two cohorts; however, the significant group × care interaction term for depression suggests a greater risk for PSP compared with GenPop over time.
Conclusions Our findings indicate that, compared with a matched cohort, PSP have an increased risk of depression from the pre-injury to post-injury period following a traumatic physical workplace injury. PSP have a unique mental health trajectory following workplace injury that should be considered when developing rehabilitation strategies for this important population.
- EPIDEMIOLOGY
- Trauma management
- Anxiety disorders
- Depression & mood disorders
- Health Services
Data availability statement
Data may be obtained from a third party and are not publicly available. Data cannot be shared publicly due to privacy and access restrictions through the Manitoba Centre for Health Policy (https://umanitoba.ca/manitoba-centre-for-health-policy/data-repository) and the Provincial Health Research Privacy Committee (https://www.rithim.ca/phrpc-submission-requirements).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This retrospective cohort study matched cases 1:5 with controls and used propensity score weighting in a generalised estimating equation model.
This study examines pre-injury and post-injury mental health.
Use of administrative data minimised risks found in other studies (eg, potential bias from loss to follow-up, data recollection issues and diagnostic criteria variability) and increased generalisability.
Administrative health data provide information on treatment prevalence (physician diagnosis or hospitalisation for mental disorders) which likely resulted in lower rates as many individuals with mental disorders do not seek care.
This study was unable to assess post-traumatic stress disorder (due to diagnostic coding limitations) and gender for both cohorts and the employment status of the general population cohort.
Introduction
Public safety personnel (PSP) are workers responsible for ensuring the safety and security of communities, often putting their own lives and well-being at risk by performing dangerous and demanding work. PSP occupations include, but are not limited to, firefighters, paramedics, police officers, correctional services officers, parole officers, courtroom security officers and general security guards.1 PSP perform challenging roles in dangerous conditions where repeated exposure to physically harmful situations (eg, fires, assaults and resuscitation in dangerous environments) and potentially psychologically traumatic events (eg, threatened or actual physical assaults, sexual violence and explosions)1–3 are the rule rather than the exception,1 and they experience these negative exposures at higher frequencies than the general public.3 4 As a consequence, the PSP population is uniquely vulnerable to experiencing workplace-related physical and psychological traumatic injury5–7 that may result in increased rates of mental health issues, such as anxiety, depression and substance use disorders.8 Recent research estimates PSP screen positive for probable mental disorders (anxiety, depression, substance use, and post-traumatic stress disorder (PTSD)) at a rate of 44.5%8 compared with the general population: 17.6% worldwide9 and 10.1% in Canada.10 Mental disorders in the general population are estimated to account for one-third of personal disability globally and equal respiratory and circulatory diseases in terms of disability-adjusted life-years.11 The economic burden of mental disorders is estimated to be in the billions of dollars in Canada12 and in the hundreds of billions of dollars in the USA.13 A large, population-based study in Australia found that first responders have a three times higher risk of making a worker’s compensation claim than other occupations14; thus, the proportionate individual and economic burden may be even more substantial for the PSP population. Manitoba Workers Compensation Board (WCB) data indicate that the mental illness burden in PSP is increasing, with 11 371 paramedic and firefighter hours lost due to mental health WCB claims in 2020 compared with only 5064 hours lost in 2019.15
There is a need to better understand the association between PSP work and a potentially increased rate of mental disorders.1 16 A large national survey study of PSP by Carleton et al found increased rates of depression, anxiety and substance abuse disorders due to staff shortages, lack of resources and training on equipment, leadership styles and inadequate support, among many other factors analysed.16 In addition, the study identified organisational and operational stressors of PSP such as fatigue from shift work and overtime, perceived risk of job-related injury and social life limitations as potentially psychologically traumatic events.16 This study is one of the most comprehensive analyses of factors contributing to mental disorders in PSP completed to date; however, it did not look at traumatic physical injury or traumatic physical injury requiring surgery. Given the increased severity of traumatic physical injuries (compared with all or non-traumatic physical injuries), the associated mental outcomes may differ. In the general population, traumatic physical injury has been shown to significantly increase post-injury rates of hospitalisation and physician visits for mental disorders, including anxiety, depression and PTSD, even after accounting for pre-injury mental disorders and physical comorbidities.17 There is an absence of published literature investigating how workplace traumatic physical injury requiring surgery might affect post-injury mental health in PSP. To address this gap, we conducted a longitudinal retrospective cohort study using administrative data to investigate whether PSP with traumatic physical workplace injuries requiring surgery have higher post-injury rates of mental disorders compared with the general population with non-workplace injuries that required surgery. This work will establish a much-needed foundation for further studies on how traumatic physical injury requiring surgery affects the risk of mental disorders in PSP and will inform enhanced mental healthcare strategies for this population.
