Article Text

Abstract
Objective This study examined real-world treatment patterns and outcomes in patients with melanoma brain metastasis (MBM) treated with first-line immunotherapy consisting of nivolumab plus ipilimumab or anti-programmed death-1 (PD-1) monotherapy (nivolumab or pembrolizumab) or targeted therapy consisting of BRAF/MEK inhibitors.
Design Retrospective chart review study.
Setting Academic medical centres, community hospitals and private practice offices.
Participants Included patients diagnosed with melanoma with brain metastasis in the USA.
Outcome measures The statistical analysis was descriptive in nature. Overall survival (OS) and progression-free survival (PFS) were estimated using the Kaplan-Meier method and compared between treatments in a univariate Cox proportional hazards model.
Results In total, 472 patients with MBM who received first-line nivolumab plus ipilimumab (n=246), anti-PD-1 monotherapy (n=112) or BRAF/MEK inhibitors (n=114) were identified. Patients receiving nivolumab plus ipilimumab, compared with patients receiving anti-PD-1 monotherapy or BRAF/MEK inhibitors, had favourable baseline prognostic factors, such as younger age, fewer or smaller brain metastases, better Eastern Cooperative Oncology Group performance status and less frequently elevated lactate dehydrogenase. Median follow-up times were 15.4 months (range 0.1 to 37.0), 13.3 months (range 0.3 to 36.6) and 13.9 months (range 1.9 to 36.5), respectively. Numerically longer OS was observed with nivolumab plus ipilimumab versus anti-PD-1 monotherapy (HR 0.47, 95% CI 0.34 to 0.67) or BRAF/MEK inhibitors (HR 0.72, 95% CI 0.50 to 1.04) and numerically longer PFS was observed with nivolumab plus ipilimumab versus anti-PD-1 monotherapy (HR 0.74, 95% CI 0.53 to 1.02) or BRAF/MEK inhibitors (HR 0.82, 95% CI 0.60 to 1.12). With nivolumab plus ipilimumab, anti-PD-1 monotherapy and BRAF/MEK inhibitors, 1-year OS rates were 79%, 60% and 72%, respectively; 1-year PFS rates were 68%, 58% and 59%.
Conclusions In this real-world study, first-line nivolumab plus ipilimumab appeared to provide benefit versus anti-PD-1 monotherapy and BRAF/MEK inhibitors in patients with MBM, consistent with pivotal trial data. However, the observed benefit may have been due to confounding and selection bias, given that patients receiving nivolumab plus ipilimumab had favourable baseline prognostic factors compared with patients receiving anti-PD-1 monotherapy or BRAF/MEK inhibitors.
- Dermatological tumours
- Adult oncology
- Neurological oncology
Data availability statement
Data are available upon reasonable request. Interested researchers may request access by contacting the corresponding author or Bristol Myers Squibb directly by submitting an inquiry through the following link: https://www.bms.com/researchers-and-partners/independent-research/data-sharing-request-process.html. Access will be subject to Bristol Myers Squibb’s policies and may require a data use agreement.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This retrospective chart review study collected real-world data of US patients diagnosed with melanoma brain metastasis and treated by medical oncologists with different types of first-line systemic therapy options, including immunotherapy and targeted therapy.
This real-world study may have been limited by heterogeneity in baseline patient characteristics between the treatment groups.
There may have been inconsistencies in investigator assessments and treatment selection between the treatment groups.
Interpretation of these results was impeded by small sample sizes in certain subgroups.
Treatment practices may have changed since patients began treatment in this study.
Introduction
Metastasis to the brain is a common sequela of metastatic melanoma, with 35% of patients presenting with brain metastasis at diagnosis,1 more than 40% developing brain metastasis during their disease2 and up to 75% having brain metastasis at the time of death.3 Historically, patients with melanoma brain metastasis (MBM) have demonstrated a poor prognosis, with a median overall survival (OS) of approximately 4 months.4 BRAF mutations are present in the tumours of approximately half of the patients with advanced (unresectable or metastatic) melanoma, and patients with BRAF mutations have a higher likelihood of developing brain metastasis and experiencing shorter OS than those without these mutations.5 Prognosis for patients with MBM has improved in recent years with therapeutic advances,6 but outcomes remain poor in a substantial number of patients, suggesting an area of unmet clinical need.