Methods
Overview
This retrospective, whole-population, longitudinal, matched cohort study investigated post-injury rates of mental disorders in PSP who experienced a traumatic18 physical workplace injury requiring surgery with anaesthetic (‘PSP’) matched 1:5 with individuals from the general population who experienced a non-workplace traumatic physical injury requiring surgery with anaesthetic and did not have a WCB claim (‘GenPop’). Diagnoses of mental disorders (depression, anxiety and substance use disorder) were based on physician diagnoses and hospital discharge data.
Data sources
The registry from the WCB of Manitoba contains claim information from workers registered with the WCB. The Population Health Research Data Repository housed at the Manitoba Centre for Health Policy (MCHP) contains deidentified individual-level data for the population of Manitoba and is linkable across data sets anonymously via a unique scrambled personal health identification number.19 Using deterministic linkage, the WCB registry was linked to administrative data from several databases (Hospital Abstracts, Medical Services, Manitoba Health Insurance Registry and Vital Statistics Mortality) in the Repository.19 As stewards of the data held at MCHP, centre staff linked and cleaned the data set and provided the study team with an anonymised data set for analysis.
Study population
The initial population included all individuals with a WCB time loss claim for a workplace traumatic physical injury that required surgery with anaesthetic (see online supplemental material 1).20 Study criteria included ≥18 years of age between 1 January 2002 and 31 December 2018; valid Manitoba health insurance for at least 30 days post-index date and minimum 30 days’ WCB insurance post-index date. Exclusion criteria included individuals less than 18 years old; military personnel (due to no Manitoba PHIN number and the ‘healthy warrior effect’21) and specific types of injuries (traumatic brain injury, burns, repetitive strain and injuries stemming from chronic conditions such as arthritis, cancer and diabetes). These exclusion criteria reflect populations and factors known to either have a unique trajectory of mental health outcomes (traumatic brain injury and burns),17 22 23 occur over time (repetitive strain) or are not related to a specific traumatic event (chronic conditions). Next, specific occupations were selected for the PSP cohort (International Standard Classification of Occupations codes in parentheses): paramedics (3258), police officers (C5412), firefighters (C5411), correctional service officers (C5413), parole officers (5419) and sheriffs, bailiffs and security guards (C5414). This resulted in a population of 293 PSP. Due to the fixed study population, an a priori power analysis was not conducted. The comparison GenPop cohort included individuals who experienced traumatic physical injuries that required surgical intervention with general anaesthetic without a WCB claim.
Supplemental material
Matching
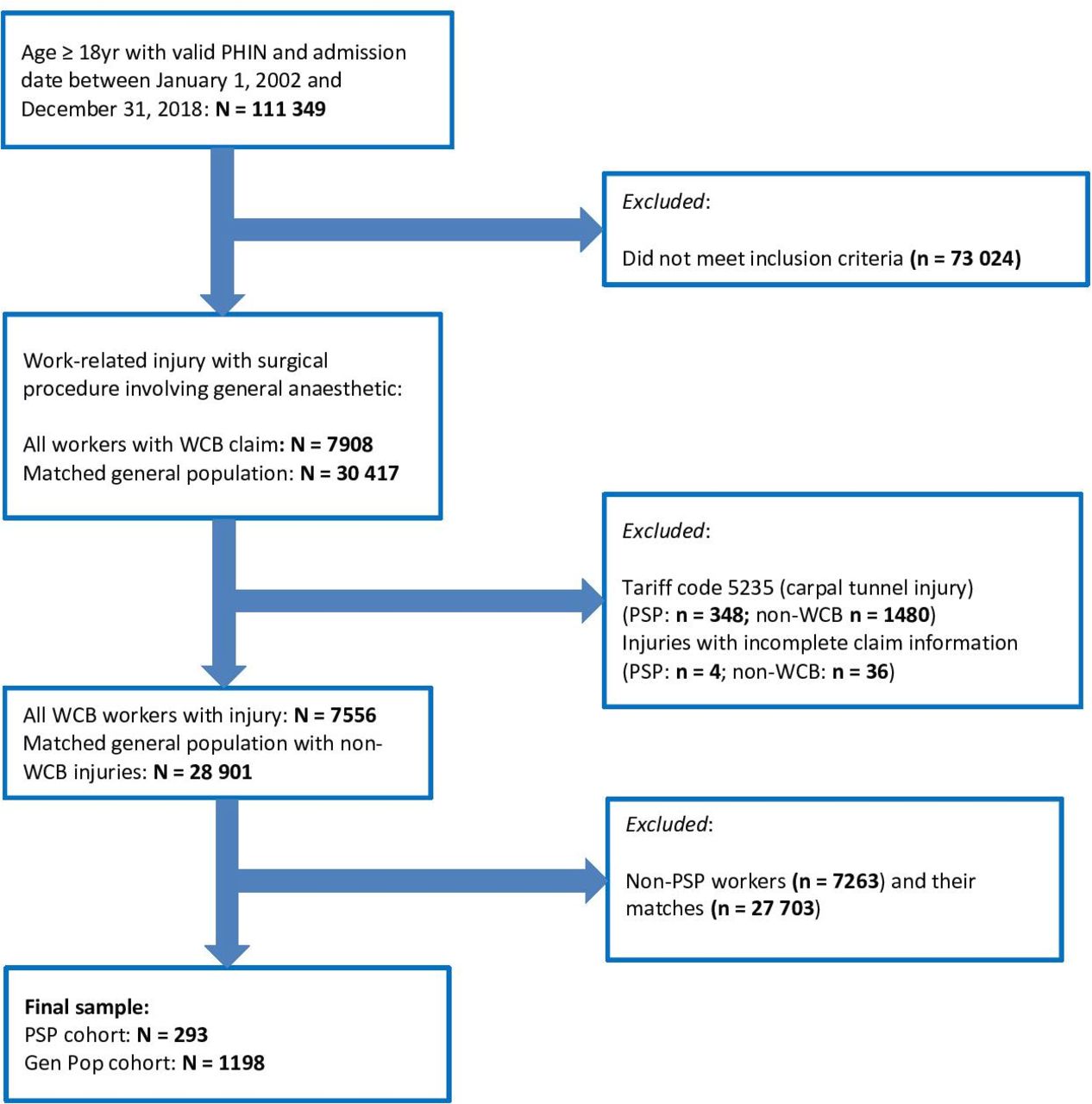
From a random sample without replacement, the PSP cohort was matched 1:524 with the GenPop cohort (who could not be in the WCB data set) on the following: age at index date ±2 years; sex (male, female); geographical region (residential postal code at index date) and surgical procedure billing code. Cases were matched in an iterative process until all potential matches were included or five matches per case were achieved. Only individuals who met the study criteria were matched; therefore, there were no unmatched cases. There were 293 PSP and 1198 GenPop in the final population. A study population flow diagram25 is shown in figure 1.

{kind=link}
Study population flow diagram. GenPop, general population; PSP, public safety personnel; WCB, Workers Compensation Board.