Primary therapeutic approaches for patients with MBM have traditionally consisted of surgery, whole-brain radiotherapy and stereotactic radiosurgery.7 Over the last decade, several systemic treatments showing activity in MBM have been introduced, including immunotherapy (immune checkpoint inhibitors) with the combination of nivolumab (an anti-programmed death-1 (PD-1) antibody) plus ipilimumab (an anti-cytotoxic T lymphocyte antigen-4 (CTLA-4) antibody),8–11 the combination of pembrolizumab (an anti-PD-1 antibody) plus ipilimumab12 and nivolumab9 10 or pembrolizumab13 monotherapy as well as targeted therapy with BRAF plus MEK inhibitor combinations (indicated for patients with tumours harbouring a BRAF mutation) such as dabrafenib plus trametinib14 and encorafenib plus binimetinib.15 Patients with MBM enrolled in clinical trials have been broadly separated into those with and without symptoms, with symptomatic patients showing worse outcomes than asymptomatic patients.8 10 14 Steroids are the mainstay treatment for symptoms of MBM, such as headache, weakness and focal neurological deficits, although steroid therapy may abrogate the clinical effects of immunotherapy.16
Nivolumab plus ipilimumab has demonstrated intracranial activity in patients with MBM, especially those with asymptomatic disease.8–11 In the phase 2 CheckMate 204 trial, patients with asymptomatic (n=101) and symptomatic (n=18) MBM treated with nivolumab plus ipilimumab demonstrated 3-year OS rates of 72% and 37%, respectively.8 In the phase 2 ABC trial, patients with asymptomatic MBM treated with nivolumab plus ipilimumab (n=35) demonstrated a 5-year OS rate of 51%.9 10 In phase 3 Italian NIBIT-M2 trial, patients with untreated, asymptomatic MBM receiving nivolumab plus ipilimumab (n=27) showed a 7-year OS rate of 43%.11 According to the National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology (NCCN Guidelines), nivolumab plus ipilimumab is the preferred systemic therapy option for patients with asymptomatic MBM who do not require steroids in comparison with anti-PD-1 monotherapy or dabrafenib plus trametinib, based on superior intracranial activity.17
Until recently, comparative data on the use of systemic agents for the treatment of patients with MBM were limited, as this population was often excluded from randomised clinical trials. Furthermore, there are no prospective head-to-head trials comparing nivolumab plus ipilimumab with anti-PD-1 monotherapy or BRAF/MEK inhibitors in patients with MBM. There is interest in examining the effectiveness and use of these first-line systemic treatments among patients with MBM in the real-world setting because these patients may more closely reflect routine clinical practice compared with patients in clinical trials. The objective of this retrospective chart review study is to examine real-world treatment patterns and clinical outcomes in US patients with MBM treated with different types of systemic therapy options in the first-line setting.
Methods
Study design
This study collected the real-world data of patients diagnosed with melanoma with brain metastasis who were treated by US medical oncologists in academic/cancer centres, community hospitals/cancer centres and private practice offices. Study recruitment employed a two-part design in which a random sample of patients with BRAF mutant or wild-type metastatic melanoma with brain metastases (n=250) was identified first, followed by the identification of an augmented BRAF mutant sample (n=113) and an augmented BRAF wild-type sample (n=125) (online supplemental figure 1).
Supplemental material
Physicians who met the study requirements were contacted by a recruitment group (Global Perspectives), and those who were interested in participating were screened to confirm eligibility. A total of 44 oncologists who were currently treating patients with advanced melanoma were recruited, 40 of whom identified patients. Participating physicians were responsible for chart data abstraction and resolution of data-related queries. Physicians were instructed to identify and enrol patients with advanced melanoma diagnosed with brain metastasis who met the inclusion and exclusion criteria. No additional direction or restrictions were provided to physicians for identifying patients.
Patients
To be eligible, patients were required to have been diagnosed with both metastatic/stage IV melanoma and MBM between June 2017 and June 2019; to be 18 years of age or older; and to have a medical history available for medical chart abstraction from initial melanoma diagnosis through the most recent visit, current therapy or death. Patients were excluded if they had used systemic therapy in the metastatic setting prior to the development of brain metastasis (see criteria for adjuvant therapy below); had received whole brain radiotherapy (other forms of radiotherapy, such as stereotactic radiosurgery, as allowed); had undergone surgical resection for brain metastasis; had a diagnosis of concurrent malignancy (other than non-melanoma skin cancer or in situ cervical carcinoma); or were enrolled in a cancer-related clinical trial since diagnosis of metastatic melanoma. Prior use of adjuvant or neoadjuvant therapy with anti-PD-1 monotherapy, anti-CTLA-4 monotherapy or BRAF/MEK inhibitors was allowed if 6 or more months had elapsed between the last dose of therapy and diagnosis of brain metastasis, as previously defined.18
Endpoints
Primary endpoints included treatment patterns in the first-line setting. Secondary endpoints included OS and progression-free survival (PFS). OS was defined as the time from the index date (start of first-line treatment in the metastatic setting) to the date of death from any cause. PFS was defined as the time from the index date to the date of the first disease progression. OS and PFS were described by type of first-line treatment, which were nivolumab plus ipilimumab, anti-PD-1 monotherapy (nivolumab or pembrolizumab) and BRAF/MEK inhibitors (only for patients with BRAF mutant disease). Patients were stratified by BRAF wild-type or mutant status and by asymptomatic or symptomatic MBM. Concurrent steroid use was evaluated to identify patients with symptomatic MBM, which was defined as any steroid therapy received within 15 days before the start of first-line treatment. The 15-day window was selected to ensure that steroid administration was not likely because of immune-related adverse events (AEs) associated with immunotherapy. OS and PFS for the three types of systemic treatments were also estimated for patients according to the use of radiation, with concurrent radiation defined as radiation therapy that was initiated less than 30 days before or after the start of first-line treatment and sequential radiation defined as radiation that started 30 days or more before/after first-line systemic treatment initiation. Tumour response was not reported because response evaluation was inconsistent among investigators, on-treatment lesion measurements were not collected, response criteria were not defined in the case report form (CRF) and centralised confirmation of radiographic images was not conducted.
Statistical analysis
The statistical analysis was descriptive in nature and precision estimates were determined using 95% CI rather than power calculations for each cohort. Median OS and PFS were estimated using the Kaplan-Meier product-limit method. HRs and corresponding CIs were estimated using a univariate Cox proportional hazards model to compare OS and PFS between the three types of systemic treatments. All analyses were performed using SAS Enterprise V.9.4.
Patient and public involvement
Patients or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Results
Baseline patient characteristics
In total, 488 patients were identified for the analysis (online supplemental figure 1). A total of 472 patients with a confirmed diagnosis of metastatic/stage IV melanoma with MBM received first-line systemic treatment with nivolumab plus ipilimumab (n=246), anti-PD-1 monotherapy (nivolumab or pembrolizumab; n=112) or BRAF/MEK inhibitors (n=114) (table 1). Among the 472 patients, 50% (n=236) had BRAF wild-type disease, 45% (n=212) had BRAF mutant disease and 5% (n=24) had missing BRAF status. Patients treated with nivolumab plus ipilimumab tended to be younger than those treated with anti-PD-1 monotherapy or BRAF/MEK inhibitors (median age, 61.0 years vs 69.0 years and 62.0 years, respectively). At baseline, patients treated with anti-PD-1 monotherapy or BRAF/MEK inhibitors were more likely to have a greater number of or larger brain metastases, poorer Eastern Cooperative Oncology Group performance status (ECOG PS), greater frequency of increased lactate dehydrogenase (LDH), worse Charlson Comorbidity Index (CCI) scores and greater frequency of steroid use before the index date than patients treated with nivolumab plus ipilimumab. No patient received prior combination immunotherapy in the adjuvant or neoadjuvant setting per the data collected in the charts.
Baseline characteristics of patients with MBM by first-line systemic therapy*†
Follow-up time
Median follow-up times from treatment initiation were 15.4 months (range 0.1 to 37.0), 13.3 months (range 0.3 to 36.6) and 14.0 months (range 1.9 to 36.5) with first-line nivolumab plus ipilimumab, anti-PD-1 monotherapy and BRAF/MEK inhibitors, respectively.
Concurrent steroid use
Concurrent steroid use served to identify patients with symptomatic MBM. Among the 472 patients included in the analysis, 369 patients (78%) did not receive steroids (and were considered asymptomatic), 52 patients (11%) received concurrent steroids (and were considered symptomatic) and 51 patients (11%) received steroids outside of the concurrent steroid definition (ie, not within the 15 days before the start of first-line treatment) (table 1).
Concurrent radiation use
Among the 472 patients included in the analysis, 347 patients (74%) did not receive concurrent radiation, 101 patients (21%) received concurrent radiation (stereotactic, intensity-modulated, three-dimensional conformal and gamma knife radiation) and 24 patients (5%) received sequential radiation (defined as radiation that started 30 days or more before/after first-line systemic treatment initiation) (table 1). The median time from the first dose of systemic therapy (with nivolumab plus ipilimumab, anti-PD-1 monotherapy or BRAF/MEK inhibitors) to radiation therapy or vice versa was 12 days (range −671 to 160). Types of first radiation therapy were stereotactic (74%), intensity-modulated (17%) and three-dimensional conformal (9%) radiation (online supplemental table 1).
OS and PFS in the overall study group
In the overall study group, numerically longer OS was observed with nivolumab plus ipilimumab versus anti-PD-1 monotherapy (HR 0.47, 95% CI 0.34 to 0.67) or BRAF/MEK inhibitors (HR 0.72, 95% CI 0.50 to 1.04) (figure 1A). Median OS was 36.0 months (95% CI 32.1 to not reached (NR)) with nivolumab plus ipilimumab, 18.8 months (95% CI 13.0 to 26.0) with anti-PD-1 monotherapy and NR (95% CI 19.4 to NR) with BRAF/MEK inhibitors. One-year OS rates were 79%, 60% and 72% with nivolumab plus ipilimumab, anti-PD-1 monotherapy and BRAF/MEK inhibitors, respectively.