Outcome variables
Diagnoses of mental disorders (anxiety, depression and substance abuse) were examined 2 years pre- and post-index date. The 2-year period was chosen to allow enough time for disorders to develop but not too much that disorders may develop due to other causes.17 These disorders were chosen due to their association with traumatic physical injury,17 26 their occurrence in response to stressors and availability in the MCHP data repository. Accounting for these disorders in the 2-year pre-injury period is important to assess the impact of the injury on mental health, including if rates have changed over time. The 2-year follow-up period was chosen to allow time for mental disorders to present in physician and hospital billing data and minimise new confounding variables affecting the development of mental disorders (ie, another injury). The presence of mental disorders was assessed using the following International Classification of Diseases (ICD) codes (ICD-9-Clinical Modification (ICD-9-CM) and ICD-10-CA): anxiety (ICD-9-CM: 300.0, 300.2, 300.3; ICD-10-CA: F40, F41.0, F41.1, F41.3, F41.8, F41.9, F42, F43.1); depression (ICD-9-CM: 296.2–296.3, 296.5, 300.4, 309, 311; ICD-10-CA: F31.3-F31.5, F32, F33, F34.1, F38.0, F38.1, F43.2, F43.8, F53.0) and substance use disorders (ICD-9-CM: 291, 292, 304, 305, 303; ICD-10-CA: F10-F19, F55). ‘Any mental disorder’ combined anxiety, depression and substance use disorders into one variable. Dichotomous variables of one or more outpatient visits (physician billing) and/or one or more hospitalisations during the pre- or post-index period were considered an outcome diagnosis. Coding for these outcomes is based on validated diagnostic definitions for the Manitoba population.27 28
Statistical analysis
Data analysis followed a similar framework used by our team in previous studies17 29 30 and reflects a larger WCB study analysis strategy. Descriptive statistics for the PSP and GenPop cohorts were calculated using Student’s t-tests for continuous variables and χ2 tests for categorical variables. Injury source, type and anatomical location were calculated for PSP. Two-sided tests at α=0.05 were used. Contingency tables were generated to examine mental health diagnoses pre- or post-index date for PSP relative to GenPop, resulting in unadjusted ORs.
Generalised estimating equations (GEE) for each mental disorder grouping were created to account for correlations among repeat observations of longitudinal data and31 corrected with a ‘repeated measures’ statement in the models. GEE with a Poisson distribution was used to calculate adjusted rate ratios (ARRs) for comparing study cohorts. An average treatment effect (ATE) was estimated and used as a propensity score weight applied in the GEE model. The ATE balances membership in the cohorts.32 In addition, a time offset (log of end of study date – index date for each individual) was included to account for the effect of time in the study for each participant in the GEE model. The structure of the GEE included group (cohort); pre-index date period or post-index date period (‘care period’); income; sex; geography and a ‘group × care period’ interaction term. This interaction term examined the presence of pre-injury mental disorders potentially affecting the relationship between the injury and rates of post-injury mental disorders and how this varied between the two groups over time.17All statistical analyses were performed using SAS V.9.4 (SAS Institute Inc., Cary, NC, USA).
Data weighting
To mitigate bias between study cohorts, inverse probability treatment weighting (IPTW) was used in the analyses.30 32 To calculate IPTW, propensity scores were generated from a logistic regression model which included binary indicators: group (case, match); sex (male, female); geographical region (urban, rural) and income (high, low). These variables were common to all eligible participants, and only individuals with complete data were included; therefore, there were no missing data in the propensity score estimation. Further, assumptions of propensity score analysis were satisfied.33 Comparisons of individual propensity score distributions showed sufficient overlap; therefore, IPTW would yield a comparable distribution of variables between the cohorts, confirming the feasibility of comparing the treatment groups.30 32
Patient and public involvement
There was no patient or public involvement in this study.
Results
A fixed population of 293 individuals met the criteria for inclusion in the PSP cohort and were matched with 1198 individuals in the comparison cohort. Table 1 includes descriptive characteristics. The average age of the PSP cohort was 41 years old, 20.8% were female and 65.9% resided in an urban region. There were no significant differences in age, sex or geographical region between study cohorts; however, PSP had higher income (p=0.0017).
Descriptive characteristics of cohorts
Table 2 details the injury characteristics of the PSP cohort, including injury source, injury type and anatomical location. The most common injury sources were bodily motion or position (eg, twisting or extending reach) (30.7%), followed by environment (eg, standing for an extended period or working in extreme conditions) (23.2%), people (eg, accidental or intentional injury caused by another person) (22.5%) and objects (eg, machinery, hand tools, ladders) (19.1%). The most common type of injury was sprains, strains and tear injuries (62.8%) followed by fractures and dislocations (16.7%), systemic diseases and disorders (9.9%) and cutaneous injuries (5.1%). For anatomical location of injuries sustained, the most common location was the upper extremities only (41.3%) followed by lower extremities only (37.5%); multilocation injuries and head/neck injuries were the least common (10.9%).