OS and PFS in the overall study group (patients with asymptomatic or symptomatic MBM) by first-line treatment. Shaded areas indicate 95% CIs. MBM, melanoma brain metastasis; mo, month; NR, not reached; OS, overall survival; PD-1, programmed death-1; PFS, progression-free survival.
Numerically longer PFS was observed with nivolumab plus ipilimumab versus anti-PD-1 monotherapy (HR 0.74, 95% CI 0.53 to 1.02) or BRAF/MEK inhibitors (HR 0.82, 95% CI 0.60 to 1.12) (figure 1B). Median PFS was 22.7 months (95% CI 19.3 to 28.3) with nivolumab plus ipilimumab, 16.8 months (95% CI 11.6 to 24.9) with anti-PD-1 monotherapy and 15.4 months (95% CI 12.7 to NR) with BRAF/MEK inhibitors. One-year PFS rates were 68%, 58% and 59% with nivolumab plus ipilimumab, anti-PD-1 monotherapy and BRAF/MEK inhibitors, respectively.
OS in patients with asymptomatic MBM
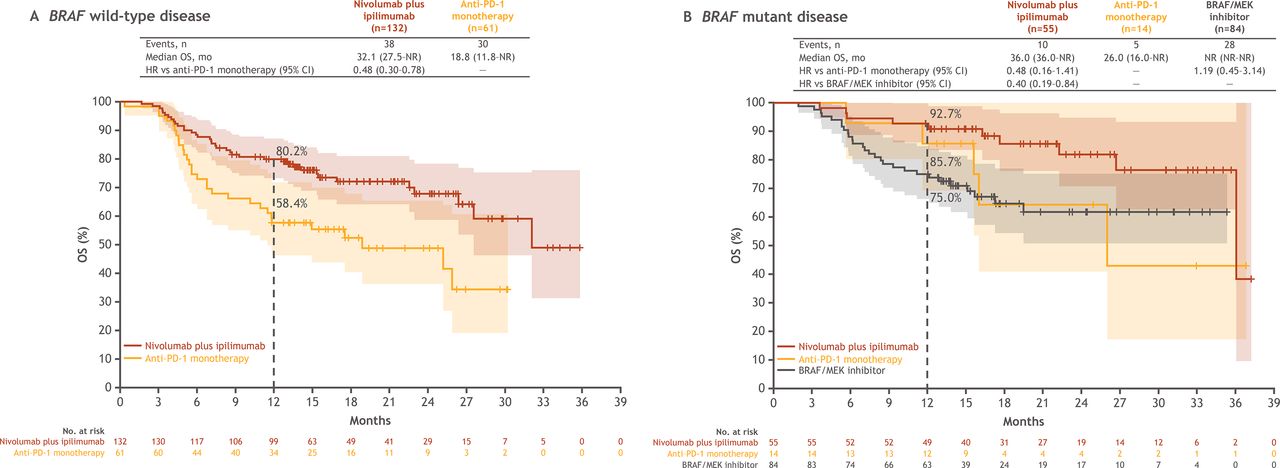
Among patients with BRAF wild-type, asymptomatic MBM, numerically longer OS was observed with nivolumab plus ipilimumab versus anti-PD-1 monotherapy (HR 0.48, 95% CI 0.30 to 0.78) (figure 2A). Median OS was 32.1 months (95% CI 27.5 to NR) with nivolumab plus ipilimumab and 18.8 months (95% CI 11.8 to NR) with anti-PD-1 monotherapy. One-year OS rates were 80% and 58%, respectively.

OS in patients with asymptomatic MBM by first-line treatment and BRAF status. Shaded areas indicate 95% CIs. MBM, melanoma brain metastasis; mo, month; NR, not reached; OS, overall survival; PD-1, programmed death-1.
Among patients with BRAF mutant, asymptomatic MBM, numerically longer OS was observed with nivolumab plus ipilimumab versus anti-PD-1 monotherapy (HR 0.48, 95% CI 0.16 to 1.41) or BRAF/MEK inhibitors (HR 0.40, 95% CI 0.19 to 0.84) (figure 2B). Median OS was 36.0 months (95% CI 36.0 to NR) with nivolumab plus ipilimumab, 26.0 months (95% CI 16.0 to NR) with anti-PD-1 monotherapy and NR (95% CI NR to NR) with BRAF/MEK inhibitors. There were few patients treated with nivolumab plus ipilimumab at 36 months, resulting in a drop in the Kaplan-Meier curve for that group. One-year OS rates were 93%, 86% and 75%, respectively.
OS in patients with symptomatic MBM
Among patients with BRAF wild-type, symptomatic MBM, numerically longer OS was observed with nivolumab plus ipilimumab versus anti-PD-1 monotherapy (HR 0.16, 95% CI 0.05 to 0.53), although sample sizes were small (online supplemental figure 2A). Median OS was NR (95% CI 9.2 to NR) with nivolumab plus ipilimumab and 4.7 months (95% CI 2.3 to NR) with anti-PD-1 monotherapy. One-year OS rates were 69% and 18%, respectively.
Among patients with BRAF mutant, symptomatic MBM, numerically longer OS was observed with nivolumab plus ipilimumab versus anti-PD-1 monotherapy (HR 0.27, 95% CI 0.06 to 1.25) and numerically shorter OS was observed with nivolumab plus ipilimumab versus BRAF/MEK inhibitors (HR 1.59, 95% CI 0.42 to 6.04), although sample sizes were small (online supplemental figure 2B). Median OS was 11.1 months (95% CI 7.7 to NR) with nivolumab plus ipilimumab, 4.1 months (95% CI 2.8 to NR) with anti-PD-1 monotherapy and 23.0 (95% CI 21.4 to NR) with BRAF/MEK inhibitors. One-year OS rates were 40%, 25% and 68%, respectively.
PFS in patients with asymptomatic MBM
Among patients with BRAF wild-type, asymptomatic MBM, numerically longer PFS was observed with nivolumab plus ipilimumab versus anti-PD-1 monotherapy (HR 0.80, 95% CI 0.50 to 1.26) (figure 3A). Median PFS was 24.1 months (95% CI 18.8 to NR) with nivolumab plus ipilimumab and 23.0 months (95% CI 13.6 to NR) with anti-PD-1 monotherapy. One-year PFS rates were 71% and 63%, respectively.

{kind=link}
{kind=link}
{kind=link}
PFS in patients with asymptomatic MBM by first-line treatment and BRAF status. Shaded areas indicate 95% CIs. MBM, melanoma brain metastasis; mo, month; NR, not reached; PD-1, programmed death-1; PFS, progression-free survival.
Among patients with BRAF mutant, asymptomatic MBM, numerically longer PFS was observed with nivolumab plus ipilimumab versus anti-PD-1 monotherapy (HR 0.80, 95% CI 0.35 to 1.85) or BRAF/MEK inhibitors (HR 0.83, 95% CI 0.51 to 1.35) (figure 3B). Median PFS was 21.5 months (95% CI 17.9 to 28.3) with nivolumab plus ipilimumab, 16.3 months (95% CI 16.2 to NR) with anti-PD-1 monotherapy and 28.9 months (95% CI 12.8 to NR) with BRAF/MEK inhibitors. One-year PFS rates were 77%, 79% and 62%, respectively.
PFS in patients with symptomatic MBM
Among patients with BRAF wild-type, symptomatic MBM, numerically longer PFS was observed with nivolumab plus ipilimumab versus anti-PD-1 monotherapy (HR 0.21, 95% CI 0.07 to 0.66), although sample sizes were small (online supplemental figure 3A). Median PFS was NR (95% CI 7.5 to NR) with nivolumab plus ipilimumab and 4.5 months (95% CI 3.1 to NR) with anti-PD-1 monotherapy. One-year PFS rates were 62% and 11%, respectively.
Among patients with BRAF mutant, symptomatic MBM, numerically longer PFS was observed with nivolumab plus ipilimumab versus anti-PD-1 monotherapy (HR 0.37, 95% CI 0.05 to 2.76) and numerically shorter PFS was observed with nivolumab plus ipilimumab versus BRAF/MEK inhibitors (HR 1.29, 95% CI 0.27 to 6.15), although sample sizes were small (online supplemental figure 3B). Median PFS was NR (95% CI 5.4 months to NR) with nivolumab plus ipilimumab, 11.6 months (95% CI 3.5 to NR) with anti-PD-1 monotherapy and 22.5 months (95% CI 14.0 to NR) with BRAF/MEK inhibitors. One-year PFS rates were 50%, 0% and 72%, respectively.
OS and PFS in patients with MBM without or with concurrent radiation
Sample sizes were small in patients with MBM without or with concurrent radiation. Among patients without concurrent radiation and with BRAF wild-type MBM, numerically longer OS was observed with nivolumab plus ipilimumab versus anti-PD-1 monotherapy (HR 0.44, 95% CI 0.28 to 0.72) (online supplemental figure 4 A). Among patients without concurrent radiation and with BRAF mutant MBM, numerically longer OS was observed with nivolumab plus ipilimumab versus anti-PD-1 monotherapy (HR 0.48, 95% CI 0.15 to 1.56) or BRAF/MEK inhibitors (HR 0.43, 95% CI 0.20 to 0.90) (online supplemental figure 4B). Among patients with concurrent radiation and BRAF wild-type MBM, numerically longer OS was observed with nivolumab plus ipilimumab versus anti-PD-1 monotherapy (HR 0.29, 95% CI 0.12 to 0.68) (online supplemental figure 5A). Among patients with concurrent radiation and BRAF mutant MBM, numerically longer PFS was observed with nivolumab plus ipilimumab versus anti-PD-1 monotherapy (HR 0.85, 95% CI 0.31 to 2.31) and numerically shorter PFS was observed with nivolumab plus ipilimumab versus BRAF/MEK inhibitors (HR 1.30, 95% CI 0.60 to 2.81) (online supplemental figure 5B).