Characteristics of PSP cohort (n=293)
Table 3 includes crude ORs for mental disorders in both cohorts 2 years pre- and post-injury. No significant differences in the unadjusted rates of mental disorders measured pre-injury between PSP and the GenPop cohort were found. Post-injury, the PSP cohort had higher unadjusted rates of depression (14.3% vs 10.1%) compared with the GenPop cohort (OR, 1.49; 95% CI, 1.02 to 2.17; p<0.0001). Rates of substance use disorder were not reported due to privacy constraints preventing reporting of small case numbers.
Crude ORs of mental disorders in cohorts pre- and post-injury
Table 4 compares ARRs for both cohorts during the pre- and post-injury periods and a ‘group × care period’ interaction term to assess differences in mental disorder rate changes between study cohorts over time. There was a significant group × care period interaction for depression (p=0.014); however, there were no differences in adjusted relative rates of mental disorders between cohorts in either the pre- or post-injury periods. Table 5 includes ARRs for model covariates (measured at the time of injury).
ARRs of mental disorders in cohorts pre- and post-injury
ARRs for model covariates
Discussion
This longitudinal comparative cohort study found that, after adjusting for pre-injury mental health, PSP with a traumatic physical workplace injury had higher relative rates of depression post-injury compared with the general population with similar non-workplace injury. This study advances the literature through the use of longitudinal administrative data linked with workers’ compensation data, physician-diagnosed mental disorders, consideration of pre-injury disorders and inclusion of a matched cohort. The cohorts were similar in demographic variables except for income. This is likely due to PSP occupations having higher incomes compared with the average of all occupations; in 2021, the median annual individual income for PSP in Canada was $102 30034 and $51 600 for employment in the general population.35
This study found that relative rates of depression significantly increased from the 2-year pre-injury period to the 2-year post-injury period for the PSP cohort compared with the matched cohort. This finding is supported by Canadian literature that found organisational and operational workplace stressors for PSP are significantly associated with depression.16 It is possible that a difference was not found for other mental disorders due to the inability to detect other changes with the smaller study population or that, as expected, anxiety is more common in women36 and the population for this study was largely male. In addition, PSP with a work-related injury may have a different trajectory of mental health services use following surgery than those in the general population. Mental health service use differences may be due to ongoing higher levels of occupational stress and trauma in the background or challenges in healthcare-seeking and physician practices (ie, billing only for the injury and no other patient concerns such as mental health).
Strengths
Strengths of this research include being the first study to investigate how traumatic physical injury requiring surgery affects rates of post-injury mental disorders in the PSP population. Second, this study addresses significant gaps in the PSP literature by including administrative data, all categories of PSP populations, the majority of Axis I mental disorders and individuals’ pre-injury mental health in the comparison. Previously, the literature was limited to mainly survey-based studies (which are susceptible to biases in sampling, non-response and social desirability) and limited to one category of PSP per study (eg, only police). Third, including administrative data minimised the risks found in other studies (eg, potential bias from loss to follow-up, data recollection issues and diagnostic criteria variability) and increased generalisability. Fourth, robust matching (age, sex, geographical region and surgical procedure code) and using IPTW reduced bias from potential differences between cohorts.