Among patients without concurrent radiation and with BRAF wild-type MBM, numerically longer PFS was observed with nivolumab plus ipilimumab versus anti-PD-1 monotherapy (HR 0.76, 95% CI 0.48 to 1.22) (online supplemental figure 6A). Among patients without concurrent radiation and with BRAF mutant MBM, numerically longer PFS was observed with nivolumab plus ipilimumab versus anti-PD-1 monotherapy (HR 0.82, 95% CI 0.31 to 2.15) or BRAF/MEK inhibitors (HR 0.72, 95% CI 0.43 to 1.21) (online supplemental figure 6B). Among patients with concurrent radiation and BRAF wild-type MBM, numerically longer PFS was observed with nivolumab plus ipilimumab versus anti-PD-1 monotherapy (HR 0.32, 95% CI 0.13 to 0.75) (online supplemental figure 7A). Among patients with concurrent radiation and BRAF mutant MBM, numerically longer PFS was observed with nivolumab plus ipilimumab versus anti-PD-1 monotherapy (HR 0.96, 95% CI 0.37 to 2.50) and numerically shorter PFS was observed with nivolumab plus ipilimumab versus BRAF/MEK inhibitors (HR 1.78, 95% CI 0.88 to 3.61) (online supplemental figure 7B).
Discussion
This retrospective chart review study collected real-world data of US patients diagnosed with MBM and treated by medical oncologists with different types of systemic therapy options in the first-line setting. Given that there is no prospective head-to-head trial comparing nivolumab plus ipilimumab with anti-PD-1 monotherapy or BRAF/MEK inhibitors in patients with MBM, this real-world study may provide valuable insights for clinical decision-making.
Certain baseline patient characteristics differed among the three treatment groups in this non-randomised study. Specifically, patients receiving nivolumab plus ipilimumab, compared with patients receiving anti-PD-1 monotherapy or BRAF/MEK inhibitors, had favourable baseline prognostic factors, such as younger age, fewer or smaller brain metastases, better ECOG PS, less frequently elevated LDH, better CCI scores and less frequent steroid use before the index date. It is possible that, in some cases, physicians may have reserved therapy with nivolumab plus ipilimumab for patients who had favourable baseline prognostic factors and were therefore considered more likely to tolerate toxicities associated with combination immunotherapy.
In this study, first-line treatment with nivolumab plus ipilimumab appeared to provide benefit compared with first-line treatment with anti-PD-1 monotherapy or BRAF/MEK inhibitors in patients with MBM, of whom 78% had asymptomatic disease (symptomatic disease was based on any steroid therapy received within the 15 days prior to the start of first-line treatment to ensure that steroid administration was not likely due to immune-related AEs; however, steroids may still have been administered during that time period for managing immune-related AEs). Numerically longer OS and PFS were observed with nivolumab plus ipilimumab versus anti-PD-1 monotherapy and BRAF/MEK inhibitors. At 1 year, OS rates were 79%, 60% and 72% with nivolumab plus ipilimumab, anti-PD-1 monotherapy and BRAF/MEK inhibitors, respectively, and PFS rates were 68%, 58% and 59%, respectively. However, the observed benefit may have been due to confounding and selection bias, given that patients receiving nivolumab plus ipilimumab had favourable baseline prognostic factors compared with patients receiving anti-PD-1 monotherapy or BRAF/MEK inhibitors.
Effectiveness results in this real-world study were generally consistent with data across clinical trials involving patients with MBM,8 10 13 14 19–22 although cross-trial comparisons are difficult because of differences in study populations and methodologies. For example, among patients with asymptomatic MBM, 1-year OS rates were 63% and approximately 80% with nivolumab plus ipilimumab in the phase 2 ABC trial10 and CheckMate 204 trial,8 respectively; 60% with nivolumab in the ABC trial10 and approximately 60% with pembrolizumab in another phase 2 trial13; and 46% with dabrafenib plus trametinib in the phase 2 COMBI-MB trial.14 Results from the current study were also consistent with those from the real-world German DeCOG and NICO studies in which 1-year OS rates were 69% and 59%, respectively, in patients with MBM treated with nivolumab plus ipilimumab.19 20 In addition, these real-world results are in line with findings of two separate meta-analyses using data from clinical trials and real-world studies, respectively, that suggested advantages with nivolumab plus ipilimumab compared with other systemic treatments in patients with MBM.21 22 Furthermore, 1-year OS rates in patients with MBM treated with nivolumab plus ipilimumab in this real-world study and the ABC trial10 and the CheckMate 204 trial8 were similar to that in patients with advanced melanoma not having active brain metastases who were treated with nivolumab plus ipilimumab in the phase 3 CheckMate 067 trial,23 suggesting that nivolumab plus ipilimumab is effective regardless of the presence of brain metastasis.
Effectiveness was evaluated in this real-world study in subgroups according to asymptomatic or symptomatic MBM and BRAF wild-type or mutant status. Numerically longer OS and PFS were observed with nivolumab plus ipilimumab versus anti-PD-1 monotherapy, regardless of symptom or BRAF status. In addition, numerically longer OS and PFS were observed with nivolumab plus ipilimumab versus BRAF/MEK inhibitors with asymptomatic, BRAF mutant MBM, but numerically shorter OS and PFS were observed with nivolumab plus ipilimumab versus BRAF/MEK inhibitors with symptomatic, BRAF mutant MBM. However, sample sizes for patients with symptomatic MBM were small. Numerically longer OS was observed among patients with asymptomatic than symptomatic MBM, consistent with results in clinical studies.8–10 14 Among patients with BRAF wild-type or mutant symptomatic MBM, 1-year OS rates with nivolumab plus ipilimumab were 69% and 40%, respectively, which were consistent with results from the CheckMate 204 trial showing a 1-year OS rate of approximately 40% in patients with symptomatic (BRAF wild-type or mutant) MBM treated with nivolumab plus ipilimumab.8
OS and PFS were estimated in this real-world study in subgroups without or with concurrent radiation by BRAF mutation status, although sample sizes were too small to allow a confident interpretation of the results. Numerically longer OS and PFS were observed with nivolumab plus ipilimumab versus anti-PD-1 monotherapy, regardless of the use of concurrent radiation or BRAF mutation status. In addition, numerically longer OS and PFS were observed with nivolumab plus ipilimumab versus BRAF/MEK inhibitors with BRAF mutant MBM and no concurrent radiation use, but numerically shorter OS and PFS were observed with nivolumab plus ipilimumab versus BRAF/MEK inhibitors with BRAF mutant MBM and concurrent radiation use.
New therapies have emerged for the treatment of patients with advanced melanoma, and in the phase 2/3 RELATIVITY 047 trial, a novel, dual immune checkpoint inhibitor combination of nivolumab plus relatlimab (a lymphocyte-activation gene 3 inhibitor) appeared to have central nervous system (CNS) activity in patients with advanced melanoma.24 In that trial, new CNS metastases developed less frequently in patients treated with nivolumab plus relatlimab than with nivolumab alone (5% vs 9%) and the time to development of new CNS lesions was longer with the combination than with nivolumab monotherapy (patients with new CNS lesions at 2 years, 6.5% and 10.0%, respectively).24 However, those results were limited by the low occurrence of new CNS metastases in both treatment groups. The safety and efficacy of nivolumab plus relatlimab in patients with active MBM is being investigated in the single-arm, open-label, phase 2 BLUEBONNET trial (ClinicalTrials.gov identifier: NCT05704647).25
This real-world study had certain limitations. First, because this was a non-randomised comparison of three treatment regimens, there was likely substantial confounding and selection bias. Thus, the study may have been limited by heterogeneity in baseline patient characteristics between the treatment groups. As previously stated, the observed benefit in patients receiving nivolumab plus ipilimumab may have been due to confounding and selection bias, given that those patients had favourable baseline prognostic factors. At baseline, patients treated with anti-PD-1 monotherapy or BRAF/MEK inhibitors were more likely to have a greater number of or larger brain metastases, poorer ECOG PS or greater frequency of increased LDH than patients treated with nivolumab plus ipilimumab. In addition, there may have been inconsistencies among the treatment groups in investigator assessments (eg, ECOG PS assessment) and in treatment selection based on clinical trial evidence and therapeutic guidelines. Interpretation of OS and PFS results in certain subgroups was impeded by small sample sizes. Furthermore, tumour response was not reported because of variability in investigator assessments. Although dates of progression were collected in the CRF, progression was based on investigator assessment and not on Response Evaluation Criteria in Solid Tumors, V.1.1. The date of progression was determined by the treating physician based on chart review and not necessarily any radiological confirmation. As the CRF did not distinguish between asymptomatic and symptomatic MBM, concurrent steroid use served as a surrogate method for identifying patients with symptomatic MBM. Although concurrent steroid use was defined as any steroid therapy received within the 15 days prior to the start of first-line treatment to ensure that steroid administration was not likely due to immune-related AEs, it was still possible that steroids were administered during that time period for managing immune-related AEs. Additionally, patients selected by the study physicians may not have been representative of the general melanoma population because of selection bias, and physicians who chose to participate in the study may not have accurately represented the broader population of melanoma-treating oncologists. Moreover, despite efforts to minimise missing or inaccurate data, the retrospective nature of this chart review study may still have resulted in some missing or inaccurate data points. Finally, treatment practices for MBM may have changed since patients in this study began treatment (June 2017 through June 2019).