Limitations
Limitations of this study include, first, the inability to examine some variables in the analysis due to the limits of administrative data. Specifically, we were unable to differentiate a diagnosis of PTSD (a common outcome for workplace events of PSP)37 from other anxiety disorders as the second decimal place for ICD codes which would identify PTSD was not available. Further, physician diagnoses were limited to one ICD code at the time of this study; other conditions that may have been present would not be recorded and, therefore, missing from the data. This limitation may explain why there was a decrease in substance abuse disorders post-injury when there was an increase in depression. Similarly, we were not able to examine gender, as the administrative data we used only record sex, and the employment status or occupation of individuals in the matched cohort was not available in the data sets. Just over one-fifth of PSP injuries were caused by ‘people’; however, information on whether the injury was intentional (ie, aggression) or accidental was not available in the data sets. This is a limitation as intentional injuries may have a greater negative impact on mental health.38 In addition, there may be differences in mental health status based on other stressors/traumas experienced by PSP that we could not examine in the administrative data.16 39 Second, although the study included a fixed population, the smaller population size reduced the ability to detect some differences in outcomes between the cohorts and to stratify analyses. We were unable to stratify analyses by occupation category and sex due to the population size and the smaller proportion of females in the study. This meant we were unable to determine whether there was a greater risk of mental disorders for one sex or occupational category. Among first responders, females have higher rates of making a compensation claim, and there is an increased risk of mental health conditions among police officers compared with other categories.14 Third, the study outcomes reflect treatment-seeking (physician diagnosis or hospitalisation for mental disorders) which does not reflect symptomology or functioning and likely resulted in lower rates as many individuals with mental disorders do not seek care.40 41 Further, PSP workers experience significant stigma surrounding mental disorders and accessing mental healthcare that may reduce help-seeking.1 42 Lastly, there may be differences in the rates of employment between the two cohorts which may be an avenue for further investigation.
Implications
These findings highlight the importance of further attention to the mental health of PSP following workplace injury and the need for ongoing support. Interventions that provide mental health support at the time of hospitalisation for injury and ongoing monitoring of mental health may prevent or mitigate later development of mental disorders in this population.
Future directions
Findings from this study indicate that PSP have an increased rate of depression and worse mental health trajectory over time following a traumatic physical workplace injury compared with the general population with similar non-workplace injuries. This study has established a much-needed foundation for further work on how traumatic physical injury requiring surgery may impact mental health in PSP. Future research directions include using other provincial and national databases to expand the cohort of PSP which would improve power and better elucidate differences in rates of mental disorders between cohorts; investigating rates of mental disorders following workplace injuries for specific PSP occupations and between sexes and comparing the current PSP cohort to another cohort consisting of non-PSP workers with similar traumatic physical workplace injuries. Lastly, future work to explore links between depression, PSP work and workplace injury and understanding optimum periods for improved prevention and intervention strategies to reduce the large burden of mental health in PSP is essential.
Conclusion
This study found that traumatic physical workplace injury requiring surgery is a risk factor for PSP developing depression post-injury, and there are likely factors unique to the PSP population that contribute to the increased rate of depression following injury compared with the general population. PSP have a unique mental health trajectory following workplace injuries that should be considered when creating improved rehabilitation strategies for this important population.
Data availability statement
Data may be obtained from a third party and are not publicly available. Data cannot be shared publicly due to privacy and access restrictions through the Manitoba Centre for Health Policy (https://umanitoba.ca/manitoba-centre-for-health-policy/data-repository) and the Provincial Health Research Privacy Committee (https://www.rithim.ca/phrpc-submission-requirements).
Ethics statements
Patient consent for publication
Ethics approval
Ethics approval for this study was obtained from the University of Manitoba Health Research Ethics Board (#HS22307(H2018:428)) and the Provincial Health Research Privacy Committee (#2018/2019-54).
Acknowledgments
The authors acknowledge the Manitoba Centre for Health Policy (MCHP) at the University of Manitoba for use of data contained in the Manitoba Population Research Data Repository under project HIPC# 2018/2019-54 and the Workers Compensation Board of Manitoba (WCB) for data from the WCB Registry. Data obtained from the MCHP Repository were derived from data provided by Manitoba Health. The results and conclusions are those of the authors and no official endorsement by the Manitoba Centre for Health Policy, Manitoba Health or Workers Compensation Board of Manitoba is intended or should be inferred.
References
Footnotes
Contributors SL is the guarantor. SL, DC, JiS, JB and AK conceptualised and designed the study and acquired funding. JG, DC, SL, LB and AW conducted data analysis. RS, JG, LB, AW, BC, JaS, DC, JB, TT, AK, AM, TOA, JiS, NM, JN and SL contributed to interpretation of the data and study conclusions. RS, SL, JG, LB and AW wrote the first draft. BC revised subsequent drafts and incorporated author feedback. All authors read, provided feedback and approved the final manuscript.
Funding This work was supported by a Research and Workplace Innovation Program (RWIP) grant (2015) from the Workers Compensation Board (WCB) of Manitoba.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.