In conclusion, results from this retrospective chart review study, which collected real-world data of US patients diagnosed with MBM and treated by medical oncologists, supplement data from clinical trials evaluating this subset of patients. Among patients with MBM in this real-world study, numerically longer OS and PFS were observed with first-line nivolumab plus ipilimumab versus first-line anti-PD-1 monotherapy or BRAF/MEK inhibitors. These results are generally consistent with those in clinical trials and real-world studies with these treatments in patients with MBM. Given that there are no prospective head-to-head trials comparing nivolumab plus ipilimumab with anti-PD-1 monotherapy or BRAF/MEK inhibitors in patients with MBM, this real-world study may provide valuable insights for clinical decision-making. Additional studies are required to investigate first-line treatments for patients with MBM.
Data availability statement
Data are available upon reasonable request. Interested researchers may request access by contacting the corresponding author or Bristol Myers Squibb directly by submitting an inquiry through the following link: https://www.bms.com/researchers-and-partners/independent-research/data-sharing-request-process.html. Access will be subject to Bristol Myers Squibb’s policies and may require a data use agreement.
Ethics statements
Patient consent for publication
Ethics approval
The protocol, amendments and subject informed consent received appropriate approval by the Institutional Review Board/Independent Ethics Committee (WCG Clinical Services, Princeton, New Jersey, USA) or other applicable review board as required by local law prior to initiation of study at the site. Investigators were to ensure that patients, or, in those situations where consent could not be given by patients, their legally acceptable representatives, were clearly informed about the purpose, potential risks and other critical issues regarding this study. The study was conducted in accordance with International Society for Pharmacoepidemiology Guidelines for Good Pharmacoepidemiology Practices.
Acknowledgments
The authors thank the patients and investigators who participated in this study. They acknowledge Ono Pharmaceutical Company, Ltd. (Osaka, Japan) for contributions to nivolumab development. Contributions to the study design and data analysis were provided by Shelby Corman, who was at Open Health at the time of the analysis. Contributions to the data analysis were provided by Joyce Qian, who was at Open Health at the time of the analysis. Professional medical writing and editorial assistance were provided by Mark Palangio and Michele Salernitano of Ashfield MedComms, an Inizio company, funded by Bristol Myers Squibb; specifically, Mark Palangio assisted with the development of the first draft and subsequent revisions, under the direction of the authors, and Michele Salernitano provided editorial support for formatting and submission.
References
Footnotes
Presented at Presented at Society for Melanoma Research (SMR) 18th International Congress; October 28–31, 2021; New Orleans, Louisiana, USA (hybrid congress).
Contributors Conception or design: JP, LAS, AM, JKS. Data acquisition: NH, SO. Data analysis: NH, SO, JKS, NN. Data interpretation: ICGO, JP, LAS, DP, AM, SC. Manuscript writing: All authors. Final approval of manuscript: All authors. Accountable for all aspects of the work: All authors. SC is the guarantor.
Funding This study was supported by Bristol Myers Squibb (Princeton, NJ, USA).
Disclaimer To view the most recent and complete version of the NCCN guideline, go online to NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way. NCCN, National Comprehensive Cancer Network.
Competing interests ICGO reports receiving medical writing support for the present manuscript from Bristol Myers Squibb; research funding (institutional) from Bristol Myers Squibb, Merck and Pfizer; consulting fees from Midatech; payment or honoraria for presentations or educational events from Pfizer; and fees for advisory board participation from Bristol Myers Squibb, Novartis and Pfizer. JP reports receiving medical writing support for the present manuscript from Bristol Myers Squibb and being an employee of and having received stocks/stock options from Bristol Myers Squibb. LAS reports receiving medical writing support for the present manuscript from Bristol Myers Squibb and being an employee of Bristol Myers Squibb. DP reports receiving medical writing support for the present manuscript from Bristol Myers Squibb and being an employee of and having received stocks/stock options from Bristol Myers Squibb. AM reports receiving medical writing support for the present manuscript from Bristol Myers Squibb and being an employee of and having received stocks/stock options from Bristol Myers Squibb. NH reports receiving medical writing support for the present manuscript from Bristol Myers Squibb and being an employee of RTI Health Solutions which received payment from Bristol Myers Squibb for participation in this research. SO reports receiving medical writing support for the present manuscript from Bristol Myers Squibb and being an employee of RTI Health Solutions which received payment from Bristol Myers Squibb for participation in this research. JKS reports receiving medical writing support for the present manuscript from Bristol Myers Squibb and being an employee of Open Health which received payment from Bristol Myers Squibb for participation in this research. NN reports receiving medical writing support for the present manuscript from Bristol Myers Squibb and being an employee of Open Health which received payment from Bristol Myers Squibb for participation in this research. SC reports receiving medical writing support for the present manuscript from Bristol Myers Squibb; fees for advisory board participation from Alkermes, Bristol Myers Squibb, Novartis, Pfizer and Regeneron; and participation in the National Comprehensive Cancer Network Guidelines for melanoma.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.